
Respiratory Syncytial Virus in Pregnant Women: Systematic Review and Meta-Analysis
by
 , ,
, ,
Matteo Riccò
1,* ,
,
Pietro Ferraro
2 ,
,
Silvia Corrado
3,
Alessandro Zaniboni
4,
Elia Satta
4 and
Silvia Ranzieri
4 1
AUSL–IRCCS di Reggio Emilia, Servizio di Prevenzione e Sicurezza Negli Ambienti di Lavoro (SPSAL), Local Health Unit of Reggio Emilia, Via Amendola n. 2, I-42122 Reggio Emilia, Italy
2
Occupational Medicine Unit, Direzione Sanità, Italian Railways’ Infrastructure Division, RFI SpA, Piazza della Croce Rossa n. 1, I-00161 Rome, Italy
3
Department of Medicine DAME, Division of Pediatrics, University of Udine, Via delle Scienze, n. 206, I-33100 Udine, Italy
4
Department of Medicine and Surgery, University of Parma, Via Gramsci 14, I-43126 Parma, Italy
*
Author to whom correspondence should be addressed.
Women 2022, 2(2), 147-160; https://doi.org/10.3390/women2020016
Submission received: 29 April 2022
/
Revised: 5 June 2022
/
Accepted: 6 June 2022
/
Published: 10 June 2022
(This article belongs to the Special Issue Health and Preventive Strategies in Order to Protect Pregnancy)
Abstract
:Human Respiratory Syncytial Virus (RSV) is a highly contagious viral pathogen. In infants, it is usually listed among the main causes of medical referrals and hospitalizations, particularly among newborns. While waiting for the results of early randomized controlled trials on maternal vaccination against RSV, the present systematic review and meta-analysis aimed to collect available evidence on maternal RSV infections. According to the PRISMA statement, Pubmed, Embase, and pre-print archive medRxiv.og were searched for eligible studies published up to 1 April 2022. Raw data included the incidence of RSV infection among sampled pregnant women, and the occurrence of complications. Data were then pooled in a random-effects model. Heterogeneity was assessed using the I2 measure, while reporting bias was assessed by means of funnel plots and regression analysis. A total of 5 studies for 282,918 pregnancies were retrieved, with a pooled prevalence of 0.2 per 100 pregnancies and 2.5 per 100 pregnancies with respiratory tract infections. Neither maternal deaths nor miscarriages were reported. Even though detailed data were available only for 6309 pregnancies and 33 RSV cases, infant outcomes such as low birth weight and preterm delivery were rare (in both cases 0.04%), but up to 9.1% in cases where RSV diagnosis was confirmed. No substantially increased risk for preterm delivery (RR 1.395; 95%CI 0.566 to 3.434) and giving birth to a low-birth-weight infant (RR 0.509; 95%CI 0.134 to 1.924) was eventually identified. Conclusions. Although RSV is uncommonly detected among pregnant women, incident cases were associated with a relatively high share of complications. However, heterogeneous design and the quality of retrieved reports stress the need for specifically designed studies.
1. Introduction
Since its first description in 1956 [1], human Respiratory Syncytial Virus (RSV) (genus orthopneumovirus, family of Pneumoviridae) [2,3,4,5,6,7,8] has emerged as a highly contagious viral pathogen. According to available figures, RSV represents the main cause of hospitalization among infants < 1 year of age in western countries, and a leading cause of lower respiratory tract infections (RTI) in children in their first year of life [4,9,10,11,12], with a well-defined seasonal trend [4,8].
Likewise, other viral agents of RTI do not elicit a long-lasting immunity, and adults are constantly re-infected throughout their lives, with annual rates ranging from 2 to 12% [13,14]. Until recently, the only available therapeutic option has been represented by supportive care (i.e., respiratory support and the management of volume depletion) [7,15], and preventive interventions have been limited to monoclonal antibodies (mAb) [16,17,18]. Even though real-world evidence has shown that mAb are rather effective in reducing hospitalizations and preventing lower RTI in some high-risk groups (i.e., prematurely born infants under 6 months of age, and children with certain comorbidities under 2 years of age during the RSV season) [19,20,21,22,23,24], mAb are affected by several shortcomings. Firstly, they must be injected once each month during the RSV season, for a total of five subsequent weight-dependent doses (i.e., 15 mg/kg), with obvious logistic issues and costs ranging between $1661 and $2584 per dose [25]. As a consequence, alternative strategies including long-acting mAb [26,27,28,29] and new, effective vaccines have been more recently explored [2,4,19,30,31].
In this regard, maternal vaccination strategies appear particularly attractive [32,33,34,35], as transplacental transfer of neutralizing antibodies is well-documented even in RSV infections, and high titers of maternal antibodies have been shown able to reduce the risk of infant RSV infections, particularly in the first 30 days of life [36,37,38,39].
Despite the potential analogies with other maternal vaccination programs, such as influenza and pertussis vaccination programs [40,41,42], some significant ethical issues still remain to be addressed. More precisely, while there is consolidated evidence that pregnant women are at increased risk of serious illness and mortality due to influenza virus infection [43], giving some further rationale to their vaccination, more limited information is available on RSV infections. On the one hand, RSV usually does not cause significant disease in healthy adults. On the other hand, some earlier reports have suggested that RSV infection in pregnancy may increase the risk of early delivery by cesarean section [44,45,46], as well as higher rates of adverse pregnancy outcomes [44,47,48]. While we are waiting for the results of the earlier large randomized controlled trials on maternal vaccination [49,50], an updated synthesis of the literature is therefore needed to ascertain (1) whether RSV infection may be acknowledged or not as a rare occurrence in pregnant women; (2) whether available evidence confirms that RSV infections in pregnancy are associated with more severe outcomes for mothers and children or not.
2. Results
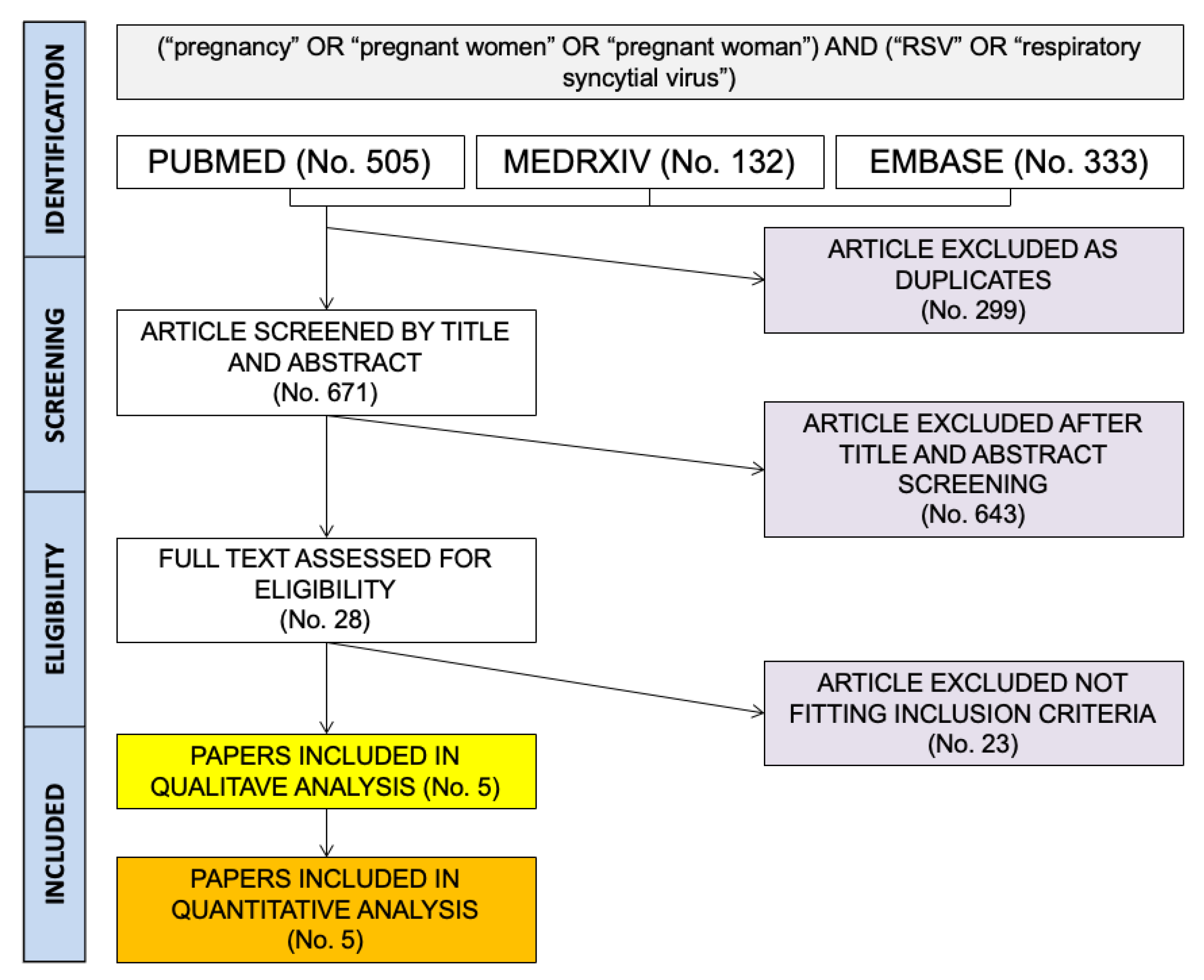
As shown in Figure 1, a total pool of 970 entries (i.e., 505 from PubMed; 132 from MedRxiv; 333 from EMBASE) were initially retrieved. After duplicates were removed (No. 299), the resulting 671 articles were screened by title and abstract. Of them, 271 entries were removed after the title and abstract screening. Twenty-eight articles were then assessed and reviewed via full-text screening. Finally, five papers were included in the qualitative and quantitative analysis.
A detailed description of individual studies is available in Table 1, and their corresponding risk of bias (ROB) assessment is summarized in Figure 2.
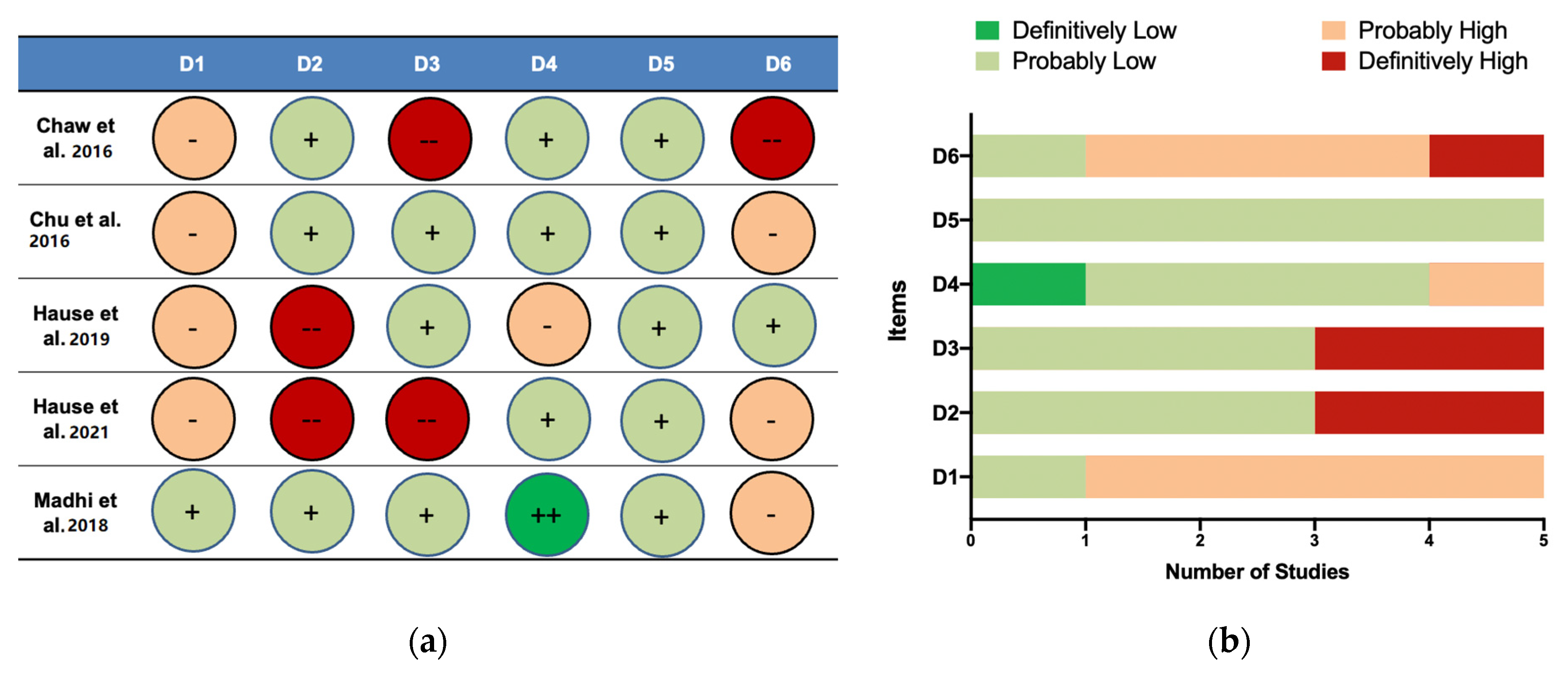
When dealing with selection bias, four out of five studies were reasonably affected by possible selection bias, as enrollment required registration with local providers [46,51,52,53] in areas affected by limited access to healthcare services, or specific healthcare plans of infrastructures [46,53]. Exposure assessment was affected by a definitively high risk of bias in two studies [46,53] where the clinical criteria for RSV testing were not strictly defined. The ROB for the outcome assessment was likely low in three of the reported studies, as both maternal and offspring clinical features were reported [46,52,53,54], while one study did not include significant information about the mother [51], and another study only reported hospitalized women giving live births [46]. Confounding factors were accurately taken into account by one study only [54], but the remaining studies considered differences among the sampled individuals for stratification, with a likely low risk of bias. Similarly, reporting bias (i.e., selective inclusion of outcomes in the publication of the study on the basis of the results) was likely low in all studies. However, in two reports [46,51], the study design presumptively impaired the proper identification of complications, while other reports lacked the proper assessment of pregnancies occurring during the RSV season or outside the RSV season [46,51,52]. Both issues were properly addressed by only one report [53].
As shown in Table 2, a total of 282,918 pregnancies were included, with the majority of them (97.3%) from a study retrieving data on women at Kaiser Permanente Southern California, whose pregnancies ended in a live birth between 1 July 2010 and 30 April 2017. A further study by Regan et al. was, in turn, excluded as reported estimates on RSV infections were only available in hospitalized women [47].
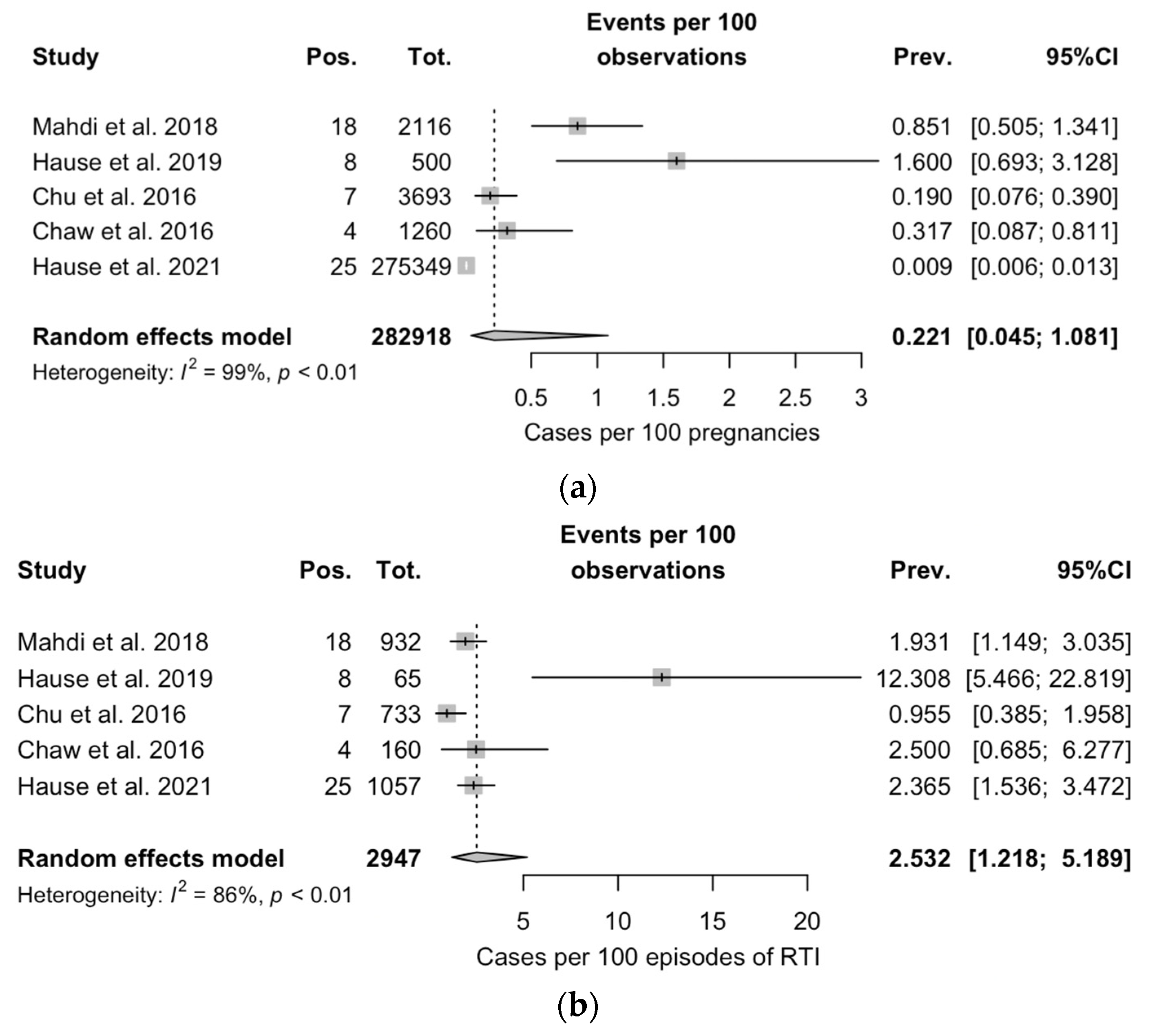
Overall, 2942 cases of RTI were documented, including a total of 62 RSV infections. In sampled pregnancies, the occurrence of RTI ranged between 0.4 and 44.0% (Figure 3a), with a corresponding share of RSV infections over RTI cases ranging between 1.0% and 12.3%, for a pooled RSV prevalence of 0.221 (95%CI 0.045 to 1.081) per 100 pregnancies, and 2.532 (95%CI 1.218 to 5.189) per 100 episodes of RTI (Figure 3b). In both cases, heterogeneity was substantial (I2 = 99% and I2 = 86%, respectively). In total, only 11 cases required hospitalization (i.e., 0.003% of all pregnancies, 0.4% of all RTIE, and 2.5% of all RSV cases).
Clinical characteristics of the pregnancies were reported by four studies [46,52,53,54], but one of them only included clinical data on hospitalized women (i.e., 10 out of 25 cases) [46]. Of them, four episodes evolved into pneumonia and two into sepsis. However, as no detailed information on other patients (i.e., 15/25 RSV positive cases) is provided, summary estimates were calculated in three studies, for a total of 33 RSV cases over 6309 pregnancies (i.e., 2% of the total sample), and are reported in Table 3 [51,53,54].
Overall, 6.1% of RSV episodes developed maternal pneumonia, but no maternal deaths were reported. On the contrary, complications in the infant were reported in approximately 1 out of 10 pregnancies, as 9.1% of RSV pregnancies resulted in preterm delivery and/or in a low-birth-weight infant.
Comparisons between RSV cases and normal pregnancies were limited to the estimates from two studies by the heterogeneity of data reporting on non-RSV cases. A pooled Risk Ratio (RR) of 1.193 was reported, 95%CI 0.076 to 18.681 (p = 0.900) for miscarriage, with an RR of 1.395 (95%CI 0.566 to 3.434; p = 0.479) for preterm delivery, and an RR of 0.509 (95%CI 0.134 to 1.924) for giving birth to a low-birth-weight infant (p = 0.289).
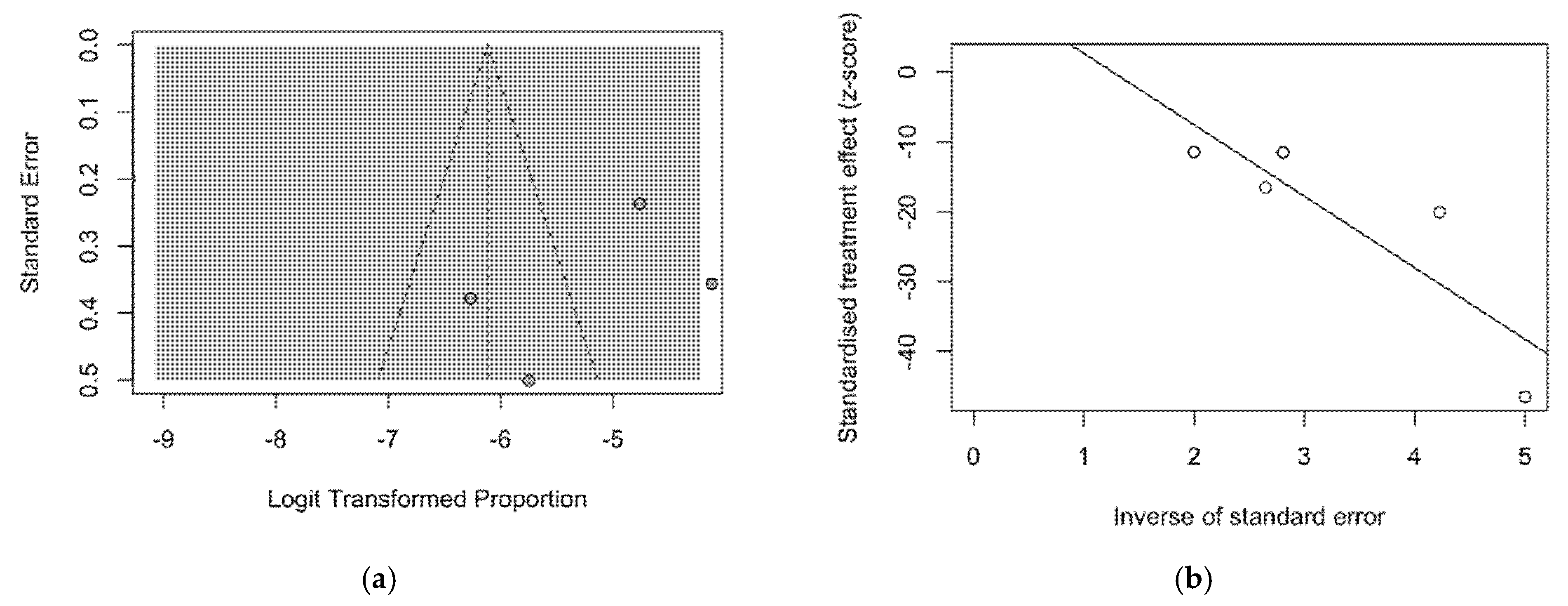
The presence of publication bias was evaluated using funnel plots and regression tests for funnel plot asymmetry. In the funnel plot, studies’ effect sizes are plotted against their standard errors; each point represents a separate study, and their asymmetrical distribution upon visual inspection is suggestive of publication bias (i.e., publication depending not just on the quality of the research, but also on the hypothesis tested, and the significance and direction of detected effects), as in Figure 4a. Such subjective evidence from the funnel plot was only partially confirmed after the regression test. In fact, the Egger test ruled out publication bias (i.e., t = 1.07, df = 4, p-value = 0.361). On the other hand, in radial plots (Figure 4b), estimates were substantially scattered across the regression line, suggesting no significant small-study effect.
3. Discussion
Recent studies have suggested that the occurrence of RSV infections in adults has been substantially underscored [13,14,55,56,57,58], but limited data exist on the clinical characteristics of infections in pregnant women [45,47]. For instance, in a previous case series from the USA, two out of three cases eventually developed respiratory distress, requiring mechanical ventilation, suggesting that RSV infections in pregnancy may represent a clinically significant event [45].
However, as RSV is uncommonly tested among women with RTI, particularly during influenza season, substantial uncertainties about the actual prevalence of RSV infections still remain [47,59]. In fact, the interest in maternal infections and complications has been only recently raised by the ongoing RCT on RSV immunization in pregnant women, a strategy that is specifically designed in order to protect the newborns during their first months of life [32,49,50]. On the one hand, future health technology assessments on maternal vaccination strategies will require a preventive, detailed definition of the burden of disease and potential outcomes of RSV infection in pregnant women [60,61,62]. On the other hand, studies on maternal influenza strategies have stressed how difficult reaching targeted vaccination rates could be for a pathogen whose actual relevance in adults is irregularly acknowledged by the general population [43,63,64,65,66]. Unfortunately, RSV is an often “forgotten” pathogen, and medical professionals may also fail to acknowledge the potentially dismal consequences of RSV infection in infants and adults [67,68,69]. Therefore, recommending a medical intervention to otherwise healthy individuals with a low risk of complications may elicit substantial ethical issues as well as unmotivated concerns [68,69] that could be mitigated only through the characterization of a direct advantage for the pregnant women themselves [54].
In our systematic review and meta-analysis, we were able to retrieve data on a total of 282,918 pregnancies, with 58 incident cases of RSV infection, for an attack rate of 0.2%. Such estimates reasonably represent an underestimation of the actual figures, as only women with signs and symptoms of RTI were regularly tested for RSV [46,48,51,52,53], and in healthy adults, RSV infections are often limited to indolent mucosal infections [56,70]. For example, in family studies, RSV infections have been associated with fever in 5 to 27% of cases [56]. Not coincidentally, in a previous report on hospitalization for RTI in California, Israel, Ontario, and Western Australia, a total of 21 women out of 846 episodes of RTI were eventually positive for RSV [47], for an attack rate of around 2.5%. Even though it is reasonable that most cases of RSV in pregnant women may have occurred unnoticed, we cannot conversely rule out the potential oversampling of RSV cases. As RSV follows a clear and well-known seasonal trend [71,72,73,74,75], studies that mostly include “in-season” pregnancies may have over-reported cases of RSV infections compared to studies including a larger share of pregnancies outside the RSV season. In this regard, only two papers properly took into account the background viral activity [46,53]. Not surprisingly, most cases did cluster between the 44th and 52nd calendar weeks (i.e., the conventional RSV season for Southern USA).
In other words, RSV infections in pregnant women do occur, but the incidence of severe infections (i.e., those cases that have a better chance to be accurately detected, tracked, and reported) is quite rare. Corresponding figures are hardly comparable to available estimates for other respiratory tract pathogens, likewise with seasonal influenza, whose attack rates usually range between 9% and 11% [76,77,78], with a 0.7 to 0.9% risk for influenza infection per month [79]. On the other hand, even though both maternal and infant deaths were recorded, the occurrence of complications in incident cases was far from being inconspicuous. Not only 11 out of the 58 sampled cases (19.0%) required hospitalization [46,53], but focusing the analyses on studies that reported both hospitalized and non-hospitalized cases (No. = 33), the incidence of pneumonia was noticeable (6.1%) [51,53,54]. Similarly, the burden of infant complications was relatively high, with 9.1% of infants born preterm and/or with low birth weight. When dealing with these figures, however, a somewhat precautionary approach is forcibly required.
Firstly, the two largest studies [52,54] were based on populations affected by poverty, gender inequalities, malnutrition, and high occurrences of infectious diseases such as HIV/AIDS and tuberculosis. In other words, these infant outcomes may be rather associated with baseline conditions of the sampled population than with RSV infections. Nonetheless, no substantially increased risk for preterm delivery (RR 1.395; 95%CI 0.566 to 3.434) and giving birth to a low-birth-weight infant (RR 0.509; 95%CI 0.134 to 1.924) was eventually identified. On the contrary, as milder cases of RSV likely failed to be sampled for the pathogen being deprived of noticeable signs and symptoms, original studies may have failed to properly assess the association between RSV infection and infant outcomes [52].
Limitations. Despite the potential interest, our study is affected by several limitations. Firstly, we had to deal with the implicit limitations of all meta-analyses, being highly dependent on the quality and heterogeneity of the original studies [80,81]. From this point of view, not only the number of studies we were able to retrieve was limited, but also their quality was highly heterogeneous. In fact, as the actual burden of RSV in adults has been only recently acknowledged, the potential impact on pregnant women has been mostly ignored until the case series from Wheeler et al. [45]. Even in subsequent studies, maternal outcomes have been only rarely addressed, with the limited evidence we were able to summarize in the present review. Likewise, the comparison of prevalence rates across various studies and different sampling strategies is particularly complicated. For example, the study from Hause et al. [46] mostly focused on hospitalized cases tested for RSV, the very same case definition and sampling strategy in other collected studies were quite heterogeneous [51,53,54,82]. Moreover, two out of the five studies were performed in countries (i.e., Nepal and Mongolia) with limited access to maternal and newborn care [4,51,52,82], and the overall figures may have been substantially biased through the oversampling of cases characterized by a more severe outcome, particularly when compared to the aforementioned studies from Texas and California [46,53,59]. Not coincidentally, the reported attack rates had a very large actual range, from 0.955% to 12.308% on total RTI.
Eventually, all the reported studies were performed before the SARS-CoV-2 pandemic. The implementation and the subsequent lifting of non-pharmaceutical interventions (NPI, i.e., public health measures that aim to prevent and/or control SARS-CoV-2 transmission in the community) have resulted in a sudden and earlier-than-expected end of the RSV epidemic season, with substantially no cases detected in the following months [83,84,85,86,87]. NPI blocked the normal transmission of RSV to susceptible individuals at the community level [85,86,88,89,90,91,92], generating a larger RSV-vulnerable population, and preserving susceptibility to the pathogen during the subsequent seasons [2,88,89,90,93]. To date, the impact of lockdown measures has been mainly assessed on infants, but updated figures during the reemergent RSV epidemics in 2021–2022 are needed to guarantee a better cost-effectiveness estimate of potential preventive interventions.
4. Materials and Methods
This systematic review and meta-analysis of the literature were conducted following the “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA) guidelines [94], and research concepts were preliminarily defined according to the “PICO” (Patient/Population/Problem; Intervention; Control/Comparator; Outcome) strategy (Table 4). The review was registered with PROSPERO (CRD42022330471).
Two scholarly databases (i.e., PubMed/MEDLINE and EMBASE) and the pre-print server medrxiv.org were searched for relevant studies from inception up to 1 April 2022, without applying any backward chronological restrictions. In order to collect the most evidence available, we opted for a broad search strategy that resulted from the combination of the following keywords (free text and Medical Subject Heading [MeSH] terms, where appropriate): (“pregnancy” OR “pregnant women” OR “pregnant woman”) AND (“RSV” OR “respiratory syncytial virus”). Articles eligible for review were original research publications available online or through inter-library loans. A language filter was applied, by retaining articles written in Italian, English, German, French, or Spanish, the languages spoken by the investigators.
Records whose title and abstract appeared pertinent to the search strategy were initially handled using references management software (Mendeley Desktop Version 1.19.5, Mendeley Ltd., London, UK, 2019), being subsequently reviewed and screened by two independent authors (E.S. and A.Z.) against eligibility criteria. More precisely, retrieved studies were included if they met the following inclusion criteria:
- Reporting a crude number of assessed pregnancies.
- Reporting the number of RSV cases diagnosed.
- Diagnosis of RSV infection by means of either polymerase chain reaction or point-of-care tests.
In order to avoid the risk of oversampling more severe cases, studies were excluded if the diagnosis of RSV infection was limited to hospitalized women. Only articles reporting original results were retained. Therefore, review articles, meta-analyses, case reports, case series, meeting reports, and conference abstracts were excluded from both qualitative and quantitative analysis. All articles meeting all of the inclusion criteria were retained for the full-text review. The investigators independently read full-text versions of eligible articles. Disagreements were resolved by consensus between the two reviewers; when it was not possible to reach a consensus, input from a third investigator (M.R.) was searched and obtained. Data extracted included:
- Settings of the study.
- Number of included pregnancies cases.
- Number of RTI assessed (if available).
- Number of RSV episodes.
- Outcome of RSV episodes, and more precisely, episodes of pneumonia, maternal deaths, miscarriages, giving birth preterm, and/or giving birth to a low-birth-weight infant.
After data extraction, studies were rated on the potential risk of bias by means of the National Toxicology Program (NTP)’s Office of Health Assessment and Translation (OHAT) handbook and respective risk of bias (ROB) tool [95,96]. The ROB tool evaluates the internal validity of a given study in order to assess whether the study’s design and conduct have compromised the credibility of the link between the exposure and the outcome or not. The OHAT ROB tool covers six possible sources of bias (i.e., participant selection, confounding, attrition/exclusion, detection, selective reporting, and other sources) with potential answers ranging from “definitely low,” “probably low,” “probably high,” to “definitely high”. Interestingly, the OHAT ROB tool does not apply an overall rating for each study, and the OHAT handbook also recommends that even studies with “probably high” or “definitely high” ratings should not be removed from consideration of the overall body of evidence.
Initially, a descriptive analysis was performed by calculating the crude prevalence figure per 100 pregnancies: If a study did not include raw data, either as the number of prevalent cases or a referent population, such figures were reverse-calculated from available data. In order to cope with the presumptive heterogeneity in the study design, we opted for a random-effect model. The amount of inconsistency between included studies was estimated by means of the I2 statistic (i.e., the percentage of total variation across studies that is due to heterogeneity rather than chance), assuming the following categorization: For I2 estimates ranging from 0 to 25%, low heterogeneity was assumed; for I2 ranging between 26% and 50%, moderate heterogeneity; for I2 ≥ 50%, the heterogeneity was acknowledged as substantial. To investigate publication bias, contour-enhanced funnel plots representing the Egger test for quantitative publication bias analysis (at a 5% of significance level) were generated. Radial plots were then calculated and visually inspected to rule out small study bias. All analyses were performed by means of “meta” and “metafor” packages with R (version 4.0.3) and RStudio (version 1.1.463) software. The meta package is an open-source add-on for conducting meta-analyses.
5. Conclusions
RSV was uncommonly detected among pregnant women, but incident cases were associated with a relatively high share of complications. In other words, RSV infections in pregnancy are a rare event that may result in severe infections, with a relatively benign outcome. However, because of the inconsistent testing strategies, it is reasonable that a substantial share of cases may have been lost from the parent estimates, eventually impairing the reliability of our estimates. Therefore, the information presented here can hardly be considered definitive, and stress the opportunity for additional studies that, through a more consistent case definition and testing strategy, would help to identify the true burden of severe RSV infections for mother and child, eventually contributing to a better definition of potential costs and benefits of upcoming maternal vaccination strategies.
Author Contributions
Conceptualization, M.R.; data curation, S.C. and S.R.; formal analysis, M.R. and A.Z.; funding acquisition, S.C.; investigation, M.R., P.F., E.S. and S.R.; methodology, S.R.; resources, P.F.; software, M.R., S.C., A.Z. and E.S.; validation, E.S.; visualization, P.F., S.C. and A.Z.; writing—original draft, M.R. and S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request to the corresponding author.
Acknowledgments
The authors would like to thank. Francesca DE NARD for their valuable support during the design and writing of the present paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morris, J.A.; Blount, R.E.; Smadel, J.E. Recovery of Cytopathogenic Agent from Chimpanzees with Coryza. Proc. Soc. Exp. Biol. Med. 1956, 92, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Checcucci Lisi, G.; et al. Epidemiology and Prevention of Respiratory Syncytial Virus Infections in Children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef] [PubMed]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory Syncytial Virus in Influenza-like Illness Cases: Epidemiology and Molecular Analyses of Four Consecutive Winter Seasons (2014–2015/2017–2018) in Lombardy (Northern Italy). J. Med. Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2021, 222, S577–S583. [Google Scholar] [CrossRef] [Green Version]
- Openshaw, P.J.M.; Chiu, C.; Culley, F.J.; Johansson, C. Protective and Harmful Immunity to RSV Infection. Annu. Rev. Immunol. 2017, 35, 501–532. [Google Scholar] [CrossRef] [PubMed]
- Andeweg, S.P.; Schepp, R.M.; van de Kassteele, J.; Mollema, L.; Berbers, G.A.M.; van Boven, M. Population-Based Serology Reveals Risk Factors for RSV Infection in Children Younger than 5 Years. Sci. Rep. 2021, 11, 8953. [Google Scholar] [CrossRef] [PubMed]
- Mazur, N.I.; Martinón-Torres, F.; Baraldi, E.; Fauroux, B.; Greenough, A.; Heikkinen, T.; Manzoni, P.; Mejias, A.; Nair, H.; Papadopoulos, N.G.; et al. Lower Respiratory Tract Infection Caused by Respiratory Syncytial Virus: Current Management and New Therapeutics. Lancet Respir. Med. 2015, 3, 888–900. [Google Scholar] [CrossRef]
- Nair, H.; Theodoratou, E.; Rudan, I.; Nokes, D.J.; Ngama HND, M.; Munywoki, P.K.; Dherani, M.; Nair, H.; James Nokes, D.; Gessner, B.D.; et al. Global Burden of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children: A Systematic Review and Meta-Analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef] [Green Version]
- Leader, S.; Kohlhase, K. Respiratory Syncytial Virus-Coded Pediatric Hospitalizations, 1997 to 1999. Pediatr. Infect. Dis. J. 2002, 21, 629–661. [Google Scholar] [CrossRef]
- Leader, S.; Kohlhase, K.; Pearlman, M.H.; Williams, J.V.; Engle, W.A. Recent Trends in Severe Respiratory Syncytial Virus (RSV) among US Infants, 1997 to 2000. J. Pediatr. 2003, 143, S127–S132. [Google Scholar] [CrossRef]
- Palmer, L.; Hall, C.B.; Katkin, J.P.; Shi, N.; Masaquel, A.S.; McLaurin, K.K.; Mahadevia, P.J. Healthcare Costs within a Year of Respiratory Syncytial Virus among Medicaid Infants. Pediatr. Pulmonol. 2010, 45, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef]
- Shi, T.; Arnott, A.; Semogas, I.; Falsey, A.R.; Openshaw, P.; Wedzicha, J.A.; Campbell, H.; Nair, H. The Etiological Role of Common Respiratory Viruses in Acute Respiratory Infections in Older Adults: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 222, S563–S569. [Google Scholar] [CrossRef] [PubMed]
- Mosalli, R.; Alqarni, S.A.; Khayyat, W.W.; Alsaidi, S.T.; Almatrafi, A.S.; Bawakid, A.S.; Paes, B. Respiratory Syncytial Virus Nosocomial Outbreak in Neonatal Intensive Care: A Review of the Incidence, Management, and Outcomes. Am. J. Infect. Control, 2021; epub ahead of print. [Google Scholar] [CrossRef]
- Nourbakhsh, S.; Shoukat, A.; Zhang, K.; Poliquin, G.; Halperin, D.; Sheffield, H.; Halperin, S.A.; Langley, J.M.; Moghadas, S.M. Effectiveness and Cost-Effectiveness of RSV Infant and Maternal Immunization Programs: A Case Study of Nunavik, Canada. EClinicalMedicine 2021, 41, 101141. [Google Scholar] [CrossRef]
- Paes, B.A.; Frcpc, M.; Mitchell, I.; Mb Frcpc, M.A.; Banerji, A.; Mph, M.D.; Lanctôt, K.L.; Langley, J.M.; Bosco, D.; Paes, A. A decade of respiratory syncytial virus epidemiology and prophylaxis: Translating evidence into everyday clinical practice case presentation. Can. Respir. J. 2011, 18, e10–e19. [Google Scholar] [CrossRef] [PubMed]
- Arriola, C.S.; Kim, L.; Langley, G.; Anderson, E.J.; Openo, K.; Martin, A.M.; Lynfield, R.; Bye, E.; Como-Sabetti, K.; Reingold, A.; et al. Estimated Burden of Community-Onset Respiratory Syncytial Virus-Associated Hospitalizations among Children Aged < 2 Years in the United States, 2014–2015. J. Pediatr. Infect. Dis. Soc. 2020, 9, 587–595. [Google Scholar] [CrossRef]
- Griffiths, C.; Drews, S.J.; Marchant, D.J. Respiratory Syncytial Virus: Infection, Detection, and New Options for Prevention and Treatment. Clin. Microbiol. Rev. 2017, 30, 277–319. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, I.; Li, A.; Bjornson, C.L.; Lanctot, K.L.; Paes, B.A. Respiratory Syncytial Virus Immunoprophylaxis with Palivizumab: 12-Year Observational Study of Usage and Outcomes in Canada. Am. J. Perinatol. 2021; online ahead of print. [Google Scholar] [CrossRef]
- Viguria, N.; Navascués, A.; Juanbeltz, R.; Echeverría, A.; Ezpeleta, C.; Castilla, J. Effectiveness of Palivizumab in Preventing Respiratory Syncytial Virus Infection in High-Risk Children. Hum. Vaccines Immunother. 2021, 17, 1867–1872. [Google Scholar] [CrossRef]
- Chida-Nagai, A.; Sato, H.; Sato, I.; Shiraishi, M.; Sasaki, D.; Izumi, G.; Yamazawa, H.; Cho, K.; Manabe, A.; Takeda, A. Risk Factors for Hospitalisation Due to Respiratory Syncytial Virus Infection in Children Receiving Prophylactic Palivizumab. Eur. J. Pediatr. 2022, 181, 539–547. [Google Scholar] [CrossRef]
- Zylbersztejn, A.; Almossawi, O.; Gudka, N.; Tompsett, D.; de Stavola, B.; Standing, J.F.; Smyth, R.; Hardelid, P. Access to Palivizumab among Children at High Risk of Respiratory Syncytial Virus Complications in English Hospitals. Br. J. Clin. Pharmacol. 2022, 88, 1246–1257. [Google Scholar] [CrossRef]
- Batista, J.D.L.; Ferreira, M.A.P.; Xavier, C.D.S.; de Souza, I.T.A.; Cruz, L.N.; Polanczyk, C.A. A Post-Incorporation Study on the Use of Palivizumab in the Brazilian Public Health System. Rev. Inst. Med. Trop. Sao Paulo 2021, 63, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hampp, C.; Kauf, T.L.; Saidi, A.S.; Winterstein, A.G. Cost-Effectiveness of Respiratory Syncytial Virus Prophylaxis in Various Indications. Arch. Pediatr. Adolesc. Med. 2011, 165, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, M.P.; Yuan, Y.; Takas, T.; Domachowske, J.B.; Madhi, S.A.; Manzoni, P.; Simões, E.A.F.; Esser, M.T.; Khan, A.A.; Dubovsky, F.; et al. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. N. Engl. J. Med. 2020, 383, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Hammitt, L.L.; Dagan, R.; Yuan, Y.; Baca Cots, M.; Bosheva, M.; Madhi, S.A.; Muller, W.J.; Zar, H.J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N. Engl. J. Med. 2022, 386, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Domachowske, J.; Madhi, S.A.; Simões, E.A.F.; Atanasova, V.; Cabañas, F.; Furuno, K.; Garcia-Garcia, M.L.; Grantina, I.; Nguyen, K.A.; Brooks, D.; et al. Safety of Nirsevimab for RSV in Infants with Heart or Lung Disease or Prematurity. N. Engl. J. Med. 2022, 386, 892–894. [Google Scholar] [CrossRef] [PubMed]
- Voirin, N.; Virlogeux, V.; Demont, C.; Kieffer, A. Potential Impact of Nirsevimab on RSV Transmission and Medically Attended Lower Respiratory Tract Illness Caused by RSV: A Disease Transmission Model. Infect. Dis. Ther. 2021, 11, 277–292. [Google Scholar] [CrossRef]
- Debes, S.; Haug, J.B.; de Blasio, B.F.; Jonassen, C.M.; Dudman, S.G. Etiology of Viral Respiratory Tract Infections in Hospitalized Adults, and Evidence of the High Frequency of Prehospitalization Antibiotic Treatment in Norway. Health Sci. Rep. 2021, 4, e403. [Google Scholar] [CrossRef]
- Obolski, U.; Kassem, E.; Na’amnih, W.; Tannous, S.; Kagan, V.; Muhsen, K. Unnecessary Antibiotic Treatment of Children Hospitalized with RSV-Bronchiolitis: Risk Factors and Prescription Patterns. J. Glob. Antimicrob. Resist. 2021, 27, 303–308. [Google Scholar] [CrossRef]
- Madhi, S.A.; Polack, F.P.; Piedra, P.A.; Munoz, F.M.; Trenholme, A.A.; Simões, E.A.F.; Swamy, G.K.; Agrawal, S.; Ahmed, K.; August, A.; et al. Respiratory Syncytial Virus Vaccination during Pregnancy and Effects in Infants. N. Engl. J. Med. 2020, 383, 426–439. [Google Scholar] [CrossRef]
- Phijffer, E.W.E.M.; Bont, L.J. Are We Ready for Maternal Respiratory Syncytial Virus Vaccination? J. Infect. Dis. 2021, jiab613. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Falsey, A.R.; Scott, D.A.; Gurtman, A.; Zareba, A.M.; Jansen, K.U.; Gruber, W.C.; Dormitzer, P.R.; Swanson, K.A.; Radley, D.; et al. A Randomized Phase 1/2 Study of a Respiratory Syncytial Virus Prefusion F Vaccine. J. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Scheltema, N.M.; Kavelaars, X.M.; Thorburn, K.; Hennus, M.P.; van Woensel, J.B.; van der Ent, C.K.; Borghans, J.A.M.; Bont, L.J.; Drylewicz, J. Potential Impact of Maternal Vaccination on Life-Threatening Respiratory Syncytial Virus Infection during Infancy. Vaccine 2018, 36, 4693–4700. [Google Scholar] [CrossRef]
- Buchwald, A.G.; Graham, B.S.; Traore, A.; Haidara, F.C.; Chen, M.; Morabito, K.; Lin, B.C.; Sow, S.O.; Levine, M.M.; Pasetti, M.F.; et al. Respiratory Syncytial Virus (RSV) Neutralizing Antibodies at Birth Predict Protection from RSV Illness in Infants in the First 3 Months of Life. Clin. Infect. Dis. 2021, 73, e4421–e4427. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Wang, L.; Falsey, A.R.; Qiu, X.; Corbett, A.; Holden-Wiltse, J.; Mariani, T.J.; Topham, D.J.; Caserta, M.T. Virus-Specific Antibody, Viral Load, and Disease Severity in Respiratory Syncytial Virus Infection. J. Infect. Dis. 2018, 218, 208–217. [Google Scholar] [CrossRef]
- Groothuis, J.R.; Simoes, E.A.; Levin, M.J.; Hall, C.B.; Long, C.E.; Rodriguez, W.J.; Arrobio, J.; Meissner, H.C.; Fulton, D.R.; Welliver, R.C.; et al. Prophylactic Administration of Respiratory Syncytial Virus Immune Globulin to High-Risk Infants and Young Children. N. Eng. J. Med. 1993, 329, 1524–1530. [Google Scholar] [CrossRef]
- Glezen, P.W.; Paredes, A.; Allison, J.E.; Taber, L.H.; Frank, A.L. Risk of Respiratory Syncytial Virus Infection for Infants from Low-Income Families in Relationship to Age, Sex, Ethnic Group, and Maternal Antibody Level. J. Pediatr. 1981, 98, 708–715. [Google Scholar] [CrossRef]
- Amirthalingam, G.; Andrews, N.; Campbell, H.; Ribeiro, S.; Kara, E.; Donegan, K.; Fry, N.K.; Miller, E.; Ramsay, M. Effectiveness of Maternal Pertussis Vaccination in England: An Observational Study. Lancet 2014, 384, 1521–1528. [Google Scholar] [CrossRef]
- Gkentzi, D.; Katsakiori, P.; Marangos, M.; Hsia, Y.; Amirthalingam, G.; Heath, P.T.; Ladhani, S. Maternal Vaccination against Pertussis: A Systematic Review of the Recent Literature. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F456–F463. [Google Scholar] [CrossRef]
- Fell, D.B.; Bhutta, Z.A.; Hutcheon, J.A.; Karron, R.A.; Knight, M.; Kramer, M.S.; Monto, A.S.; Swamy, G.K.; Ortiz, J.R.; Savitz, D.A. Report of the WHO Technical Consultation on the Effect of Maternal Influenza and Influenza Vaccination on the Developing Fetus: Montreal, Canada, September 30–October 1, 2015. Vaccine 2017, 35, 2279–2287. [Google Scholar] [CrossRef]
- Buchy, P.; Badur, S.; Kassianos, G.; Preiss, S.; Tam, J.S. Vaccinating Pregnant Women against Influenza Needs to Be a Priority for All Countries: An Expert Commentary. Int. J. Infect. Dis. 2020, 92, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunatilaka, A.; Giles, M.L. Maternal RSV Vaccine Development. Where to from Here? Hum. Vaccines Immunother. 2021, 17, 4542–4548. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, S.M.; Dotters-Katz, S.; Heine, R.P.; Grotegut, C.A.; Swamy, G.K. Maternal Effects of Respiratory Syncytial Virus Infection during Pregnancy. Emerg. Infect. Dis. 2015, 21, 1951–1955. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Panagiotakopoulos, L.; Weintraub, E.S.; Sy, L.S.; Glenn, S.C.; Tseng, H.F.; McNeil, M.M. Adverse Outcomes in Pregnant Women Hospitalized with Respiratory Syncytial Virus Infection: A Case Series. Clin. Infect. Dis. 2021, 72, 138–140. [Google Scholar] [CrossRef]
- Regan, A.K.; Klein, N.P.; Langley, G.; Drews, S.J.; Buchan, S.; Ball, S.; Kwong, J.C.; Naleway, A.; Thompson, M.; Wyant, B.E.; et al. Respiratory Syncytial Virus Hospitalization during Pregnancy in 4 High-Income Countries, 2010–2016. Clin. Infect. Dis. 2018, 67, 1915–1918. [Google Scholar] [CrossRef]
- Manti, S.; Leonardi, S.; Rezaee, F.; Harford, T.; Perez, M.K.; Piedimonte, G.; Nunes, M.C. Effects of Vertical Transmission of Respiratory Viruses to the Offspring. Front. Immunol. 2022, 13, 853009. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. A Trial to Evaluate the Efficacy and Safety of RSVpreF in Infants Born to Women Vaccinated During Pregnancy; The United States National Library of Medicine: Bethesda, MD, USA, 2022.
- ClinicalTrials.gov. A Phase III Double-Blind Study to Assess Safety and Efficacy of an RSV Maternal Unadjuvanted Vaccine, in Pregnant Women and Infants Born to Vaccinated Mothers (GRACE); The United States National Library of Medicine: Bethesda, MD, USA, 2022.
- Chaw, L.; Kamigaki, T.; Burmaa, A.; Urtnasan, C.; Od, I.; Nyamaa, G.; Nymadawa, P.; Oshitani, H. Burden of Influenza and Respiratory Syncytial Virus Infection in Pregnant Women and Infants under 6 Months in Mongolia: A Prospective Cohort Study. PLoS ONE 2016, 11, e0148421. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.Y.; Katz, J.; Tielsch, J.; Khatry, S.K.; Shrestha, L.; LeClerq, S.C.; Magaret, A.; Kuypers, J.; Steinhoff, M.C.; Englund, J.A. Clinical Presentation and Birth Outcomes Associated with Respiratory Syncytial Virus Infection in Pregnancy. PLoS ONE 2016, 11, e0152015. [Google Scholar] [CrossRef]
- Hause, A.M.; Avadhanula, V.; Maccato, M.L.; Pinell, P.M.; Bond, N.; Santarcangelo, P.; Ferlic-Stark, L.; Ye, X.; Iwuchukwu, O.; Maurer, L.; et al. Clinical Characteristics and Outcomes of Respiratory Syncytial Virus Infection in Pregnant Women. Vaccine 2019, 37, 3464–3471. [Google Scholar] [CrossRef]
- Madhi, S.A.; Cutland, C.L.; Downs, S.; Jones, S.; van Niekerk, N.; Simoes, E.A.F.; Nunes, M.C. Burden of Respiratory Syncytial Virus Infection in South African Human Immunodeficiency Virus (HIV)-Infected and HIV-Uninfected Pregnant and Postpartum Women: A Longitudinal Cohort Study. Clin. Infect. Dis. 2018, 66, 1658–1665. [Google Scholar] [CrossRef] [Green Version]
- Hurley, L.P.; Allison, M.A.; Kim, L.; O’Leary, S.T.; Crane, L.A.; Brtnikova, M.; Beaty, B.L.; Allen, K.E.; Poser, S.; Lindley, M.C.; et al. Primary Care Physicians’ Perspectives on Respiratory Syncytial Virus (RSV) Disease in Adults and a Potential RSV Vaccine for Adults. Vaccine 2019, 37, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Long, C.E.; Schnabel, K.C. Respiratory Syncytial Virus Infections in Previously Healthy Working Adults. Clin. Infect. Dis. 2001, 33, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Pastula, S.T.; Hackett, J.; Coalson, J.; Jiang, X.; Villafana, T.; Ambrose, C.; Fryzek, J. Hospitalizations for Respiratory Syncytial Virus Among Adults in the United States, 1997–2012. Open Forum Infect. Dis. 2017, 4, ofw270. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Hill-Ricciuti, A.; Branche, A.R.; Sieling, W.D.; Saiman, L.; Walsh, E.E.; Phillips, M.; Falsey, A.R.; Finelli, L. Cost Determinants among Adults Hospitalized with Respiratory Syncytial Virus in the United States, 2017–2019. Influenza Other Respir. Viruses 2021, 16, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Hause, A.M.; Avadhanula, V.; Maccato, M.L.; Pinell, P.M.; Bond, N.; Santarcangelo, P.; Ferlic-Stark, L.; Munoz, F.M.; Piedra, P.A. A Cross-Sectional Surveillance Study of the Frequency and Etiology of Acute Respiratory Illness Among Pregnant Women. J. Infect. Dis. 2018, 218, 528–535. [Google Scholar] [CrossRef]
- Li, X.; Bilcke, J.; Vázquez Fernández, L.; Bont, L.; Willem, L.; Wisløff, T.; Jit, M.; Beutels, P.; Beutels, P.; Bont, L.; et al. Cost-Effectiveness of Respiratory Syncytial Virus Disease Prevention Strategies: Maternal Vaccine Versus Seasonal or Year-Round Monoclonal Antibody Program in Norwegian Children. J. Infect. Dis. 2022, jiac064. [Google Scholar] [CrossRef]
- Hodgson, D.; Pebody, R.; Panovska-Griffiths, J.; Baguelin, M.; Atkins, K.E. Evaluating the next Generation of RSV Intervention Strategies: A Mathematical Modelling Study and Cost-Effectiveness Analysis. BMC Med. 2020, 18, 348. [Google Scholar] [CrossRef]
- Laufer, R.S.; Driscoll, A.J.; Baral, R.; Buchwald, A.G.; Campbell, J.D.; Coulibaly, F.; Diallo, F.; Doumbia, M.; Galvani, A.P.; Haidara, F.C.; et al. Cost-Effectiveness of Infant Respiratory Syncytial Virus Preventive Interventions in Mali: A Modeling Study to Inform Policy and Investment Decisions. Vaccine 2021, 39, 5037–5045. [Google Scholar] [CrossRef]
- Sperling, R.S.; Riley, L.E. Immunization and Emerging Infections Expert Work Group Influenza Vaccination, Pregnancy Safety, and Risk of Early Pregnancy Loss. Obstet. Gynecol. 2018, 131, 799–802. [Google Scholar] [CrossRef]
- Fell, D.B.; Azziz-Baumgartner, E.; Baker, M.G.; Batra, M.; Beauté, J.; Beutels, P.; Bhat, N.; Bhutta, Z.A.; Cohen, C.; de Mucio, B.; et al. Influenza Epidemiology and Immunization during Pregnancy: Final Report of a World Health Organization Working Group. Vaccine 2017, 35, 5738–5750. [Google Scholar] [CrossRef]
- Karlsson, E.A.; Marcelin, G.; Webby, R.J.; Schultz-Cherry, S. Review on the Impact of Pregnancy and Obesity on Influenza Virus Infection. Influenza Other Respir. Viruses 2012, 6, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Capozzi, V.A.; Volpi, L. Knowledge, Attitudes, Beliefs and Practices of Obstetrics-Gynecologists on Seasonal Influenza and Pertussis Immunizations in Pregnant Women: Preliminary Results from North-Western Italy. Minerva Ginecol. 2019, 71, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Ranzieri, S. Respiratory Syncytial Virus: Knowledge, Attitudes and Beliefs of General Practitioners from North-Eastern Italy (2021). Pediatr. Rep. 2022, 14, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Giles, M.L.; Buttery, J.; Davey, M.A.; Wallace, E. Pregnant Women’s Knowledge and Attitude to Maternal Vaccination Including Group B Streptococcus and Respiratory Syncytial Virus Vaccines. Vaccine 2019, 37, 6743–6749. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.R.; Calvert, A.; Metz, J.; Kilich, E.; Macleod, R.; Beadon, K.; Heath, P.T.; Khalil, A.; Finn, A.; Snape, M.D.; et al. Attitudes of Pregnant Women and Healthcare Professionals Toward Clinical Trials and Routine Implementation of Antenatal Vaccination Against Respiratory Syncytial Virus: A Multicenter Questionnaire Study. Pediatr. Infect. Dis. J. 2019, 38, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Auvinen, R.; Syrjänen, R.; Ollgren, J.; Nohynek, H.; Skogberg, K. Clinical Characteristics and Population-Based Attack Rates of Respiratory Syncytial Virus versus Influenza Hospitalizations among Adults—An Observational Study. Influenza Other Respir. Viruses, 2021; online ahead of print. [Google Scholar] [CrossRef]
- Rose, E.B.; Wheatley, A.; Langley, G.; Gerber, S.; Haynes, A. Amber Morbidity and Mortality Weekly Report Respiratory Syncytial Virus Seasonality-United States, 2014–2017. Morb. Mortal. Wkly. Rep. 2018, 67, 71–76. [Google Scholar] [CrossRef]
- Janet, S.; Broad, J.; Snape, M.D. Respiratory Syncytial Virus Seasonality and Its Implications on Prevention Strategies. Hum. Vaccines Immunother. 2018, 14, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Yassine, H.M.; Sohail, M.U.; Younes, N.; Nasrallah, G.K. Systematic Review of the Respiratory Syncytial Virus (RSV) Prevalence, Genotype Distribution, and Seasonality in Children from the Middle East and North Africa (MENA) Region. Microorganisms 2020, 8, 713. [Google Scholar] [CrossRef]
- Barbati, F.; Moriondo, M.; Pisano, L.; Calistri, E.; Lodi, L.; Ricci, S.; Giovannini, M.; Canessa, C.; Indolfi, G.; Azzari, C. Epidemiology of Respiratory Syncytial Virus-Related Hospitalization over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution before Vaccine Introduction. Vaccines 2020, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Tramuto, F.; Maida, C.M.; di Naro, D.; Randazzo, G.; Vitale, F.; Restivo, V.; Costantino, C.; Amodio, E.; Casuccio, A.; Graziano, G.; et al. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines 2021, 9, 1334. [Google Scholar] [CrossRef]
- Atamna, A.; Babich, T.; Froimovici, D.; Yahav, D.; Sorek, N.; Ben-Zvi, H.; Leibovici, L.; Bishara, J.; Avni, T. Morbidity and Mortality of Respiratory Syncytial Virus Infection in Hospitalized Adults: Comparison with Seasonal Influenza. Int. J. Infect. Dis. 2021, 103, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Irving, W.L.; James, D.K.; Stephenson, T.; Laing, P.; Jameson, C.; Oxford, J.S.; Chakraverty, P.; Brown, D.W.; Coon, A.C.; Zambon, M.C. Influenza Virus Infection in the Second and Third Trimesters of Pregnancy a Clinical and Seroepidemiological Study. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 1282–1289. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R.; Director Harold Jaffe, M.W.; Stephens, J.W.; Thacker, S.B.; Spriggs Terraye M Starr, S.R.; Doan, Q.M.; Phyllis King, M.H.; Roper, W.L.; Holtzman, D.; John Iglehart, G.K.; et al. Prevention and Control of Influenza with Vaccines Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Morb. Mortal. Wkly. Rep. 2009, 59, 1–62. [Google Scholar]
- Dawood, F.S.; Kittikraisak, W.; Patel, A.; Rentz Hunt, D.; Suntarattiwong, P.; Wesley, M.G.; Thompson, M.G.; Soto, G.; Mundhada, S.; Arriola, C.S.; et al. Incidence of Influenza during Pregnancy and Association with Pregnancy and Perinatal Outcomes in Three Middle-Income Countries: A Multisite Prospective Longitudinal Cohort Study. Lancet Infect. Dis. 2021, 21, 97–106. [Google Scholar] [CrossRef]
- Esterhuizen, T.M.; Thabane, L. Con: Meta-Analysis: Some Key Limitations and Potential Solutions. Nephrol. Dial. Transplant. 2016, 31, 882–885. [Google Scholar] [CrossRef] [Green Version]
- Imrey, P.B. Limitations of Meta-Analyses of Studies with High Heterogeneity. JAMA Netw. Open 2020, 3, e1919325. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.Y.; Tielsch, J.; Katz, J.; Magaret, A.S.; Khatry, S.; LeClerq, S.C.; Shrestha, L.; Kuypers, J.; Steinhoff, M.C.; Englund, J.A. Transplacental Transfer of Maternal Respiratory Syncytial Virus (RSV) Antibody and Protection against RSV Disease in Infants in Rural Nepal. J. Clin. Virol. 2017, 95, 90–95. [Google Scholar] [CrossRef]
- Calderaro, A.; de Conto, F.; Buttrini, M.; Piccolo, G.; Montecchini, S.; Maccari, C.; Martinelli, M.; di Maio, A.; Ferraglia, F.; Pinardi, F.; et al. Human Respiratory Viruses, Including SARS-CoV-2, Circulating in the Winter Season 2019–2020 in Parma, Northern Italy. Int. J. Infect. Dis. 2021, 102, 79–84. [Google Scholar] [CrossRef]
- Sherman, A.C.; Babiker, A.; Sieben, A.J.; Pyden, A.; Steinberg, J.; Kraft, C.S.; Koelle, K.; Kanjilal, S. The Effect of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Mitigation Strategies on Seasonal Respiratory Viruses: A Tale of 2 Large Metropolitan Centers in the United States. Clin. Infect. Dis. 2021, 72, E154–E157. [Google Scholar] [CrossRef]
- Kuitunen, I.; Artama, M.; Mäkelä, L.; Backman, K.; Heiskanen-Kosma, T.; Renko, M. Effect of Social Distancing Due to the COVID-19 Pandemic on the Incidence of Viral Respiratory Tract Infections in Children in Finland during Early 2020. Pediatr. Infect. Dis. J. 2020, 39, E423–E427. [Google Scholar] [CrossRef]
- van Brusselen, D.; de Troeyer, K.; ter Haar, E.; vander Auwera, A.; Poschet, K.; van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; van Herendael, B.; et al. Bronchiolitis in COVID-19 Times: A Nearly Absent Disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 Public Health Measures and Respiratory Syncytial Virus. Lancet Child Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef]
- Hatter, L.; Eathorne, A.; Hills, T.; Bruce, P.; Beasley, R. Respiratory Syncytial Virus: Paying the Immunity Debt with Interest. Lancet Child Adolesc. Health 2021, 5, e44–e45. [Google Scholar] [CrossRef]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, E2829–E2830. [Google Scholar] [CrossRef]
- Foley, D.A.; Phuong, L.K.; Peplinski, J.; Lim, S.M.; Lee, W.H.; Farhat, A.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; et al. Examining the Interseasonal Resurgence of Respiratory Syncytial Virus in Western Australia. Arch. Dis. Child. 2021, 107, e1–e7. [Google Scholar] [CrossRef]
- Varela, F.H.; Scotta, M.C.; Polese-Bonatto, M.; Sartor, I.T.S.; Ferreira, C.F.; Fernandes, I.R.; Zavaglia, G.O.; de Almeida, W.A.F.; Arakaki-Sanchez, D.; Pinto, L.A.; et al. Absence of Detection of RSV and Influenza during the COVID-19 Pandemic in a Brazilian Cohort: Likely Role of Lower Transmission in the Community. J. Glob. Health 2021, 11, 05007. [Google Scholar] [CrossRef]
- Ippolito, G.; la Vecchia, A.; Umbrello, G.; di Pietro, G.; Bono, P.; Scalia, S.; Pinzani, R.; Tagliabue, C.; Bosis, S.; Agostoni, C.; et al. Disappearance of Seasonal Respiratory Viruses in Children Under Two Years Old During COVID-19 Pandemic: A Monocentric Retrospective Study in Milan, Italy. Front. Pediatr. 2021, 9, 721005. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N.; Ujiie, M. Resurgence of Respiratory Syncytial Virus Infections during Covid-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration; U.S. Department of Health and Human Services: Washington, DC, USA, 2019.
- Eick, S.M.; Goin, D.E.; Chartres, N.; Lam, J.; Woodruff, T.J. Assessing Risk of Bias in Human Environmental Epidemiology Studies Using Three Tools: Different Conclusions from Different Tools. Syst. Rev. 2020, 9, 249. [Google Scholar] [CrossRef]
Figure 1.
Flow chart for studies included in the systematic review and meta-analysis.

Figure 2.
Summary of risk of bias assessment (Note: D1: Possibility of selection bias; D2: Exposure assessment; D3: Outcome assessment; D4: Confounding; D5: Reporting bias; D6: Other bias). (a) detailed report by single study [46,51,52,53,54], (b) summary report.

Figure 3.
Incidence of RSV infections (a) among sampled pregnancies and (b) among cases of respiratory tract infections (RTI) in sampled pregnancies. A pooled incidence of 0.221 cases per 100 pregnancies (95%CI 0.045 to 1.081) and 2.532 per 100 RTI episodes (95%CI 1.218 to 5.189) was identified. In both cases, estimates were affected by substantial heterogeneity (I2 = 99% and I2 = 86%, respectively).
Figure 3.
Incidence of RSV infections (a) among sampled pregnancies and (b) among cases of respiratory tract infections (RTI) in sampled pregnancies. A pooled incidence of 0.221 cases per 100 pregnancies (95%CI 0.045 to 1.081) and 2.532 per 100 RTI episodes (95%CI 1.218 to 5.189) was identified. In both cases, estimates were affected by substantial heterogeneity (I2 = 99% and I2 = 86%, respectively).

Figure 4.
Funnel plots for studies included in the meta-analysis (a). Despite the reduced number of included studies, visual inspection suggested substantial evidence of publication bias for both subgroups, but this was substantially rejected by Egger test (1.07, df = 4, p-value = 0.361). On the other hand, in radial plots (b), the studies were substantially scattered across the regression line, suggesting no substantial small-study effect.
Figure 4.
Funnel plots for studies included in the meta-analysis (a). Despite the reduced number of included studies, visual inspection suggested substantial evidence of publication bias for both subgroups, but this was substantially rejected by Egger test (1.07, df = 4, p-value = 0.361). On the other hand, in radial plots (b), the studies were substantially scattered across the regression line, suggesting no substantial small-study effect.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary description of individual studies.
| Reference | Year | Settings | Study Design | Target Population | RSV Sampling |
|---|---|---|---|---|---|
| Chaw et al. [51] | 2016 | Mongolia 2013–2015 | Prospective study on influenza-like illnesses (ILI) and severe acute respiratory infections (sARI) in the semirural district of Baganuur. Periodic follow-up (1 call every 2 to 5 days) in order to catch ILI episodes. | Pregnant women with ILI and sARI | Reported ILI and sARI |
| Chu et al. [52] | 2016 | Nepal 2011–2014 | Prospective study performed during a randomized controlled trial on maternal influenza immunization. | Pregnant women in the second trimester of pregnancy. | Reported or measured fever (>38 °C) with at least one symptom among cough, myalgia, sore throat, or rhinorrhea. |
| Hause et al. [53] | 2019 | USA (Texas) 2015–2016 | Cross-sectional surveillance study. | Outpatients from an outpatient obstetric and gynecologic clinic. Pregnant women in 2nd or 3rd trimester with diagnosis of sARI in the 7 days before the visit. | Reported sARI |
| Hause et al. [46] | 2021 | USA (California) 2010–2017 | Case series, retrospective study. | Pregnant women having live births outcomes at Kaiser Permanente in Southern California. | Unclear rationale. |
| Madhi et al. [54] | 2018 | South Africa 2011–2012 | Retrospective study on three cohorts of pregnant women: 2 HIV-uninfected and 1 HIV-infected that were initially defined for a randomized controlled trial on maternal influenza immunization. | Women developing any respiratory symptoms during the follow-up. | Women complaining symptoms compatible with the diagnosis of ILI (i.e., presence of fever (≥38 °C on oral measurements) or chills/rigors or feeling feverish in past <7 days, and one of the following for <7 days duration: (i) cough/sore throat/pharyngitis, or (ii) muscle aches/joint aches/headaches, or (iii) chest pain while breathing/feeling short of breath/difficulty breathing) |
Table 2.
Characteristics of the studies included in the quantitative analysis (Note: RSV = Respiratory Syncytial Virus; RTI = Respiratory Tract Infection).
Table 2.
Characteristics of the studies included in the quantitative analysis (Note: RSV = Respiratory Syncytial Virus; RTI = Respiratory Tract Infection).
| Reference | Pregnancies (No.) | RTI (No./Total, %) | RSV (No./RTI, %) | Hospitalizations (No./RSV, %) | Pneumonia (No./RSV, %) | Miscarriage (No./RSV, %) | Preterm (No./RSV, %) | Low Birth Weight (No./RSV, %) |
|---|---|---|---|---|---|---|---|---|
| Chaw et al. [51] | 1260 | 160, 12.7% | 4, 2.5% | NA | NA | NA | NA | NA |
| Chu et al. [52] | 3693 | 733, 19.8% | 7, 1.0% | 0, - | 0, - | 0, - | 1, 14.3% | 2, 28.6% |
| Hause et al. [53] | 500 | 65, 13.0% | 8, 12.3% | 1, 12.5% | 0, - | 0, - | 0, - | 0, - |
| Hause et al. [46] | 27,5349 | 1057, 0.4% | 25, 2.4% | 10, 40.0% | 4, 16.0% | 0, - | 1, 4.0% | 1, 4.0% |
| Madhi et al. [54] | 2116 | 932, 44.0% | 18, 1.9% | 0, - | 2, 11.1% | 0, - | 2, 11.1% | 1, 5.6% |
Table 3.
Summary of collected outcomes of RSV cases in pregnancies. Data on studies reporting on maternal episodes in both hospitalized and non-hospitalized women were summarized [51,53,54].
| Outcome | No. | % (No./6309 Pregnancies) | % (No./33 RSV Cases) |
|---|---|---|---|
| Pneumonia in mother | 2 | 0.03% | 6.1% |
| Deaths in mother | 0 | - | - |
| Miscarriage | 0 | - | - |
| Preterm delivery | 3 | 0.04% | 9.1% |
| Low Birth Weight | 3 | 0.04% | 9.1% |
Table 4.
PICO worksheet (note: RSV = respiratory syncytial virus).
| Item | Definition |
|---|---|
| Population of interest | Pregnant women |
| Investigated result | Prevalence of RSV infections |
| Control | Pregnancies negative for RSV infections |
| Outcome | Complications for mother and infant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Riccò, M.; Ferraro, P.; Corrado, S.; Zaniboni, A.; Satta, E.; Ranzieri, S. Respiratory Syncytial Virus in Pregnant Women: Systematic Review and Meta-Analysis. Women 2022, 2, 147-160. https://doi.org/10.3390/women2020016
AMA Style
Riccò M, Ferraro P, Corrado S, Zaniboni A, Satta E, Ranzieri S. Respiratory Syncytial Virus in Pregnant Women: Systematic Review and Meta-Analysis. Women. 2022; 2(2):147-160. https://doi.org/10.3390/women2020016
Chicago/Turabian StyleRiccò, Matteo, Pietro Ferraro, Silvia Corrado, Alessandro Zaniboni, Elia Satta, and Silvia Ranzieri. 2022. "Respiratory Syncytial Virus in Pregnant Women: Systematic Review and Meta-Analysis" Women 2, no. 2: 147-160. https://doi.org/10.3390/women2020016