
Cervical Cancer Protection in Japan: Where Are We?

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Politics, Policies, and Events Related to HPV Vaccinations
3. Safety and Efficacy of HPV Vaccination
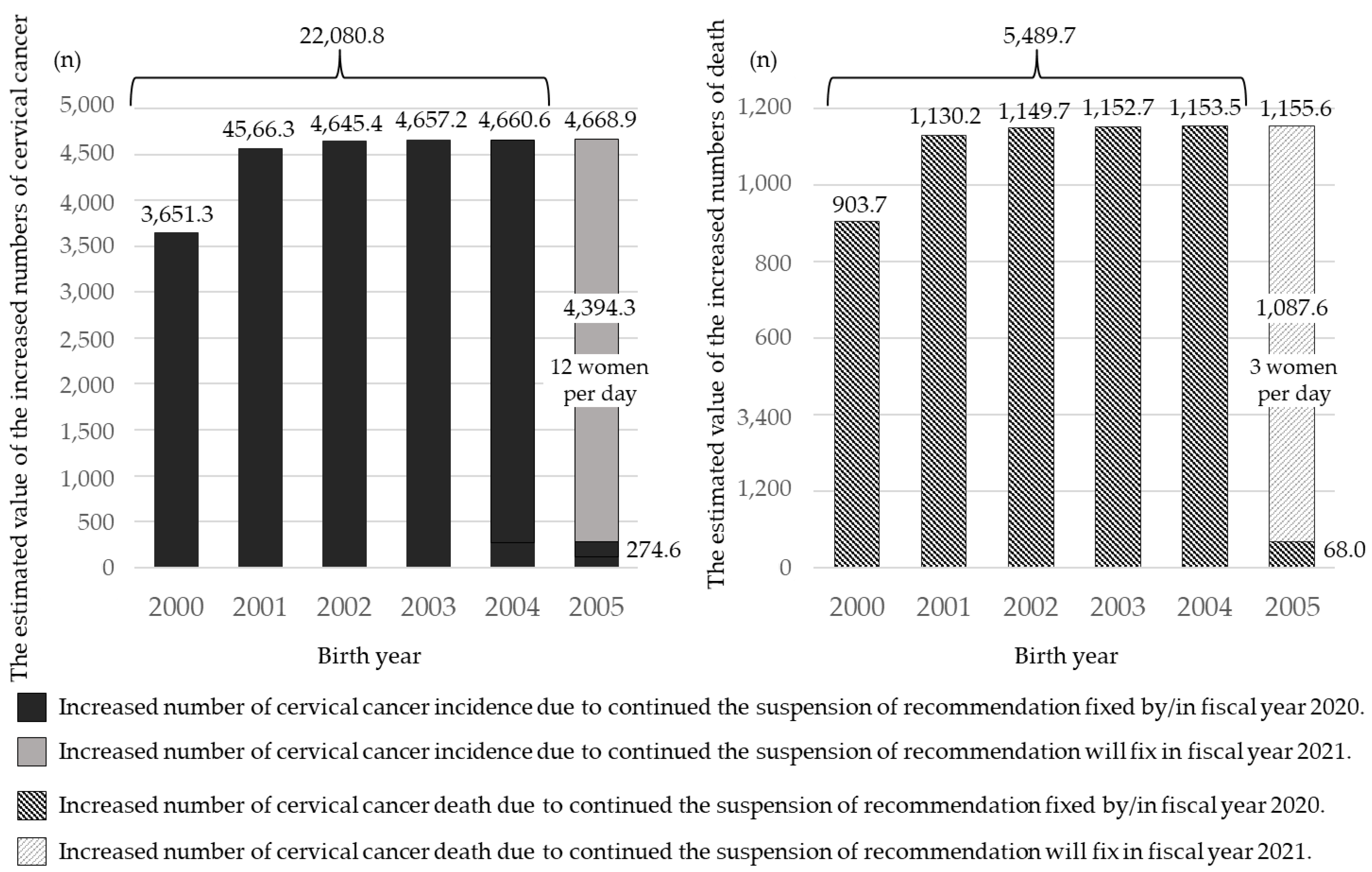
4. Future Risk Caused by the Governmental Recommendation for HPV Vaccination
5. Future Prospects for Discussion
5.1. After a Resumption of the Governmental Recommendation?
5.2. Women Who Missed Their Opportunity of HPV Vaccination
6. The Real Harm Caused by Vaccine Hesitancy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Today. Available online: https://gco.iarc.fr/today (accessed on 4 September 2021).
- World Health Organization, Cervical Cancer Elimination Initiative. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed on 4 September 2021).
- Yagi, A.; Ueda, Y.; Kakuda, M.; Tanaka, Y.; Ikeda, S.; Matsuzaki, S.; Kobayashi, E.; Morishima, T.; Miyashiro, I.; Fukui, K.; et al. Epidemiologic and clinical analysis of cervical cancer using data from the population-based Osaka Cancer Registry. Cancer Res. 2019, 79, 1252–1259. [Google Scholar] [CrossRef] [Green Version]
- Cancer Incidence. Cancer Statistics. Cancer Information Service, National Cancer Center, Japan (National Cancer Registry, Ministry of Health, Labour and Welfare). Available online: https://ganjoho.jp/reg_stat/statistics/data/dl/index.html#a14 (accessed on 4 September 2021).
- Cancer Mortality. Cancer Statistics. Cancer Information Service, National Cancer Center, Japan (National Cancer Registry, Ministry of Health, Labour and Welfare). Available online: https://ganjoho.jp/reg_stat/statistics/data/dl/index.html#a7 (accessed on 4 September 2021).
- Baseman, J.G.; Koutsky, L.A. The epidemiology of human papillomavirus infections. J. Clin. Virol. 2005, 32, 16–24. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Satoh, T.; Oki, A.; Okada, S.; Minaguchi, T.; Ochi, H.; Nakao, S.; Someya, K.; Yamada, N.; et al. Human papillomavirus infections among Japanese women: Age-related prevalence and type-specific risk for cervical cancer. Cancer Sci. 2009, 100, 1312–1316. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Iwata, T.; Yamamoto, K.; Aoki, Y.; Maenohara, S.; Tsuda, N.; Kamiura, S.; Takehara, K.; Horie, K.; et al. Human papillomavirus genotype contribution to cervical cancer and precancer: Implications for screening and vaccination in Japan. Cancer Sci. 2020, 111, 2546–2557. [Google Scholar] [CrossRef]
- Miura, S.; Matsumoto, K.; Oki, A.; Satoh, T.; Tsunoda, H.; Yasugi, T.; Taketani, Y.; Yoshikawa, H. Do we need a different strategy for HPV screening and vaccination in East Asia? Int. J. Cancer 2006, 119, 2713–2715. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; Castellsagué, X.; Diaz, M.; José, F.X.B.; Hammouda, D.; Shah, K.V.; Meijer, C.J. Against which human papillomavirus types shall we vaccinate and screen? the international perspective. Int. J. Cancer 2004, 111, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Franceschi, S.; Bosetti, C.; Moreno, V.; Herrero, R.; Smith, J.S.; Shah, K.V.; Meijer, C.J.; Bosch, F.X.; International Agency for Research on Cancer. Multicentric Cervical Cancer Study Group. Role of parity and human papillomavirus in cervical cancer: The IARC multicentric case-control study. Lancet 2002, 359, 1093–1101. [Google Scholar] [CrossRef]
- Moreno, V.; Bosch, F.X.; Muñoz, N.; Meijer, C.J.; Shah, K.V.; Walboomers, J.M.; Herrero, R.; Franceschi, S.; International Agency for Research on Cancer Multicentric Cervical Cancer Study Group. Effect of oral contraceptives on risk of cervical cancer in women with human papillomavirus infection: The IARC multicentric case-control study. Lancet 2002, 359, 1085–1092. [Google Scholar] [CrossRef]
- International Collaboration of Epidemiological Studies of Cervical Cancer; Appleby, P.; Beral, V.; Berrington de González, A.; Colin, D.; Franceschi, S.; Goodill, A.; Green, J.; Peto, J.; Plummer, M.; et al. Carcinoma of the cervix and tobacco smoking: Collaborative reanalysis of individual data on 13,541 women with carcinoma of the cervix and 23,017 women without carcinoma of the cervix from 23 epidemiological studies. Int. J. Cancer 2006, 18, 1481–1495. [Google Scholar]
- Comprehensive Survey of Living Conditions. The Ministry of Health, Labor and Welfare, Japan. Available online: https://www.mhlw.go.jp/toukei/list/20-21.html (accessed on 4 September 2021).
- Organisation for Economic Co-Operation and Development (OECD). OECD Reviews of Public Health: Japan: A Healthier Tomorrow; OECD Reviews of Public Health; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Nakagawa, S.; Ueda, Y.; Yagi, A.; Ikeda, S.; Hiramatsu, K.; Kimura, T. Corrected human papillomavirus vaccination rates for each birth fiscal year in Japan. Cancer Sci. 2020, 111, 2156–2162. [Google Scholar] [CrossRef] [PubMed]
- Merck & Co., Inc. Sylgard®9 Interview Form Revised February 2021 (3rd Edition). Available online: https://www.msdconnect.jp/static/mcijapan/images/if_silgard9.pdf (accessed on 4 September 2021).
- Merck & Co., Inc. Gardasil® Interview Form, Revised December 2020 (9th Edition). Available online: https://www.msdconnect.jp/static/mcijapan/images/if_gardasil.pdf (accessed on 4 September 2021).
- Global Advisory Committee on Vaccine Safety (World Health Organization). Safety of HPV Vaccines. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/human-papillomavirus-vaccines/safety (accessed on 4 September 2021).
- The Japan Expert Council on Promotion of Vaccine. Views of Relevant Academic Groups on Promoting HPV Vaccination. Available online: http://vaccine-kyogikai.umin.jp/ (accessed on 4 September 2021).
- The 23rd Welfare Science Council Vaccination and Vaccine Subcommittee Side-Reaction Study Group. 26 December 2016. Available online: https://www.mhlw.go.jp/stf/shingi2/0000147015.html (accessed on 4 September 2021).
- The 26th Welfare Science Council Vaccination and Vaccine Subcommittee Side-Reaction Study Group. 10 April 2017. Available online: https://www.mhlw.go.jp/stf/shingi2/0000161332.html (accessed on 4 September 2021).
- The 42nd Welfare Science Council Vaccination and Vaccine Subcommittee Side-Reaction Study Group. 30 August 2019. Available online: https://www.mhlw.go.jp/stf/newpage_06462.html (accessed on 4 September 2021).
- Larson, H.J.; Wilson, R.; Hanley, S.; Parys, A.; Paterson, P. Tracking the global spread of vaccine sentiments: The global response to Japan’s suspension of its HPV vaccine recommendation. Hum Vaccin Immunother. 2014, 10, 2543–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Disease Control and Prevention, Advisory Committee on Immunization Practices (ACIP) Summary Report. 2015. Available online: http://www.cdc.gov/vaccines/acip/meetings/downloads/min-archive/min-2015-10.pdf (accessed on 4 September 2021).
- European Medicines Agency, HPV Vaccines: EMA Confirms Evidence Does Not Support That They Cause CRPS or POTS. 2015. Available online: https://www.ema.europa.eu/en/news/hpv-vaccines-ema-confirms-evidence-does-not-support-they-cause-crps-pots (accessed on 4 September 2021).
- French National Agency for Medicines and Health Products Safety, Vaccination Contre les Infections à HPV et Risque de Maladies Auto-Immunes: Une étude Cnamts/ANSM Rassurante. 2015. Available online: https://ansm.sante.fr/actualites/vaccination-contre-les-infections-a-hpv-et-risque-de-maladies-auto-immunes-une-etude-cnamts-ansm-rassurante-1 (accessed on 4 September 2021).
- Arbyn, M.; Xu, L.; Simoens, C.; Martin-Hirsch, P.P. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst. Rev. 2018, 5, CD009069. [Google Scholar] [CrossRef]
- Suzuki, S.; Hosono, A. No association between HPV vaccine and reported post-vaccination symptoms in Japanese young women: Results of the Nagoya study. Papillomavirus Res. 2018, 5, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Luostarinen, T.; Apter, D.; Dillner, J.; Eriksson, T.; Harjula, K.; Natunen, K.; Paavonen, J.; Pukkala, E.; Lehtinen, M. Vaccination protects against invasive HPV-associated cancers. Int. J. Cancer 2018, 142, 2186–2187. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef]
- Ueda, Y.; Yagi, A.; Nakayama, T.; Hirai, K.; Ikeda, S.; Sekine, M.; Miyagi, E.; Enomoto, T. Author Correction: Dynamic changes in Japan’s prevalence of abnormal findings in cervical cytology depending on birth year. Sci. Rep. 2018, 8, 13384. [Google Scholar] [CrossRef]
- Ikeda, S.; Ueda, Y.; Hara, M.; Yagi, A.; Kitamura, T.; Kitamura, Y.; Konishi, H.; Kakizoe, T.; Sekine, M.; Enomoto, T.; et al. Human papillomavirus vaccine to prevent cervical intraepithelial neoplasia in Japan: A nationwide case-control study. Cancer Sci. 2021, 112, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Yagi, A.; Ueda, Y.; Ikeda, S.; Sekine, M.; Nakayama, T.; Miyagi, E.; Enomoto, T. Evaluation of future cervical cancer risk in Japan, based on birth year. Vaccine 2019, 37, 2889–2891. [Google Scholar] [CrossRef]
- Yagi, A.; Ueda, Y.; Nakagawa, S.; Masuda, T.; Miyatake, T.; Ikeda, S.; Abe, H.; Hirai, K.; Sekine, M.; Miyagi, E.; et al. A nationwide birth year-by-year analysis of effectiveness of HPV vaccine in Japan. Cancer Sci. 2021, 112, 3691–3698. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Infectious Disease, Pertussis, Whooping Cough. 2018. Available online: https://www.niid.go.jp/niid/ja/kansennohanashi/477-pertussis.html (accessed on 4 September 2021).
- World Health Organization, Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 4 September 2021).
- Yagi, A.; Ueda, Y.; Nakagawa, S.; Ikeda, S.; Tanaka, Y.; Sekine, M.; Miyagi, E.; Enomoto, T.; Kimura, T. Potential for cervical cancer incidence and death resulting from Japan’s current policy of prolonged suspension of its governmental recommendation of the HPV vaccine. Sci. Rep. 2020, 10, 15945. [Google Scholar] [CrossRef] [PubMed]
- Simms, K.T.; Hanley, S.J.B.; Smith, M.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: A modelling study. Lancet Public Health 2020, 5, e223–e234. [Google Scholar] [CrossRef]
- Yagi, A.; Ueda, Y.; Masuda, T.; Ikeda, S.; Miyatake, T.; Nakagawa, S.; Hirai, K.; Nakayama, T.; Miyagi, E.; Enomoto, T.; et al. Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation? Vaccines 2020, 8, 502. [Google Scholar] [CrossRef]
- Ueda, Y.; Yagi, A.; Abe, H.; Nakagawa, S.; Minekawa, R.; Kuroki, H.; Miwa, A.; Kimura, T. The last strategy for re-dissemination of HPV vaccination in Japan while still under the suspension of the governmental recommendation. Sci. Rep. 2020, 10, 16091. [Google Scholar] [CrossRef]
- Ugumori, N.; Ueda, Y.; Yagi, A.; Abe, H.; Shiomi, M.; Nakagawa, S.; Hiramatsu, K.; Miyoshi, A.; Kobayashi, E.; Kimura, T.; et al. A potential means to help the HPV vaccine penetrate the Japanese public while under the continued suspension of governmental recommendation. Hum. Vaccines Immunother. 2021, 17, 3096–3101. [Google Scholar] [CrossRef]
- Ueda, Y.; Katayama, K.; Yagi, A.; Kimura, T. The Chasm We Must Cross in Japan for Re-promotion of the HPV Vaccine. Cancer Prev. Res. 2021, 14, 683–686. [Google Scholar] [CrossRef]
- Japan Family Planning Association, 7th Survey on the Lives and Attitudes of Men and Women. 2014. Available online: https://www.jfpa.or.jp/paper/main/000047.html (accessed on 4 September 2021).
- Miyoshi, A.; Ueda, Y.; Yagi, A.; Taniguchi, M.; Sekine, M.; Enomoto, T.; Kimura, T. Health consciousness and cervical cancer screening rates in HPV-unvaccinated girls: Comparison from HPV-recommended and HPV-recommendation-suspended program periods. Hum. Vaccines Immunother. 2021, 17, 1068–1072. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Ueda, Y.; Egawa-Takata, T.; Yagi, A.; Yoshino, K.; Kimura, T. Outcomes for girls without HPV vaccination in Japan. Lancet Oncol. 2016, 17, 868–869. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, B.; Clarke, A.; Barrett, T. Rapid response to HPV vaccination crisis in Ireland. Lancet 2018, 391, 2103. [Google Scholar] [CrossRef] [Green Version]
- Hansen, P.R.; Schmidtblaicher, M.; Brewer, N.T. Resilience of HPV vaccine uptake in Denmark: Decline and recovery. Vaccine 2020, 38, 1842–1848. [Google Scholar] [CrossRef]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine Hesitancy and Its Associated Factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef]
- Tsuda, K.; Yamamoto, K.; Leppold, C.; Tanimoto, T.; Kusumi, E.; Komatsu, T.; Kami, M. Trends of Media Coverage on Human Papillomavirus Vaccination in Japanese Newspapers. Clin. Infect. Dis. 2016, 63, 1634–1638. [Google Scholar] [CrossRef] [Green Version]
- Ueda, Y.; Yagi, A.; Ikeda, S.; Enomoto, T.; Kimura, T. Beyond resumption of the Japanese Government’s recommendation of the HPV vaccine. Lancet Oncol. 2018, 19, 1563–1564. [Google Scholar] [CrossRef]


{kind=link}
| 2009 | October | The bi-valent HPV vaccine was licensed. |
| 2010 | November | Subsidies from local and national governments for an HPV vaccination program for girls 13–16 commenced. |
| 2011 | July | The quadra-valent HPV vaccine was licensed. |
| 2013 | April | The national immunization program for girls aged 12–16 years commenced |
| June | The VARRC ruled that “It is necessary to determine the frequency of pain occurrence whose relationship can be undeniably linked to HPV vaccination. HPV vaccination should not be actively recommended until proper information can be provided to the public.” The VARRC announced the suspension of its recommendation for vaccination (Notification by the Director-General of the Health Service Bureau of the MHLW). | |
| 2014 | January and July | The VARRC evaluated the pathogenesis and causal relationship of the “diverse symptoms” reportedly experienced after HPV vaccination. The reported chronic pain and motor impairment were regarded as functional physical symptoms (a form of functional somatic syndrome). |
| 2015 | August | The “Guide for the Management and Treatment of Symptoms that Occur after HPV Vaccine Injection” was published. An organization of cooperative medical institutions from all 47 prefectures agreed to provide treatment for any girl suffering from symptoms after HPV vaccination in any community throughout Japan. The MHLW announced three measures for patients with symptoms, mainly of pain or movement disorders. |
| September | The result of the adverse events follow-up survey was released. The suspension of governmental recommendation was continued. The MHLW and the Ministry of Education, Culture, Sports, Science, and Technology issued their “Improvement of the Consultation and Support System for Persons with Symptoms after HPV Vaccination”. Relief (subsidies for medical expenses, etc.) based on the Immunization Law and the Pharmaceuticals and Medical Devices Agency Law, was implemented | |
| November | Symptom consultation services were established in the health and education departments of each prefecture. | |
| December | The VARRC evaluated the safety and efficacy of HPV vaccines in Japan and abroad. | |
| 2017 | April | The conclusions of a nationwide epidemiological survey by a research team designated by the MHLW were reported to the VARRC (Key finding: Unvaccinated girls had a similar number of “diverse symptoms”). |
| November | The VARRC evaluated all available information on the safety and efficacy of the HPV vaccine in Japan and abroad and expressed its commitment to continue to provide close support to patients who presented with any of the diverse symptoms. The VARRC discussed ways to better inform the public about the HPV vaccine. | |
| 2018 | January | An extensively revised informational leaflet was released by the MHLW to better inform the public about the HPV vaccine. |
| 2019 | August | The VARRC reported the results of a survey on the provision of HPV vaccine information. |
| 2020 | July | The “Parliamentary Association for the Resumption of Recommendation of HPV Vaccination” submitted a petition to the MHLW. The 9-valent HPV vaccine was licensed in Japan. |
| October | MHLW’s ‘Leaflet to Inform the Public about the HPV Vaccine’ was revised. | |
| December | The quadra-valent HPV vaccine was approved to prevent anal cancer for males. | |
| 2021 | August | “Parliamentary Association for the Resumption of Recommendation of HPV Vaccination” submitted a petition to the MHLW again. The Japanese Society of Obstetrics and Gynecology submitted a petition to the MHLW to extend the period of routine vaccination. |
| 1. Easy access to vaccination should be provided for women who are older than the normally targeted ages of 12–16 years who were not vaccinated during the vaccine recommendation hiatus. |
| 2. The 9-valent vaccine should be introduced into a national immunization program. |
| 3. Start a routine immunization program for boys of the same ages as the targeted girls. |
| 4. Cervical cancer screenings should be especially strongly recommended for women who have not been vaccinated. |
| 5. Special national action to revive HPV vaccination based on a behavioral economics approach. |
| 6. Provide accurate vaccination information to the media. |
| 7. Establish a vaccination registry and to verify the safety and efficacy of the vaccine. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagi, A.; Ueda, Y.; Kakuda, M.; Nakagawa, S.; Hiramatsu, K.; Miyoshi, A.; Kobayashi, E.; Kimura, T.; Kurosawa, M.; Yamaguchi, M.; et al. Cervical Cancer Protection in Japan: Where Are We? Vaccines 2021, 9, 1263. https://doi.org/10.3390/vaccines9111263
Yagi A, Ueda Y, Kakuda M, Nakagawa S, Hiramatsu K, Miyoshi A, Kobayashi E, Kimura T, Kurosawa M, Yamaguchi M, et al. Cervical Cancer Protection in Japan: Where Are We? Vaccines. 2021; 9(11):1263. https://doi.org/10.3390/vaccines9111263
Chicago/Turabian StyleYagi, Asami, Yutaka Ueda, Mamoru Kakuda, Satoshi Nakagawa, Kosuke Hiramatsu, Ai Miyoshi, Eiji Kobayashi, Toshihiro Kimura, Megumi Kurosawa, Manako Yamaguchi, and et al. 2021. "Cervical Cancer Protection in Japan: Where Are We?" Vaccines 9, no. 11: 1263. https://doi.org/10.3390/vaccines9111263