INTRODUCTION In inflammatory respiratory diseases, the imbalance between proteases and endogenous protease inhibitors leads to an exacerbated activity of human neutrophil elastase (a protease that destroys the extracellular matrix and stimulates proinflammatory cytokine release). Elastase is considered a target in the search for therapeutic treatments for inflammatory respiratory diseases. Pulmonary surfactant is a promising product for this purpose, because in addition to its biophysical function, it has anti-inflammatory properties.
OBJECTIVES Evaluate effect of the Cuban porcine pulmonary surfactant (Surfacen), the rCmPI-II elastase inhibitor, and the Surfacen/rCmPI-II combination on activated neutrophil elastase activity in vitro, and determine if Surfacen’s interface property changes in the presence of the inhibitor.
METHODS The anti-elastase effect of Surfacen, rCmPI-II and the Surfacen/rCmPI-II combination was evaluated in an in vitro model of activated neutrophils, previously purified from the blood of healthy subjects. The cells were stimulated with LPS/fMLP and were incubated with different concentrations of Surfacen, rCmPI-II and the Surfacen/rCmPI-II combination. Elastase activity was measured. The interface property was determined on a Langmuir surface balance.
The new index, called the abdominal adipose deposit index, was obtained by multiplying the subcutaneous fat thickness by visceral fat thickness, both measured by ultrasound. A cutoff point was established that facilitated discernment of an unhealthy phenotype: normal weight but metabolically obese, a cardiometabolic risk factor.
RESULTS Surfacen at 10 mg/mL inhibited 71% of stimulated neutrophil elastase activity. rCmPI-II at 0.1 μM reduced 20% of elastase activity; at 200 μM—the maximum concentration evaluated—inhibition was 68%. Both products had a dose-dependent effect. The Surfacen/inhibitor combination (0.5 mg/mL/80 µM) did not affect the surfactant interface property or the inhibitory activity of rCmPI-II against human neutrophil elastase.
CONCLUSIONS Surfacen and the rCmPI-II inhibitor have an anti-elastase effect on an activated neutrophil model. rCmPI-II does not affect Surfacen’s interface property and, therefore, both can be evaluated for combined use in treating inflammatory lung diseases.
KEYWORDS Pulmonary surfactants, elastase inhibitor, drug carriers, neutrophils, Cuba
ABSTRACT INTRODUCTION In inflammatory respiratory diseases, the imbalance between proteases and endogenous protease inhibitors leads to an exacerbated activity of human neutrophil elastase (a protease that destroys the extracellular matrix and stimulates proinflammatory cytokine release). Elastase is considered a target in the search for therapeutic treatments for inflammatory respiratory diseases. Pulmonary surfactant is a promising product for this purpose, because in addition to its biophysical function, it has anti-inflammatory properties.
OBJECTIVE Evaluate effect of the Cuban porcine pulmonary surfactant (Surfacen), the rCmPI-II elastase inhibitor, and the Surfacen/rCmPI-II combination on activated neutrophil elastase activity in vitro, and determine if Surfacen’s interface property changes in the presence of the inhibitor.
METHODS The anti-elastase effect of Surfacen, rCmPI-II and the Surfacen/rCmPI-II combination was evaluated in an in vitro model of activated neutrophils, previously purified from the blood of healthy subjects. The cells were stimulated with LPS/fMLP and were incubated with different concentrations of Surfacen, rCmPI-II and the Surfacen/rCmPI-II combination. Elastase activity was measured. The interface property was determined on a Langmuir surface balance.
RESULTS Surfacen at 10 mg/mL inhibited 71% of stimulated neutrophil elastase activity. rCmPI-II at 0.1 μM reduced 20% of elastase activity; at 200 μM—the maximum concentration evaluated—inhibition was 68%. Both products had a dose-dependent effect. The Surfacen/inhibitor combination (0.5 mg/mL/80 µM) did not affect the surfactant interface property or the inhibitory activity of rCmPI-II against human neutrophil elastase.
CONCLUSIONS Surfacen and the rCmPI-II inhibitor have an anti-elastase effect on an activated neutrophil model. rCmPI-II does not affect Surfacen’s interface property and, therefore, both can be evaluated for combined use in treating inflammatory lung diseases.
KEYWORDS Pulmonary surfactants, elastase inhibitor, drug carriers, neutrophils, Cuba
INTRODUCTION Endogenous pulmonary surfactant is a complex mixture of lipids and proteins. It is synthesized and secreted into the alveolar space by type II pneumocytes. Its main function is to reduce surface tension at the air–liquid interface in the alveolus, preventing alveolar collapse and reducing respiratory effort. Pulmonary surfactant is essential and its absence, deficiency or inactivation is associated with several pulmonary diseases, such as neonatal respiratory distress syndrome (NRDS, or hyaline membrane disease), acute respiratory distress syndrome (ARDS), meconium aspiration syndrome, asthma and chronic obstructive pulmonary disease.[1] In addition to improving pulmonary function and oxygenation, surfactant is a key modulator of innate and acquired pulmonary immunity.[2,3]
Natural exogenous surfactant preparations are quite safe and effective standard therapy in newborns with NRDS.[4] The preparations used in neonatology services come from bovine or porcine surfactant extracts. Surfactants for clinical use are obtained from bronchoalveolar lavage or from lung tissue. Hydrophobic lipid and protein fractions, which contain the surfactant’s main tensoactive components, are extracted using organic solvents, usually chloroform/methanol. Five surfactant preparations have been marketed by large pharmaceutical companies, all registered for use in NRDS: Curosurf (Chiesi Farmaceutici, Italy); Survanta (AbbVie, USA); BLES (BLES, Canada); Infasurf (ONY Biotech, USA), and Alveofact (Boehringer-Ingelheim, Germany).[5] Cuba also markets a registered surfactant preparation called Surfacen.[6] WHO includes these kinds of products on its Essential Medicines List.
IMPORTANCE Surfacen, rCmPI-II, and the Surfacen/rCmPI-II combination are shown to inhibit elastase in vitro in a stimulated neutrophil model, which supports research targeting its therapeutic application in inflammatory respiratory diseases.
Several respiratory diseases characterized by a strong inflammatory response involve an imbalance between proteolytic enzymes and their inhibitors. Neutrophils (and especially neutrophil elastase) are the main inflammatory mediators involved in acute alveolar injury and interstitial edema related to an increase in vascular permeability in ARDS.[7] In other chronic inflammatory lung conditions (cystic fibrosis, chronic obstructive pulmonary disease and bronchiectasis), abundant neutrophils are present in lung tissue. Excessive release of neutrophil elastase accelerates lung tissue damage, which causes a decrease in pulmonary function.[8]
Uncontrolled neutrophil elastase proteolytic activity is regulated by various endogenous protein inhibitors; however, this enzyme can evade this regulation using several pathways.[9] Recognizing neutrophil elastase as a therapeutic target in inflammatory lung diseases has led to discovery of new elastase inhibitors,[10‒12] now undergoing clinical studies.[13,14]
Recently, two surfactants in clinical use, Alveofact and Curosurf, were shown to inhibit formation of neutrophil extracellular traps (NETs) by decreasing elastase, myeloperoxidase and cell-free DNA (cfDNA) levels.[15]
Surfacen is a natural porcine surfactant, approved for use in Cuba in 1995 by the country’s regulatory agency, the Center for State Control of Medicines, Equipment and Medical Devices (CECMED) (health registration No. 0800).[6] It was introduced into medical practice in all neonatal intensive care units to treat hyaline membrane disease or NRDS in preterm infants.[16] Later, in 2011, Surfacen was approved for ARDS treatment in adults,[17] and in 2014, for ARDS in pediatric patients.[18] Surfacen is a safe product; no adverse reactions have been reported in any of the clinical trials conducted, and it has a safety profile similar to the other surfactants marketed internationally.[19] In the Cuban protocol for clinical management of patients with COVID-19 published in 2020, Surfacen is one of the medicines recommended for use.[20]
In addition to its biophysical function, Surfacen has an in vitro anti-inflammatory effect, decreasing tumor necrosis factor-alpha (TNF alpha) and interleukin 6 (IL-6),[21] and has shown an anti-inflammatory and anti-allergic immunomodulatory effect in an animal model of allergen-induced asthma.[22]
Pulmonary surfactant has been evaluated as a drug carrier or vehicle since the 1990s;[23] it has been used as a budesonide carrier in premature newborns at risk of developing bronchopulmonary dysplasia and is currently undergoing clinical trials.[24,25] Those studies provide the first clinical proof of concept for a surfactant-drug combination and justify research on its possible use in combination therapies with other drugs.
Given the importance of neutrophil elastase in respiratory diseases, the combination of Surfacen with inhibitors of this enzyme could lead to new therapeutic options for these diseases. CmPI-II, a Kazal-type serine protease inhibitor, is isolated from the Cenchritis muricatus marine snail. CmPI-II is a strong inhibitor of serine proteases, especially human neutrophil elastase.[26,27] The recombinant variant of this inhibitor (rCmPI-II) has functional and molecular characteristics similar to the natural inhibitor. Its ability to inhibit human neutrophil elastase has suggested important biomedical applications, including in inflammatory diseases.[28]
Very few in vitro and in vivo studies have been conducted on the combination of surfactants and protease inhibitors. Belai[29] demonstrated that use of Survanta pulmonary surfactant with alpha-1 antitrypsin had a positive effect on oxygenation and surfactant metabolism in surfactant-deficient rats. Cochrane[30] demonstrated that the combination of elafin and a surfactant in an animal model of lung damage decreased the lung damage.
The objective of this study was to evaluate the effect of Surfacen pulmonary surfactant, the rCmPI-II elastase inhibitor, and the Surfacen/rCmP-I-II combination on elastase activity in an in vitro model of activated neutrophils, as well as the surfactant’s interface property when combined with the inhibitor.
METHODS Evaluated products Surfacen Natural surfactant obtained from porcine pulmonary lavage. The final product is supplied as a sterile white lyophilized powder in a 6R vial containing 50 mg total phospholipids. Composition: phospholipids (95%), hydrophobic proteins (SP-B and SP-C, 1.5%) and other lipids (3.5%).[6,31] Surfacen is produced in the National Center for Animal and Plant Health (CENSA) in collaboration with the National Biopreparations Center (BIOCEN), both in Cuba. Each vial is reconstituted in 2 mL of water for injection, obtaining a phospholipid concentration of 25 mg/mL.
rCmPI-II Elastase inhibitor obtained at the University of Havana Biology Faculty’s Protein Studies Center (CEP) via recombinant pathway in Pichia pastoris yeast. Its characteristics are similar to those of the CmPI-II natural protein from the Cenchritis muricatus marine snail. The inhibitor concentration was determined by measuring absorbance at 280 nm using the coefficient of extinction ξ1%, 280 nm = 16.1, previously determined for the natural inhibitor. The concentration was 2 mg/mL. Molecular mass of rCmPI-II is 5485 Da.[32]
Human neutrophil purification from human blood Neutrophils were obtained from 10 mL of venous blood from healthy volunteers using Ficoll density gradient cell separation (Ficoll-Histopaque-10771, density: 1.077 g/mL, Sigma-Aldrich, USA).[33] First, blood was collected in EDTA tubes (Vacuette 4 mL K3EDTA, Greiner Bio-One, Germany) and centrifuged at 1500 rpm (DL6M centrifuge, Kaida, China) for 15 minutes at 20 ºC. Plasma was collected and centrifuged at 2500 rpm for 5 minutes at 20 ºC, to obtain a platelet-poor supernatant, which was remixed with the rest of the blood. After gravity sedimentation gradient was performed using Ficoll-Histopaque, plasma was collected and put through a second centrifugation gradient at 2500 rpm for 30 minutes at 20 ºC with Ficoll-Histopaque. To eliminate the remaining Ficoll, the precipitate obtained was resuspended in 5 mL of phosphate-buffered saline and centrifuged at 2500 rpm for 5 minutes at 20 ºC. Finally, the precipitate was collected and resuspended in 1 mL of pH 7.2 phosphate-buffered saline (PBS) solution supplemented with 0.1% bovine serum albumin (BSA, Sigma-Aldrich, USA). Purity of purified neutrophils (>95%) was determined in the MacsQuant 10 flow cytometer (Miltenyi, Germany) by fluorescence-activated cell sorting (FACS) using anti-CD45-FITC and anti-CD3-PE antibodies (Miltenyi, Germany).
Neutrophil activation assay Purified neutrophils were adjusted to a concentration of 1×107 cells per mL in PBS solution supplemented with 0.1% BSA (Sigma-Aldrich, USA). Then, 100 mL of the neutrophil suspension was activated for 10 minutes through incubation with 10 mL of cytochalasin B from Drechslera (Sigma-Aldrich, USA) at a final assay concentration of 5 μg/mL, and then stimulated for 5 minutes through the addition of 10 mL lipopolysaccharides (LPSs) from Escherichia coli O55:B5 (Sigma-Aldrich, USA) at a final assay concentration of 1 μg/mL. Simultaneously, 10 mL of the N-formylmethionyl leucyl-phenylalanine (fMLP, Sigma Aldrich, USA) stimulant was added at a final assay concentration of 50 nM, along with the compounds to be evaluated (surfactant and inhibitor) and incubated for 30 minutes at 37 °C while mixing in a thermo shaker (TS 100, Fisher, USA). Surfacen was used at the final assay concentrations of 0.25 mg/mL to 10 mg/mL, and rCmPI-II was used at final concentrations of 0.1 µM to 200 µM. In the Surfacen/rCmPI-II combination assays, 0.5 mg/mL of Surfacen and 80 µM of inhibitor were used. The final assay volume was adjusted to 200 mL with PBS. Samples corresponding to the different designs were centrifuged at 2500 rpm for 10 minutes at 22 °C, and the supernatant was used to determine elastase activity.
In parallel, a positive control was performed with activated/stimulated neutrophils, and a negative control was performed with untreated neutrophils. To evaluate the effect of Surfacen and rCmPI-II, these were treated with neutrophils that were not activated/stimulated. The maximum elastase percentage present in neutrophils was determined by lysing activated/stimulated cells with 0.1% hexadecyltrimethylammonium bromide (HTAB) detergent (Sigma-Aldrich, USA) for 15 minutes at 4 oC.
Elastase enzyme activity Elastase enzyme activity was evaluated in 90 µL of the supernatant by measuring at 405 nm hydrolysis of methoxysuccinyl-Ala-Ala-Pro-Val-p-nitroaniline substrate; 10 µL, 2.8 mM dissolved in dimethyl sulfoxide (DMSO, Calbiochem, Merck, Germany), in Tris HCl 0.02 mol/L, NaCl 0.5 mol/L pH 8.0 (100 µL), for 30 minutes, in a plate reader (ChemWell Manager, EIA mode, USA). Each reaction (200 µL) was done in triplicate in a 96-well plate. The initial velocity of the reaction was calculated using the slope of the curve (DDO/Dt) in the linear area. Enzyme activity was expressed in U/mL.
Determining kinetics of spreading Equilibrium surface pressure was determined on a Langmuir surface balance. Surfacen (25 mg/mL), rCmPI-II (10 and 80 µM), and the Surfacen/rCmPI-II combination were applied with a 10 μL syringe (Hamilton, USA) to the air-liquid interface in the shape of a T, from a Langmuir balance made with teflon (Nima Technology, UK). The subphase volume is 15 mL (Tris buffer 5 mM, NaCl 150 mM, pH 7.0). Samples were applied at one end of the container, while a pressure sensor with surface plate (typically a small piece of filter paper) monitored changes in surface pressure of the active surface material, as a function of time. The kinetics of spreading (p vs. time) was obtained at 37 ± 1 °C for 300 seconds.
Statistical analysis This was performed using GraphPad software version 5.0 (GraphPad Software, USA). The mean and standard deviation (SD) were used as descriptive statistics, and the groups were compared using analysis of variance and a posteriori comparisons using Tukey’s test. The p value of 0.05 was used as the statistical significance threshold.
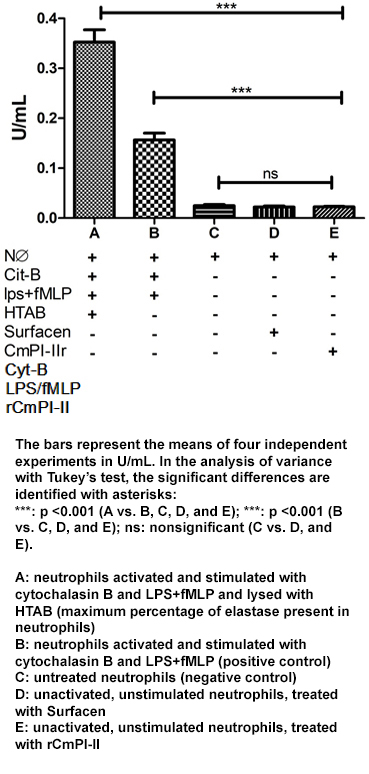
RESULTS Elastase enzyme activity present in the positive control after neutrophil lysis with the HTAB detergent was 0.35 ± 0.05 U/mL (Figure 1, bar A). This value corresponds to total elastase enzyme activity in the neutrophil and was considered the maximum enzymatic activity.
Figure 1: Neutrophil elastase enzyme activity
The amount of elastase released in response to activation with cytochalasin B and to LPS and fMLP stimuli (positive control, Figure 1, bar B) corresponds to about 45% of the maximum enzyme activity in neutrophils, determined by cell lysis. In the unstimulated, untreated neutrophils (negative control, Figure 1, bar C), spontaneous release of the enzyme was detected, representing about 10% of the positive control value (Figure 1, bar B). In the inactivated, unstimulated neutrophils treated with surfactant and elastase inhibitor (Figure 1, bars D and E), the enzyme activity value was similar to the negative control, which suggests that these compounds do not cause neutrophil activation.
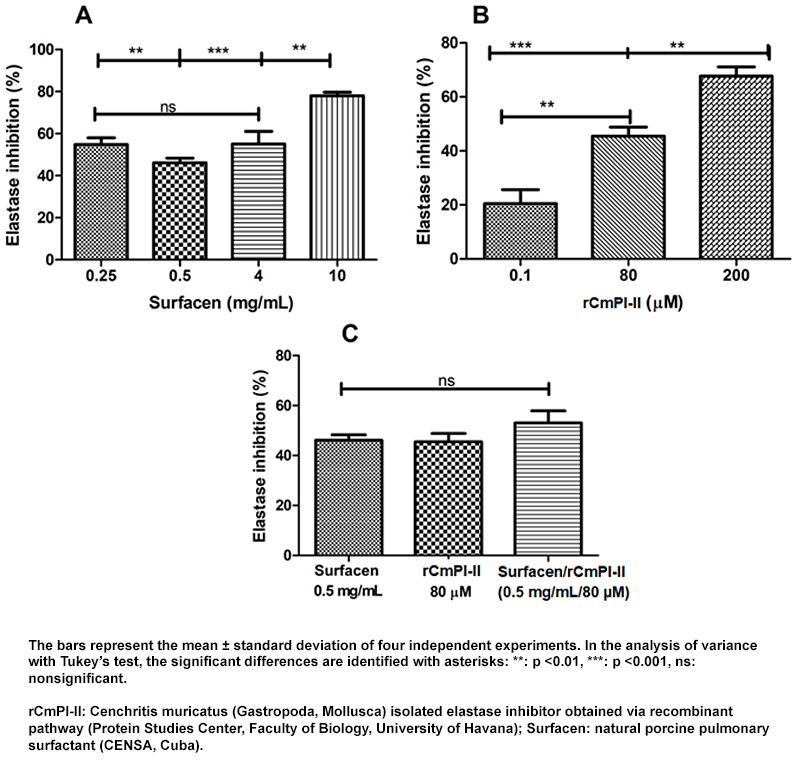
Effect of Surfacen, rCmPI-II, and the Surfacen/rCmPI-II combination on activated neutrophil elastase activity At concentrations of 0.25, 0.5 and 4 mg/mL, Surfacen inhibited 45% to 57% of elastase activity. At 10 mg/mL, inhibition was 78% (statistically significant value compared with other studied concentrations) (Figure 2-A).
In activated and stimulated neutrophils, incubated with rCmPI-II, elastase activity was inhibited at a magnitude dependent on the inhibitor concentration (Figure 2-B). rCmPI-II at 0.1 μM reduced 20% of elastase activity; at the maximum concentration evaluated (200 μM), inhibition was 68%. rCmPI-II is a competitive inhibitor of this enzyme and, therefore, increasing its concentration increases its inhibition. This characteristic has been described for the inhibitor in an enzyme assay with a chromogenic substrate. To study the effect of the product combination, the concentration that resulted in about 50% inhibition in the assays of each product was selected: for rCmPI-II, 80 µM, and for Surfacen, 0.5 mg/mL. The Surfacen/rCmPI-II combination did not affect the elastase inhibitor activity observed for both independently (Figure 2-C).
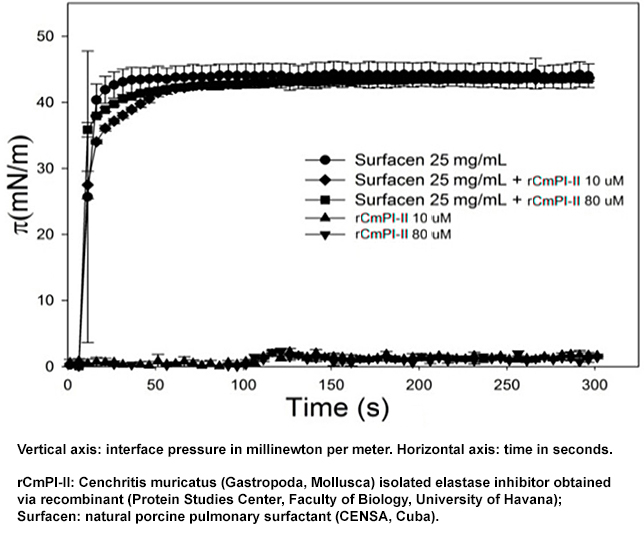
Effect of rCmPI-II on Surfacen interface properties Figure 3 compares the kinetics of spreading of Surfacen and the Surfacen/rCmPI-II combination, measured using changes in surface pressure (p) over time. Surfacen adsorbs very efficiently at the air-liquid interface, with an equilibrium surface pressure around 42 mN/m in less than 1 minute. The addition of rCmPI-II to Surfacen did not modify the kinetics of spreading. At the two concentrations evaluated, rCmPI-II did not modify the surface pressure.
Figure 2: Effect of Surfacen (A), rCmPI-II (B) and the Surfacen/rCmPI-II combination (C) on activated and stimulated neutrophil elastase activity
Figure 3: Spreading assays of Surfacen and Surfacen/rCmPI-II combination in a Langmuir surface balance
DISCUSSION Human pulmonary surfactant improves pulmonary function and oxygenation, and modulates innate and acquired immunity, regulating the lung’s inflammatory processes. Various surfactant preparations decrease respiratory burst cytokine release and nitric oxide production in inflammatory cells (neutrophils, monocytes and macrophages).[34,35] Among them, Surfacen, the Cuban porcine surfactant, decreases TNFa and IL-6 production in human monocytes responding to Staphylococcus aureus.[21]
There are few in vitro model studies on the modulatory effect of surfactants in clinical use on neutrophil activation. In 1996, Tegtmeyer evaluated the modulatory effect of surfactants in clinical use on the function of neutrophils responding to different damage-inducing agents.[36] The surfactants tested did not produce neutrophil activation. However, when the neutrophils stimulated with interleukin-8 (IL-8), neutrophil-activating peptide-2 (NAP-2), or fMLP were incubated with different surfactant combinations, elastase release depended on the type of surfactant. Exosurf and Alveofact had little effect on the elastase release induced by the three mediators, while Curosurf and Survanta inhibited cell response in a dose-dependent manner. Schulz demonstrated that Curosurf and Alveofact had an inhibitory effect on in vitro NET formation in neutrophils stimulated with phorbol-12-myristate-13-acetate (PMA). In both preparations, the effect was dose- and time-dependent; the effect was stronger with Alveofact. When the neutrophils were incubated with these preparations before PMA activation, the inhibitory effect was higher, which suggests a preventive effect. The authors suggest that these preparations reduce neutrophil activation and highlight pulmonary surfactant as a possible candidate for attenuating inflammation.[15]
This study showed that Surfacen inhibits the activity of released elastase, present in activated/stimulated human neutrophils in vitro. Some surfactants show different effectiveness against this enzyme in in vitro models of activated neutrophils, likely due to differences in its composition.[15,36] The inhibitory activity of Surfacen could be related to the release process of this enzyme by neutrophils once activated/stimulated. In this model, Surfacen’s elastase inhibition mechanism is unknown; however, for other surfactants (Survanta and Infasurf), the enzyme release mechanism is known to be modulated by their action on neutrophils, and it is mediated by depolarization and release of intracellular Ca++ through activation of the G protein pathway.[37] Recently, pulmonary surfactant preparations in clinical use have been shown to decrease expression of P2Y6, a G-coupled extracellular receptor that participates in NET formation by interacting with calcium pathways.[15]
rCmPI-II is an inhibitor of serine proteases, including human neutrophil elastase, that reduces elastase activity in an in vitro activated/stimulated neutrophil assay in a dose-dependent manner. This inhibitory activity is not affected by the presence of Surfacen. Several preclinical trials have investigated the therapeutic potential of neutrophil elastase inhibitors Sivelestat, Sirtinol, DX-890 and
BAY 85-8501 for treating lung diseases. The synthetic inhibitor Sivelestat is one of the most studied. In a murine model of acute lung injury involving the lung tissue repair process, the inhibitor decreased neutrophil accumulation in bronchoalveolar lavage and collagen deposition in lung parenchyma, and improved lung compliance.[38] In a clinical trial in patients with ARDS, Sivelestat increased ventilator-free days and 180-day survival.[39]
The mechanism of action of the synthetic inhibitor Sirtinol in an in vitro activated neutrophil model was to inhibit elastase enzyme activity, since its effect was not mediated by protein kinase A, or by calcium and kinase pathways regulated outside the cell; therefore, it did not directly affect neutrophil function. In an animal model of LPS-induced acute lung injury, Sirtinol reduced neutrophil recruitment and lung edema.[40]
DX-890, a peptide enzyme inhibitor, inhibits activity of elastase released by fMLP-stimulated neutrophils obtained from healthy individuals and patients with cystic fibrosis, inhibits neutrophil transmigration through epithelial cells, and decreases IL-8 secretion in nasal epithelial cells and sputum of patients with cystic fibrosis.[41] BAY 85-8501, another synthetic enzyme inhibitor, had a favorable safety and tolerance profile when administered over 28 days to patients with bronchiectasis not associated with cystic fibrosis; however, additional studies of prolonged treatment are needed to evaluate its clinical efficacy.[14]
rCmPI-II’s ability to reduce human neutrophil elastase activity, not only in experiments with a commercial enzyme,[26] but also in an in vitro model of activated/stimulated neutrophils obtained in this study, suggests that rCmPI-II might be used in inflammatory processes in which neutrophils are involved.
The combination of the surfactant Survanta and the alpha-1 antitrypsin elastase inhibitor in an in vivo model showed that the addition of alpha-1 antitrypsin improved oxygenation and surfactant metabolism in surfactant-deficient rats.[29] Here, Surfacen is shown to be absorbed very efficiently into the air–liquid interface with an equilibrium surface pressure of about 42 mN/m in less than 1 minute. The results of this study show that rCmPI-II does not affect the Surfacen surface properties.
Pulmonary surfactant may be combined with medications; to do so, both the surfactant and the drug transported by the surfactant must preserve their therapeutic functions. This study shows that the Surfacen/rCmPI-II combination did not modify the properties of either one in vitro. Inhibition of neutrophil elastase did not increase with respect to the values obtained with each compound separately, which could be related to different mechanisms of action of these compounds. Understanding these mechanisms on activated/stimulated neutrophils would open the door to using the Surfacen/rCmPI-II combination to treat inflammatory lung diseases.
Despite these advances, transferring the results with elastase inhibitors from the preclinical phase to the clinical phase is a challenge. Preclinical and clinical research continues, alongside development of new, more powerful and selective inhibitors.[42] Only two of these medications are used in clinical practice to date: alpha-1 antitrypsin (Prolastin), approved by the US Food and Drug Administration in 1987,[43,44] and Sivelestat (ONO-5046), approved for clinical use to treat ARDS and acute lung injury associated with systemic inflammatory response syndrome in Japan and South Korea.[13]
Respiratory failure is one of the causes of death in patients with COVID-19.[45,46] Clinical trials of pulmonary surfactants in COVID-19 are in process.[47,48] Surfacen is indicated in the Cuban COVID-19 Protocols for treatment of these patients.[6,49] The potential benefit of neutrophil elastase inhibitors in patients with severe COVID-19 is being investigated because these inhibitors could mitigate elastase damage on the lung connective tissue and limit the virus spreading capabilities by preventing S protein proteolytic activation.[50]
A limitation of this study is that it does not provide information about the mechanism of action of each of the compounds.
CONCLUSION The anti-elastase effect of the two Cuban products, Surfacen and the rCmPI-II inhibitor, is demonstrated in an activated neutrophil model. rCmPI-II does not affect Surfacen’s interface property and, therefore, both can be evaluated for combined use in treating inflammatory lung diseases.
FUNDING This study was partially funded by the International Foundation for Science (IFS, Grant F/5187-2, Sweden) and the Fondo Financiero de Ciencia e Innovación [Cuba’s Science and Innovation Finance Fund] (FONCI 9470).
Autilio C, Pérez-Gil J. Understanding the principle biophysics concepts of pulmonary surfactant in health and disease. Arch Dis Child Fetal Neonatal Ed. 2019 Jul;104(4):F443–F51. http://doi.org/10.1136/archdischild-2018-315413
Han S, Mallampalli RK. The role of surfactant in lung disease and host defense against pulmonary infections. Ann Am Thorac Soc. 2015 May;12(5):765–74. http://doi.org/10.1513/AnnalsATS.201411-507FR
Fessler MB, Summer RS. Surfactant lipids at the host–environment interface. Metabolic sensors, suppressors, and effectors of inflammatory lung disease. Am J Respir Cell Mol Biol. 2016 May;54(5):624–35. http://doi.org/10.1165/rcmb.2016-0011PS
Polin RA, Carlo WA. Surfactant replacement therapy for preterm and term neonates with respiratory distress. Pediatrics. 2014 Jan;133(1):156–63. http://doi.org/10.1542/peds.2013-3443
Blanco O, Pérez-Gil J. Biochemical and pharmacological differences between preparations of exogenous natural surfactant used to treat respiratory distress syndrome: role of the different components in an efficient pulmonary surfactant. European J Pharmacol. 2007 Jul 30;568(1–3):1–15. http://doi.org/10.1016/j.ejphar.2007.04.035
Center for State Control of Medicines, Equipments and Medical Devices (CU) [Internet]. Havana: Center for Control of Medicines, Equipment and Medical Devices – CECMED (CU); c2022. Registro. SURFACEN® (Surfactante pulmonar natural); 1995 Apr 7 [revised 2022 Feb 2; cited 2022 Apr 21]. 9 p. Available at: https://www.cecmed.cu/registro/rcp/biologicos/surfacenr-surfactante-pulmonar-natural. Spanish.
Yang SC, Tsai YF, Pan YL, Hwang TL. Understanding the role of neutrophils in acute respiratory distress syndrome. Biomed J. 2021 Aug;44(4):439–46. https://doi.org/10.1016/j.bj.2020.09.001
Jasper AE, McIver WJ, Sapey E, Walton GM. Understanding the role of neutrophils in chronic inflammatory airway disease. F1000Res. 2019 Apr 26;8. http://doi.org/10.12688/f1000research.18411.1
Korkmaz B, Moreau T, Gauthier F. Neutrophil elastase, proteinase 3 and cathepsin G: physicochemical properties, activity and physiopathological functions. Biochimie. 2008 Feb;90(2):227–42. http://doi.org/10.1016/j.biochi.2007.10.009
Tsai YF, Hwang TL. Neutrophil elastase inhibitors: a patent review and potential applications for inflammatory lung diseases (2010-2014). Expert Opin Ther Pat. 2015;25(10):1145–58. http://doi.org/10.1517/13543776.2015.1061998
Polverino E, Rosales-Mayor E, Dale GE, Dembowsky K, Torres A. The role of neutrophil elastase inhibitors in lung diseases. Chest. 2017 Aug;152(2):249–62. http://doi.org/10.1016/j.chest.2017.03.056
Ahmad S, Saleem M, Riaz N, Lee YS, Diri R, Noor A, et al. The natural polypeptides as significant elastase inhibitors. Front Pharmacol. 2020 Jun 5;11:688. http://doi.org/10.3389/fphar.2020.00688
Kido T, Muramatsu K, Yatera K, Asakawa T, Otsubo H, Kubo T, et al. Efficacy of early sivelestat administration on acute lung injury and acute respiratory distress syndrome. Respirology. 2017 May;22(4):708–13. http://doi.org/10.1111/resp.12969
Watz H, Nagelschmitz J, Kirsten A, Pedersen F, van der Mey D, Schwers S, et al. Safety and efficacy of the human neutrophil elastase inhibitor BAY 85-8501 for the treatment of non-cystic fibrosis bronchiectasis: a randomized controlled trial. Pulm Pharmacol Ther. 2019 Jun;56:86–93. http://doi.org/10.1016/j.pupt.2019.03.009
Schulz A, Pagerols Raluy L, Kolman JP, Königs I, Trochimiuk M, Appl B, et al. The inhibitory effect of Curosurf® and Alveofact® on the formation of neutrophil extracellular traps. Front Immunol. 2021 Jan 19;11:582895. http://doi.org/10.3389/fimmu.2020.582895
Morilla Guzmán AA, Díaz Casañas E, Debesa García F, Fernández Limia O. Efectividad del SURFACEN® en neonatos prematuros con síndrome de dificultad respiratoria. Rev Cubana Farm. 2015 Jul–Sep;49(3):502–11. Spanish.
Barrese-Pérez Y, Hidalgo-Sánchez AO, Ávila-Albuerne Y, Uranga-Piña R, Díaz-Casañas E, Fernández-Limia O. Surfactante pulmonar exógeno en adultos con síndrome de dificultad respiratoria aguda. Neumol Cir Torax. 2015 Jul–Sep;74(3):172–8. Spanish. https://dx.doi.org/10.35366/62367
Rodríguez-Moya VS, Gallo-Borrero CM, Santos-Áreas D, Prince-Martínez IA, Díaz-Casañas E, López-Herce Cid J. Exogenous surfactant and alveolar recruitment in the treatment of the acute respiratory distress syndrome. Clin Respiratory J. 2017 Nov;11(6):1032–9. http://doi.org/10.1111/crj.12462
Barrese Pérez Y, Hidalgo Sánchez AO, Ávila Albuerne Y, Uranga Piña R, Díaz Casañas E, Fernández Limia O. Seguridad del tratamiento con surfactante pulmonar en el síndrome de dificultad respiratoria aguda en adultos. AMC [Internet]. 2015 Jul 9 [cited 2016 Apr 27];19(6):557–8. Available at: http://www.revistaamc.sld.cu/index.php/amc/issue/view/88. Spanish.
de Guevara YLL, Hidalgo OB, Santos SS, Brunialti MKC, Faure R, Salomao R. Effect of natural porcine surfactant in Staphylococcus aureus induced pro-inflammatory cytokines and reactive oxygen species generation in monocytes and neutrophils from human blood. Int Immunopharmacol. 2014 Aug;21(2):369–74. http://doi.org/10.1016/j.intimp.2014.05.020
Blanco O, Ramírez W, Lugones Y, Díaz E, Morejón A, Rodríguez VS, et al. Protective effects of Surfacen® in allergen-induced asthma mice model. Int Immunopharmacol. 2022 Jan;102:108391. http://doi.org/10.1016/j.intimp.2021.108391
Haitsma JJ, Lachmann U, Lachmann B. Exogenous surfactant as a drug delivery agent. Adv Drug Delivery Rev. 2001 Apr 25;47(2–3):197–207.
Boel L, Banerjee S, Chakraborty M. Postnatal steroids in extreme preterm infants: intra-tracheal instillation using surfactant as a vehicle. Paediatric Respir Rev. 2018 Jan;25:78–84. http://doi.org/10.1016/j.prrv.2017.05.002
Hascoët JM, Picaud JC, Ligi I, Blanc T, Daoud P, Zupan V, et al. Review shows that using surfactant a number of times or as a vehicle for budesonide may reduce the risk of bronchopulmonary dysplasia. Acta Paediatr. 2018 Jul;107(7):1140–4. http://doi.org/10.1111/apa.14171
González Y, Tanaka AS, Hirata IY, del Rivero MA, Oliva ML, Araujo MS, et al. Purification and partial characterization of human neutrophil elastase inhibitors from the marine snail Cenchritis muricatus (Mollusca). Comp Biochem Physiol A Mol Integr Physiol. 2007 Apr;146(4):506–13. http://doi.org/10.1016/j.cbpa.2006.01.022
González Y, Pons T, Gil J, Besada V, Alonso-del-Rivero M, Tanaka AS, et al. Characterization and comparative 3D modeling of CmPI-II, a novel ‘non-classical’Kazal-type inhibitor from the marine snail Cenchritis muricatus (Mollusca). Biol Chem. 2007 Nov;388(11):1183–94. http://doi.org/10.1515/BC.2007.129
Cabrera-Muñoz A, Valiente PA, Rojas L, Alonso-del-Rivero Antigua M, Pires JR. NMR structure of CmPI-II, a non-classical Kazal protease inhibitor: understanding its conformational dynamics and subtilisin A inhibition. J Struct Biol. 2019 Jun 1;206(3):280–94. http://doi.org/10.1016/j.jsb.2019.03.011
Belai Y, Hernández-Juviel JM, Bruni R, Waring AJ, Walther FJ. Addition of alpha1-antitrypsin to surfactant improves oxygenation in surfactant-deficient rats. Am J Respir Crit Care Med. 1999 Mar;159(3):917–23. http://doi.org/10.1164/ajrccm.159.3.9801121
Charles G. Cochrane, inventor; The Scripps Research Institute, La Jolla. Compositions for treatment and prevention of pulmonary conditions. United States patent US7863241B2. 2011 Jan. 4
Manzanares D, Díaz E, Alfonso W, Escobar A, Colomé H, Muñoz M, et al, inventors. Surfactante pulmonar natural porcino. Republic of Cuba patente CU, A 61:35–42K. 1995. Spanish.
Cabrera-Muñoz A, Rojas L, Gil DF, González-González Y, Mansur M, Camejo A, et al. Heterologous expression of Cenchritis muricatus protease inhibitor II (CmPI-II) in Pichia pastoris system: purification, isotopic labeling and preliminary characterization. Protein Expr Purif. 2016 Oct;126:127–36. http://doi.org/10.1016/j.pep.2016.06.011
Böyum A. Isolation of mononuclear cells and granulocytes from human blood. Isolation of monuclear cells by one centrifugation, and of granulocytes by combining centrifugation and sedimentation at 1 g. Scand J Clin Lab Invest Suppl. 1968;97:77–89. PMID: 4179068.
Bersani I, Kunzmann S, Speer CP. Immunomodulatory properties of surfactant preparations. Expert Rev Anti Infect Ther. 2013 Jan;11(1):99–110. http://doi.org/10.1586/eri.12.156
Baur FM, Brenner B, Goetze-Speer B, Neu S, Speer CP. Natural porcine surfactant (Curosurf) down-regulates mRNA of tumor necrosis factor-alpha (TNF-alpha) and TNF-alpha type II receptor in lipopolysaccharide-stimulated monocytes. Pediatr Res. 1998 Jul;44(1):32–6. http://doi.org/10.1203/00006450-199807000-00005
Tegtmeyer FK, Gortner L, Ludwig A, Brandt E. In vitro modulation of induced neutrophil activation by different surfactant preparations. Eur Respir J. 1996 Apr;9(4):752–7. http://doi.org/10.1183/09031936.96.09040752
Boston ME, Frech GC, Chacón-Cruz E, Buescher ES, Oelberg DG. Surfactant releases internal calcium stores in neutrophils by G protein-activated pathway. Exp Biol Med (Maywood). 2004 Jan;229(1):99–107. http://doi.org/10.1177/153537020422900112
Fujino N, Kubo H, Suzuki T, Suzuki T, He M, Yamada M, et al. Administration of a specific inhibitor of neutrophil elastase attenuates pulmonary fibrosis after acute lung injury in mice. Exp Lung Res. 2012 Feb;38(1):28–36. http://doi.org/10.3109/01902148.2011.633306
Tagami T, Tosa R, Omura M, Fukushima H, Kaneko T, Endo T, et al. Effect of a selective neutrophil elastase inhibitor on mortality and ventilator-free days in patients with increased extravascular lung water: a post hoc analysis of the PiCCO Pulmonary Edema Study. J Intensive Care. 2014 Dec 31;2(1):67. http://doi.org/10.1186/s40560-014-0067-y
Tsai Y-F, Yu H-P, Chang W-Y, Liu F-C, Huang Z-C, Hwang T-L. Sirtinol inhibits neutrophil elastase activity and attenuates lipopolysaccharide-mediated acute lung injury in mice. Sci Reports. 2015 Feb 10;5:8347. http://doi.org/10.1038/srep08347
Dunlevy FK, Martin SL, de Courcey F, Elborn JS, Ennis M. Anti-inflammatory effects of DX-890, a human neutrophil elastase inhibitor. J Cyst Fibros. 2012 Jul;11(4):300–4. http://doi.org/10.1016/j.jcf.2012.02.003
Crocetti L, Giovannoni MP, Cantini N, Guerrini G, Vergelli C, Schepetkin IA, et al. Novel sulfonamide analogs of sivelestat as potent human neutrophil elastase inhibitors. Front Chem. 2020 Sep 1;8:795. http://doi.org/10.3389/fchem.2020.00795
Wewers MD, Casolaro MA, Sellers SE, Swayze SC, McPhaul KM, Wittes JT, et al. Replacement therapy for alpha 1-antitrypsin deficiency associated with emphysema. N Engl J Med. 1987 Apr 23;316(17):1055–62. http://doi.org/10.1056/nejm198704233161704
Mohanka M, Khemasuwan D, Stoller JK. A review of augmentation therapy for alpha-1 antitrypsin deficiency. Expert Opinion Biol Ther. 2012 Jun;12(6):685–700. http://doi.org/10.1517/14712598.2012.676638
Gibson PG, Qin L, Puah SH. COVID-19 acute respiratory distress syndrome (ARDS): clinical features and differences from typical pre-COVID-19 ARDS. Med J Aust. 2020 Jul;213(2):54–6.e1. http://doi.org/10.5694/mja2.50674
Fan E, Beitler JR, Brochard L, Calfee CS, Ferguson ND, Slutsky AS, et al. COVID-19-associated acute respiratory distress syndrome: is a different approach to management warranted? Lancet Respir Med. 2020 Aug;8(8):816–21. http://doi.org/10.1016/s2213-2600(20)30304-0
Busani S, Dall’Ara L, Tonelli R, Clini E, Munari E, Venturelli S, et al. Surfactant replacement might help recovery of low-compliance lung in severe COVID-19 pneumonia. Therc Adv Resp Dis. 2020 Jan–Dec;14:1753466620951043. http://doi.org/10.1177/175346662095104344
Bautin AEB, Avdeev SN, Seyliev AA, Shvechkova MV, Merzhoeva ZM, Trushenko NV, et al. [Inhalation surfactant therapy in the integrated treatment of severe COVID-19 pneumonia]. Tuberc Lung Dis. 2020;98(9). http://doi.org/10.21292/2075-1230-2020-98-9-6-12. Russian.
Díaz Casañas E, Rodríguez Moya VS, Montes de Oca Martínez N. Surfactante pulmonar: posible intervención frente al nuevo Síndrome Respiratorio Agudo Severo Coronavirus 2 (SARS-CoV-2). Rev Habanera Cienc Médicas. 2020;19(Suppl 1):1–5. Spanish.
Mohamed MMA, El-Shimy IA, Hadi MA. Neutrophil elastase inhibitors: a potential prophylactic treatment option for SARSCoV-2-induced respiratory complications? Crit Care. 2020 Jun 8;24(311):1–2. http://doi.org/10.3389/fphar.2020.00688
THE AUTHORS
Yuliannis Lugones-Ladrón de Guevara*, pharmacist with a master’s degree in pharmacology. Assistant researcher, National Center for Animal and Plant Health (CENSA), San José de las Lajas, Cuba. https://orcid.org/0000-0002-8467-4736
Aymara Cabrera-Muñoz, biochemist with a doctorate in biological sciences. Assistant professor, Protein Studies Center (CEP), Faculty of Biology, University of Havana, Cuba. https://orcid.org/0000-0002-8208-2446
Arturo Chang-Monteagudo, physician specializing in immunology. Researcher and assistant professor, Hematology and Immunology Institute, Havana, Cuba. https://orcid.org/0000-0002-0843-372X
Maday Alonso del Rivero-Antigua, biochemist with a doctorate in biological sciences. Senior researcher, CEP, Faculty of Biology, University of Havana, Cuba. https://orcid.org/0000-0003-1988-6852
Odalys Blanco-Hidalgo (Corresponding author: oblanco@censa.edu.cu, odalysbh@infomed.sld.cu), biochemist with a doctorate in pharmaceutical sciences. Senior researcher, CENSA, San José de las Lajas, Cuba. https://orcid.org/000-0002-8947-9251
Submitted: February 11, 2022 Approved: August 17, 2022 Disclosures: Yuliannis Lugones, Mercyleidi Díaz and Odalys Blanco are employed at CENSA, the center that produces Surfacen. Aymara Cabrera and Maday Alonso are employed at the center that obtains rCmPI-II.
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.