
Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: A Scoping Review




Abstract
:1. Introduction
2. Materials and Methods
- We identified key concepts underlying our research question.
- We identified search terms related to each key concept.
- With the help of a public health librarian, we
- a.
- identified databases (Medline, CINAHL, and PubMed) from which to select literature; and
- b.
- created and implemented a search strategy for each database to generate a list of possible literature for review.
- Two authors independently implemented the search strategies and identified literature from the three databases. They identified additional search terms from the literature and re-ran the searches. This was repeated until no new search terms were added to the search strategy.
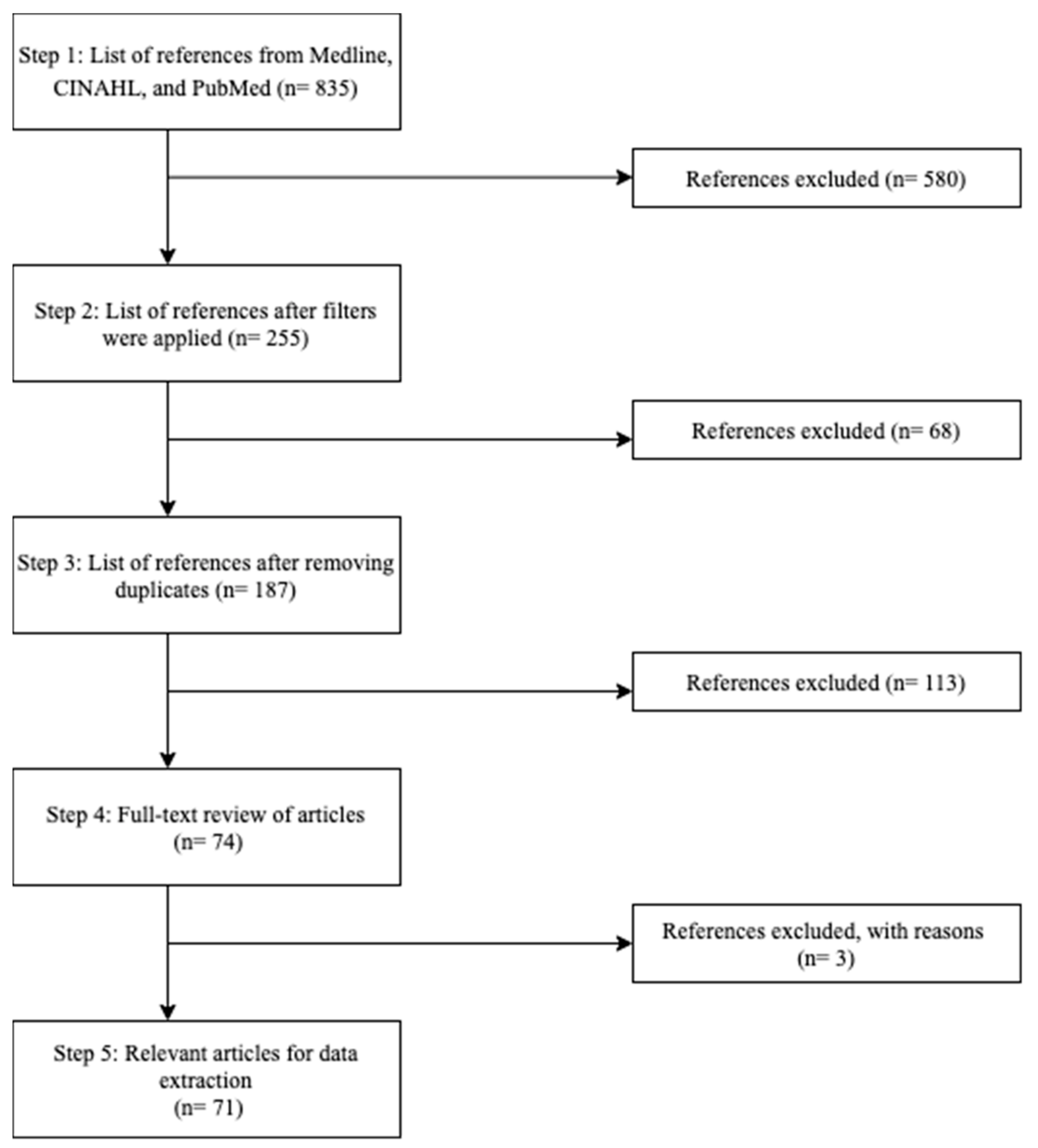
- These two authors independently implemented the final search strategy for each database to generate a list of possible articles for review. They then applied the filters: journal articles, full-text availability, papers published in 2020 and onwards, English language, and human participants, to create a reduced list of articles from each database.
- A single reviewer transferred the reduced lists obtained in Step 5 to Zotero and compiled one list of articles for review while removing any duplicate articles.
- Our scoping review process deviated from the Arksey and O’Malley strategy at this point because we hypothesized that findings regarding visible minorities and their respective reasons for vaccine hesitancy may not be found within the titles or abstracts of research papers. Therefore, to ensure that all relevant articles were included in our final list, we skipped title and abstract screening, and two reviewers performed full-text reviews applying the inclusion/exclusion criteria independently (Table 1) to create a final list of articles for data extraction. During this full-text review process, two reviewers discussed and resolved any disagreement that arose in terms of whether to include an article for data extraction. For when the two reviewers disagreed on whether or not to include an article, a third reviewer reviewed the article and decided on whether or not to include it. The final list of articles for data extraction was collated. The levels of agreement between both reviewers were calculated using the Cohen’s Kappa statistic.
- While performing full-text reviews, the reviewers extracted themes of vaccine hesitancy in visible minority populations and stored them in an excel spreadsheet. Figure 1 depicts the steps taken to arrive at the final list of relevant articles for our scoping review.
- ADJ3: is a syntax used in a proximity search used in the Medline database—it is also known as (ADJ = adjacency). ADJ3 is the same as searching by having up to three words next to each other in any order. One needs to separate their search terms with ADJ3 in between when using this adjacency operator.
- N3: is a syntax used in the CINAHL database, (N = near). N3 specifies there are three words between each search term while searching in no particular order.
- AND, OR, NOT: are Boolean operators used in the PubMed database to retrieve all search terms results, retrieve results with at least search term or exclude search terms retrieved from the search.
Data Analysis
- Thematic qualitative analysis: Two reviewers independently grouped the extracted themes from the final list of articles that arose in step 8, into overarching factors. The level of agreement between both reviewers was calculated using the Cohen’s Kappa statistic.
- Principal component analysis (PCA): Using the themes identified by both reviewers in step 8, a PCA with Promax oblique rotation was used to group the themes into overarching factors influencing COVID-19 vaccine hesitancy. A parallel analysis (with 1000 Monte Carlo simulation repetitions) was used to select the initial list of overarching factors. Themes that had a correlation of 0.6 or more or −0.6 or less with a factor were used to determine the name of the factor. An author different from the two who did the qualitative thematic analysis named the factors identified through the PCA.
- Word cloud: To qualitatively complement the themes extracted during data extraction, a word cloud was created for 100 of the most frequently occurring words in the titles and abstracts of the final set of articles.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dubé, E.; Bettinger, J.A.; Fisher, W.A.; Naus, M.; Mahmud, S.M.; Hilderman, T. Vaccine acceptance, hesitancy, and refusal in Canada: Challenges and potential approaches. Can. Commun. Dis. Rep. 2016, 42, 246–251. [Google Scholar] [CrossRef]
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 26 July 2021).
- Macdonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1339. [Google Scholar] [CrossRef] [PubMed]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy: A Challenge the United States Must Overcome. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- Andersson, O.; Campos-Mercade, P.; Meier, A.; Wengström, E. Anticipation of COVID-19 Vaccines Reduces Social Distancing. SSRN Electron. J. 2020, 80, 102530. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Lurie, N.; Fremont, A. Looking Forward: Cross-cutting Issues in the Collection and Use of Racial/Ethnic Data. Health Serv. Res. 2006, 41, 1519–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minority Rights Group International. Canada: World Directory of Minorities and Indigenous Peoples. Available online: https://minorityrights.org/country/canada/ (accessed on 21 June 2021).
- Chui, T.; Maheux, H. Women in Canada: A Gender-Based Statistical Report Visible Minority Women. 2021. Available online: https://www.oaith.ca/assets/files/Publications/Government%20Documents/Women_In_Canada_6thReport/WmCanada_WmColour.pdf (accessed on 21 June 2021).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2007, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; Hanif, W.; Patel, K.; Khunti, K. South Asian Health Foundation, UK. Ramadan and COVID-19 vaccine hesitancy-a call for action. Lancet 2021, 397, 1443–1444. [Google Scholar] [CrossRef]
- Unroe, K.T.; Evans, R.; Weaver, L.; Rusyniak, D.; Blackburn, J. Willingness of Long-Term Care Staff to Receive a COVID-19 Vaccine: A Single State Survey. J. Am. Geriatr. Soc. 2021, 69, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.; Osama, T.; McKechnie, D.; Majeed, A. COVID-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef]
- Nikolovski, J.; Koldijk, M.; Weverling, G.J.; Spertus, J.; Turakhia, M.; Saxon, L.; Gibson, M.; Whang, J.; Sarich, T.; Zambon, R.; et al. Factors indicating intention to vaccinate with a COVID-19 vaccine among older U.S. adults. PLoS ONE 2021, 16, e0251963. [Google Scholar] [CrossRef]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel—implications for vaccination implementation policies. Isr. J. Health Policy Res. 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Bogart, L.; Ojikutu, B.; Tyagi, K.; Klein, D.; Mutchler, M.; Dong, L.; Kellman, S. COVID-19 Related Medical Mistrust, Health Impacts, and Potential Vaccine Hesitancy Among Black Americans Living With HIV. J. Acquir. Immune Defic. Syndr. 2021, 86, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Corpuz, J. Multisectoral Approach on COVID-19 vaccination: A proposed solution on vaccine hesitancy. J. Public Health 2021, 43, E370–E371. [Google Scholar] [CrossRef]
- Latkin, C.; Dayton, L.A.; Yi, G.; Konstantopoulos, A.; Park, J.; Maulsby, C.; Kong, X. COVID-19 vaccine intentions in the United States, a social-ecological framework. Vaccine 2021, 39, 2288–2294. [Google Scholar] [CrossRef]
- Mosby, I.; Swidrovich, J. Medical experimentation, and the roots of COVID-19 vaccine hesitancy among Indigenous Peoples in Canada. Can. Med. Assoc. J. 2021, 193, E381–E383. [Google Scholar] [CrossRef] [PubMed]
- Lux, M. Perfect Subjects: Race, Tuberculosis, and the Qu’Appelle BCG Vaccine Trial. Can. Bull. Med. Hist. 1998, 15, 277–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreps, S.; Prasad, S.; Brownstein, J.; Hswen, Y.; Garibaldi, B.; Zhang, B.; Kriner, D. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.T.; Feng, D.; Feng, Z.; Yeoh, E.K.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health expectations: An international journal of public participation in health care and health policy. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.S.; Manning, M.; Mitchell, J.; Kim, S.; Harper, F.; Cresswell, S.; Marks, B. Factors Associated with Racial/Ethnic GroupBased Medical Mistrust and Perspectives on COVID-19 Vaccine Trial Participation and Vaccine Uptake in the US. JAMA Netw. Open 2021, 4, e211162. [Google Scholar] [CrossRef]
- Bunch, L. A Tale of Two Crises: Addressing COVID-19 Vaccine Hesitancy as Promoting Racial Justice. HEC Forum 2021, 33, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Laurencin, C.T. Addressing Justified Vaccine Hesitancy in the Black Community. J. Racial Ethn. Health Disparities 2021, 8, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Okorodudu, D.O.; Okorodudu, D.E. An issue of trust-vaccinating Black patients against COVID-19. Lancet Respir. Med. 2021, 9, 228–229. [Google Scholar] [CrossRef]
- Allen, J.D.; Abuelezam, N.N.; Rose, R.; Fontenot, H.B. Factors associated with the intention to obtain a COVID-19 vaccine among a racially/ethnically diverse sample of women in the USA. Transl. Behav. Med. 2021, 11, 785–792. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Gatwood, J.; McKnight, M.; Fiscus, M.; Hohmeier, K.C.; Chisholm-Burns, M. Factors influencing likelihood of COVID-19 vaccination: A survey of Tennessee adults. Am. J. Health-Syst. Pharm. 2021, 78, 879–889. [Google Scholar] [CrossRef]
- Ogilvie, G.S.; Gordon, S.; Smith, L.W.; Albert, A.; Racey, C.S.; Booth, A.; Sadarangani, M. Intention to receive a COVID-19 vaccine: Results from a population-based survey in Canada. BMC Public Health 2021, 21, 1017. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.M.; Stein, R.; Brown, M.F.; Hershberger, J.; Scott, E.M.; Wenger, O.K. Vaccination patterns of the northeast Ohio Amish revisited. Vaccine 2021, 39, 1058–1063. [Google Scholar] [CrossRef]
- Gramacho, W.G.; Turgeon, M. When politics collides with public health: COVID-19 vaccine country of origin and vaccination acceptance in Brazil. Vaccine 2021, 39, 2608–2612. [Google Scholar] [CrossRef]
- Kreps, S.E.; Kriner, D.L. Factors influencing COVID-19 vaccine acceptance across subgroups in the United States: Evidence from a conjoint experiment. Vaccine 2021, 39, 3250–3258. [Google Scholar] [CrossRef] [PubMed]
- Perkins, D.E. A COVID-19 Vaccination Challenge. Am. J. Nurs. 2021, 121, 11. [Google Scholar] [CrossRef]
- Qin, W.; Wang, E.; Ni, Z. Chinese consumers’ willingness to get a COVID-19 vaccine and willingness to pay for it. PLoS ONE 2021, 16, e0250112. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Reid, J.A.; Mabhala, M.A. Ethnic and minority group differences in engagement with COVID-19 vaccination programmes-at Pandemic Pace, when vaccine confidence in mass rollout meets local vaccine hesitancy. Isr. J. Health Policy Res. 2021, 10, 33. [Google Scholar] [CrossRef]
- Woko, C.; Siegel, L.; Hornik, R. An Investigation of Low COVID-19 Vaccination Intentions among Black Americans: The Role of Behavioral Beliefs and Trust in COVID-19 Information Sources. J. Health Commun. 2020, 25, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Coyne-Beasley, T.; Hill, S.V.; Zimet, G.; Kanbur, N.; Kimberlin, D.; Raymond-Flesch, M.; Simpson, T.; Svetaz, M.V.; Trent, M.; Walker-Harding, L. COVID-19 Vaccination of Adolescents and Young Adults of Color: Viewing Acceptance and Uptake with a Health Equity Lens. J. Adolesc Health. 2021, 68, 844–846. [Google Scholar] [CrossRef] [PubMed]
- Salmon, D.A.; Dudley, M.Z.; Brewer, J.; Kan, L.; Gerber, J.E.; Budigan, H.; Schwartz, B. COVID-19 vaccination attitudes, values and intentions among United States adults prior to emergency use authorization. Vaccine 2021, 39, 2698–2711. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Yu, L.M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]
- Katherine, W.; Chris, M.; Christopher, M.; Laura, N.B.; Anna, G.L.; Carl, M.; Bryant, L.; Mayuri, G.; Wobi, F.; Al-Oraibi, A.; et al. Ethnic differences in SARS-CoV-2 vaccine hesitancy in United Kingdom healthcare workers: Results from the UK-REACH prospective nationwide cohort study. Lancet Reg. Health 2021, 9, 100180. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Han, B.; Zhao, T.; Liu, H.; Liu, B.; Chen, L.; Cui, F. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021, 39, 2833–2842. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Peer-reviewed journal articles | Non-peer reviewed articles/grey literature |
| Articles related to COVID-19 and visible minorities | Articles studying diseases other than COVID-19 and non-visible minorities |
| Papers written in English language | Papers written in languages other than English language |
| Papers published in 2020 and onwards | Papers published prior to 2020 |
| Papers involving human participants | Papers involving non-human participants |
| Articles discussing reasons for COVID-19 vaccine hesitancy | Articles not discussing reasons but rather stating statistics related to COVID-19 vaccine hesitancy |
| Articles studying COVID-19 vaccine hesitancy in clinical/vaccine trial participation |
| Concept 1 (Vaccine): (Combine Terms below with OR) | ADJ3 * | Concept 2 (Hesitancy): (Combine Terms below with OR) | AND | Concept 3 (Visible Minority): (Combine Terms below with OR) | AND | Concept 4 (COVID-19): (Combine Terms below with OR) |
|---|---|---|---|---|---|---|
| Vaccin * Inoculat * Immuniz * Inject * Shot Shots | Hesita * Confiden * Refus * Decision Decisions Decision making Concern * Accept * Attitud * Barrier Barriers Trust * Adher * Uptak * Reluctan * Skeptic * Intent * | Visible minorit * (Race OR racial OR ethnic) ADJ3 (disparit * OR inequality * OR inequit * OR segregate * OR minorit *) Ethnic * Divers * Vulnerable * (Vulnerab * ADJ3 population *) Non-white * Non-Caucasian * (South ADJ3 Asian *) Chinese (Black OR Blacks OR African ADJ3 American *) Filipino * (Latin American * OR Latino * OR Hispanic *) Arab * (Southeast ADJ3 Asian *) (West ADJ3 Asian *) Korean * Japanese Aboriginal * Indigenous Native * First Nation * Indian Indians Metis Inuit | COVID-19 COVID-19 Coronavirus Corona virus Coronavirus 19 SARS CoV 2 Coronavirus disease 2019 COVID 2019 COVID19 Global pandemic Novel coronavirus Novel corona virus 2019 nCoV nCoV 2019 2019 ncov CoV 2019 2019 CoV ncov19 ncov 19 2019 novel CoV SARS coronavirus 2 Sars coronavirus 2 SARS like coronavirus Severe Acute Respiratory Syndrome Coronavirus 2 Severe acture respiratory syndrome coronavirus 2 severe-acute-respiratory-syndrome-coronavirus-2 wuhan OR hubei OR huanan OR china OR chinese) AND (severe acute respiratory OR pneumonia *) AND outbreak *) cov-19 COVID pandemic Coronavirus infection Coronavirus infections |
| Factor | Themes | Frequency |
|---|---|---|
| Safety and effectiveness of vaccine | 88 | |
| Safety | 31 | |
| Effectiveness | 31 | |
| Side Effects | 22 | |
| Frequency of Injections/Fear of Needles | 4 | |
| Mistrust | 72 | |
| Lack of Trust | 39 | |
| Racism | 21 | |
| Underrepresentation in Medical/Clinical Research | 10 | |
| Biased/Non-diverse HCPs | 2 | |
| Socioeconomic characteristics | 52 | |
| Gender | 21 | |
| Age | 12 | |
| Education | 9 | |
| Income | 5 | |
| Occupation | 2 | |
| Location | 2 | |
| Having children | 1 | |
| Vaccine development | 45 | |
| Short duration of Vaccine Development | 14 | |
| Cost of Vaccine | 12 | |
| Place of Manufacturing | 8 | |
| Novelty of Vaccine | 7 | |
| Duration of Immunity | 4 | |
| Information circulation | 42 | |
| Information Reliability | 18 | |
| Type of media Information | 17 | |
| Political Ideology | 7 | |
| Knowledge and acceptance | 18 | |
| Religious Beliefs | 8 | |
| General Vaccine Beliefs | 7 | |
| Past Vaccine Compliance | 3 | |
| Perceived risk of COVID-19 | 17 | |
| Perceived risk of acquiring COVID-19 | 13 | |
| infection | ||
| Opinion of HCP | 4 | |
| Perceived benefit | 5 | |
| Personal Benefit | 2 | |
| Collective Benefit | 2 | |
| Number of people Vaccinated | 1 |
| Factor (Eigenvalue) | Themes (Loading) |
|---|---|
| Perceived benefit (4.584) | Occupation (0.688) |
| Collective benefit (0.916) | |
| Personal benefit (0.916) | |
| Safety and effectiveness of vaccine (3.532) | Side effects (0.714) |
| Safety (0.820) | |
| Effectiveness (0.862) | |
| Socioeconomic characteristics (2.863) | Income (0.834) |
| Location (0.785) | |
| Having children (0.767) | |
| Convenience associated with getting the vaccine (2.525) | Frequency of injections/schedule (0.656) |
| Location (0.656) | |
| Number of people vaccinated (0.855) | |
| Knowledge and acceptance of vaccine (2.099) | Education (0.622) |
| Past vaccine compliance (0.699) | |
| General vaccine beliefs (0.665) | |
| Mistrust (2.002) | Lack of trust (0.787) |
| Source of information about vaccine (1.855) | Type of media information |
| Information reliability | |
| External factors (1.706) | Duration of immunity (0.623) |
| Opinion of HCP (0.643) | |
| Pre-existing medical conditions (0.619) | |
| Vaccine coverage (0.794) |
| Factors from Thematic Qualitative Analysis | Factors from Principal Component Analysis | Factors in Agreement |
|---|---|---|
| Perceived benefit | Perceived benefit | Perceived benefit |
| Safety and effectiveness of vaccine | Safety and effectiveness of vaccine | Safety and effectiveness of vaccine |
| Socioeconomic characteristics | Socioeconomic characteristics | Socioeconomic characteristics |
| Information circulation | Source of information about vaccine | Source of information about vaccine |
| Knowledge and acceptance | Knowledge and acceptance of vaccine | Knowledge and acceptance of vaccine |
| Mistrust | Mistrust | Mistrust |
| Vaccine development | Convenience associated with getting the vaccine | |
| Perceived risk of COVID-19 | External factors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochieng, C.; Anand, S.; Mutwiri, G.; Szafron, M.; Alphonsus, K. Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: A Scoping Review. Vaccines 2021, 9, 1445. https://doi.org/10.3390/vaccines9121445
Ochieng C, Anand S, Mutwiri G, Szafron M, Alphonsus K. Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: A Scoping Review. Vaccines. 2021; 9(12):1445. https://doi.org/10.3390/vaccines9121445
Chicago/Turabian StyleOchieng, Candy, Sabrita Anand, George Mutwiri, Michael Szafron, and Khrisha Alphonsus. 2021. "Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: A Scoping Review" Vaccines 9, no. 12: 1445. https://doi.org/10.3390/vaccines9121445