Introduction
Delirium is common in intensive care unit (ICU) patients. In Indian ICUs, the prevalence of delirium is 31-68%.1,2 It is associated with increased morbidity and mortality.3 There is some evidence that prophylactic antipsychotic medications reduce the incidence of delirium in high-risk surgical trauma ICU patients.4 This study examined the efficacy of risperidone in preventing delirium in patients admitted to a medical ICU.
Methods
Study design
This study is a parallel arm, double-blind, placebo-controlled, randomised trial.
Setting
The study was conducted in a 24-bed medical ICU of a tertiary-care hospital.
Participants
Consecutive adult patients admitted to the ICU, who were expected to stay for at least two days, were screened for inclusion. Exclusion criteria were anticipated survival <2 days, severe hemodynamic instability, drug overdose causing coma, prolonged QTc interval >450 msec, neurodegenerative disorders, prior delirium, dementia, alcohol dependence, use of antipsychotic drugs, pregnancy or breastfeeding, difficulty in assessment (e.g., serious auditory or visual disorders) using the Confusion Assessment Method for the ICU (CAM-ICU), known allergy to risperidone, liver failure and renal failure.
Randomisation
Eligible patients were randomly assigned in blocks of 4 using a computer-generated randomisation sequence with a 1:1 allocation ratio to oral/naso-enteral risperidone 1-mg twice daily or identical oral placebo for the duration of ICU stay or until delirium developed.
Blinding and allocation concealment
The study drugs were prepared by a pharmacist according to the randomisation sequence and stored in sequentially labelled containers, thereby concealing allocation. Patients, healthcare providers and investigators were blinded to the treatment.
Assessments
CAM-ICU, the validated diagnostic tool for delirium assessment in the ICU,5,6 was used in English or two local languages (Tamil, Hindi) as appropriate, by the primary investigator, to identify delirium. Patients were followed up for 28-days post-enrolment. The primary outcome was the incidence of delirium. Secondary outcomes included ventilator-free days (VFD),7 duration of ICU and hospital stay, mortality and adverse events due to risperidone. Factors predisposing to delirium, such as electrolyte imbalance and infection, were screened for and treated.
Sample size calculation
For this study, assuming an incidence of delirium of 70% in the control arm1 and a reduction in the incidence of delirium to 30% in the risperidone-treated arm, with 80% power and 95% confidence, a sample size of 46 was calculated. Continuous and categorical variables were compared between the treatment and control groups using mean (standard deviation, SD) or median (interquartile range, IQR) as appropriate. Student t-test and the Mann-Whitney U test were used for continuous variables. Categorical variables were analysed using frequencies and the chi-squared test. We used an intention-to-treat analysis. Statistical analysis was performed using SPSS version 16.0
Ethical considerations
The study was approved by the Institutional Review Board (IRB) and the institution’s ethics committee (IRB no.10226). We obtained written informed consent from the patient or the next of kin. This trial was registered at ISRCTN (ISRCTN17375500). The study was funded by an institutional research grant.
Results
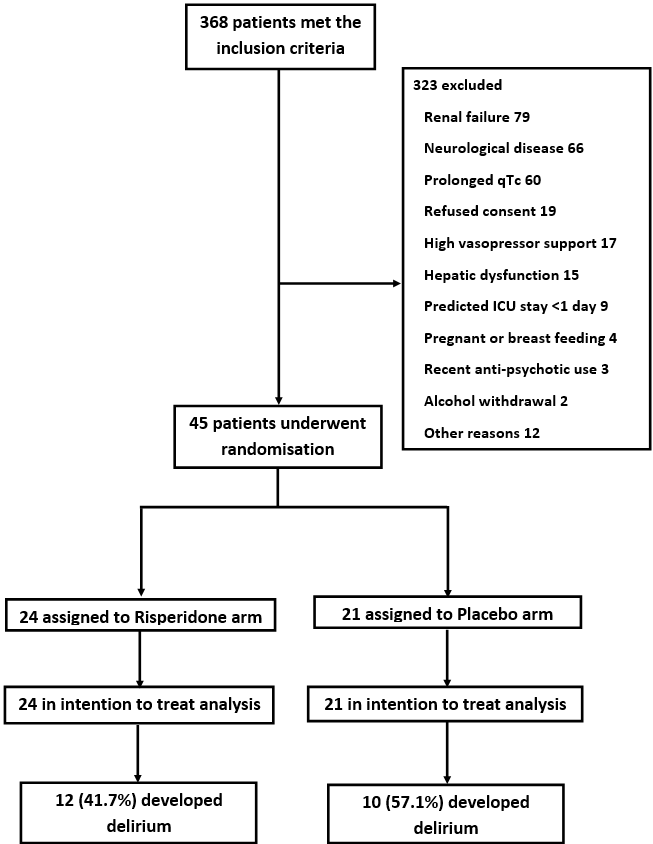
During the study period from February 2017 to October 2018, of the 368 patients screened, 304 were excluded. An additional 19 patients did not consent to participate (Figure 1). The mean (SD) age of the recruited patients (n=45) was 41.0 (17.3) years; 62% were men. Most were admitted due to an infection or poisoning; the APACHE-II score was 13.0 (5.8). Baseline characteristics were similar in both arms (Table 1).

The incidence of delirium was 49% (22/45). Of the 5 patients who died, 3 had documented delirium. The other two were intubated and too sedated to be assessed; they were considered to have developed delirium in the intention-to-treat analysis. The median time to onset of delirium was 1 day (IQR 1-2) from ICU admission, similar in both groups (p=0.65). The proportion of patients who developed delirium was lower in the risperidone group (42%) when compared with placebo (57%), though this was not statistically significant (p=0.3).
Overall mortality was 11% and similar in both groups (Table 1). There was no significant difference between the two groups with respect to VFD (p=0.93) or length of ICU (p=0.99), or hospital stay (p=0.1). The medication was discontinued in four patients. One patient in the control group developed neurological symptoms; in three patients, the treating physicians requested withdrawal from the study due to the worsening clinical condition.
Discussion
Delirium is a significant problem in the ICU. In this study, 49% of patients developed delirium at a median time of 1 day (IQR 1-2 days) following ICU admission. Compared with placebo, risperidone did not reduce the incidence of delirium in patients admitted to the medical ICU.
Previous small trials reported reduced delirium with antipsychotic prophylaxis in peri-operative and critically-ill surgical patients.4,8 However, a large randomised trial of 1789 patients that compared two doses of haloperidol (1-mg, 2-mg) with placebo in a mixed cohort of medical, surgical and trauma patients showed that haloperidol did not prevent delirium.9 A recent meta-analysis that examined the role of pharmacological prophylaxis for delirium in the ICU found insufficient evidence of benefit.10 However, the review noted that multiple trials were ongoing and a definite recommendation could not be made. Current guidelines provide the option for short-term use of haloperidol and atypical antipsychotic medications, along with non-pharmacological measures for delirium treatment and prevention.11
The lack of a consistent effect of pharmacological prophylaxis on the incidence of delirium in the current and previous studies is likely due to several factors. The early onset of delirium in our study (1 day) and another study,4 which reported a mean onset time of 1.4 days in the placebo arm, suggests insufficient time for the full efficacy of the drug. Likely, complex pathologies and multiple aetiologies of delirium and the heterogeneous nature of the disease makes it less likely for a single intervention to be effective across multiple aetiologies and subtypes of delirium (hypoactive, hyperactive). The study’s limitations were the small sample size and the exclusion of a large number of patients. Nevertheless, this study adds to the body of literature on the role of pharmacological prophylaxis for delirium in ICU patients.
A review of delirium in India showed that the prevalence of ICU delirium is between 16.1 and 68.2%.12 The majority of studies reported a hypoactive or a mixed delirium as the most common subtypes.12 Multiple scales including the ICDSC, MAS and CAM-ICU have been validated in Indian ICUs for the diagnosis of delirium.12 Patients with delirium were found to have longer ICU stays and a higher mortality rate.12 Studies assessing ICU clinicians showed that most did not routinely screen for delirium and underestimated its prevalence in ICUs.12 Although ICU staff were aware of some preventive practices such as early mobilization, many did not implement these for logistic reasons.12 The only study assessing the treatment of delirium in ICU showed that melatonin reduced the duration of delirium in ICU patients with organophosphate poisoning.12
Conclusion
Prophylactic use of risperidone did not reduce the incidence of delirium among patients admitted to the medical ICU. Further trials are required for a definitive recommendation.