A Novel Approach to Maintaining Normothermia in Major Spinal Deformity Surgery with an Esophageal Warming Device
A B S T R A C T
Maintenance of normothermia is a priority during major spinal deformity surgery. However, this is difficult due to the large body surface area exposed to ambient temperatures. We report the novel use of an esophageal warming device, added to standard care, to maintain normothermia in three patients. We conclude that esophageal warming is feasible in major spine surgery with no apparent complications. Safety and efficacy, as compared to standard warming devices, will need to be determined in future prospective trials.
Keywords
Spine surgery, intraoperative, normothermia, esophageal warming
Introduction
Maintenance of intraoperative normothermia is standard of care in modern surgical practice. Intraoperative hypothermia may contribute to perioperative morbidity by causing coagulopathy and increasing the risk of postoperative shivering and cardiac events [1]. Furthermore, current international guidelines recommend the maintenance of normothermia intraoperatively to reduce the risk of surgical site infection [2].
Normothermia is difficult to maintain during major spine deformity surgery, with core temperatures easily falling below 35°C. This occurs due to heat loss from large body surface exposure and low ambient temperatures. During these cases, only the upper and lower extremities and head can be covered with an external warming device and actively warmed. We explored the feasibility of using a novel esophageal warming device (EWD; ensoETM, Attune Medical, Chicago, IL, USA) to maintain normothermia in patients undergoing major spinal deformity surgery. The device is approved by the United States Food and Drug Administration.
Methods
After induction of general anesthesia and endotracheal intubation, the EWD was lubricated and inserted into the esophagus (Figures 1-4). Patients with esophageal pathology were excluded. The EWD is composed of a non-permeable, silicone triple lumen system consisting of a fluid intake lumen, fluid return/output lumen, and separate central orogastric tube (for suction of gastric secretions). The device transfers heat to the body from the esophagus to closely apposed vascular structures such as the vena cava, aorta, and left atrium. The device was connected to a Norm-O-Temp® fluid warmer (Cincinnati Sub-Zero, Cincinnati, OH) and run at 42 °C throughout the case. The core temperature was monitored with a bladder probe (embedded in a urinary catheter). Lower body forced-air warmers, and IV fluid warmers were also used to avoid hypothermia.

Figure 1: Esophageal warming device (EWD; clear tubing) attached to the fluid intake/return line (black tubing).

Figure 2: Norm-o-temp warming device which attaches to the EWD.

Figure 3: Anteroposterior chest radiograph showing the tip of the EWD in the stomach.

Figure 4: Lateral lumbar spine radiographs showing the tip of the EWD in the stomach.
Case Presentation
Case I
A 69-year-old 45 kg woman had a lumbar scoliotic deformity with progressive low back & leg pain. The medical history was significant for common variable immunodeficiency on intravenous immunoglobulin therapy, and psoriatic arthritis on chronic steroids. She underwent L3-L4 laminectomies and T4-pelvic fusion. The intra-operative temperature was maintained at 36.1-37.1 °C.
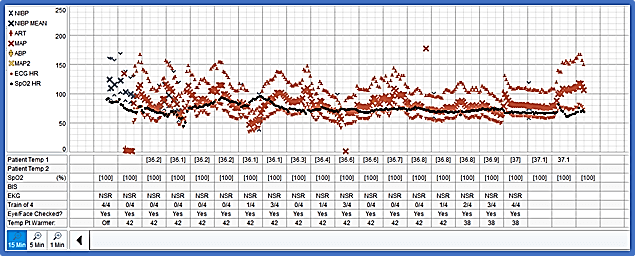
Figure 5: Intraoperative vital signs including temperature from Case I.
Case II
A 77-year-old 48kg woman with a lumbar scoliotic deformity underwent T10-pelvic fusion for medically refractory back pain and radiculopathy. The intra-operative temperature was maintained at 36.1-36.7 °C.
Case III
A 77-year-old 47kg woman with a history of chronic lymphocytic leukemia, osteopenia, hypothyroidism, and obstructive sleep apnea had lumbar scoliotic deformity with associated severe L2-L4 stenosis and progressive low back and leg pain. She underwent fusion from T10-pelvis with pedicle screw fixation, L3-4 laminectomies, and L3 subtraction osteotomy. The intra-operative temperature was maintained at 36.7-37.0 ℃. There were no adverse events associated with the device and no reports of postoperative dysphagia.
Discussion
The EWD appears to be useful in maintaining normothermia in major spine deformity surgery, in conjunction with both forced-air warming of the legs and intravenous fluid warming. The EWD was originally developed as a cooling device for maintenance of hypothermia in comatose survivors of cardiac arrest [3, 4]. Its use in treating hyperthermia in the setting of acute brain injury has also been reported [5].This is the first report, to our knowledge, to describe the use of the device to maintain intraoperative normothermia via esophageal warming.
Major spinal deformity surgery for degenerative scoliosis in fragile elderly patients is challenging from both a surgical and anesthetic perspective. Optimal care of these patients requires maintenance of normothermia to minimize coagulopathy, blood loss, and postoperative morbidity, including surgical site infections. The use of an EWD to maintain normothermia, in conjunction with forced air and IV fluid warming, is a novel approach to accomplishing this goal.
Current options for maintaining normothermia in spine surgery are limited. Forced-air warming is limited by the lack of access to the torso. Underbody fluid warming blankets are difficult to position and use on an OSI surgical table. Fluid warmers and forced air warmers are useful but are usually inadequate for maintaining normothermia. No single device, in our experience, has adequate efficacy in maintaining normothermia in these cases. Therefore, further study of the EWD in major spine surgery is warranted.
Conclusion
Intraoperative patient warming with an EWD is feasible in major spine deformity surgery. Internal esophageal warming is a novel approach that will need to be formally tested against other methods of intraoperative temperature control.
Abbreviation
EWD: Esophageal Warming Device
Funding
UT Southwestern Medical Center; Esophageal warming devices provided by Attune Medical (Link).
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Wed 13, May 2020Accepted: Mon 01, Jun 2020
Published: Fri 12, Jun 2020
Copyright
© 2023 David L. McDonagh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.06.05
Figures & Tables
References
- McSwain JR, Yared M, Doty JW, Wilson SH (2015) Perioperative hypothermia: Causes, consequences and treatment. World J Anesthesiol 4: 58-65.
- Berríos Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC et al. (2017) Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg 152: 784-791. [Crossref]
- Goury A, Poirson F, Chaput U, Voicu S, Garçon P et al. (2017) Targeted Temperature Management Using the "Esophageal Cooling Device" After Cardiac Arrest (The COOL Study): A Feasibility and Safety Study. Resuscitation 121: 54-61. [Crossref]
- Naiman MI, Gray M, Haymore J, Hegazy AF, Markota A et al. (2017) Esophageal Heat Transfer for Patient Temperature Control and Targeted Temperature Management. J Vis Exp 129: 56579. [Crossref]
- Khan I, Haymore J, Barnaba B, Armahizer M, Melinosky C et al. (2018) Esophageal Cooling Device Versus Other Temperature Modulation Devices for Therapeutic Normothermia in Subarachnoid and Intracranial Hemorrhage. Ther Hypothermia Temp Manag 8: 53-58. [Crossref]