
Successful Treatment of Central Nervous System Lymphoma with Combination Therapy of Nimustine and Prednisolone in Two Dogs

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Case Presentation
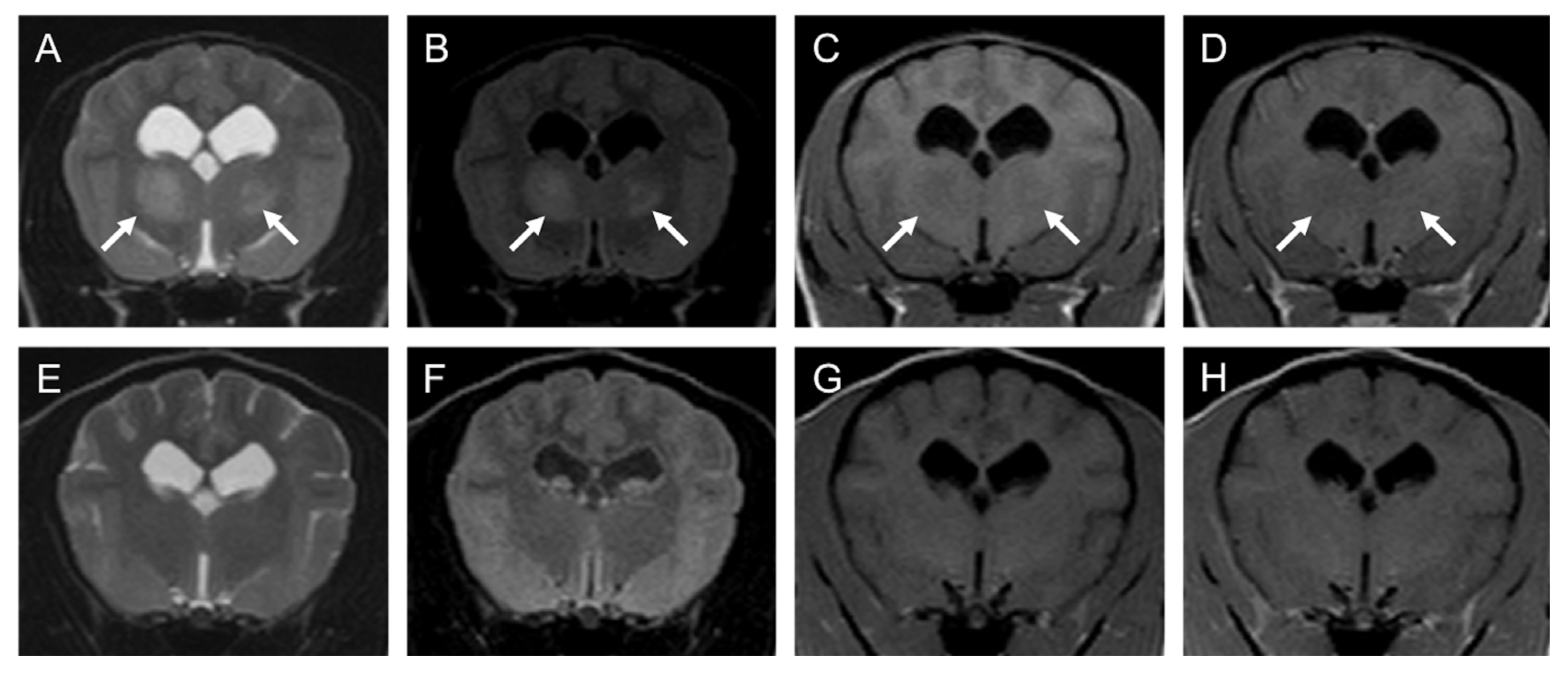
2.1. Case 1
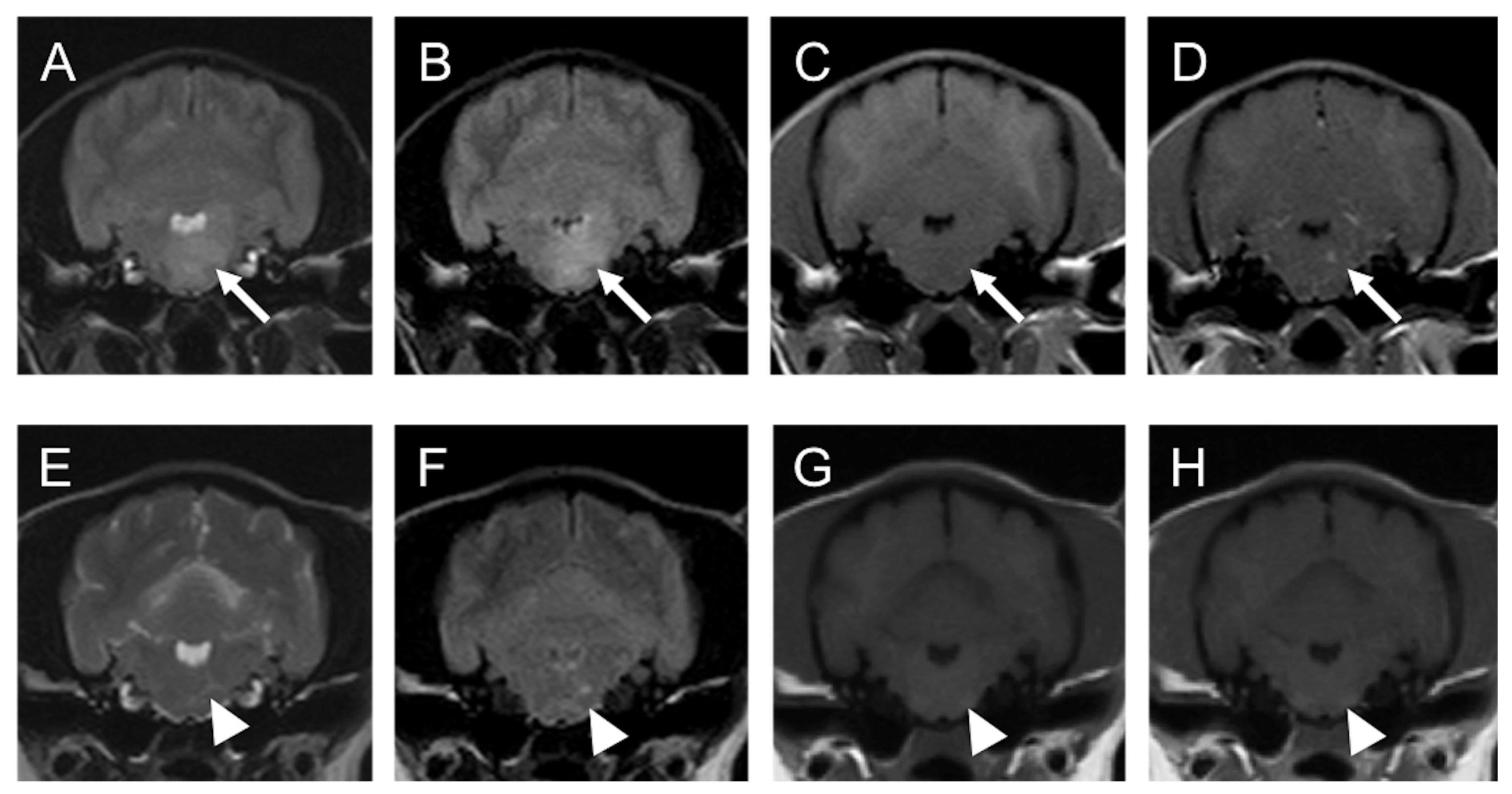
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dobson, J.M.; Samuel, S.; Milstein, H.; Rogers, K.; Wood, J.L. Canine neoplasia in the UK: Estimates of incidence rates from a population of insured dogs. J. Small Anim. Pract. 2002, 43, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Teske, E. Canine malignant lymphoma: A review and comparison with human non-hodgkin’s lymphoma. Vet. Q. 1994, 16, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Zandvliet, M. Canine lymphoma: A review. Vet. Q. 2016, 36, 76–104. [Google Scholar] [CrossRef]
- LaRue, M.K.; Taylor, A.R.; Back, A.R.; Lindley, S.E.; Boudreaux, B.L.; Almond, G.T.; Shores, A.; Brawner, W.R.; Smith, A.N. Central nervous system lymphoma in 18 dogs (2001 to 2015). J. Small. Anim. Pract. 2018, 59, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Rossmeisl, J.H.; Pancotto, T.E. Tumors of the Nervous System. Withrow and MacEwen’s Small Animal Clinical Oncology, 6th ed.; W.B. Saunders: Philadelphia, PA, USA, 2019; pp. 657–674. [Google Scholar]
- Vandevelde, M. Brain tumors in domestic animals: An overview. In Proceedings of the Conference on Brain Tumors in Man and Animals, Research Triangle Park, NC, USA, 5–6 September 1984. [Google Scholar]
- Dorn, C.R.; Taylor, D.O.; Schneider, R.; Hibbard, H.H.; Klauber, M.R. Survey of animal neoplasms in Alameda and Contra Costa Counties, California. II. Cancer morbidity in dogs and cats from Alameda County. J. Natl. Cancer Inst. 1968, 40, 307–318. [Google Scholar]
- McGrath, J.T. Intracranial Pathology of the dog. Acta Neuropathol. 1962, 1 (Suppl. 1), 3–4. [Google Scholar]
- Song, R.B.; Vite, C.H.; Bradley, C.W.; Cross, J.R. Postmortem evaluation of 435 cases of intracranial neoplasia in dogs and relationship of neoplasm with breed, age, and body weight. J. Vet. Intern. Med. 2013, 27, 1143–1152. [Google Scholar] [CrossRef]
- Snyder, J.M.; Shofer, F.S.; Van Winkle, T.J.; Massicotte, C. Canine intracranial primary neoplasia: 173 cases (1986–2003). J. Vet. Intern. Med. 2006, 20, 669–675. [Google Scholar]
- Snyder, J.M.; Lipitz, L.; Skorupski, K.A.; Shofer, F.S.; Van Winkle, T.J. Secondary intracranial neoplasia in the dog: 177 cases (1986–2003). J. Vet. Intern. Med. 2008, 22, 172–177. [Google Scholar] [CrossRef]
- Long, S.N.; Johnston, P.E.; Anderson, T.J. Primary T-cell lymphoma of the central nervous system in a dog. J. Am. Vet. Med. Assoc. 2001, 218, 719–722. [Google Scholar] [CrossRef]
- Mita, R.; Ishii, M.; Suzuki, M. Chemotherapy of malignant brain tumor with ACNU. Gan To Kagaku Ryoho. 1978, 5, 1184–1191. (In Japanese) [Google Scholar]
- Mori, T.; Mineura, K.; Katakura, R. A consideration on pharmacokinetics of a new water-soluble anti-tumor nitrosourea, ACNU, in patients with malignant brain tumor (author’s transl). No Shinkei. 1979, 31, 601–606. (In Japanese) [Google Scholar]
- Wakui, A. Cancer chemotherapy with special reference to pharmacokinetics of nitrosoureas. Gan Kagaku Ryoho. 1982, 9, 1327–1338. (In Japanese) [Google Scholar]
- Onishi, I. Nimustine (ACNU) treatment for refractory high-grade multicentric lymphoma in dogs. (Abstracts from the 2021 Veterinary Cancer Society Annual Conference). Vet. Comp. Oncol. 2022, 20 (Suppl. S1), 31–32. [Google Scholar]
- LeBlanc, A.K.; Atherton, M.; Bentley, R.T.; Boudreau, C.E.; Burton, J.H.; Curran, K.M.; Dow, S.; Giuffrida, M.A.; Kellihan, H.B.; Mason, N.J.; et al. Veterinary Cooperative Oncology Group-Common Terminology Criteria for Adverse Events (VCOG-CTCAE v2) following investigational therapy in dogs and cats. Vet. Comp. Oncol. 2021, 19, 311–352. [Google Scholar] [CrossRef]
- Isobe, K.; Kobayashi, K.; Kosaihira, S.; Kurimoto, F.; Sakai, H.; Uchida, Y.; Nagai, Y.; Yamaguchi, T.; Miyanaga, A.; Ando, M.; et al. Phase II study of nimustine hydrochloride (ACNU) plus paclitaxel for refractory small cell lung cancer. Lung Cancer 2009, 66, 350–354. [Google Scholar] [CrossRef]
- Kodama, K.; Kodama, K. Long-term complete remission in a cat with large granular lymphocyte lymphoma by nimusutine treatment. J. Jpn. Vet. Cancer. Soc. 2022, 11, 11–16. [Google Scholar] [CrossRef]
- Kariya, K.; Konno, A.; Ishida, T. Perforin-like immunoreactivity in four cases of lymphoma of large granular lymphocytes in the cat. Vet. Pathol. 1997, 34, 156–159. [Google Scholar] [CrossRef]
- Darbès, J.; Majzoub, M.; Breuer, W.; Hermanns, W. Large granular lymphocyte leukemia/lymphoma in six cats. Vet. Pathol. 1998, 35, 370–379. [Google Scholar] [CrossRef]
- Hasegawa, D.; Uchida, K.; Kuwabara, T.; Mizoguchi, S.; Yayoshi, N.; Fujita, M. Long-term survival in a dog with anaplastic oligodendroglioma treated with radiation therapy and CCNU. J. Vet. Med. Sci. 2012, 74, 1517–1521. [Google Scholar] [CrossRef] [PubMed]
- Moirano, S.J.; Dewey, C.W.; Wright, K.Z.; Cohen, P.W. Survival times in dogs with presumptive intracranial gliomas treated with oral lomustine: A comparative retrospective study (2008–2017). Vet. Comp. Oncol. 2018, 16, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.S.; London, C.A.; Wood, C.A.; Williams, L.E.; Cotter, S.M.; L’Heureux, D.A.; Frimberger, A.E. Lomustine (CCNU) for the treatment of resistant lymphoma in dogs. J. Vet. Intern. Med. 1999, 13, 395–398. [Google Scholar] [CrossRef]
- Williams, L.E.; Rassnick, K.M.; Power, H.T.; Lana, S.E.; Morrison-Collister, K.E.; Hansen, K.; Johnson, J.L. CCNU in the treatment of canine epitheliotropic lymphoma. J. Vet. Intern. Med. 2006, 20, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Goto-Koshino, Y.; Fukushima, K.; Kanemoto, H.; Nakashima, K.; Fujino, Y.; Ohno, K.; Endo, Y.; Tsujimoto, H. Phase I dose-escalation study of nimustine in tumor-bearing dogs. J. Vet. Med. Sci. 2014, 76, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Kristal, O.; Rassnick, K.M.; Gliatto, J.M.; Northrup, N.C.; Chretin, J.D.; Morrison-Collister, K.; Cotter, S.M.; Moore, A.S. Hepatotoxicity associated with CCNU (lomustine) chemotherapy in dogs. J. Vet. Intern. Med. 2004, 18, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Heading, K.L.; Brockley, L.K.; Bennett, P.F. CCNU (lomustine) toxicity in dogs: A retrospective study (2002–07). Aust. Vet. J. 2011, 89, 109–116. [Google Scholar] [CrossRef]
- Sakai, K.; Hatoya, S.; Furuya, M.; Nabetani, T.; Kanegi, R.; Shimamura, S.; Tani, H.; Shimada, T. Retrospective evaluation of nimusutine use in the treatment of feline lymphoma. Vet. Med. Sci. 2022, 8, 3–8. [Google Scholar] [CrossRef]
- Sugita, Y.; Takao, K.; Uesawa, Y.; Nagai, J.; Iijima, Y.; Sano, M.; Sakagami, H. Development of Newly Synthesized Chromone Derivatives with High Tumor Specificity against Human Oral Squamous Cell Carcinoma. Medicines 2020, 7, 50. [Google Scholar] [CrossRef]
- Sonoda, Y.; Matsumoto, K.; Kakuto, Y.; Nishino, Y.; Kumabe, T.; Tominaga, T.; Katakura, R. Primary CNS lymphoma treated with combined intra-arterinal ACNU and radiotherapy. Acta Neurochir. 2007, 149, 1183–1189. [Google Scholar] [CrossRef]
- Hori, T.; Muraoka, K.; Saito, Y.; Sasahara, K.; Inagaki, H.; Inoue, Y.; Adachi, S.; Anno, Y. Influence of modes of ACNU administration on tissue and blood drug concentration in malignant brain tumors. J. Neurosurg. 1987, 66, 372–378. [Google Scholar] [CrossRef]
- Kluin, P.M.; Deckeert, M.; Ferry, J.A. Primary diffuse large B-cell lymphoma of the CNS. In WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues, 4th ed.; Campo, E., Swerdlow, S.H., Harris, N.L., Pileri, S., Stein, H., Jaffe, E.S., Eds.; International Agency for Research on Cancer: Lyon, France, 2008; pp. 240–241. [Google Scholar]
- Sisó, S.; Marco-Salazar, P.; Moore, P.F.; Sturges, B.K.; Vernau, W.; Wisner, E.R.; Bollen, A.W.; Dickinson, P.J.; Higgins, R.J. Canine Nervous System Lymphoma Subtypes Display Characteristic Neuroanatomical Patterns. Vet. Pathol. 2017, 54, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Ehrhart, E.J.; Wong, S.; Richter, K.; Zismann, V.; Grimes, C.; Hendricks, W.; Khanna, C. Polymerase chain reaction for antigen receptor rearrangement: Benchmarking performance of a lymphoid clonality assay in diverse canine sample types. J. Vet. Intern. Med. 2019, 33, 1392–1402. [Google Scholar] [CrossRef]
- Burnett, R.C.; Vernau, W.; Modiano, J.F.; Olver, C.S.; Moore, P.F.; Avery, A.C. Diangnosis of canine lymphoid neoplasia using clonal rearrangements of antigen receptor genes. Vet. Pathol. 2003, 40, 32–41. [Google Scholar] [CrossRef]
- Andrews, C.; Operacz, M.; Maes, R.; Kiupel, M. Cross lineage rearrangement in feline enteropathy-associated T-cell lymphoma. Vet. Pathol. 2016, 53, 559–562. [Google Scholar] [CrossRef]
- Tanaka, T.; Ashida, K.; Iimori, Y.; Yamazaki, H.; Mie, K.; Nishida, H.; Akiyoshi, H. MRI findings, including diffusion-weighted imaging, in seven cats with nasal lymphoma and two cats with nasal adenocarcinoma. J. Feline Med. Surg. 2021, 23, 393–399. [Google Scholar] [CrossRef]
- Tanaka, T.; Akiyoshi, H.; Shimazaki, H.; Kawakami, R.; Mie, K.; Yamada, Y.; Ohashi, F. Apparent diffusion coefficient value for a B-cell central nervous system lymphoma in a cat. J. Feline Med. Surg. Open Rep. 2018, 4, 2055116917750762. [Google Scholar] [CrossRef] [PubMed]
- Zacharia, T.T.; Law, M.; Naidich, T.P.; Leeds, N.E. Central nervous system lymphoma characterization by diffusion-weighted imaging and MR spectroscopy. J. Neuroimaging 2008, 18, 411–417. [Google Scholar] [CrossRef]
- Fox, C.P.; Phillips, E.H.; Smith, J.; Linton, K.; Gallop-Evans, E.; Hemmaway, C.; Auer, D.P.; Fuller, C.; Davies, A.; Mckay, P.; et al. British Society for Haematology. Guidelines for the diagnosis and management of primary central nervous system diffuse large B-cell lymphoma. Br. J. Haematol. 2019, 184, 348–363. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Injection | 2nd Injection | 3rd Injection | 4th Injection | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 Day | After | 0 Day | After | 0 Day | After | 0 Day | After | ||
| Case 1 | Blood examination day after injection (day) | 7 | 7 | 8 | 9 | ||||
| WBC (cells/μL) | 17,100 | 1300 †† | 10,700 | 1500 †† | 8700 | 1200 †† | 11,100 | 4300 | |
| neutrophil (cells/μL) | N.D. | N.D. | 8453 | N.D. | 7134 | N.D. | 7992 | N.D. | |
| Lymphocyte (cells/μL) | N.D. | N.D. | 1445 | N.D. | 304 | N.D. | 1221 | N.D. | |
| Thrombocyte (cells/μL) | 591,000 | 116,000 | 280,000 | 130,000 | 134,000 | 48,000 ††† | 119,000 | 27,000 ††† | |
| Alkaline phosphatase (U/L) | 427 †† (1.68 × ULN) | N.D. | 311 † (1.22 × ULN) | N.D. | N.D. | N.D. | N.D. | N.D. | |
| Alanine aminotrasferase (U/L) | 218 †† (2.79 × ULN) | N.D. | 62 (<ULN) | N.D. | 42 (<ULN) | N.D. | N.D. | N.D. | |
| Aspartate aminotrasferase (U/L) | 33 (<ULN) | N.D. | 27 (<ULN) | N.D. | N.D. | N.D. | N.D. | N.D. | |
| Dose of nimustine (mg/m2) | 50 | 45 | 40 | 35 | |||||
| Case 2 | Blood examination day after injection (day) | 7 | 6 | 7 | 7 | ||||
| WBC (cells/μL) | 21,000 | 6000 | 22,000 | 800 ††† | 18,900 | 700 ††† | 16,500 | 1600 † | |
| neutrophil (cells/μL) | N.D. | N.D. | 21,560 | N.D. | 17,199 | N.D. | 13,695 | N.D. | |
| Lymphocyte (cells/μL) | N.D. | N.D. | 220 | N.D. | 593 | N.D. | 495 | N.D. | |
| Thrombocyte (cells/μL) | 281,000 | 201,000 | 294,000 | 298,000 | 275,000 | 274,400 | 480,000 | 119,000 | |
| Alkaline phosphatase (U/L) | 1149 †† (4.52 × ULN) | N.D. | 895 †† (3.52 × ULN) | N.D. | 597 † (2.35 × ULN) | N.D. | 873 †† (3.44 × ULN) | N.D. | |
| Alanine aminotrasferase (U/L) | 266 †† (3.41 × ULN) | N.D. | 119 †† (1.53 × ULN) | N.D. | 79 † (1.01 × ULN) | N.D. | 93 † (1.19 × ULN) | N.D. | |
| Aspartate aminotrasferase (U/L) | 45 † (1.02 × ULN) | N.D. | 26 (<ULN) | N.D. | 21 (<ULN) | N.D. | 25 (<ULN) | N.D. | |
| Dose of nimustine (mg/m2) | 35 | 35 | 32 | 30 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mizutani, Y.; Inoue, Y.; Goda, Y.; Mizutani, S.; Asanuma, T.; Miura, N.; Hidaka, Y.; Sato, R.; Satoh, H. Successful Treatment of Central Nervous System Lymphoma with Combination Therapy of Nimustine and Prednisolone in Two Dogs. Vet. Sci. 2023, 10, 533. https://doi.org/10.3390/vetsci10090533
Mizutani Y, Inoue Y, Goda Y, Mizutani S, Asanuma T, Miura N, Hidaka Y, Sato R, Satoh H. Successful Treatment of Central Nervous System Lymphoma with Combination Therapy of Nimustine and Prednisolone in Two Dogs. Veterinary Sciences. 2023; 10(9):533. https://doi.org/10.3390/vetsci10090533
Chicago/Turabian StyleMizutani, Yuko, Yoshiyuki Inoue, Yoshimichi Goda, Shinya Mizutani, Taketoshi Asanuma, Naoki Miura, Yuichi Hidaka, Reiichiro Sato, and Hiroyuki Satoh. 2023. "Successful Treatment of Central Nervous System Lymphoma with Combination Therapy of Nimustine and Prednisolone in Two Dogs" Veterinary Sciences 10, no. 9: 533. https://doi.org/10.3390/vetsci10090533