

Abstract
Objective. To analyze the prevalence, associations, and fine specificity of autoantibodies to primary biliary cirrhosis (PBC)-associated antigens (MIT3, Sp100, and gp210) in a cohort of Italian patients with systemic sclerosis (SSc).
Methods. Sera samples from 201 patients with SSc were tested for antibodies to MIT3, gp210, and Sp100 by ELISA (the PBC screen). Anti-MIT3-positive sera were studied for IgG or IgA isotypes. All sera were analyzed by indirect immunofluorescence on HEp-2 cells and on rodent kidney/stomach/liver tissue sections in order to detect antinuclear and antimitochondrial antibodies (AMA). SSc was selected by American College of Rheumatology criteria and classified based on LeRoy’s criteria.
Results. Forty-three (21.4%) sera samples were positive for PBC screen antibodies. Anti-MIT3 antibodies were detected in 36 samples, anti-Sp100 in 5, and anti-gp210 in 1 sample. The other 3 PBC screen-positive samples showed no specificity for the single antigens. PBC screen-positive patients more frequently showed a limited cutaneous SSc subtype (p = 0.04), anticentromere antibodies (ACA; p = 0.0013), elevated alkaline phosphatase (ALP) (p < 0.0001), PBC (p = 0.002), and AMA (p = 0.008). Teleangiectasia and calcinosis were less frequent in this group of patients. IgG+IgA anti-MIT3-positive patients had higher prevalence of AMA (p = 0.0035), diagnosis of PBC (p = 0.014), and increased ALP (p = 0.039), all considered biochemical markers of severe liver disease.
Conclusion. PBC screen antibodies were detected in 20% of patients with SSc, strongly associated with ACA. ACA+/PBC screen+ patients had higher risk of developing PBC or elevation of ALP.
- PRIMARY BILIARY CIRRHOSIS
- SYSTEMIC SCLEROSIS
- ANTICENTROMERE
- ANTIMITOCHONDRIAL ANTIBODIES
- ALKALINE PHOSPHATASE
Primary biliary cirrhosis (PBC) is a chronic autoimmune cholestatic liver disease, characterized by slow and indolent progression to liver failure. It can frequently be associated with autoimmune diseases such as Sjögren’s syndrome, autoimmune thyroiditis, and systemic sclerosis (SSc). It has been reported that 2%–3% of cases of SSc have coexisting PBC1,2,3. The serological hallmark of PBC is presence of antimitochondrial antibodies (AMA), detected in about 90% of cases, occurring long before clinical onset of the disease4,5. Nevertheless, AMA do not predict the severity of PBC or any clinical subset of disease6. Antibodies to multiple nuclear dots, including promyelocytic leukemia and Sp100 antigens7, and antibodies recognizing different peptides of nuclear pore complex, such as gp210 or p62, are also currently considered serological markers of the disease8,9 associated with severe prognosis8,9,10,11. Recently, an ELISA has been developed to detect AMA using a combination of 3 mitochondrial antigens: MIT3 (pyruvate dehydrogenase complex, branched chain oxo-acid dehydrogenase complex, and oxo-acid glutarate dehydronase complex), anti-Sp100, and anti-gp21012. The combination of anti-MIT3 and anti-Sp100 has been shown to retain high sensitivity and specificity for a diagnosis of clinically evident PBC in SSc2. The aim of our study was to analyze the prevalence, clinical associations, and the isotype specificity of antibodies to MIT3, Sp100, and gp210 in a cohort of Italian patients with SSc. Considering the diagnosis of PBC as the “gold standard,” we assessed the sensitivity and specificity of anti-MIT3 antibodies.
MATERIALS AND METHODS
Patients
Among 440 consecutive patients with SSc followed at our institution (Rheumatology Unit, Brescia, Italy) since 1983, we analyzed clinical and laboratory data of 201 subjects whose sera were available for autoantibody analysis. All patients gave their informed consent for the study. More than 99% of patients were Caucasians of Italian ancestry. SSc was diagnosed according to the American College of Rheumatology criteria13 and classified according to the LeRoy criteria14 in order to define the different clinical subsets. Patients were routinely evaluated following the standard recommended guidelines15: active interstitial lung disease was diagnosed on high-resolution computer tomography and/or bronchoalveolar lavage findings; pulmonary arterial hypertension (PAH) was defined using Doppler echocardiography, performed at least yearly, as screening test and right heart catheterization as the gold standard, as recommended15. A total of 23 PBC cases were followed in our clinic. Among 201 patients considered in this report, a liver biopsy was performed in 8: a histological diagnosis of PBC was confirmed in 7 cases, and 1 case of hepatitis C virus-related cirrhosis was detected and not considered in the analysis. A diagnosis of PBC was made globally in 8 patients combining laboratory, immunological, and/or histological data according to the European Association for the Study of the Liver Clinical Practice Guidelines16: 6 cases with anti-PBC screen antibodies (histologically confirmed in 5) and 2 cases without anti-PBC screen antibodies. Patients with chronic hepatitis B or C viral infections were excluded. No case of autoimmune hepatitis was diagnosed. All the patients with a clinical/histological diagnosis of PBC were undergoing urso-deoxycholic acid (UDCA) treatment. The Mayo risk score was performed on individual subjects with PBC at time of liver disease diagnosis in order to determine their survival17 and the timing of liver transplantation18. Elevation of alkaline phosphatase (ALP; defined as a value 3-fold higher than normal values) was the best available marker of PBC activity in our cases, as collected from medical records19: elevation of ALP was defined when confirmed in more than 3 consecutive assessments during followup.
Methods
The available sera samples of 201 SSc patients were analyzed by indirect immunofluorescence (IIF) test on HEp-2 cells (Bio-Rad, Hercules, CA, USA) for antinuclear antibodies, including anticentromere (ACA), considered positive at a titer ≥ 1:80. Antiextractable nuclear antigen antibodies, namely those directed to topo-1, Ku, PM/Scl, U1RNP, Ro/SSA, La/SSB, Jo-1, Sm, PCNA, ribosomal P, and Ki/SL antigen, were tested by counterimmunoelectrophoresis, using rabbit thymus and human or porcine spleen extracts as substrates20,21,22. Anti-RNA polymerase III (RNAPIII) antibodies were tested with a commercial ELISA kit (Inova Diagnostics Inc., San Diego, CA, USA). Anti-Th/To antibodies were tested by RNA immunoprecipitation of K562 cell extract, with urea-PAGE and silver staining (Silver Stain Plus; Bio-Rad)23.
AMA were identified by IIF on rodent kidney/stomach/liver tissue sections using anti-human total immunoglobulin antibodies (Kallestad, Chaska, MN, USA), considered positive at titer > 1:20. All the 201 sera were analyzed by ELISA (QuantaLite™ PBC Screen IgG/IgA ELISA, Inova Diagnostics) for antibodies to MIT3, using goat anti-human IgA or anti-human IgG antibodies as secondary antibodies, anti-Sp100, and anti-gp210. All 201 sera were tested by ELISA using a mixture of MIT3, Sp100, and gp210 antigens, called the PBC screen. Positive sera were then tested on individual MIT3, Sp100, and gp210 antigens by ELISA.
Statistical analysis
All the variables were expressed as mean values and SD. The prevalence between groups was compared by Fisher exact test. Student’s t or Mann-Whitney U test was used for comparison of levels/values between groups. Statistical significance was accepted at p < 0.05.
RESULTS
Antibodies to at least 1 of MIT3, gp210, or Sp100 (PBC screen) were found in 21% (43/201) of sera. Anti-MIT3 antibodies were detected in 17.9% (36/201), anti-Sp100 antibodies in 2.5% (5/201: 3 cases as isolated specificity and 2 cases associated with anti-MIT3), and only 1 serum sample was positive for anti-gp210 (0.5%). The other 3 sera were positive for the PBC screen, but showed no specificity for individual antigens and were not included in the analysis.
Clinical data of 40 PBC screen-positive and 158 screen-negative patients are summarized in Table 1. Mean ages at SSc onset, followup, and mortality were similar between groups. The female:male ratio was 12:1 in the PBC screen-positive group compared to the negative group (5.8:1) but the difference was not statistically significant. A diagnosis of PBC was assessed globally in 8 patients: 6 were PBC screen-positive and 2 were PBC screen-negative cases. At the time of PBC diagnosis, patients in both groups showed a low and comparable Mayo risk score. No cases of liver decompensation were detected during followup. A limited cutaneous SSc variant was more common in PBC screen-positive (80%) compared to PBC screen-negative (63%) cases (p = 0.04); however, calcinosis was significantly less frequent (p = 0.012) in the PBC screen-positive group. Elevated ALP (p < 0.0001), PBC (p = 0.0024), and AMA by immunofluorescence (p = 0.008) were associated with the PBC screen-positive group.
Clinical and immunological data of 40 patients with SSc screened for PBC antibodies.
The most frequent SSc-related autoantibody in the PBC screen-positive group was ACA (55%), followed by anti-topo-I (20%). ACA showed a significantly higher prevalence in the PBC screen-positive group (p = 0.0013). Anti-U1RNP, anti-Ku, anti-Ro/SSA, and anti-RNAPIII antibodies were found in 1 case each.
Since ACA was twice as prevalent in the PBC screen-positive group compared to the screen-negative group, we examined only ACA-positive patients in order to determine whether this clinical association was due to a different prevalence of ACA (Table 2). The same trend was found (reduced telangiectasia and calcinosis; significant increase of ALP, PBC, and AMA), indicating that the association was not due to a different prevalence of ACA between the groups. In contrast, no differences were found between PBC screen-positive and negative subjects when anti-topo-I-positive patients were considered (data not shown). Indeed, PBC was found in 5 cases of ACA-positive/PBC screen-positive, in 1 case of PBC screen-positive, and in 2 cases without PBC screen or the other SSc-related autoantibodies.
Comparison of ACA+/PBC screen-positive (23 cases) and ACA+/PBC screen-negative (43 cases).
Distributions of PBC, prevalence of elevated ALP in SSc, and different SSc-related autoantibodies are illustrated in Table 3 and Figure 1. PBC screen antibodies were more prevalent in the ACA-positive group, compared with the anti-topo-I-positive group (p = 0.068), anti-RNAP III-positive group (p = 0.05), or other autoantiody-positive group (p = 0.036). The diagnosis of PBC was more frequent in the ACA-positive than the anti-topo-I-positive group (p = 0.028). Further, comparing ACA-positive/PBC screen-positive cases with other autoantibody-positive/PBC screen-positive cases, we found more frequent PBC [5/22 (22.7%) vs 1/18 (5.5%)] and PBC and/or ALP elevation [9/22 (40.9%) vs 3/18 (16.7%)] in the former group.
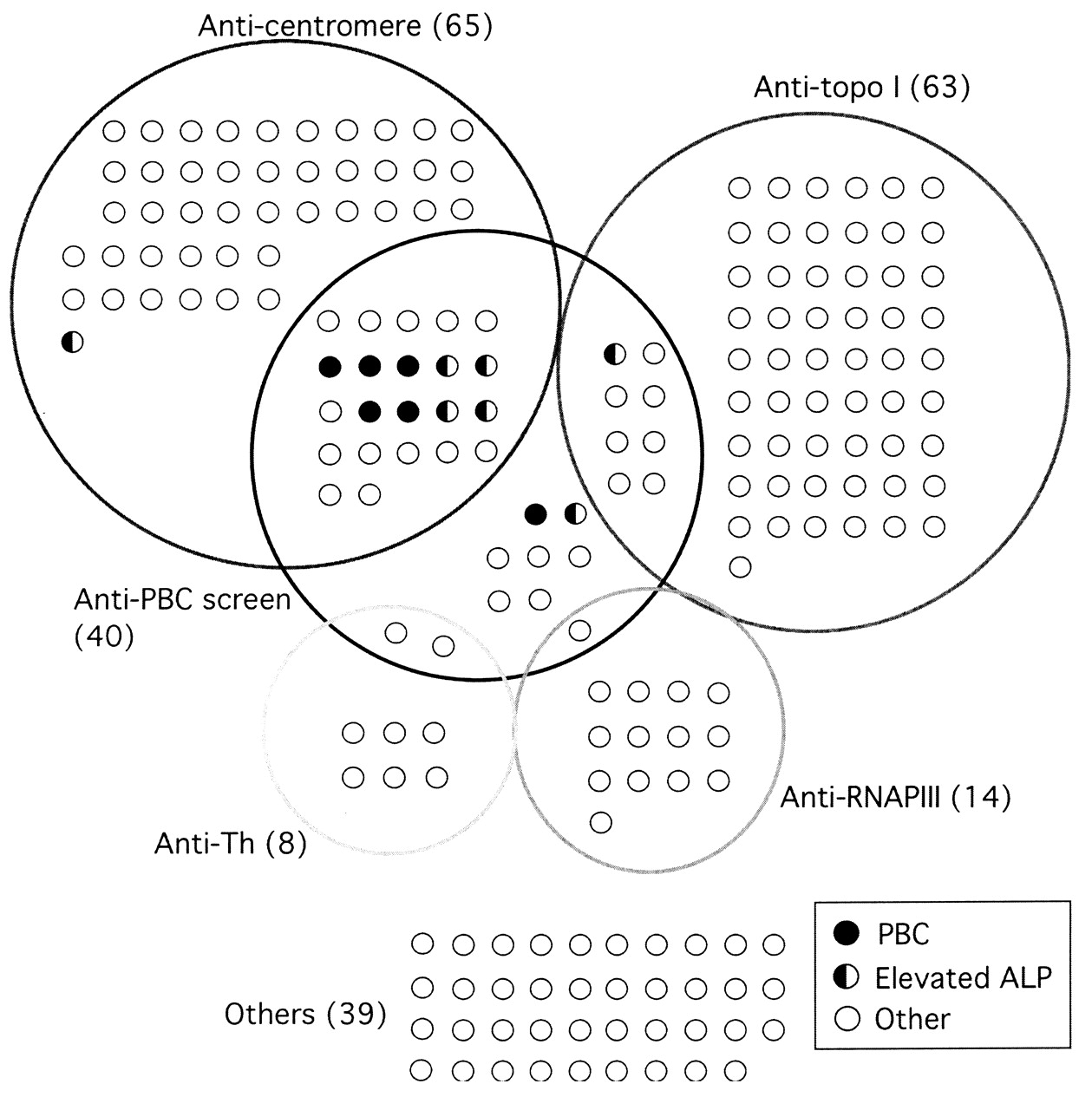
Distribution of primary biliary cirrhosis (PBC) and prevalence of elevated alkaline phosphatase (ALP) in SSc cases with different SSc-related autoantibodies in 201 patients with SSc.
PBC screening antibodies and PBC in different SSc-related autoantibodies.
The distribution of different anti-MIT3 isotypes is summarized in Figure 2: isolated IgG anti-MIT3 were found in 16/36 (44.5%) sera samples; isolated IgA anti-MIT3 in 12/36 (33.4%) samples, in 1 case associated with anti-Sp100 antibodies; and IgG+IgA anti-MIT3 in 8/36 (22.3%) samples, in 1 case with anti-Sp100 antibodies. Anti-Sp100 were found in 5 sera samples: in 3 as an isolated specificity; in 2 cases associated with IgG; and in IgG+IgA anti-MIT3 antibodies in 1 case each. Anti-gp210 antibodies were detected in 1 case.

Associations among primary biliary cirrhosis (PBC) and various anti-MIT3 isotype antibodies.
Clinical associations of different anti-MIT3 isotypes are shown in Table 4. Skin ulcers were observed more frequently in patients with isolated IgG anti-MIT3 compared with the IgA anti-MIT3-positive group (p = 0.026). PAH was frequently observed in IgG anti-MIT3-positive cases (31%) and in IgG+IgA anti-MIT3-positive cases (38%) compared with isolated IgA MIT3-positive (p = 0.024 and p = 0.048, respectively). No case of PAH was observed in IgA anti-MIT3-positive, thus this association is specific for IgG class anti-MIT3. The IgG+IgA anti-MIT3 group appeared to be most closely associated with clinical PBC: the IgG+IgA anti-MIT3-positive group showed a more frequent diagnosis of PBC (50%) and a more frequent elevation of serum ALP (62.5%) compared with other groups (p = 0.014 and p = 0.039, respectively). AMA were more frequently detected in IgG+IgA anti-MIT3-positive patients (62.5%) vs isolated IgA (0%) or IgG (13%; p = 0.005 and p = 0.0026, respectively). Within IgG+IgA anti-MIT3-positive patients, ALP elevation was found in 4/5 ACA-positive cases and 1/3 ACA-negative cases. Although diagnosis of PBC was more frequent in IgG+IgA anti-MIT3 cases, we did not observe higher IgM levels in this group, as expected (data not shown).
Clinical and laboratory features in 36 patients with positive SSc for anti-MIT3 antibodies.
Anti-MIT3 antibodies by ELISA showed an overall sensitivity and specificity of 75% and 85.4%, respectively, for the diagnosis of PBC, while AMA (by IIF) showed a lower sensitivity (62.5%) and a higher specificity (97.2%).
DISCUSSION
Autoantibodies can be produced in patients years before the clinical onset of disease, as described for anticitrullinated protein antibodies in rheumatoid arthritis or anti-dsDNA in systemic lupus erythematosus24,25. Similarly, AMA is considered a specific autoimmune marker of PBC, produced many years before clinical onset of disease4,5. However, no direct correlation between AMA and disease severity has been described to date. Although found more rarely, anti-Sp100 and anti-gp210 seem to carry a higher risk for more severe and aggressive PBC8,9,10,11. AMA are usually detected using the IIF test on rodent tissue extracts, while anti-Sp100 and anti-gp210 can be detected by line immunoassays on recombinant antigens26 or less readily available tests, such as immunoprecipitation on purified rat liver nuclear membrane as antigen source27. An ELISA with the 3 major antigens for AMA (namely, anti-MIT3), Sp100, and gp210 seemed to enhance the sensitivity and specificity for the diagnosis of isolated PBC28 or PBC-SSc overlap2. Nevertheless, the prognostic value of these autoantibodies detected by ELISA has not been established in PBC to date.
Anti-MIT3, anti-gp210, and Sp100 antibodies (the PBC screen) were found globally in 21.4% of our cohort of 201 unselected SSc cases, while anti-MIT3 antibodies were detected in 18% of cases. These autoantibodies have been described in SSc without clinical or biochemical signs of autoimmune liver disease28,29,30. Although the prevalence of PBC screen antibodies in our patients with SSc was similar to the prevalence reported by others2,29, a diagnosis of PBC was determined more frequently in our cohort. Indeed, PBC was diagnosed in 14% of PBC screen-positive patients and in only 1.3% of screen-negative patients (p = 0.0009). Among PBC screen antibodies, anti-MIT3 showed a high sensitivity (6/8; 75%) and specificity (85.4%) for the diagnosis of PBC, confirming previous reports2. By contrast, the occurrence of anti-Sp100 antibodies or anti-gp210 did not confer any additional value to anti-MIT3 for the diagnosis of PBC, probably because of the small number of positive sera samples in our cohort.
Analyzing the isotypes of anti-MIT3 antibodies, IgG+IgA anti-MIT3 showed a significant association with the diagnosis of PBC (p = 0.014) and AMA (p = 0.0035) compared with other groups. The occurrence of anti-MIT3 of the IgG and IgA isotypes, with no evidence of elevation of total circulating IgG or IgA levels, may be consistent with the immune system affinity maturation and class switching toward specific mitochondrial antigens rather than simple polyclonal B cell activation. Indeed, specific antipyruvate dehydrogenase complex IgA have been described in PBC, in circulation or localized in the apical surface and in the cytoplasm of biliary epithelial cells7. Moreover, AMA-IgA seems to possess a direct toxic effect on biliary epithelium31, contributing to the complex pathogenesis of bile duct damage in PBC7.
The occurrence of IgG+IgA anti-MIT3 antibodies was associated with persistent elevation of ALP in our series. High ALP value, along with increased bilirubin and reduced serum albumin, is considered a very sensitive indicator of disease severity, poor response to UDCA treatment, and progression to liver failure in PBC15,19,31,32. Some investigators have reported a significant association between ALP elevation and ACA or anti-topo-I antibodies, independent from AMA or anti-Sp100 status2. By contrast, presence of anti-RNAPIII antibodies was associated with lower ALP levels2. In our experience ALP elevation is associated with IgG+IgA anti-MIT3 antibodies, independent from ACA or anti-topo-I positivity.
Most of the AMA-positive sera samples (7/8) showed anti-MIT3 antibodies. Although time-consuming, the IIF assay using rodent tissue sections as substrate is considered the gold standard for detection of AMA33. This test showed a lower specificity and sensitivity compared with Western blot or ELISA tests34, with good performance when compared with the line immunoassay26.
The availability of fully automated ELISA testing could enhance investigation of various autoantibodies that are considered markers of PBC in routine laboratory analysis, avoiding the use of different assays with diversified antigen sources. In addition, given the specific association between PBC and IgG+IgA anti-MIT3, characterization of the isotype specificity could be helpful for more accurate assessment of patients. Further studies are needed to clarify the possible association between the development of PBC and the anti-MIT3 antibodies in IgG vs IgG+IgA classes.
- Accepted for publication June 9, 2011.








{kind=link}
{kind=link}