1. Introduction
Osteonecrosis is a relatively common degenerative disease. It is characterized by the death of the cellular components of the subchondral bone due to ischemia, which can lead to devastating, progressive destruction of various joints.1–3 The most significantly affected joints are the hip, the knee, the shoulder, and the ankle; however, the disease can affect certain other small bones (e.g., metatarsal bone, semilunar bone, etc.).3
Firstly described by Ahlbäck in 1968, knee osteonecrosis is nowadays classified into three types: primary, spontaneous or idiopathic osteonecrosis (SONK), which appears in patients without any risk factors, secondary osteonecrosis (SON), which is associated with recognized, predisposing conditions such as steroid use, alcohol excess, obesity, chemotherapy, dialysis, organ transplantation and other general diseases (e.g., sickle cells anemia, systemic lupus erythematosus, liver disease, dysphoric disease, etc.), and post arthroscopy osteonecrosis, which arises as a result of chondral damage during knee arthroscopy.4–10
The incidence of knee SON is approximately 90% less than that of the hip.8 SON occurs predominantly among females and is typically associated with the epiphysis, the metaphysis, and the diaphysis of a particular condyle. Both femoral condyles can be affected. The lateral femoral condyle is associated with up to 60% of cases, either independently or with the medial femoral condyle.4 The tibia plateau may be affected in approximately 20% of cases; SON can have multiple localizations, and both knees are involved in 30–80% of cases.4 Multifocal osteonecrosis (MFON) is a disorder that affects three or more different anatomic sites simultaneously or in a series.3
Unlike spontaneous osteonecrosis, SON generally manifests in young people under 50 and presents particular anatomopathological, clinical, imaging, and progression features.7
The management of SON is limited by problems concerning the true etiology, the diagnostic tools (especially in the early phases), the effectiveness of the conservative treatment and the joint conservation surgery, as well as the choice of arthroplasty (e.g., uni-compartmental, total, stem use, etc.). In the early phase, its management is conservative. However, in the case of patients who would not benefit from such a therapy, surgical management is recommended.9–11
In light of these considerations, the main question is the choice of the appropriate treatment based on the patient characteristics and the phase of the disease. Therefore, this narrative review aims to evaluate the medical and surgical options for the treatment, focusing on the early stage of the disease. This is intended to avoid the progression of the degenerative condition with subchondral collapse and knee osteoarthritis, particularly among young people, which would require joint replacement.
2. Methods
PubMed/MEDLINE was searched between January 1, 2000, and December 31, 2020, using a combination of the following keywords: secondary osteonecrosis, knee, aetiopathogenesis, diagnosis, management, and treatment. The most recent and relevant studies investigating the diagnostic tools and therapeutic strategies for the management of SON were reviewed. In addition, a manual search was carried out to retrieve other articles which met the inclusion criteria that the initial search strategy had not identified. The non-English studies, those relating to spontaneous and post arthroscopy osteonecrosis, and reports concerning other joints were excluded from this narrative review.
3. Aetiopathogenesis
The etiopathology of knee SON is similar to that of the hip and shoulder.8 SON is related to several direct and indirect factors (Table 1), which may lead to the impairment of bone blood circulation. The actual pathogenesis, however, remains largely undefined.9–12 The possible mechanisms are the restriction or occlusion of the blood supply, direct tissue injury, and increased intraosseous pressure. Indirect factors include alcohol abuse, smoking, obesity, and corticosteroid use. Natural factors include hemopoietic disorders (e.g., sickle cell disease, etc.), myeloproliferative disease, Gaucher disease, dysbarism disorders, systemic lupus erythematosus, and other particulars diseases for which long-term corticosteroid treatment is prescribed.13–16 Corticosteroid use and alcohol excess are the two most significant risk factors in the case of SON.16
The exact mechanism of the pathogenesis is unclear.17–21 Recent research indicates that several factors (i.e., corticosteroids, alcohol, etc.) cause adipose cell enlargement in the bone marrow, leading to increased intra-osseous pressure, resulting in bone ischemia.14 Furthermore, other conditions associated with osteonecroses, such as myeloproliferative disorders and glycogen storage diseases like Gaucher’s, may be explained by this theory. Risk factors, such as cigarette abuse, coagulopathies, and sickle cell disease, may cause vaso-occlusive effects.13 In sickle cell disease, hemolytic anemia, the deformable red blood cell is more likely to bind to vascular walls, leading to vascular occlusion.18 In Caisson’s condition, the mechanism may be a direct vessel occlusion due to nitrogen gas emboli, directly correlated to the depth of dive, the amount of time under pressure, the rate of descent, and the inappropriate decompression procedure. A genetic predisposition towards osteonecrosis may be present, but no correlation has been found.3
4. Diagnosis
4.1. Clinical manifestation
In more than 60% of patients, the onset of symptoms is progressive, with moderate pain occurring under joint stresses (e.g., weight-bearing, etc.). The pain can be localized in the medial, lateral, or both condyles and may be exacerbated by palpation of the affected area.5
Typically, patients are young, can have bilateral knee pain, and, in some instances, a history of other joint dysfunction is present. With the progression of the disease, the knee symptoms are exacerbated and can include pain, swelling, and joint dysfunction. Knee deformity can also be present.
4.2. Imaging
The diagnosis is based on X-ray and magnetic resonance imaging (M.R.I.) examination.22–26 X-ray is helpful in the advanced stages and for the monitoring of disease progression, while M.R.I. is the method of choice for early-stage diagnosis.22–25
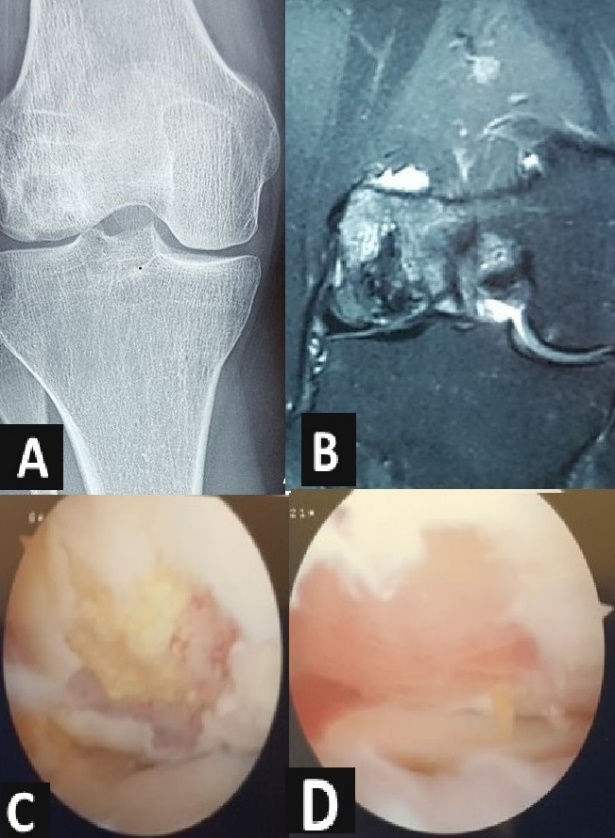
Imaging investigations enable the diagnosis of SON and identify the stage of the disease (Figures 1A and B). There are several classifications for osteonecrosis, initially for the more common osteonecrosis of the femoral head.22 The categories are based on the trabecular pattern, the shape of the particular area, the presence of subchondral collapse, and the joint space narrowing. One of the most used classifications for knee osteonecrosis is the Fiat and Arlet X-ray staging system, which divides knee osteonecrosis into four types: type I (normal appearance), type II (the presence of radiolucency surrounded by the sclerotic area, but the condyle still having a normal curvature), type III (the company of crescent sign with subchondral bone fractures and collapse), and type IV (the presence of failure and symptoms of degenerative, advanced osteoarthritis).3 However, it does not consider the size, location, and extension of the necrotic area, and there is excellent variability of intra- and interobserver interpretation.

M.R.I. is the gold standard of imaging in investigating and understanding the bone and soft tissue features of SON especially in the early stages. M.R.I. can present the characteristics of multiple foci of bone marrow oedema with the epiphysis and the diaphysis, which contrasts with SONK, where the lesion is confined to the epiphysis.26 Bone marrow oedema indicates an osseous perfusion disorder and can be related to an initial stage of osteonecrosis or a transient clinical condition not associated with osteonecrosis.
The disease-specific findings of SON are manifested by a central area, surrounded by a serpentine-like lesion, with a well-defined border of reactive bone; these findings have a low signal on T1-weighted images and a high signal T2-weighted, FS PD-FSE and STIR ideas.27 These features are significant for secondary osteonecrosis diagnosis.28 Moreover, M.R.I. detects cartilage lesions, the presence of loose bodies, and the associated intra-articular lesions (e.g., meniscal tear, etc.). M.R.I. can result in a negative diagnosis in too early a stage; the optimal time to perform an M.R.I. is between one and 3.5 months from the onset of knee symptoms.29
Bone scintigraphy has traditionally been the imaging modality of choice for investigating and staging SON, especially in the early stages of the disease.30 However, according to a study by Mont, in symptomatic cases of ON, bone scanning detected just 37 (64%) of the 53 lesions, while M.R.I. detected 100% of the lesions.8 In selected cases, computed tomography (C.T.) can be employed to confirm or exclude the presence of articular surface collapse, and it’s helpful for patients who cannot undergo MRI.30
5. Treatment options and clinical outcomes
In the literature, there are few reports regarding the management of SON, which is based on the clinical manifestations, the stage, the extension of the necrotic area, whether it is unilateral, bilateral, or multifocal, the grade of osteoarthritis, the age of the patient,
the level of activity, the general health, and one’s life expectancy.3,5,13
For the management of SON several conservative and surgical procedures have been proposed, with variable clinical outcomes.6 In a study by Boontanapibul et al., considering 164 knees with SON, the management was conservative in 57% of cases, and joint preservation surgery and total joint replacement were recommended in 20% and 23% of cases, respectively.6 Since SON. mainly affects young people, conservative management and joint-preserving treatments should be at the forefront of treatment options.31,32 Patients with advanced Stages 3 and 4 require surgical treatment (Table 2). A delay in diagnosis and treatment can lead to the collapse of the lesion, resulting in a joint disruption in the final stages.28
5.1. Nonsurgical Treatment
Conservative treatment is recommended at Stages 1 and 2 of osteonecrosis and in small lesions.31,32 Conservative treatment includes lifestyle modification, pharmacological therapy (analgesic, non-steroid anti-inflammatory drugs (NSAIDs), bisphosphonates, prostaglandin agents, etc.), physiotherapy (extracorporeal shockwave therapy and pulsed electromagnetic field therapy), and hyperbaric oxygen (HBO).33–38
Lifestyle modification includes protected weight-bearing and strength exercises for the quadriceps and gluteus.3 Analgesics and NSAIDs relieve the pain associated with avascular necrosis and maintain joint motility in the initial observational period. NSAIDs reduce swelling and inflammation in the soft tissues surrounding the joint.33
Bisphosphonates are a class of medication that includes alendronate, ibandronate, and others widely used in clinical practice to treat osteoporosis and osteolysis in cases of bone tumors. Bisphosphonates promote the reconstruction of subchondral fractures and the prevention of further aggravation, resulting in improving symptoms and imaging appearance.34,35
Iloprots (PGI2) is a vasoactive prostaglandin analogue drug that is generally used to treat peripheral angiopathy, pulmonary hypertension, and organ transplantation. In addition, it is employed in managing bone marrow oedema and in the early stage of avascular osteonecrosis, involving different localizations in the body.36 Iloprost caused vasodilatation and increased blood flow, which facilitates microcirculation. Nevertheless, the short-term outcome is promising. Claßen shares the results of 136 avascular osteonecroses of different joints in 108 patients treated with iloprost, with 74.8% reporting significant subjective improvement without irreversible side effects.36 Total total joint arthroplasty was needed in 71% of grade 3 patients and 100% osteonecrosis grade 4 patients.
Several studies have shown the positive effect of biophysical stimulation on the proliferation of cells, the development of extracellular matrix (E.C.M.), the apoptosis of chondrocytes, and the control of inflammatory cytokines.37,38 Marcheggiani Muccioli found that pulsed electromagnetic field stimulation substantially decreased knee pain and the necrosis region during the first six months, maintaining 86% of knees from prosthetic surgery at the 24-month follow-up.38
HBO therapy is used to increase tissue oxygenation and perfusion of the ischaemic area.39–42 Aseptic bone necrosis is approved as a recommendation for hyperbaric treatment by the Undersea and Hyperbaric Medical Society.43 In the early stages of SONK, a systematic review showed that HBO could improve the clinical treatment effect in patients with femoral head necrosis.42 Bosco presented good results after 30 sessions in patients with condylar femoral necrosis.41
In the literature, there are no randomized trials that confirm the efficacy of conservative therapy in the management of SON Furthermore, certain studies concern all types of osteonecrosis or only the more common SONK, and only a limited number of studies have an adequate number of patients and have found long-term follow-ups to be conclusive. Boontanapibul reported that in around 80% of patients who underwent conservative treatment methods, SON had progressed to advanced stages, requiring surgical intervention.6
5.2. Joint Preservation Surgery
Surgical treatment is a challenge, owing to the young age of patients affected by SON.44 Since SON progresses to end-stage disease, early surgical procedure is recommended.45,46 Joint preservation surgery is generally indicated for symptomatic patients after the failure of conservative treatment and in the absence of joint collapse (Figures 1C and D). In select young patients with a small lesion, knee arthroplasty must be avoided even in the post-collapse phase.3 The results of surgical treatment are summarized in Table 3.
Joint preservation surgery can be performed using arthroscopy, an open approach or a percutaneous technique under fluoroscopic control. Joint preservation surgery includes debridement, drilling, microfractures, core decompression, bone grafting, osteochondral autologous transplantation or allograft, autologous chondrocyte implantation, and the employment of mesenchymal stem cell (M.S.C.) with possible use of the scaffold.
Arthroscopy is indicated in the early phase of the disease. The main arthroscopic procedures are debridement, loose body removal, meniscal and chondral treatment, and the employment of marrow stimulation techniques (i.e., Pridie drilling, microfractures, abrasion arthroplasty).
Bone marrow stimulation procedures are subchondral perforation techniques aimed at releasing the marrow components such as mesenchymal stem cells (M.S.C.), growth factors, and other healing proteins to perform a super-clot that will create an enriched environment for fibrocartilage repair and new tissue development.47 The procedure of subchondral drilling with microfractures is safe, simple, cost-effective, and maybe a viable alternative for treating early-stage SON in young patients before joint arthroplasty. Akgun reported an improvement in the Lysholm score from 41 to 75 at a 37-month follow-up of 15 patients affected by SON, with average defects’ size of 3.6 cm2 treated by debridement and microfractures.47 The limit of microfractures in the extension of the diseases (i.e., depth, diameter, etc.); however, in exceptional cases, the Pridie drilling can be employed to reach the deep localisations better. Moreover, after bone marrow stimulation, implanting a scaffold can help regenerate bone and cartilage; in literature studies, the combination of microfractures and scaffold augmentation for osteochondral repair is a single-stage modality that is related to better outcomes compared with microfractures alone.
Core decompression can be successfully employed in knee osteonecrosis in the pre-collapse phase. Core decompression aims to remove the necrotic area, reduce the interosseous pressure, and restore adequate circulation in the affected bone; this can delay the need for total knee arthroplasty (T.K.A.). In a systematic review among patients in the pre-collapse phase, core decompression effectively treated small osteonecrosis lesions and avoided further surgical operation, with a failure rate of 10.4%.44 Small lesions have better results. Marulanda, who studied 61 knees with SON., reported, at a three years follow-up, positive results after using a decompression technique (small, multiple, percutaneous 3 mm drilling under fluoroscopic guidance) in 24 knees with small lesions, and in 86% of the 37 remaining knees with extensive lesions.48
Core decompression can be associated with refilling the drill hole and the defect area with a bone substitute, auto-or allograft, or osteochondral transplantation. Bone grafting procedures effectively treat patients affected by SON, with and without knee joint collapse.49 In some instances, especially among obese patients, core decompression of the femoral condyle by precise drilling while remaining extra-articular is a challenge.48
Osteochondral transplantation has the advantage of repairing both hyaline cartilage and subchondral bone and can even be used in the post-collapse phase.50 The limit is the extension of the lesion; in the case of small lesions, this can be used in both the pre-collapse and post-collapse stages.57 Autologous and osteochondral allografts can reduce the need for additional surgery. In literature studies, autologous transplantation prevents joint arthroplasty in young patients with SON. of the knee for at least the first decade.44 Matsusue reported good results in 94.3% of 25 patients affected by SONK and SON. treated with osteochondral autologous transplantation at the 42-month follow-up.45
The limit of autologous osteochondral transplantation is the size of the defect. Autologous chondrocyte implantation and M.S.C., combined with the scaffold, can be employed for large lesions.
Even with significant cartilage defects, two-stage autologous chondrocyte transplantation is an effective and safe treatment option.58 In patients with an associated bone defect, the use of bone grafting or matrix-induced chondrocyte transplantation can benefit sizeable osteochondral reconstruction. The limit of this technique is the need to use a two-stage procedure. Minas described the sandwich technique for patients with deep osteochondral lesions and avascular necrosis.58 This procedure consists of the employment of autologous chondrocyte implantation, in addition to autologous bone grafting. He reported better results using the sandwich technique than only a bone graft in patients with osteochondral lesions (87% vs. 54% at the five-year follow-up). In 21 cases of osteonecrosis, secondary to steroid use and treated with matrix-induced, autologous, chondrocyte implantation in the knee, Aydin reported an improvement of the International Cartilage Repair Society (ICRS) score from 28.33 at the preoperative stage to 70.88 at the mean follow-up of 72.4 months. In the 18 cases of osteochondritis dissecans, on the other hand, the result improved from 29.75 to 87.58.46
In combination with tissue engineering therapy, cell therapy and stem cell research play an important role in regenerative medicine.51,59 Certain studies suggest that M.S.C. represents a safe treatment for numerous degenerative diseases.60 M.S.C. can be bone marrow-derived or adipose tissue-derived and rarely obtained from other sources. S.O.N. can be treated by an intralesional injection or an MSC-impregnated scaffold. The precise localization of the injection can be administered under direct visualization or ample scope control to restore the structure of the necrotic bone. Kouroupis reported on the case of an 18-year-old female who was affected by ON secondary to systemic lupus erythematosus (S.L.E.) and received successful treatment on both knees under ultrasound guidance, with serial, local, direct injections of autologous bone marrow aspiration concentrate (BMAC), obtained from the posterior-superior iliac crest.61 In a prospective, randomized, and controlled clinical trial, carried out on 60 knees of 30 patients affected by bilateral SON and treated with T.K.A. in 30 knees and a subchondral injection of bone marrow concentrate in the contralateral knee, Hernigou reported similar positive results, with fewer complications and quick recovery after a subchondral M.S.C. injection.16
M.S.C. represents the future of SON management, but as for all joint conservative surgery, clinical trials are needed to confirm the effectiveness of this treatment for secondary osteonecrosis.
5.3. Joint Arthroplasty
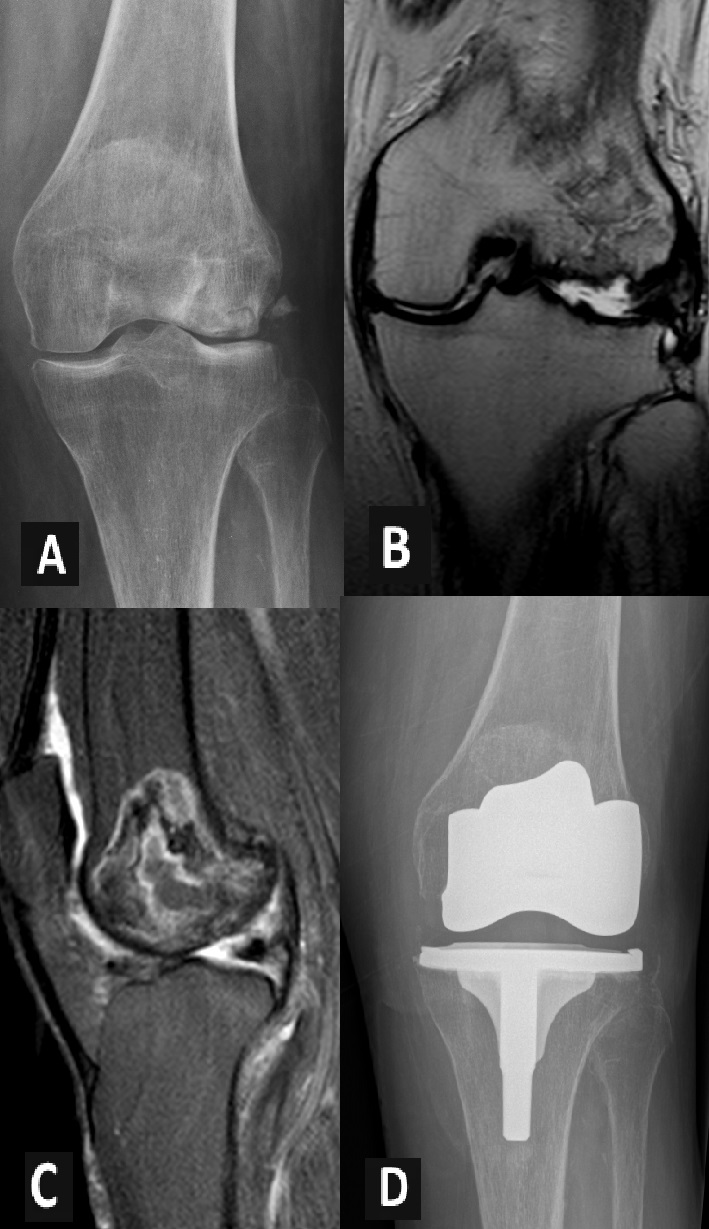
Joint arthroplasty is generally recommended in cases of phase three large lesions covering more than 50% of the common, and in phase 4, with progressive degenerative change and mutual destruction (Figure 2). The choice of appropriate arthroplasty is based on local and general conditions.54–56,62–64

Uni-compartmental arthroplasty is a successful treatment of SONK. However, unlike spontaneous osteonecrosis, SON can involve epiphysis and diaphysis, and most of the cases have bicondylar involvement. For this reason, high tibial osteotomy and unicompartmental arthroplasty have certain limitations.62,63 The dates in the literature are controversial and, in selected cases when the lesion is located only in one compartment, unicompartmental knee arthroplasty should be considered. Ollivier found no survival rate difference between primary and secondary osteonecrosis in 28 patients (primary in 19 knees and secondary in 10 knees) who underwent unicompartmental knee arthroplasty at the 26-year follow-up.53 Yang presents a case study of a 54-year-old woman who had a SON. of the lateral femoral condyle successfully treated with fixed-bearing, lateral, unicompartmental knee arthroplasty.65 Conversely, Chalmers found that unicompartmental arthroplasty for S.O.N. was less durable at the middle-term follow-up.52
The treatment of choice for advanced-stage osteonecrosis is cemented total knee replacement, which restores joint anatomy, relieves symptoms, and has good long-term outcomes.54,56 To maximize prosthesis stability, early diagnoses, strict indications, and effective surgical techniques are essential.55,66 In a literature review, Myers66 found that T.K.A. for SONK was associated with a better outcome than T.K.A. for SON. and U.K.A. for SONK. However, Chalmers recently reported a 93% survival rate for any revision at the 10-year follow-up in 167 primary T.K.A.s for SONK and S.O.N., with no risk factors related to S.O.N. present in 57 cases.55
In cases of extended lesions, the use of a stem is recommended to guarantee good stability; moreover, based on the extension of the lesions and the local and general features of the patient, specific authors suggested considering the use of stem in combination with a wedge or hinged arthroplasty.63,64 Recently, Boontanapibul reported an implant survival rate of 92%, with a significant improvement of symptoms at the 72-month follow-up in 32 cemented T.K.A.s among patients treated for S.O.N., with a mean age of 43 years; stem extension was used in 8% of cases and constraint implants in 3% of cases.56
6. Conclusions
SON is a rare disease with specific characteristics (Table 4). It affects young people and may evolve to complete joint destruction. Therefore, early diagnosis and treatment are crucial for reconstructing the subchondral bone and preserving the native articular cartilage until it collapses. The choice of appropriate therapy is based on the phase of the disease, the clinical manifestation, and the imaging appearance (i.e., extension, diameter, localization, etc.).
The management of SON. aims to avoid the progression of the disease and the onset of severe knee osteoarthritis. The treatment in the early phase is conservative, with pharmacological therapy, lifestyle modification, and physiotherapy. The surgical management in the pre-collapse and selected post-collapse of small lesions consist of joint preservation with arthroscopic perforation, osteochondral graft, regenerative surgery with the employment of scaffold, and M.S.C. The limitations of our narrative review include the fact that there are only a limited number of available studies, each with a small number of cases, regarding the management of the early phase of the disease; clinical trials are needed to confirm the effectiveness of a particular treatment. In the case of disease progression with the possible involvement of epiphysis, metaphysis, and diaphysis, the final treatment is total knee replacement.
Acknowledgments
The authors gratefully thank Adam Agha Kline for the language assistance and manuscript proofreading during the conduction of this study.
Author Contributions
Conceptualization, H.Z. and I.A.; methodology, H.Z.; software, M.M.; validation, V.D.G.; resources, H.Z. and M.M.; data curation, R.G.; writing—original draft preparation, I. A and R.G..; writing—review and editing, H.Z. and V.D.G.; supervision, V.D.G.
All authors have read and agreed to the published version of the manuscript.
Funding
There was no funding source for the manuscript.
Conflicts of Interest
The authors declared no conflict of interest.