
Does the Heart Fall Asleep?—Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Protocol
2.2.1. Austria
2.2.2. Belgium
2.3. Behavioral Assessment and Data Analysis
2.3.1. Coma Recovery Scale-Revised
2.3.2. Electrocardiography
2.3.3. Heart Rate and Heart Rate Variability
2.3.4. Respiration
2.3.5. EEG Permutation Entropy
2.4. Statistical Analyses
3. Results
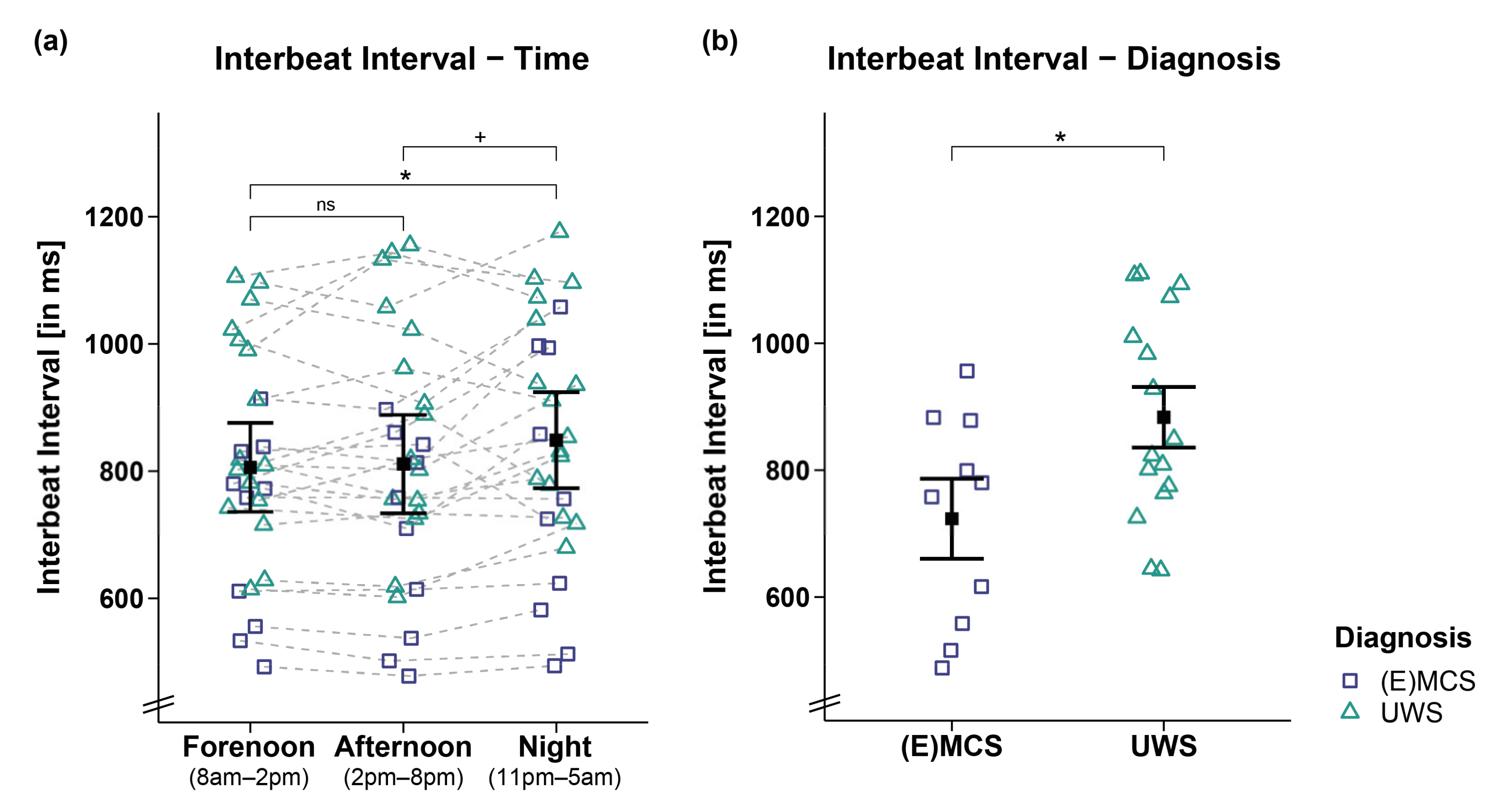
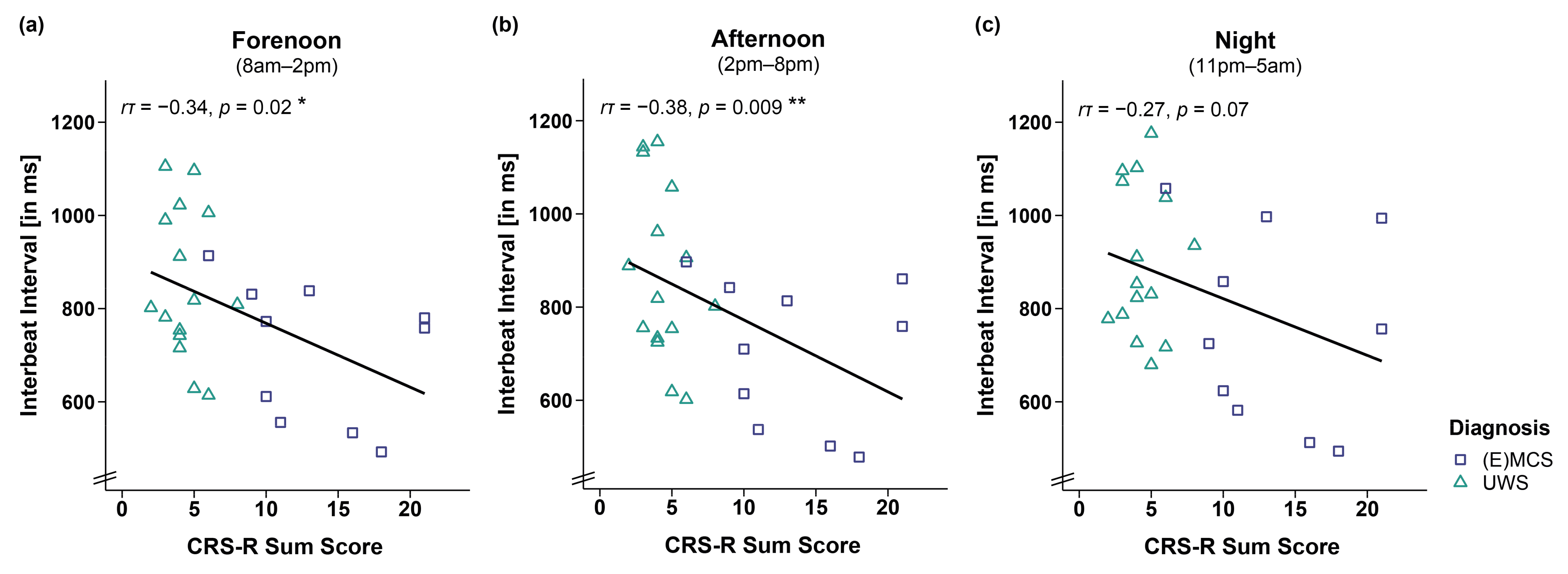
3.1. Interbeat Interval and Heart Rate
3.2. HRV Time Domain
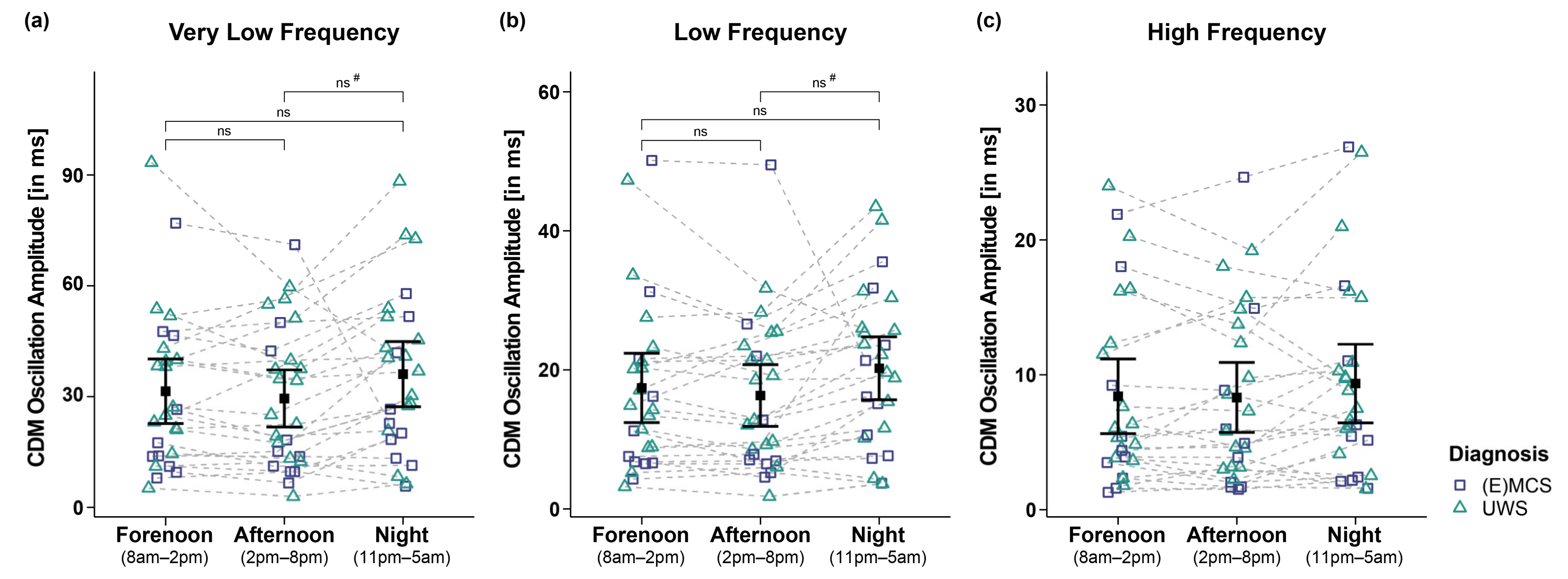
3.3. HRV Frequency Domain
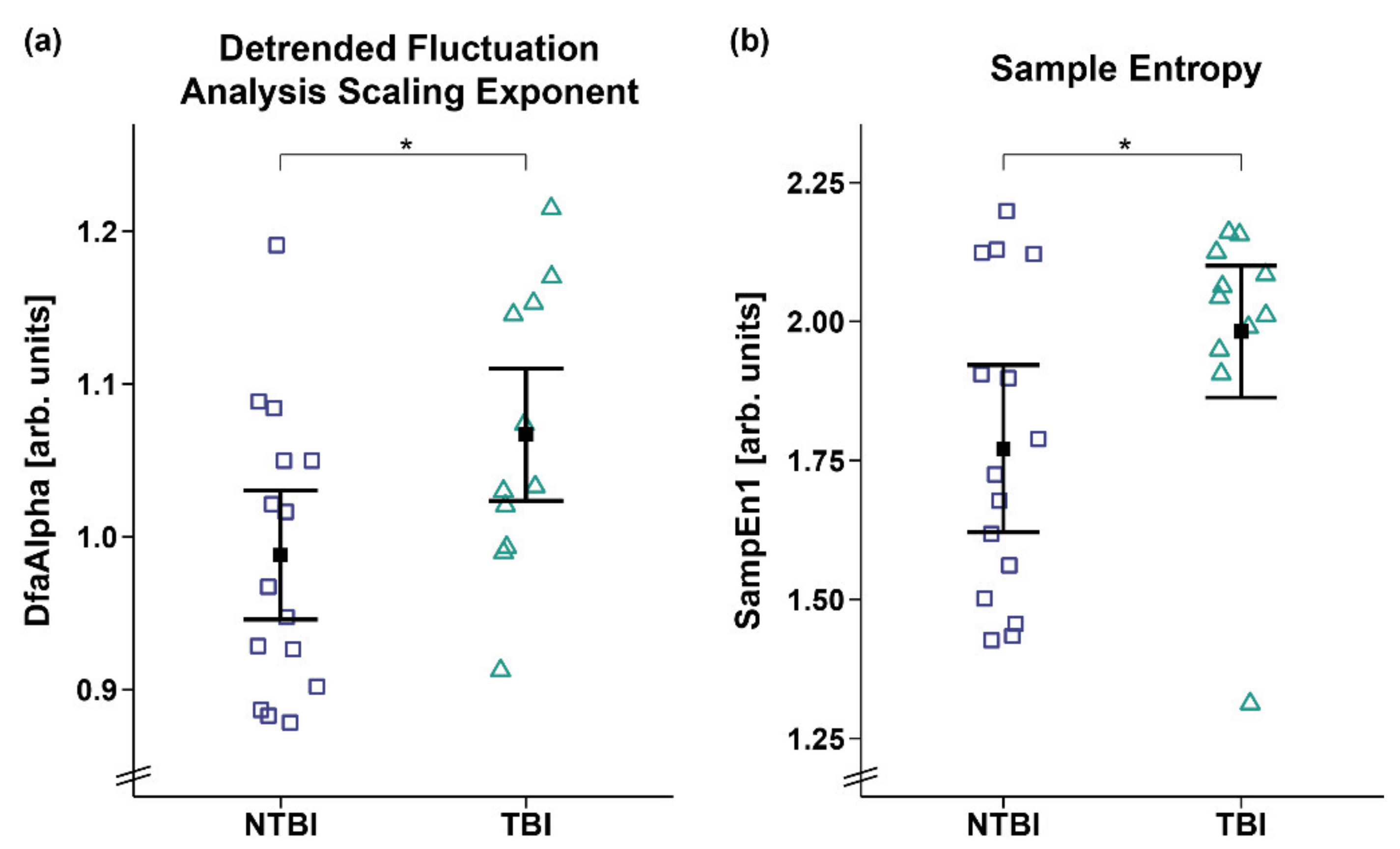
3.4. HRV Entropy Domain
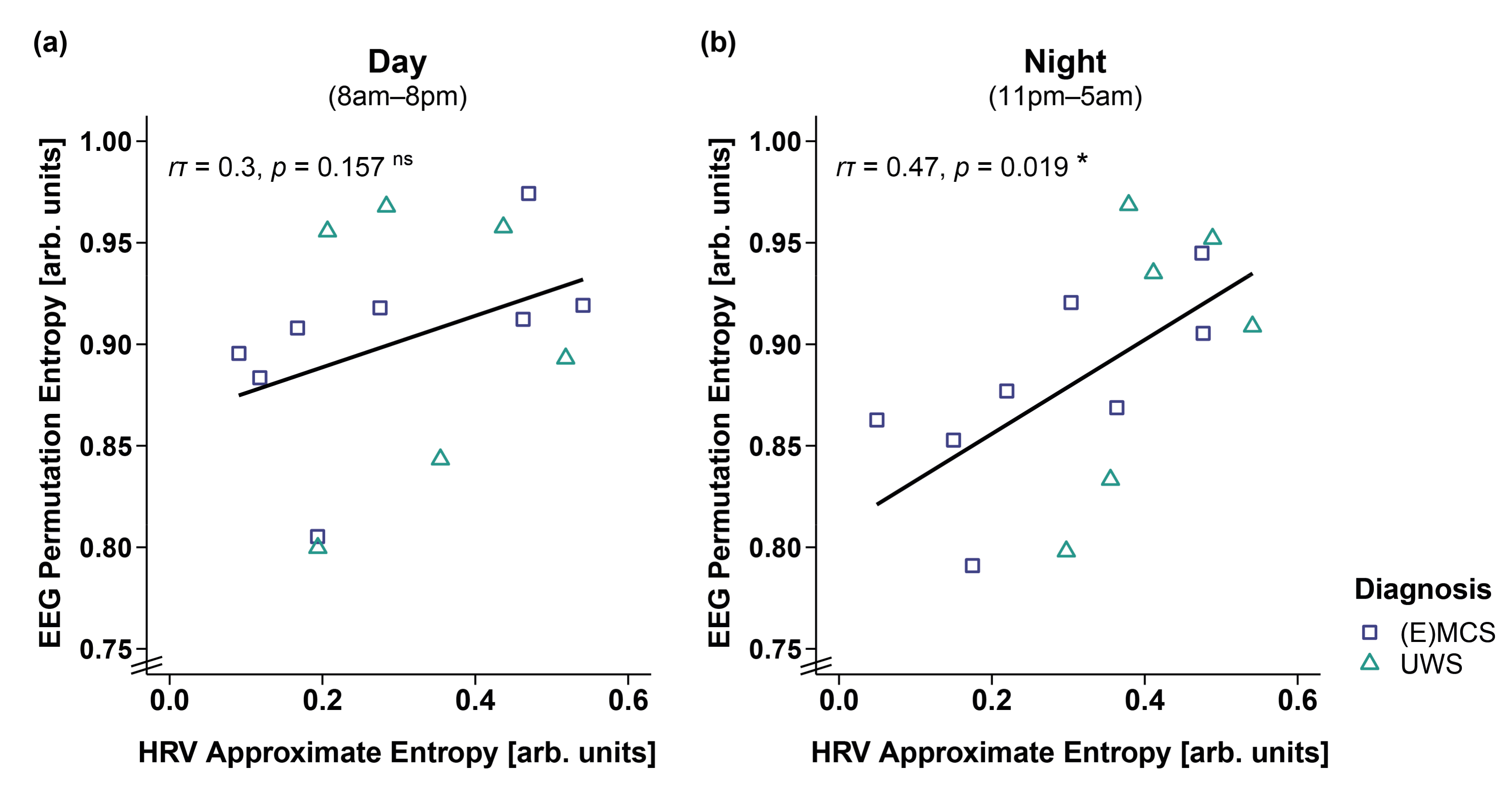
3.5. Correlation of EEG and HRV Entropy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANS | Autonomic nervous system |
| ApEn | Approximate entropy |
| BH | Benjamini–Hochberg correction for multiple comparisons |
| CDM | Complex demodulation |
| CI | Credibility interval |
| Cpm | Cycles per minute |
| CRS-R | Coma Recovery Scale-Revised |
| DDL | Dynamic daylight |
| DfaAlpha | Detrended fluctuation analysis scaling exponent |
| DOC | Disorders of consciousness |
| ECG | Electrocardiography |
| EEG | Electroencephalography |
| EMCS | Emergence from minimally conscious state |
| EMG | Electromyography |
| EOG | Electrooculography |
| fMRI | Functional magnetic resonance imaging |
| HF | High frequencies (0.15–0.4 Hz) |
| HL | Habitual light |
| HR | Heart rate |
| HRV | Heart rate variability |
| Hurst | Hurst exponent |
| IBI | Interbeat interval |
| LF | Low frequencies (0.04–0.15 Hz) |
| LF/HF ratio | Ratio between low and high frequencies |
| MCS | Minimally conscious state |
| NTBI | Non-traumatic brain injury |
| PE | Permutation entropy |
| PSG | Polysomnography |
| RMSSD | Root mean square of successive differences between adjacent heartbeats |
| SampEn | Sample entropy |
| SDRR | Standard deviation of interbeat intervals |
| TBI | Traumatic brain injury |
| UWS | Unresponsive wakefulness syndrome |
| VLF | Very low frequencies (0.003–0.04 Hz) |
| WTS | Wald-type statistic |
References
- Laureys, S. The neural correlate of (un)awareness: Lessons from the vegetative state. Trends Cogn. Sci. 2005, 9, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; Leon-Carrion, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacino, J.T.; Malone, R. The vegetative and minimally conscious states. Handb. Clin. Neurol. 2008, 90, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Kalmar, K.; Giacino, J.T. The JFK Coma Recovery Scale—revised. Neuropsychol. Rehabil. 2005, 15, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Andrews, K.; Murphy, L.; Munday, R.; Littlewood, C. Misdiagnosis of the vegetative state: Retrospective study in a rehabilitation unit. Brit. Med. J. 1996, 313, 13–16. [Google Scholar] [CrossRef] [Green Version]
- Blume, C.; Angerer, M.; Raml, M.; del Giudice, R.; Santhi, N.; Pichler, G.; Kunz, A.B.; Scarpatetti, M.; Trinka, E.; Schabus, M. Healthier rhythm, healthier brain? Integrity of circadian melatonin and temperature rhythms relates to the clinical state of brain-injured patients. Eur. J. Neurol. 2019, 26, 1051–1059. [Google Scholar] [CrossRef] [Green Version]
- Schnakers, C.; Vanhaudenhuyse, A.; Giacino, J.; Ventura, M.; Boly, M.; Majerus, S.; Moonen, G.; Laureys, S. Diagnostic accuracy of the vegetative and minimally conscious state: Clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 2009, 9, 35. [Google Scholar] [CrossRef] [Green Version]
- Demertzi, A.; Antonopoulos, G.; Heine, L.; Voss, H.U.; Crone, J.S.; de Los Angeles, C.; Bahri, M.A.; Di Perri, C.; Vanhaudenhuyse, A.; Charland-Verville, V.; et al. Intrinsic functional connectivity differentiates minimally conscious from unresponsive patients. Brain 2015, 138, 2619–2631. [Google Scholar] [CrossRef] [Green Version]
- Stender, J.; Gosseries, O.; Bruno, M.A.; Charland-Verville, V.; Vanhaudenhuyse, A.; Demertzi, A.; Chatelle, C.; Thonnard, M.; Thibaut, A.; Heine, L.; et al. Diagnostic precision of PET imaging and functional MRI in disorders of consciousness: A clinical validation study. Lancet 2014, 384, 514–522. [Google Scholar] [CrossRef]
- Monti, M.M.; Vanhaudenhuyse, A.; Coleman, M.R.; Boly, M.; Pickard, J.D.; Tshibanda, L.; Owen, A.M.; Laureys, S. Willful Modulation of Brain Activity in Disorders of Consciousness. N. Engl. J. Med. 2010, 362, 579–589. [Google Scholar] [CrossRef] [Green Version]
- Riganello, F.; Larroque, S.K.; Bahri, M.A.; Heine, L.; Martial, C.; Carriere, M.; Charland-Verville, V.; Aubinet, C.; Vanhaudenhuyse, A.; Chatelle, C.; et al. A Heartbeat Away From Consciousness: Heart Rate Variability Entropy Can Discriminate Disorders of Consciousness and Is Correlated With Resting-State fMRI Brain Connectivity of the Central Autonomic Network. Front. Neurol. 2018, 9, 769. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-regulation, Adaptation, and Health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef]
- Gujjar, A.R.; Sathyaprabha, T.N.; Nagaraja, D.; Thennarasu, K.; Pradhan, N. Heart rate variability and outcome in acute severe stroke: Role of power spectral analysis. Neurocrit. Care 2004, 1, 347–353. [Google Scholar] [CrossRef]
- Rapenne, T.; Moreau, D.; Lenfant, F.; Vernet, M.; Boggio, V.; Cottin, Y.; Freysz, M. Could heart rate variability predict outcome in patients with severe head injury? A pilot study. J. Neurosurg. Anesthesiol. 2001, 13, 260–268. [Google Scholar] [CrossRef]
- Sara, M.; Sebastiano, F.; Sacco, S.; Pistoia, F.; Onorati, P.; Albertini, G.; Carolei, A. Heart rate non linear dynamics in patients with persistent vegetative state: A preliminary report. Brain Inj. 2008, 22, 33–37. [Google Scholar] [CrossRef]
- Leo, A.; Naro, A.; Cannavo, A.; Pisani, L.R.; Bruno, R.; Salviera, C.; Bramanti, P.; Calabro, R.S. Could autonomic system assessment be helpful in disorders of consciousness diagnosis? A neurophysiological study. Exp. Brain Res. 2016, 234, 2189–2199. [Google Scholar] [CrossRef]
- Garbarino, S.; Lanteri, P.; Feeling, N.R.; Jarczok, M.N.; Quintana, D.S.; Koenig, J.; Sannita, W.G. Circadian Rhythms, Sleep, and the Autonomic Nervous System. J. Psychophysiol. 2020, 34, 1–9. [Google Scholar] [CrossRef]
- Bilan, A.; Witczak, A.; Palusinski, R.; Myslinski, W.; Hanzlik, J. Circadian rhythm of spectral indices of heart rate variability in healthy subjects. J. Electrocardiol. 2005, 38, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Boudreau, P.; Yeh, W.H.; Dumont, G.A.; Boivin, D.B. A circadian rhythm in heart rate variability contributes to the increased cardiac sympathovagal response to awakening in the morning. Chronobiol. Int. 2012, 29, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.; Lechinger, J.; Santhi, N.; del Giudice, R.; Gnjezda, M.T.; Pichler, G.; Scarpatetti, M.; Donis, J.; Michitsch, G.; Schabus, M. Significance of circadian rhythms in severely brain-injured patients A clue to consciousness? Neurology 2017, 88, 1933–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angerer, M.; Schabus, M.; Raml, M.; Pichler, G.; Kunz, A.B.; Scarpatetti, M.; Trinka, E.; Blume, C. Actigraphy in brain-injured patients—A valid measurement for assessing circadian rhythms? BMC Med. 2020, 18, 1–10. [Google Scholar] [CrossRef]
- Riganello, F.; Napoletano, G.; Cortese, M.D.; Arcuri, F.; Solano, A.; Lucca, L.F.; Tonin, P.; Soddu, A. What impact can hospitalization environment produce on the ANS functioning in patients with Unresponsive Wakefulness Syndrome? —24-hour monitoring. Brain Inj. 2019, 33, 1347–1353. [Google Scholar] [CrossRef]
- Czeisler, C.A.; Gooley, J.J. Sleep and circadian rhythms in humans. Cold Spring Harb. Symp. Quant. Biol. 2007, 72, 579–597. [Google Scholar] [CrossRef] [Green Version]
- Voss, A.; Schulz, S.; Schroeder, R.; Baumert, M.; Caminal, P. Methods derived from nonlinear dynamics for analysing heart rate variability. Philos. Trans. Math. Phys. Eng. Sci. 2009, 367, 277–296. [Google Scholar] [CrossRef]
- Sheng, H.; Chen, Y.Q.; Qiu, T. On the robustness of Hurst estimators. IET Signal Process. 2011, 5, 209–225. [Google Scholar] [CrossRef]
- Wislowska, M.; Del Giudice, R.; Lechinger, J.; Wielek, T.; Heib, D.P.J.; Pitiot, A.; Pichler, G.; Michitsch, G.; Donis, J.; Schabus, M. Night and day variations of sleep in patients with disorders of consciousness. Sci. Rep. 2017, 7, 266. [Google Scholar] [CrossRef]
- Angerer, M.; Pichler, G.; Angerer, B.; Scarpatetti, M.; Schabus, M.; Blume, C. From Dawn to Dusk—Mimicking Natural Daylight Exposure Improves Circadian Rhythm Entrainment in Patients with Severe Brain Injury, Sleep 2022, In press. Available online: https://osf.io/vk2d6/ (accessed on 29 January 2022).
- Blechert, J.; Peyk, P.; Liedlgruber, M.; Wilhelm, F.H. ANSLAB: Integrated multichannel peripheral biosignal processing in psychophysiological science. Behav. Res. Methods 2016, 48, 1528–1545. [Google Scholar] [CrossRef]
- Berntson, G.G.; Stowell, J.R. ECG artifacts and heart period variability: Don’t miss a beat! Psychophysiology 1998, 35, 127–132. [Google Scholar] [CrossRef]
- Wilhelm, F.H.; Grossman, P.; Roth, W.T. Assessment of heart rate variability during alterations in stress: Complex demodulation vs. spectral analysis. Biomed. Sci. Instrum. 2005, 41, 346–351. [Google Scholar]
- Hayano, J.; Taylor, J.A.; Yamada, A.; Mukai, S.; Hori, R.; Asakawa, T.; Yokoyama, K.; Watanabe, Y.; Takata, K.; Fujinami, T. Continuous Assessment of Hemodynamic Control by Complex Demodulation of Cardiovascular Variability. Am. J. Physiol. 1993, 264, H1229–H1238. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015. [Google Scholar]
- Asehnoune, K.; Roquilly, A.; Cinotti, R. Respiratory Management in Patients with Severe Brain. Inj. Crit. Care 2018, 22, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Grossman, P.; Karemaker, J.; Wieling, W. Prediction of Tonic Parasympathetic Cardiac Control Using Respiratory Sinus Arrhythmia—The Need for Respiratory Control. Psychophysiology 1991, 28, 201–216. [Google Scholar] [CrossRef]
- Friedrich, S.; Konietschke, F.; Pauly, M. Resampling-Based Analysis of Multivariate Data and Repeated Measures Designs with the R Package MANOVA. RM. R J. 2019, 11, 380–400. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate—A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a World Beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Bürkner, P.C. brms: An R Package for Bayesian Multilevel Models Using Stan. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, B.; Gelman, A.; Hoffman, M.D.; Lee, D.; Goodrich, B.; Betancourt, M.; Riddell, A.; Guo, J.Q.; Li, P.; Riddell, A. Stan: A Probabilistic Programming Language. J. Stat. Softw. 2017, 76, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Cugini, P.; Curione, M.; Cammarota, C.; Bernardini, F.; Cipriani, D.; Rosa, R.D.; Francia, P.; Laurentis, T.D.; Marco, E.D.; Napoli, A.; et al. Is a Reduced Entropy in Heart Rate Variability an Early Finding of Silent Cardiac Neurovegetative Dysautonomia in Type 2 Diabetes Mellitus. J. Clin. Basic Cardiol. 2001, 4, 289–294. [Google Scholar]
- Byun, S.; Kim, A.Y.; Jang, E.H.; Kim, S.; Choi, K.W.; Yu, H.Y.; Jeon, H.J. Entropy analysis of heart rate variability and its application to recognize major depressive disorder: A pilot study. Technol. Health Care 2019, 27, S407–S424. [Google Scholar] [CrossRef] [Green Version]
- Lechinger, J.; Bothe, K.; Pichler, G.; Michitsch, G.; Donis, J.; Klimesch, W.; Schabus, M. CRS-R score in disorders of consciousness is strongly related to spectral EEG at rest. J. Neurol. 2013, 260, 2348–2356. [Google Scholar] [CrossRef]
- Batchinsky, A.L.; Cancio, L.C.; Salinas, J.; Kuusela, T.; Cooke, W.H.; Wang, J.J.; Boehme, M.; Convertino, V.A.; Holcomb, J.B. Prehospital loss of R-to-R interval complexity is associated with mortality in trauma patients. J.Trauma 2007, 63, 512–518. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Smielewski, P.; Czosnyka, M.; Ercole, A. Cerebrovascular Signal Complexity Six Hours after Intensive Care Unit Admission Correlates with Outcome after Severe Traumatic Brain Injury. J. Neurotrauma 2016, 33, 2011–2018. [Google Scholar] [CrossRef] [Green Version]
- Bagnato, S.; Boccagni, C.; Sant’Angelo, A.; Fingelkurts, A.A.; Fingelkurts, A.A.; Galardi, G. Longitudinal Assessment of Clinical Signs of Recovery in Patients with Unresponsive Wakefulness Syndrome after Traumatic or Nontraumatic Brain Injury. J. Neurotrauma 2017, 34, 535–539. [Google Scholar] [CrossRef]
- Luaute, J.; Maucort-Boulch, D.; Tell, L.; Quelard, F.; Sarraf, T.; Iwaz, J.; Boisson, D.; Fischer, C. Long-term outcomes of chronic minimally conscious and vegetative states. Neurology 2010, 75, 246–252. [Google Scholar] [CrossRef]
- Katz, D.I.; Polyak, M.; Coughlan, D.; Nichols, M.; Roche, A. Natural history of recovery from brain injury after prolonged disorders of consciousness: Outcome of patients admitted to inpatient rehabilitation with 1–4 year follow-up. Prog. Brain Res. 2009, 177, 73–88. [Google Scholar] [CrossRef]
- Echeverria, J.C.; Woolfson, M.S.; Crowe, J.A.; Hayes-Gill, B.R.; Croaker, G.D.; Vyas, H. Interpretation of heart rate variability via detrended fluctuation analysis and alphabeta filter. Chaos 2003, 13, 467–475. [Google Scholar] [CrossRef]
- Goldberger, A.L. Is the Normal Heartbeat Chaotic or Homeostatic. News Physiol. Sci. 1991, 6, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart C 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Age | Sex | Etiology | Time Since Injury (Months) | Diagnosis | CRS-R Sum Score |
|---|---|---|---|---|---|---|
| P1 | 64 | M | NTBI | 8.8 | UWS | 3 |
| P2 | 77 | M | NTBI | 15.7 | UWS | 3 |
| P3 | 35 | M | NTBI | 14.6 | UWS | 4 |
| P4 | 71 | M | NTBI | 20.7 | EMCS | 21 |
| P5 | 55 | F | NTBI | 23.8 | UWS | 4 |
| P6 | 59 | M | NTBI | 25.8 | UWS | 4 |
| P7 | 80 | M | TBI | 21.9 | MCS | 9 |
| P8 | 22 | F | NTBI | 48.3 | UWS | - |
| P9 | 48 | M | TBI | 7.7 | UWS | 5 |
| P10 | 76 | M | TBI | 3.5 | UWS | 4 |
| P11 | 70 | M | NTBI | 3.4 | UWS | 2 |
| P12 | 71 | F | TBI | 4.7 | UWS | 4 |
| P13 | 16 | F | TBI | 0.8 | MCS | 16 |
| P14 | 21 | M | TBI | 7.0 | UWS | 6 |
| P15 | 48 | M | NTBI | 1.4 | MCS | 18 |
| P16 | 66 | M | NTBI | 3.2 | MCS | 10 |
| P17 | 61 | M | NTBI | 2.0 | MCS | 10 |
| P18 | 36 | M | TBI | 6.0 | MCS | 6 |
| P19 | 74 | F | TBI | 0.5 | UWS | 3 |
| P20 | 31 | F | NTBI | 1.4 | MCS | 11 |
| P21 | 43 | F | TBI | 6.0 | MCS | 21 |
| P22 | 61 | F | NTBI | 0.9 | UWS | 6 |
| P23 | 37 | M | NTBI | 9.4 | UWS | 5 |
| P24 | 34 | M | NTBI | 240.0 | UWS | 8 |
| P25 | 32 | M | TBI | 6.1 | UWS | 5 |
| P26 | 20 | M | TBI | 36.0 | MCS | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angerer, M.; Wilhelm, F.H.; Liedlgruber, M.; Pichler, G.; Angerer, B.; Scarpatetti, M.; Blume, C.; Schabus, M. Does the Heart Fall Asleep?—Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness. Brain Sci. 2022, 12, 375. https://doi.org/10.3390/brainsci12030375
Angerer M, Wilhelm FH, Liedlgruber M, Pichler G, Angerer B, Scarpatetti M, Blume C, Schabus M. Does the Heart Fall Asleep?—Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness. Brain Sciences. 2022; 12(3):375. https://doi.org/10.3390/brainsci12030375
Chicago/Turabian StyleAngerer, Monika, Frank H. Wilhelm, Michael Liedlgruber, Gerald Pichler, Birgit Angerer, Monika Scarpatetti, Christine Blume, and Manuel Schabus. 2022. "Does the Heart Fall Asleep?—Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness" Brain Sciences 12, no. 3: 375. https://doi.org/10.3390/brainsci12030375