.jpg)
Adenomatoid Hyperplasia: Case Report of a Rare Lesion in Uncommon Location
Atousa Aminzadeh1 , Keivan Shirneshan2* , Nooshnaz Sabour3 and Mohammadreza Korang Beheshti3
1Department of Oral Pathology, School of Dentistry, Islamic Azad University Isfahan (Khorasgan) Branch, Isfahan, Iran .
2Md, MSc, General Pathologist, Private Practice, Isfahan, Iran .
3School of Dentistry, Islamic Azad University Isfahan(Khorasgan) Branch, Isfahan, Iran .
http://dx.doi.org/10.12944/EDJ.02.02.04
Adenomatoid hyperplasia is a rare lesion of the minor salivary glands recognized by localized swelling that mimics a neoplasm. This so called pseudotumor usually occurring in adults 4th to 6th decade of life mostly, in 80 percent, occurs as a unilateral swelling without ulcer on the hard and soft palate. The pathogenesis of this condition is not well known but local trauma might have a role. In this case report three cases of adenomatoid hyperplasia have been reported to bring attention to this lesion as it is clinically similar to many soft tissue lesions of oral mucosa so should be considered while making a clinical diagnosis. Also, Pathologists should investigate a proper sample size under a microscope not to confuse a normal salivary gland adjacent to salivary gland tumours with Adenomatoid hyperplasia.
Adenomatoid Hyperplasia; Hypertrophy; Minor Salivary Gland; Mouth; Palate
Copy the following to cite this article:
Aminzadeh A, Shirneshan K, Sabour N, Beheshti M. K. Adenomatoid Hyperplasia: Case Report of a Rare Lesion in Uncommon Location. Enviro Dental Journal 2021; 2(2). DOI:http://dx.doi.org/10.12944/EDJ.02.02.04
Copy the following to cite this URL:
Aminzadeh A, Shirneshan K, Sabour N, Beheshti M. K. Adenomatoid Hyperplasia: Case Report of a Rare Lesion in Uncommon Location. Enviro Dental Journal 2021; 2(2). Available From : https://bit.ly/3v1cxqT
Download article (pdf) Citation Manager

Introduction
Adenomatoid hyperplasia was first described by Giansanti et al in 1971. They described Two cases of an intraoral minor salivary gland lesion which they introduced as unique lesions. The nature of these lesions was not known by that time for authors but they believed it was a hyperplasia kind of adenoma. (1) Adenomatoid hyperplasia is a rare lesion of the minor salivary glands recognized by localized swelling that mimics a neoplasm. (2) Adenomatoid hyperplasia or adenomatoid acinar hyperplasia as opposed to adenomatoid ductal hyperplasia which occurs mostly in the parotid gland occurs in the minor salivary gland and involves acinar hyperplasia. (3). This so-called pseudotumor usually occurring in adults 4th to 6th decade of life mostly, in 80%, occurs as a unilateral swelling without ulcer on the hard and soft palate. The pathogenesis of this condition is not well known but local trauma might have a role. This reactive hyperplasia has been seen in smokers and denture wearers. also adjacent to neoplasms and necrotizing sialo metaplasia. In a rare case, it was related to a chromosomal translocation t (2,14). (2,3,4) Adenomatoid hyperplasia most often occurs as a sessile soft or firm painless mass normal in colour or as some have been reported previously red or blue. In the microscopic examination, lobular aggregates of normal-appearing mucous acini are found which are greater in number than would usually find in any given area. (2) Hyperplasia and hypertrophy of mucous acini often with fewer ducts than normal are seen. Since clinically it looks like a tumour biopsy is necessary to rule out benign and malignant soft tissue tumours. Once the diagnosis of adenomatoid hyperplasia is made no other treatment is required and the lesion should not recur. The pathologist has to be careful not to mistake adenomatoid hyperplasia with adjacent normal salivary glands in biopsies of true salivary gland tumours. So a good clinical and pathological correlation is important in the final diagnosis. (2) Although this lesion is benign a conservative biopsy and histological examination is necessary to rule out salivary gland neoplasms. Here 3 case of adenomatoid hyperplasia is introduced to bring attention to this lesion.
Report of Cases
Case Number 1
A 45 years old female patient with an asymptomatic red bluish lesion on the floor of the mouth with a clinical diagnosis of soft tissue tumour was referred to an oral surgeon. Under local anaesthesia, an excisional biopsy was performed and submitted for histopathologic review to the oral pathology laboratory in 10% buffered formalin. Routine laboratory processes were performed, and paraffin blocks were prepared. From each paraffin block,4 to 5µm sections were prepared and stained with H&E stain for microscopic examination. Microscopically circumscribed encapsulated lobules of normal-looking mucinous acini were observed in excess in lamina progeria of the otherwise normal oral mucosa. Hypertrophy of mucous acini was not observed. (figure 1A) The patient was followed for 1 year and no recurrence was reported.
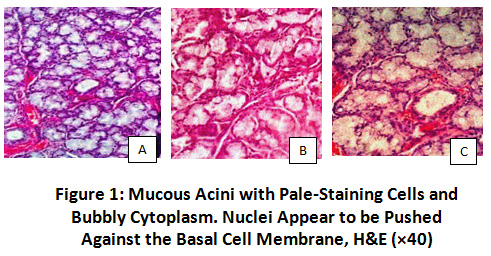 |
Figure 1: Mucous acini with pale-staining cells and bubbly cytoplasm. Nuclei appear to be pushed against the basal cell membrane, H&E (×40) Click here to view Figure |
Case Number 2
A 32 years old male patient with the complaint of brown projection in the inferior labial vestibule with the primary clinical diagnosis of mucocele and hemangioma was referred to the oral surgeon. A biopsy was performed and paraffin blocks were prepared under routine laboratory processes. Microscopic evaluation of the lesion was performed, and the final diagnosis was adenomatoid hyperplasia of a minor labial salivary gland. (figure1B) The patient was followed for 6 months with no recurrence.
Case Number 3
A 35-year-old male patient was referred to the dental clinic with a chief complaint of pain while chewing. A red lesion was observed on the palate without any secretion and a gradual enlargement was reported by the patient without any familial history. An excisional biopsy was performed. In microscopic evaluation hypertrophy and hyperplasia of mucous acini were observed with few ductal hyperplasia’s and local minor inflammation around ducts. (figure1C) The patient was followed for 6 months with no recurrence.
Table 1: Clinical and Histopathologic Features of Reported Cases in Brief.
|
|
Age |
Gender |
Location |
Symptom |
Histopathology |
Recurrence |
|
Case 1 |
45 |
female |
Floor of mouth |
Non
|
hyperplasia of mucous acini
|
No |
|
Case 2 |
32 |
male |
Inferior labial vestibule |
Non
|
hyperplasia of mucous acini
|
No
|
|
Case 3 |
35 |
male |
palate |
Pain on chewing |
hypertrophy and hyperplasia of mucous acini ductal hyperplasia localized minor inflammation around ducts |
No
|
Discussion
Adenomatoid hyperplasia is a rare lesion of the 4th and 6th decade as seen in our study and other case reports. Barrettes and Speight have reported adenomatoid hyperplasia is a rare cause of oral mucosal swelling but it is significant because of its clinical resemblance to salivary gland tumors.19 of 20 cases reported by these authors have occurred in the hard or soft palate (4). Bryanti et al have also reported a case of adenomatoid hyperplasia in the palate. (5) And as it was mentioned previously the most commonplace reported for this lesion in the palate. But cases reported in our case have occurred in unusual places: labial mucosa and floor of the mouth and one case was in the hard palate. In 2014 Dereci and Cimen have reported a case of adenomatoid hyperplasia in the buccal mucosa. (6) Iwaki et al have reported mouth floor enlargements in edentulous patients because of sublingual salivary gland hyperplasia which is not implicated in our case (7). In the study of Barretts and Speight 14 subjects of 20 subjects diagnosed with adenomatoid hyperplasia were tobacco smokers, denture wearers, or both, which suggests chronic, local trauma may be an important factor in the development of the condition. In our case report none of the patients were smokers or denture users and had no history of local trauma to the area or any systemic disease as in the case reported by Dereci and Cimen. (6, 4).
Buchner et al have studied 40 cases of adenomatoid hyperplasia and believe some of the cases may represent a hamartoma or reactive hyperplasia, but in most cases, the nature of the hyperplasia isn't clear. Despite sialadenosis or enlarged major salivary glands, adenomatoid acini hyperplasia is not related to drugs, nutritional deficits, anorexia, Nervosa, and neurogenic factors. (6,9,8)
Among cases reported by us, only one had complained of pain and two others were asymptomatic. In that case, as inflammation was observed in microscopic evaluation of sample, pain might be due to local trauma to the lesion. Patients reported by Dereci and Cimen and Bryant et al did not have pain. (6,5)
Three cases reported here did not show recurrence after 12, and 6 months follow-ups as no recurrence have been reported in the literature yet. (12,13) No recurrence was even after 10 years of follow-up was seen in the study of Giansanti et al. (1) However, it is reported that one palatal case has developed into mucoepidermoid carcinoma years after diagnosis of adenomatoid hyperplasia. Malignant transformation of this case was thought to be related to chromosomal translocation t (2;14) which is the first cytogenetic study of this lesion by Manor et al. (5,10,8). Although shimoyama et al have studied the nuclear proliferation rate of cells in adenomatoid hyperplasia and found this was equal to normal cells in palatal mucosa. So it is not clear if this lesion has the potential to recur or change into a malignant lesion in the future. (11) We did not have clinical pictures of patients reported here which is a limitation of our study. Follow up was performed by phone.
Conclusion
Adenomatoid hyperplasia of minor salivary glands is a rare lesion usually occurring in palatal mucosa. Although as reported here can happen in any location of the oral cavity which has minor salivary glands. Its etiology and clinical significance are not known yet but as it is similar to many soft tissue lesions of oral mucosa such as fibroma, neurofibroma, hemangioma, mucocele, and salivary gland tumours it should be considered while making a clinical diagnosis (12,14). Pathologists should investigate a proper sample size under a microscope not to confuse a normal salivary gland adjacent to salivary gland tumours with Adenomatoid hyperplasia.
Acknowledgement
The author would like to thank, school of dentistry, Islamic azad university Isfahan(khorasgan) branch, Isfahan, Iran for their guidance and support to complete this article.
Funding Source
The author (s) received no financial support for the research, authorship, and/or publication of this article.
References
- Giansanti J.S, Baker G.O, Waldron C.A. Intraoral, mucinous, minor salivary gland lesions presenting clinically as tumors. Oral Surg Oral Med Oral Pathol. 1971; 32:918–922.
CrossRef - Neville BW, Damm DD, Allen CM, Chi A. Oral and maxillofacial pathology. 4th ed. New York: Elsevier.2016
- Woo, S.Oral pathology: A comprehensive atlas and text. 2nd edition. Philadelphia: Elsevier 2017.
- Barrett AW, Speight PM. Adenomatoid hyperplasia of oral minor salivary glands. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1995; 79: 482-487.
CrossRef - Bryant C, Manisali M, Barrett AW. Adenomatoid hyperplasia of palatal minor salivary glands. J Laryngol Otol. 1996 Feb;110(2):167-9. DOI: 10.1017/s0022215100133067. PMID: 8729505.
CrossRef - Dereci O, Cimen E. Adenomatoid hyperplasia of the minor salivary glands on the buccal mucosa: A rare case report. Int J Surg Case Rep. 2014;5(5):274-276. doi: 10.1016/j.ijscr.2014.03.020.
CrossRef - Iwaki Filho L, Damante José H, Consolaro A, Bonachela Wellington C, Damante Carla A. Mouth floor enlargements related to the sublingual glands in edentulous or partially edentulous patients: a microscopic study. J. Appl. Oral Sci. [Internet]. 2006 Aug [cited 2021 Jan 15]; 14(4): 264-269. https://doi.org/10.1590/S1678-77572006000400010.
CrossRef - Buchner A, Merrel P.W, Carpenter W.M, Leider A.S. Adenomatoid hyperplasia of minor salivary glands. Oral Surg Oral Med Oral Pathol. 1991; 71:583–587.
CrossRef - Arafat A, Brannon RB, Ellis GL. Adenomatoid hyperplasia of mucous salivary glands. Oral Surg Oral Med Oral Pathol.1981; 52: 51-55.
CrossRef - Manor E, Sinelnikov I, Brennan PA, Bodner L. Chromosomal aberrations in adenomatoid hyperplasia of the palatal minor salivary gland. Br J Oral Maxillofac Surg. 2013 Mar;51(2):170-2. DOI: 10.1016/j.bjoms.2012.04.079. Epub 2012 May 7. PMID: 22571812.
CrossRef - Shimoyama T, Wakabayashi M, Kato T, Kaneko T, Horie N, Ide F. Adenomatoid hyperplasia of the palate mimicking clinically as a salivary gland tumor. J Oral Sci. 2001 Jun;43(2):135-8. DOI: 10.2334/joined.43.135. PMID: 11515598.
CrossRef - Fernandes D, Silveria H, BUFALINO A, Almeida L, Dominguette M, Dominguette K, Leon J.Adenomatoid hyperplasia of the palate : An uncommon lesion often mimicking salivary gland tumor .Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology,Volume 130, Issue 3, 2020, Pages e125-e126.
CrossRef - Feitosa S, Marinho E, Viana K, Turatti E, BituU F, Cavalcante R, PEREIR K.Adenomatoid hyperplasia of the minor salivary glands :case report.Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology,Volume 129, Issue 1,2020,Page e102.
CrossRef - Srivathsa SH. Adenomatoid hyperplasia of the palatal minor salivary glands: A forgotten diagnosis? Int J Med Dent Case Rep 2017; 4:1-3.
CrossRef






