
Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials

 , , ,
, , , 
Abstract
:1. Introduction
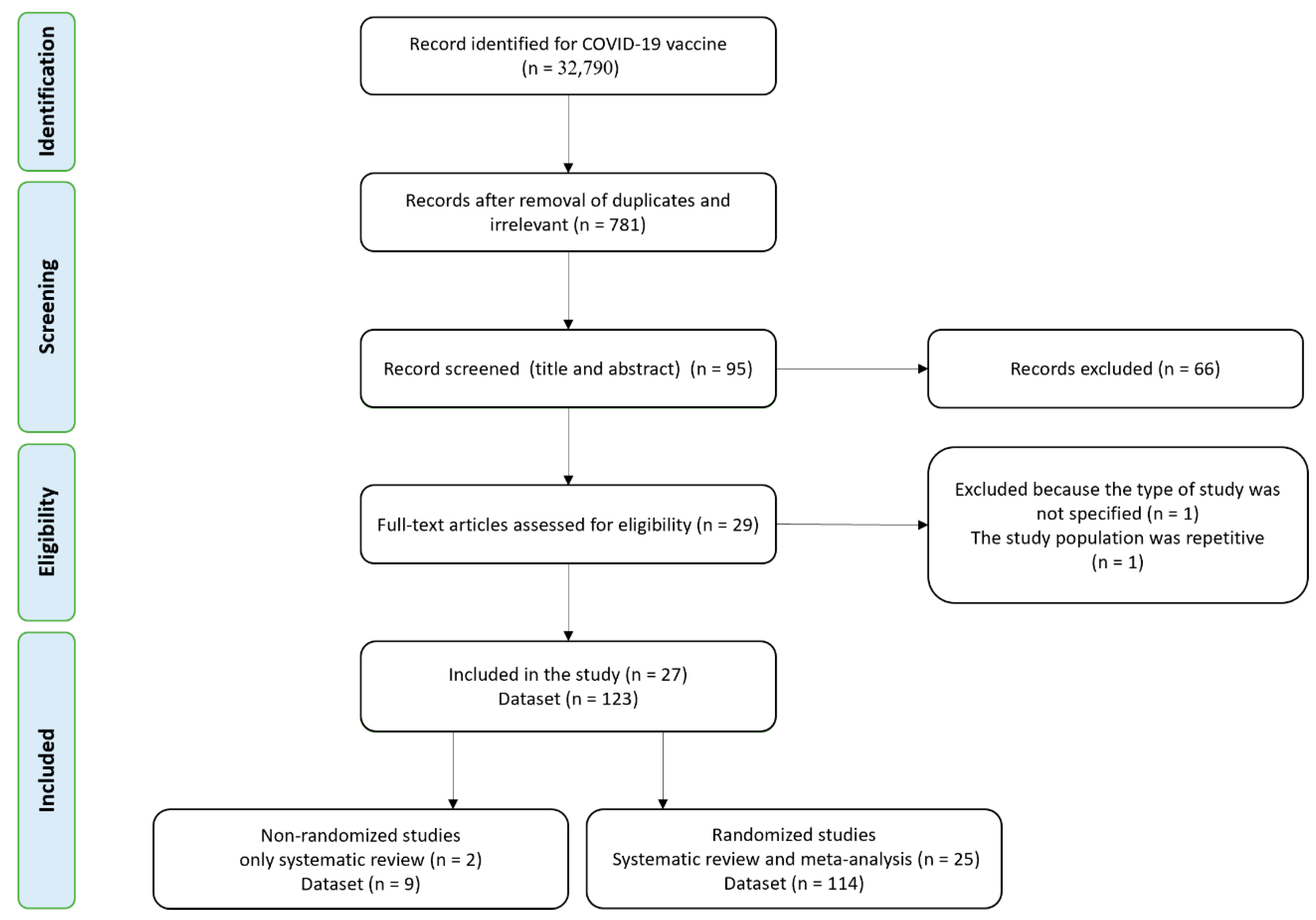
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Eligibility and Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Quality Assessment
2.7. Analysis
3. Result
3.1. Characteristics of Included Studies
3.2. Characteristics of Participants
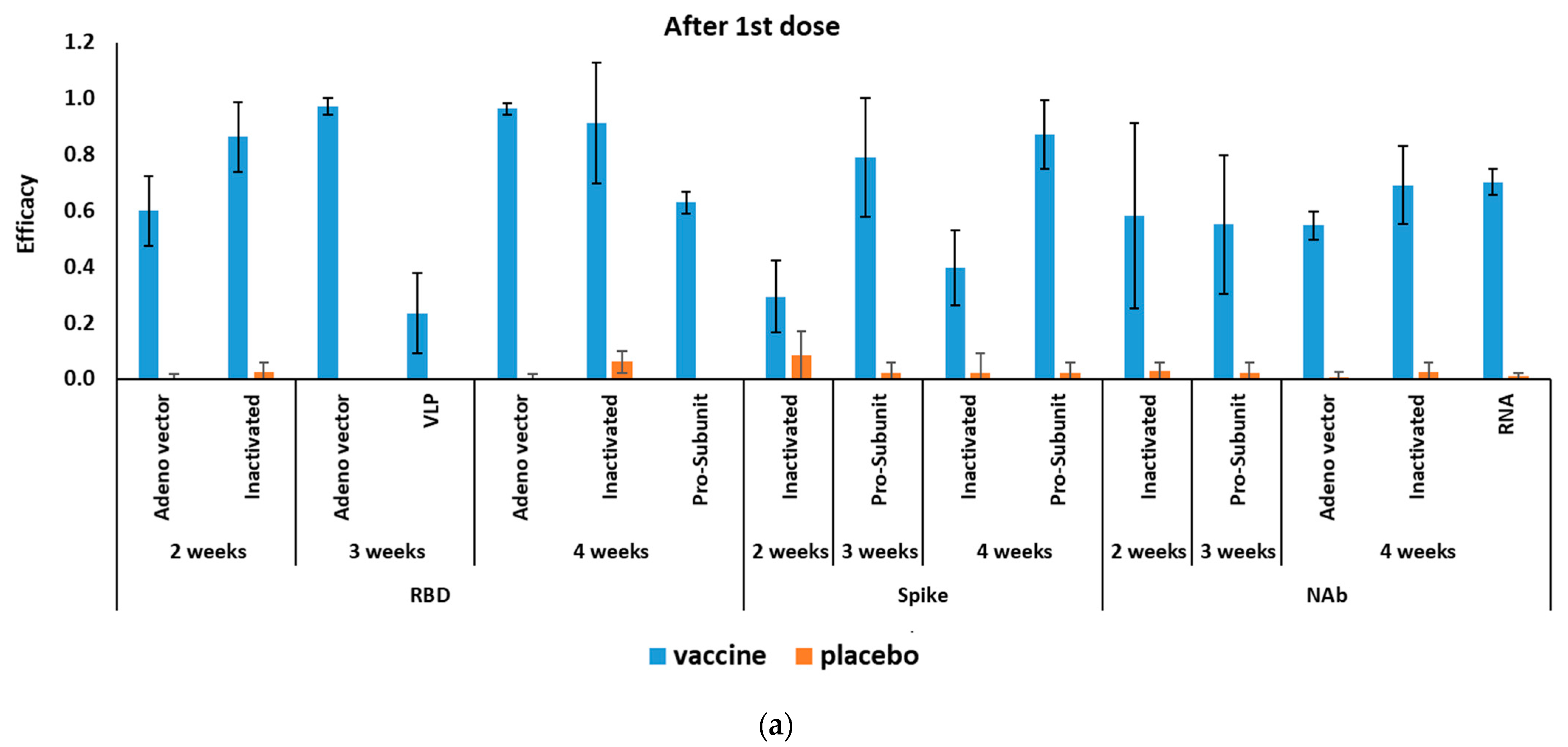
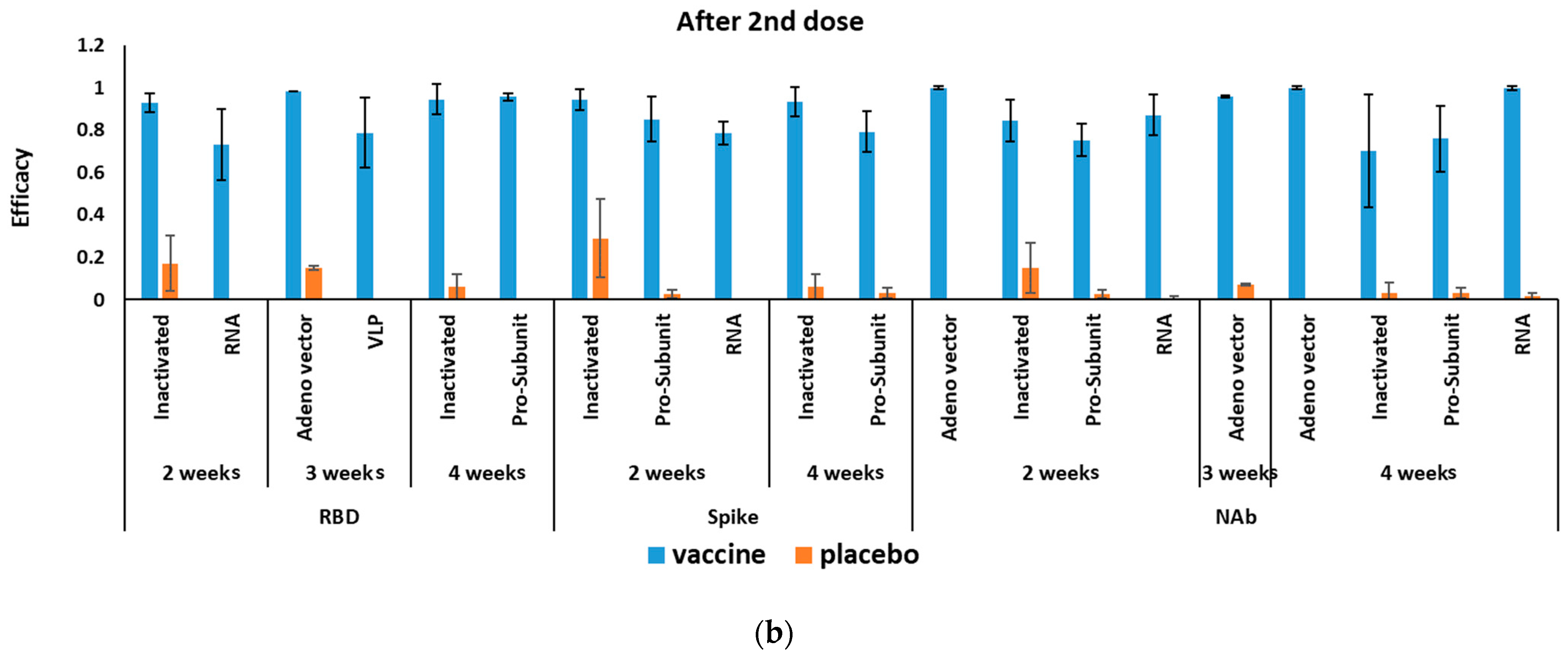
3.3. Efficacy of Different COVID-19 Vaccines
3.3.1. Efficacy of mRNA-Based COVID-19 Vaccines
3.3.2. Efficacy of Adenovirus-Vectored COVID-19 Vaccines
3.3.3. Efficacy of Inactivated COVID-19 Vaccines
3.3.4. Efficacy of Pro-Subunit COVID-19 Vaccines
3.3.5. Efficacy of VLP COVID-19 Vaccines
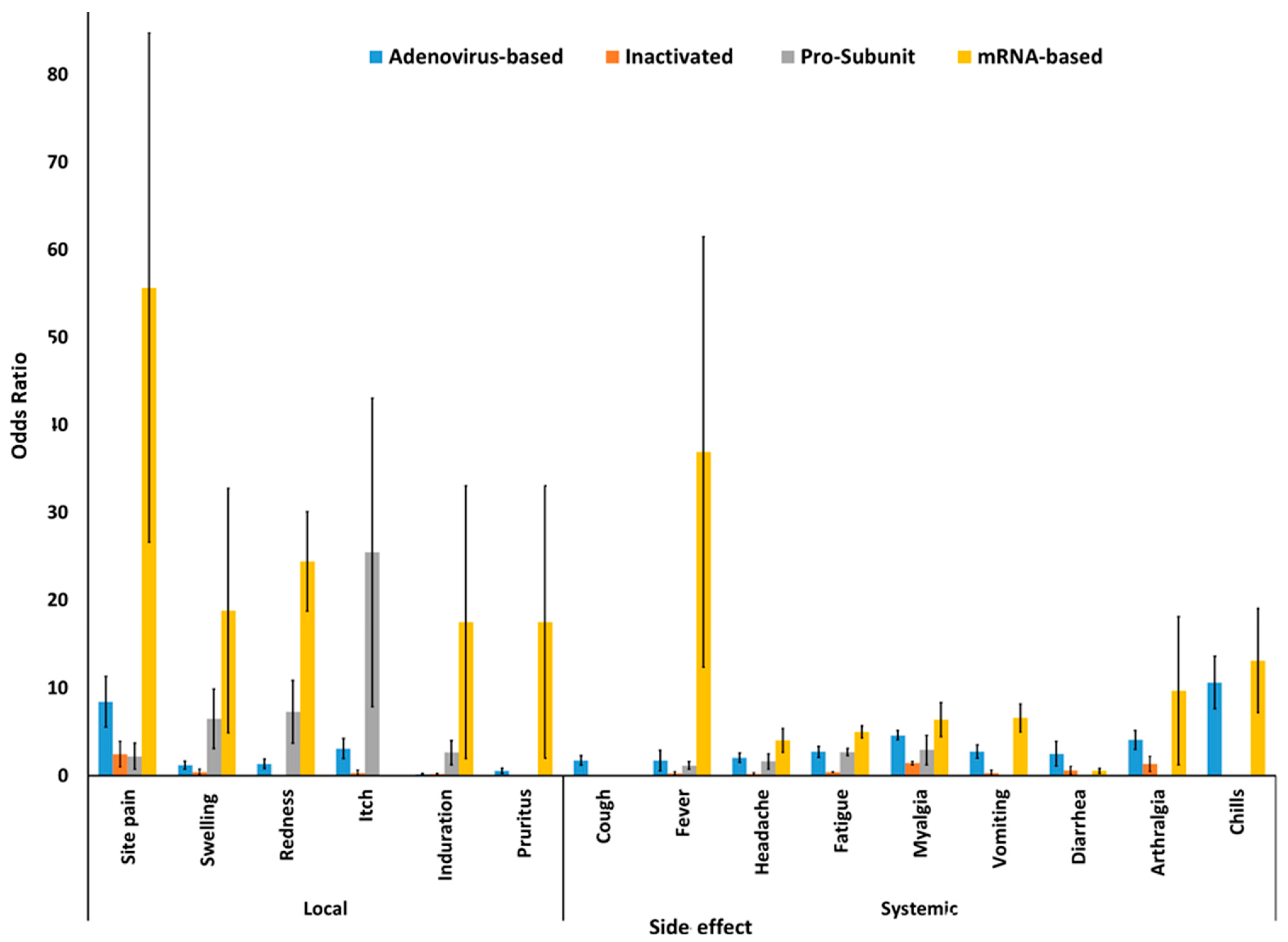
3.4. Side Effects of Different COVID-19 Vaccines
Serious Adverse Side Effects of COVID-19 Vaccines
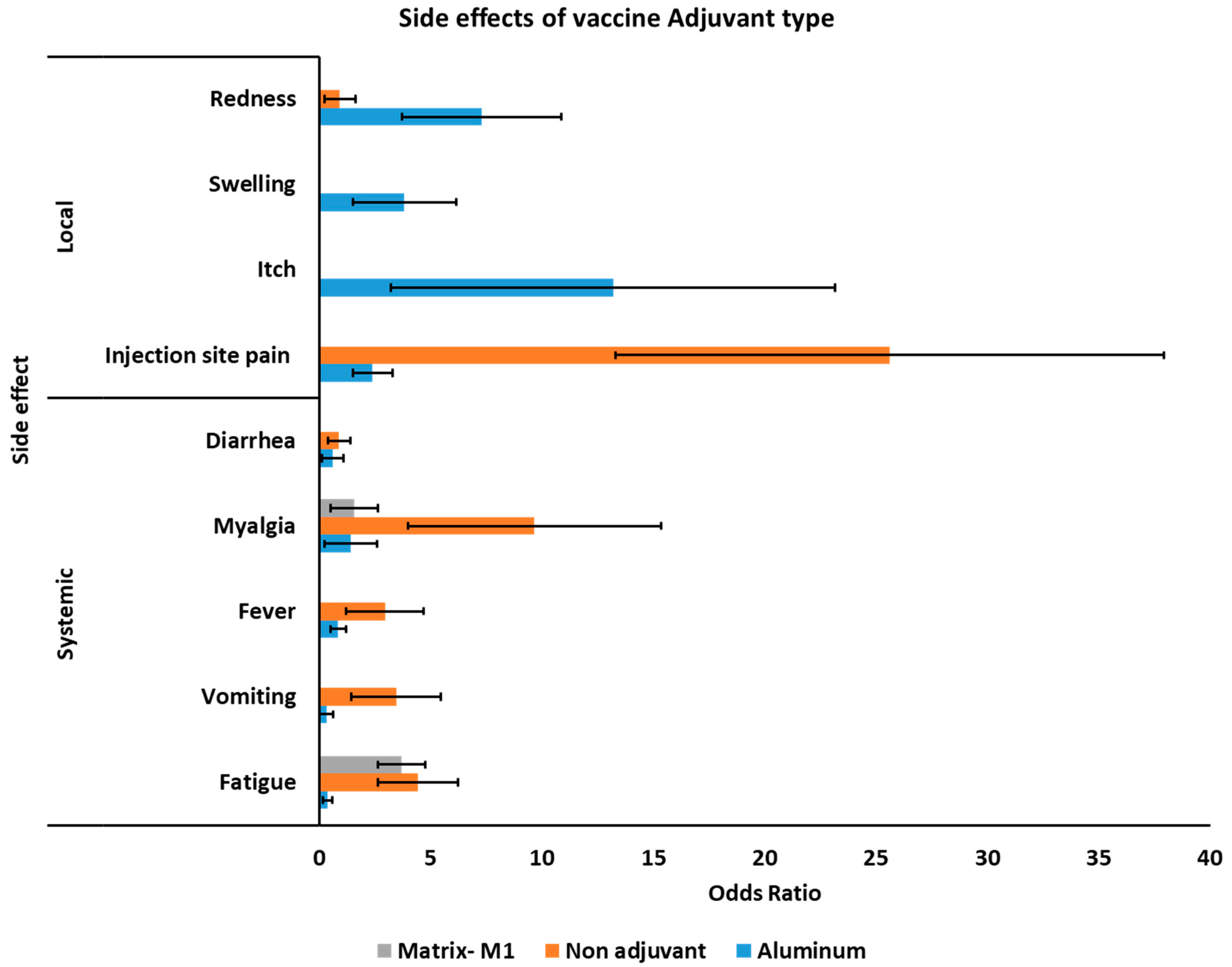
3.5. Side Effects of COVID-19 Vaccines Based on Different Adjuvants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PRISMA | The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement |
| MeSH | Medical subject headings |
| WHO | World Health Organization |
| CDC | Center for Disease Control |
| RCT | Randomized clinical trial |
| COVID-19 | Coronavirus disease 2019 |
| alum | Potassium aluminum sulfate |
| VLPs | Virus-like particles |
| ORs | Odds ratios |
| 6-HB | six-helical bundle |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| 95% CI | 95% confidence interval |
| GMT | Geometric mean titer |
| RBD | Receptor-binding domain |
| PLpro | Papain-like proteases |
| 3CLpro | Cysteine-like protease |
| NAb | Neutralizing antibody |
| Pro-subunit | Protein subunit |
| VLP | Virus-like particle |
| BMI | Body mass index |
| CFR | Case fatality ratio |
| RNA | Ribonucleic acid |
| messenger RNA | mRNA |
| S-protein | Spike protein |
| ACE2 | Angiotensin-converting enzyme 2 |
| nsp | Non-structural proteins |
| IM | Intramuscular |
References
- V’kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2020, 19, 1–16. [Google Scholar] [CrossRef]
- World Health Organization. Estimating Mortality from COVID-19: Scientific Brief, 4 August 2020; World Health Organization: Genova, Switzerland, 2020. [Google Scholar]
- Forni, G.; Mantovani, A. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef]
- World Health Organization. Draft Landscape and Tracker of COVID-19 Candidate Vaccines; World Health Organization: Genova, Switzerland, 2021. [Google Scholar]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Riel, D.; de Wit, E. Next-generation vaccine platforms for COVID-19. Nat. Mater. 2020, 19, 810–812. [Google Scholar] [CrossRef]
- Sanders, B.; Koldijk, M.; Schuitemaker, H. Inactivated viral vaccines. In Vaccine Analysis: Strategies, Principles, and Control; Springer: Berlin/Heidelberg, Germany, 2015; pp. 45–80. [Google Scholar]
- Kyriakidis, N.C.; López-Cortés, A.; González, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. npj Vaccines 2021, 6, 1–17. [Google Scholar] [CrossRef]
- Roldão, A.; Mellado, M.C.M.; Castilho, L.R.; Carrondo, M.J.; Alves, P.M. Virus-like particles in vaccine development. Expert Rev. Vaccines 2010, 9, 1149–1176. [Google Scholar] [CrossRef] [PubMed]
- Bosch, B.J.; Van der Zee, R.; De Haan, C.A.; Rottier, P.J. The coronavirus spike protein is a class I virus fusion protein: Structural and functional characterization of the fusion core complex. J. Virol. 2003, 77, 8801–8811. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Dai, T.; Wei, Y.; Zhang, L.; Zheng, M.; Zhou, F. A systematic review of SARS-CoV-2 vaccine candidates. Signal Transduct. Target. Ther. 2020, 5, 1–14. [Google Scholar] [CrossRef]
- Ong, E.; Wong, M.U.; Huffman, A.; He, Y. COVID-19 coronavirus vaccine design using reverse vaccinology and machine learning. Front. Immunol. 2020, 11, 1581. [Google Scholar] [CrossRef]
- Dhama, K.; Sharun, K.; Tiwari, R.; Dadar, M.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W. COVID-19, an emerging coronavirus infection: Advances and prospects in designing and developing vaccines, immunotherapeutics, and therapeutics. Hum. Vaccines Immunother. 2020, 16, 1232–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. Bmj 2000, 320, 1574–1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. Jama 2006, 295, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Li, Y.; Dai, L.; Wang, J.; He, P.; Li, C.; Fang, X.; Wang, C.; Zhao, X.; Huang, E. Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD protein vaccine against COVID-19 in adults: Pooled analysis of two randomized, double-blind, placebo-controlled, phase 1 and 2 trials. medRxiv 2020. [Google Scholar] [CrossRef]
- Ella, R.; Vadrevu, K.M.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.; Ganneru, B.; Sapkal, G.; Yadav, P.; Abraham, P. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: A double-blind, randomised, phase 1 trial. Lancet Infect. Dis. 2021, 21, 637–646. [Google Scholar] [CrossRef]
- Zhu, F.-C.; Li, Y.-H.; Guan, X.-H.; Hou, L.-H.; Wang, W.-J.; Li, J.-X.; Wu, S.-P.; Wang, B.-S.; Wang, Z.; Wang, L. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Richmond, P.; Hatchuel, L.; Dong, M.; Ma, B.; Hu, B.; Smolenov, I.; Li, P.; Liang, P.; Han, H.H.; Liang, J. Safety and immunogenicity of S-Trimer (SCB-2019), a protein subunit vaccine candidate for COVID-19 in healthy adults: A phase 1, randomised, double-blind, placebo-controlled trial. Lancet 2021, 397, 682–694. [Google Scholar] [CrossRef]
- Oostvogels, L.; Kremsner, P.; Kreidenweiss, A.; Leroux-Roels, I.; Leroux-Roels, G.; Kroidl, A.; Schunk, M.; Schindler, C.; Bosch, J.; Fendel, R. Phase 1 assessment of the safety and immunogenicity of an mRNA-lipid nanoparticle vaccine candidate against SARS-CoV-2 in human volunteers. medRxiv 2020. [Google Scholar] [CrossRef]
- Ward, B.J.; Gobeil, P.; Seguin, A.; Atkins, J.; Boulay, I.; Charbonneau, P.-Y.; Couture, M.; D’Aoust, M.-A.; Dhaliwall, J.; Finkle, C. Phase 1 trial of a Candidate Recombinant Virus-Like Particle Vaccine for Covid-19 Disease Produced in Plants. medRxiv 2020. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J. An mRNA vaccine against SARS-CoV-2—Preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. N. Engl. J. Med. 2020, 383, 2320–2332. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D. COVID-19 vaccine BNT162b1 elicits human antibody and TH 1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N. Engl. J.Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Duan, K.; Zhang, Y.; Zhao, D.; Zhang, H.; Xie, Z.; Li, X.; Peng, C.; Zhang, Y.; Zhang, W. Effect of an inactivated vaccine against SARS-CoV-2 on safety and immunogenicity outcomes: Interim analysis of 2 randomized clinical trials. Jama 2020, 324, 951–960. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2020, 21, 181–192. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V.; Tukhvatullin, A.I.; Shcheblyakov, D.V.; Dzharullaeva, A.S.; Grousova, D.M.; Erokhova, A.S.; Kovyrshina, A.V.; Botikov, A.G. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: Two open, non-randomised phase 1/2 studies from Russia. Lancet 2020, 396, 887–897. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Chu, L.; McPhee, R.; Huang, W.; Bennett, H.; Pajon, R.; Nestorova, B.; Leav, B. mRNA-1273 Study Group. A preliminary report of a randomized controlled phase 2 trial of the safety and immunogenicity of mRNA-1273 SARS-CoV-2 vaccine. Vaccine 2021. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I. Interim Results of a Phase 1–2a Trial of Ad26. COV2. S Covid-19 Vaccine. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: WHO Says Rollout of AstraZeneca Vaccine Should Continue, as Europe Divides over Safety; British Medical Journal Publishing Group: London, UK, 2021. [Google Scholar]
- Muik, A.; Wallisch, A.-K.; Sänger, B.; Swanson, K.A.; Mühl, J.; Chen, W.; Cai, H.; Maurus, D.; Sarkar, R.; Türeci, Ö. Neutralization of SARS-CoV-2 lineage B. 1.1. 7 pseudovirus by BNT162b2 vaccine–elicited human sera. Science 2021, 371, 1152–1153. [Google Scholar] [CrossRef]
- Shen, X.; Tang, H.; McDanal, C.; Wagh, K.; Fischer, W.; Theiler, J.; Yoon, H.; Li, D.; Haynes, B.F.; Sanders, K.O. SARS-CoV-2 variant B. 1.1. 7 is susceptible to neutralizing antibodies elicited by ancestral Spike vaccines. Cell Host Microbe 2021, 29, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Arora, P.; Groß, R.; Seidel, A.; Hörnich, B.; Hahn, A.; Krüger, N.; Graichen, L.; Hofmann-Winkler, H.; Kempf, A. SARS-CoV-2 variants B. 1.351 and B. 1.1. 248: Escape from therapeutic antibodies and antibodies induced by infection and vaccination. BioRxiv 2021. [Google Scholar] [CrossRef]
- Mascola, J.R.; Graham, B.S.; Fauci, A.S. SARS-CoV-2 Viral Variants—Tackling a Moving Target. Jama 2021, 325, 1261–1262. [Google Scholar] [CrossRef] [PubMed]
- Wibmer, C.K.; Ayres, F.; Hermanus, T.; Madzivhandila, M.; Kgagudi, P.; Oosthuysen, B.; Lambson, B.E.; de Oliveira, T.; Vermeulen, M.; van der Berg, K. SARS-CoV-2 501Y. V2 escapes neutralization by South African COVID-19 donor plasma. Nat. Med. 2021, 27, 622–625. [Google Scholar] [CrossRef]
- Yuan, P.; Ai, P.; Liu, Y.; Ai, Z.; Wang, Y.; Cao, W.; Xia, X.; Zheng, J.C. Safety, Tolerability, and Immunogenicity of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Available online: https://pubmed.ncbi.nlm.nih.gov/33173896/ (accessed on 4 November 2020).
- Wise, J. Covid-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ 2021. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID-19 Vaccinations in the United States; Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/reporting-vaccinations.html (accessed on 22 April 2021).
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, K.G.; Robinson, L.B.; Camargo, C.A.; Shenoy, E.S.; Banerji, A.; Landman, A.B.; Wickner, P. Acute Allergic Reactions to mRNA COVID-19 Vaccines. JAMA 2021, 325, 1562–1565. [Google Scholar] [CrossRef] [PubMed]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N. Allergic Reactions to Current Available COVID-19 Vaccinations: Pathophysiology, Causality, and Therapeutic Considerations. Vaccines 2021, 9, 221. [Google Scholar] [CrossRef]
- Cines, D.B.; Bussel, J.B. SARS-CoV-2 Vaccine–Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Liang, Z.; Zhu, H.; Wang, X.; Jing, B.; Li, Z.; Xia, X.; Sun, H.; Yang, Y.; Zhang, W.; Shi, L. Adjuvants for coronavirus vaccines. Front. Immunol. 2020, 11, 2896. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Trial Initiation Date | Pub. Year | Vaccine Name | Company | Study Type | Vaccine Type | Adjuvant | Store Temp (°C) | RCT Phase | Dose (s) | Age Range (Year) | Injection Interval (Days) | Concentration | Trial Country | Ref |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yang et al. | 22 June and 3 July 2020 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | I | 3 | 22.9–54.7 | 30 | 25 μg * | China | [18] |
| Yang et al. | 22 June and 3 July 2020 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | I | 3 | 20.9–49.4 | 30 | 50 μg * | China | [18] |
| Ella et al. | 13 and 30 July 2020 | 2021 | BBV152 (Covaxin) | Bharat Biotech | Randomized, double-blind, placebo-controlled | Inactivated | Algel-IMDG | 2–8 | I | 2 | 18–55 | 14 | 3 μg * | India | [19] |
| Ella et al. | 13 and 30 July 2020 | 2021 | BBV152 (Covaxin) | Bharat Biotech | Randomized, double-blind, placebo-controlled | Inactivated | Algel-IMDG | 2–8 | I | 2 | 18–55 | 14 | 6 μg * | India | [19] |
| Ella et al. | 13 and 30 July 2020 | 2021 | BBV152 (Covaxin) | Bharat Biotech | Randomized, double-blind, placebo-controlled | Inactivated | Algel | 2–8 | I | 2 | 18–55 | 14 | 6 μg* | India | [19] |
| Zhu et al. | 16 and 27 March 2020 | 2020 | Ad5-nCoV | CanSino | Non-randomized | Adenovirus-based | No adjuvant | UN | I | 1 | 18–60 | No | 5 × 101⁰ VP * | China | [20] |
| Zhu et al. | 16 and 27 March 2020 | 2020 | Ad5-nCoV | CanSino | Non-randomized | Adenovirus-based | No adjuvant | UN | I | 1 | 18–60 | No | 1 × 1011 VP * | China | [20] |
| Zhu et al. | 16 and 27 March 2020 | 2020 | Ad5-nCoV | CanSino | Non-randomized | Adenovirus-based | No adjuvant | UN | I | 1 | 18–60 | No | 1.5 × 1011 VP * | China | [20] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | No adjuvant | 2–8 | I | 2 | 20–50 | 21 | 3 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 24–53 | 21 | 3 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 55–70 | 21 | 3 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 20–53 | 21 | 3 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 55–71 | 21 | 3 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | No adjuvant | 2–8 | I | 2 | 20–54 | 21 | 9 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 21–53 | 21 | 9 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 55–64 | 21 | 9 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 19–55 | 21 | 9 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 55–67 | 21 | 9 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | No adjuvant | 2–8 | I | 2 | 18–49 | 21 | 30 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 19–47 | 21 | 30 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | AS03 | 2–8 | I | 2 | 55–63 | 21 | 30 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 21–50 | 21 | 30 μg * | Australia | [21] |
| Richmond et al. | 19 June and 23 September 2020 | 2021 | SCB-2019 | Clover | Randomized, double-blind, placebo-controlled | Pro-Subunit | CpG/Alum | 2–8 | I | 2 | 55–74 | 21 | 30 μg * | Australia | [21] |
| Kremsner et al. | June, 2020 | 2020 | CVnCoV | Curevac | Randomized, partially blind, placebo-controlled | mRNA-based | No adjuvant | 5 | I | 2 | 18–60 | 28 | 2 μg * | Germany | [22] |
| Kremsner et al. | June, 2020 | 2020 | CVnCoV | Curevac | Randomized, partially blind, placebo-controlled | mRNA-based | No adjuvant | 5 | I | 2 | 19–59 | 28 | 4 μg * | Germany | [22] |
| Kremsner et al. | June, 2020 | 2020 | CVnCoV | Curevac | Randomized, partially blind, placebo-controlled | mRNA-based | No adjuvant | 5 | I | 2 | 20–59 | 28 | 6 μg * | Germany | [22] |
| Kremsner et al. | June, 2020 | 2020 | CVnCoV | Curevac | Randomized, partially blind, placebo-controlled | mRNA-based | No adjuvant | 5 | I | 2 | 20–59 | 28 | 8 μg * | Germany | [22] |
| Kremsner et al. | June, 2020 | 2020 | CVnCoV | Curevac | Randomized, partially blind, placebo-controlled | mRNA-based | No adjuvant | 5 | I | 2 | 19–59 | 28 | 12 μg * | Germany | [22] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | No adjuvant | 2–8 | I | 2 | 18–55 | 21 | 3.75 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | CpG 1018 | 2–8 | I | 2 | 18–55 | 21 | 3.75 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | AS03 | 2–8 | I | 2 | 18–55 | 21 | 3.75 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | No adjuvant | 2–8 | I | 2 | 18–55 | 21 | 7.5 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | CpG 1018 | 2–8 | I | 2 | 18–55 | 21 | 7.5 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | AS03 | 2–8 | I | 2 | 18–55 | 21 | 7.5 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | No adjuvant | 2–8 | I | 2 | 18–55 | 21 | 15 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | CpG 1018 | 2–8 | I | 2 | 18–55 | 21 | 15 μg * | Canada | [23] |
| Ward et al. | July, 2020 | 2020 | CoVLP | Medicago | Randomized, partially blind | VLP | AS03 | 2–8 | I | 2 | 18–55 | 21 | 15 μg | Canada | [23] |
| Jackson et al. | 16 March and 14 April 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 18–55 | 28 | 25 μg * | United States | [24] |
| Jackson et al. | 16 March and 14 April 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 18–55 | 28 | 100 mg * | United States | [24] |
| Jackson et al. | 16 March and 14 April 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 18–55 | 28 | 250 mg * | United States | [24] |
| Anderson et al. | 16 April and 12 May 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 56–70 | 28 | 25 mg * | United States | [25] |
| Anderson et al. | 16 April and 12 May 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 71≤ | 28 | 25 mg * | United States | [25] |
| Anderson et al. | 16 April and 12 May 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 56–70 | 28 | 100 mg * | United States | [25] |
| Anderson et al. | 16 April and 12 May 2020 | 2020 | mRNA-1273 | Moderna | Open-label | mRNA-based | No adjuvant | −20 | I | 2 | 71≤ | 28 | 100 mg * | United States | [25] |
| Keech et al. | 26 May and 6 June 2020 | 2020 | NVX-CoV2373 | Novavax | Randomized, observer-blind, placebo-controlled | Pro-Subunit | No adjuvant | 2–8 | I | 2 | 18–59 | 21 | 25 μg/0.6 ml | Australia, United States | [26] |
| Keech et al. | 26 May and 6 June 2020 | 2020 | NVX-CoV2373 | Novavax | Randomized, observer-blind, placebo-controlled | Pro-Subunit | Matrix-M1 | 2–8 | I | 2 | 18–59 | 21 | 5 μg/0.6 ml | Australia, United States | [26] |
| Keech et al. | 26 May and 6 June 2020 | 2020 | NVX-CoV2373 | Novavax | Randomized, observer-blind, placebo-controlled | Pro-Subunit | Matrix-M1 | 2–8 | I | 2 | 18–59 | 21 | 25 μg/0.6 ml | Australia, United States | [26] |
| Keech et al. | 26 May and 6 June 2020 | 2020 | NVX-CoV2373 | Novavax | Randomized, observer-blind, placebo-controlled | Pro-Subunit | Matrix-M1 | 2–8 | I | 1 | 18–59 | 21 | 25 μg/0.6 ml | Australia, United States | [26] |
| Sahin et al. | 23 April and 22 May 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, single-blind | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 1 μg * | Germany | [27] |
| Sahin et al. | 23 April and 22 May 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, single-blind | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 21.4–55.8 | 21 | 10 μg * | Germany | [27] |
| Sahin et al. | 23 April and 22 May 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, single-blind | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 25.1–55 | 21 | 30 μg * | Germany | [27] |
| Sahin et al. | 23 April and 22 May 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, single-blind | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 23.9–54 | 21 | 50 μg * | Germany | [27] |
| Sahin et al. | 23 April and 22 May 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, single-blind | mRNA-based | No adjuvant | (−60)–(−80) | I | 1 | 19.9–47.8 | No | 60 μg * | Germany | [27] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 20.9–53.2 | 21 | 10 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 10 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 65–85 | 21 | 20 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 20 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 65–85 | 21 | 30 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | 1 | 2 | 18–55 | 21 | 30 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 65–85 | 21 | 10 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 10 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 65–85 | 21 | 20 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 20 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 65–85 | 21 | 30 μg * | United States, Germany | [28] |
| Walsh et al. | 4 May and 22 June 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I | 2 | 18–55 | 21 | 30 μg * | United States, Germany | [28] |
| Xia et al. | 12 April and 2 May 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 3 | 65–85 | 28 | 2.5 μg * | China | [29] |
| Xia et al. | 12 April and 2 May 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 3 | 18–59 | 28 | 5 μg * | China | [29] |
| Xia et al. | 12 April and 2 May 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 3 | 18–59 | 28 | 10 μg * | China | [29] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 2 μg * | China | [30] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 2 μg * | China | [30] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 60 ≤ | 28 | 4 μg * | China | [30] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 4 μg * | China | [30] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 60 ≤ | 28 | 8 μg * | China | [30] |
| Xia et al. | 29 April and 28 June 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 8 μg * | China | [30] |
| Zhang et al. | 16 and 25 April 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 60≤ | 14 | 3 μg * | China | [31] |
| Zhang et al. | 16 and 25 April 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 3 μg * | China | [31] |
| Zhang et al. | 16 and 25 April 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 14 | 6 μg * | China | [31] |
| Zhang et al. | 16 and 25 April 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | I | 2 | 18–59 | 28 | 6 μg * | China | [31] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | I | 1 | 18–59 | No | 1011 VP * | Russia | [32] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | I | 1 | 18–60 | No | 1011 * | Russia | [32] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V (Lyo) | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | I | 1 | 18–60 | No | 1011 * | Russia | [32] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V (Lyo) | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | I | 1 | 18–60 | No | 1011 * | Russia | [32] |
| Folegatti et al. | 23 April and 21 May 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | I/II | 2 | 18–60 | 28 | 5 × 101⁰ VP * | United Kingdom | [33] |
| Mulligan et al. | 4 May and 19 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I/II | 2 | 18–55 | 21 | 10 μg * | Multicenter 1 | [34] |
| Mulligan et al. | 4 May and 19 June,2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I/II | 2 | 24–42 | 21 | 30 μg * | Multicenter 1 | [34] |
| Mulligan et al. | 4 May and 19 June 2020 | 2020 | BNT162b1 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | I/II | 1 | 23–52 | No | 100 μg * | Multicenter 1 | [34] |
| Yang et al. | 12 and 17 July 2020 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | II | 2 | 25–53 | 30 | 25 μg * | China | [18] |
| Yang et al. | 12 and 17 July 2021 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | II | 2 | 18.8–58.4 | 30 | 50 μg * | China | [18] |
| Yang et al. | 12 and 17 July 2022 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | II | 3 | 19.9–59.1 | 30 | 25 μg * | China | [18] |
| Yang et al. | 12 and 17 July 2023 | 2020 | ZF2001 | Anhui Zhifei Longcom | Randomized, double-blind, placebo-controlled | Pro-Subunit | Aluminum hydroxide | 2–8 | II | 3 | 20–59.7 | 30 | 50 μg * | China | [18] |
| Zhu et al. | 11 and 16 April 2020 | 2020 | Ad5-nCoV | CanSino | Randomized, double-blind, placebo-controlled | Adenovirus-based | No adjuvant | UN | II | 1 | 19.3–59.6 | No | 1 × 1011 * | China | [35] |
| Zhu et al. | 11 and 16 April 2020 | 2020 | Ad5-nCoV | CanSino | Randomized, double-blind, placebo-controlled | Adenovirus-based | No adjuvant | UN | II | 1 | 18≤ | No | 5 × 101⁰ * | China | [35] |
| Chu et al. | 29 May and 8 July 2020 | 2020 | mRNA-1273 | Moderna | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | −20 | II | 2 | 18≤ | 28 | 50 mg * | United States | [36] |
| Chu et al. | 29 May and 8 July 2020 | 2020 | mRNA-1273 | Moderna | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | −20 | II | 2 | 18–54.99 | 28 | 50 mg * | United States | [36] |
| Chu et al. | 29 May and 8 July 2020 | 2020 | mRNA-1273 | Moderna | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | −20 | II | 2 | 55≤ | 28 | 100 mg * | United States | [36] |
| Chu et al. | 29 May and 8 July 2020 | 2020 | mRNA-1273 | Moderna | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | −20 | II | 2 | 18–54.99 | 28 | 100 mg * | United States | [36] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 55≤ | 28 | 2.2 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 1 | 18–55 | No | 2.2 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 56–69 | 28 | 2.2 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 1 | 56–69 | No | 2.2 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 70≤ | 28 | 2.2 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 70≤ | 28 | 3.5–6.5 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 1 | 18–55 | No | 3.5–6.5 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 56–69 | 28 | 3.5–6.5 × 101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 1 | 56–69 | No | 3.5–6.5 ×101⁰ VP * | United Kingdom | [37] |
| Ramasamy et al. | 30 May and 8 August 2020 | 2020 | AZD1222 | Oxford/AstraZeneca | Randomized, participant-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 70≤ | 28 | 3.5–6.5 × 101⁰ VP * | United Kingdom | [37] |
| Xia et al. | 12 April and 2 May 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 3 | 70≤ | 28 | 5 μg * | China | [29] |
| Xia et al. | 12 April and 2 May 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 3 | 18–59 | 28 | 5 μg * | China | [29] |
| Xia et al. | 18 May and 30 July 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 1 | 18–59 | No | 8 μg * | China | [30] |
| Xia et al. | 18 May and 30 July 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 14 | 4 μg * | China | [30] |
| Xia et al. | 18 May and 30 July 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 21 | 4 μg * | China | [30] |
| Xia et al. | 18 May and 30 July 2020 | 2020 | BBIBP-CorV | Sinopharm | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 28 | 4 μg * | China | [30] |
| Zhang et al. | 3 and 5 May 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 14 | 3 μg * | China | [31] |
| Zhang et al. | 3 and 5 May 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 28 | 3 μg * | China | [31] |
| Zhang et al. | 3 and 5 May 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 14 | 6 μg * | China | [31] |
| Zhang et al. | 3 and 5 May 2020 | 2020 | CoronaVac | Sinovac | Randomized, double-blind, placebo controlled | Inactivated | Aluminum hydroxide | 2–8 | II | 2 | 18–59 | 28 | 6 μg * | China | [31] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 18–59 | 21 | 1011 VP * | Russia | [32] |
| Logunov et al. | 18 June and 3 August 2020 | 2020 | Sputnik V (lyophilised) | Gamaleya | Non-randomized | Adenovirus-based | No adjuvant | 2–8 | II | 2 | 18–60 | 21 | 1011 VP * | Russia | [32] |
| Voysey et al. | 23 April and 4 November 2020 | 2021 | AZD1222 | Oxford/AstraZeneca | Randomized, single-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II/III | 2 | 18–60 | 28 | 2.2 × 101⁰ VP * (1st)/5 × 101⁰ VP * (2nd) | United Kingdom | [38] |
| Voysey et al. | 23 April and 4 November 2020 | 2021 | AZD1222 | Oxford/AstraZeneca | Randomized, single-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | II/III | 2 | 18≤ | 28 | 5 × 101⁰ VP * | United Kingdom | [38] |
| Pollack et al. | 27 July and 14 November 2020 | 2020 | BNT162b2 | Pfizer/BioNTech | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | (−60)–(−80) | II/III | 2 | 18≤ | 21 | 30 μg/0.3 ml | Multinational 1 | [39] |
| Baden et al. | 27 July and 23 October | 2020 | mRNA-1273 | Moderna | Randomized, observer-blind, placebo-controlled | mRNA-based | No adjuvant | −20 | III | 2 | 16–89 | 28 | 100 μg * | United States | [40] |
| Voysey et al. | 23 April and 4 November 2020 | 2021 | AZD1222 | Oxford/AstraZeneca | Randomized, single-blind, placebo-controlled | Adenovirus-based | No adjuvant | 2–8 | III | 2 | 18–95 | 28 | 5 × 101⁰ VP * | Brazil | [38] |
| Logunov et al. | 7 September and 24 November 2020 | 2021 | Sputnik V | Gamaleya | Randomized, double-blind, placebo controlled | Adenovirus-based | No adjuvant | 2–8 | III | 2 | 18≤ | 21 | 1011 VP * | Russia | [41] |
| Sadoff et al. | 20 July 2020 | 2021 | Ad26.COV2.S | Johnson & Johnson | Randomized, double-blind, placebo-controlled | Adenoviral vector | No adjuvant | UN | I/II | 2 | 18–55 | No | 5 × 1010 | Belgium, US | [42] |
| Sadoff et al. | 20 July 2020 | 2021 | Ad26.COV2.S | Johnson & Johnson | Randomized, double-blind, placebo-controlled | Adenoviral vector | No adjuvant | UN | I/II | 2 | 19–55 | No | 1 × 1011 | Belgium, US | [42] |
| Sadoff et al. | November 2020 | 2021 | Ad26.COV2.S | Johnson & Johnson | Randomized, double-blind, placebo-controlled | Adenoviral vector | No adjuvant | UN | I/II | 2 | 65–83 | No | 5 × 1010 | Belgium, US | [42] |
| Sadoff et al. | November 2020 | 2021 | Ad26.COV2.S | Johnson & Johnson | Randomized, double-blind, placebo-controlled | Adenoviral vector | No adjuvant | UN | I/II | 2 | 65–88 | No | 1 × 1011 | Belgium, US | [42] |
| Vaccine Type | RCT Phase | Number Studies | Efficacy (%) | 95% CI (%) | Included Case N | Heterogeneity Test, p-Value | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Adenovirus-based | 2/3 | 4 | 80.2 | 0.564 | 0.927 | 20771 | <0.001 |
| mRNA-based | 2/3 | 2 | 94.6 | 0.936 | 0.954 | 34041 | <0.001 |
| Vaccine | Placebo | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shot | Antigen/Antibody | After Injection (Week) | Vaccine Type | Studies N | Efficacy | Lower Limit | Upper Limit | I-Squared | Studies N | Efficacy | Lower Limit | Upper Limit | I-Squared |
| After 1st dose | RBD | 2 | Adenovirus-based | 4 | 0.603 | 0.471 | 0.722 | 73.8 | 2 | 0.004 | 0.001 | 0.027 | 0 |
| Inactivated | 4 | 0.870 | 0.734 | 0.983 | 93.8 | 4 | 0.024 | 0.008 | 0.072 | 0 | |||
| 3 | Adenovirus-based | 2 | 0.976 | 0.939 | 0.997 | 0.0 | NA | NA | NA | NA | NA | ||
| VLP | 8 | 0.238 | 0.091 | 0.375 | 84.3 | NA | NA | NA | NA | NA | |||
| 4 | Adenovirus-based | 2 | 0.966 | 0.942 | 0.980 | 0.0 | 2 | 0.004 | 0.001 | 0.027 | 0 | ||
| Inactivated | 4 | 0.913 | 0.564 | 0.958 | 90.7 | 4 | 0.061 | 0.033 | 0.110 | 0 | |||
| Pro-Subunit | 6 | 0.628 | 0.590 | 0.665 | 0.0 | NA | NA | NA | NA | NA | |||
| S-protein | 2 | Inactivated | 2 | 0.293 | 0.182 | 0.437 | 0.0 | 2 | 0.083 | 0.032 | 0.202 | 0 | |
| 3 | Pro-Subunit | 4 | 0.790 | 0.474 | 0.874 | 91.0 | 4 | 0.021 | 0.005 | 0.079 | 0 | ||
| 4 | Inactivated | 2 | 0.396 | 0.269 | 0.539 | 0.0 | 2 | 0.021 | 0.003 | 0.134 | 0 | ||
| Pro-Subunit | 4 | 0.873 | 0.671 | 0.892 | 91.9 | 4 | 0.021 | 0.005 | 0.079 | 0 | |||
| NAb | 2 | Inactivated | 4 | 0.583 | 0.210 | 0.868 | 95.0 | 4 | 0.030 | 0.013 | 0.070 | 0 | |
| 3 | Pro-Subunit | 4 | 0.551 | 0.291 | 0.786 | 85.0 | 4 | 0.021 | 0.005 | 0.079 | 0 | ||
| 4 | Adenovirus-based | 2 | 0.547 | 0.496 | 0.596 | 76.8 | 2 | 0.008 | 0.002 | 0.031 | 0 | ||
| Inactivated | 4 | 0.691 | 0.537 | 0.812 | 95.0 | 4 | 0.025 | 0.008 | 0.074 | 0 | |||
| mRNA-based | 4 | 0.702 | 0.655 | 0.746 | 73.9 | 4 | 0.010 | 0.004 | 0.026 | 0 | |||
| After 2nd dose | RBD | 2 | Inactivated | 9 | 0.929 | 0.876 | 0.960 | 61.8 | 9 | 0.171 | 0.077 | 0.336 | 85 |
| mRNA-based | 5 | 0.731 | 0.532 | 0.866 | 86.0 | NA | NA | NA | NA | NA | |||
| 3 | Adenovirus-based | 3 | 0.982 | 0.980 | 0.984 | 0.0 | 1 | 0.149 | 0.139 | 0.159 | 0 | ||
| VLP | 9 | 0.787 | 0.581 | 0.908 | 78.1 | NA | NA | NA | NA | NA | |||
| 4 | Inactivated | 4 | 0.944 | 0.842 | 0.982 | 15.9 | 4 | 0.063 | 0.026 | 0.143 | 0 | ||
| Pro-Subunit | 6 | 0.956 | 0.937 | 0.970 | 0.0 | NA | NA | NA | NA | NA | |||
| S-protein | 2 | Inactivated | 7 | 0.941 | 0.877 | 0.973 | 61.4 | 7 | 0.290 | 0.139 | 0.507 | 87 | |
| Pro-Subunit | 18 | 0.852 | 0.719 | 0.928 | 62.4 | 18 | 0.028 | 0.014 | 0.052 | 0 | |||
| mRNA-based | 5 | 0.786 | 0.725 | 0.836 | 0.0 | NA | NA | NA | NA | NA | |||
| 4 | Inactivated | 4 | 0.934 | 0.842 | 0.974 | 15.9 | 4 | 0.063 | 0.026 | 0.143 | 0 | ||
| Pro-Subunit | 14 | 0.792 | 0.679 | 0.873 | 50.7 | 15 | 0.031 | 0.015 | 0.061 | 0 | |||
| NAbs | 2 | Adenovirus-based | 1 | 0.999 | 0.985 | 1.000 | 0.0 | NA | NA | NA | NA | NA | |
| Inactivated | 9 | 0.845 | 0.724 | 0.919 | 86.5 | 9 | 0.151 | 0.068 | 0.303 | 85 | |||
| Pro-Subunit | 23 | 0.753 | 0.667 | 0.823 | 68.2 | 19 | 0.028 | 0.015 | 0.052 | 0 | |||
| mRNA-based | 9 | 0.870 | 0.747 | 0.938 | 82.4 | 4 | 0.008 | 0.003 | 0.024 | 0 | |||
| 3 | Adenovirus-based | 1 | 0.958 | 0.955 | 0.961 | 0.0 | 1 | 0.071 | 0.065 | 0.079 | 0 | ||
| 4 | Adenovirus-based | 1 | 0.999 | 0.985 | 1.000 | 0.0 | NA | NA | NA | NA | NA | ||
| Inactivated | 4 | 0.700 | 0.375 | 0.901 | 86.1 | 4 | 0.033 | 0.011 | 0.099 | 0 | |||
| Pro-Subunit | 17 | 0.759 | 0.574 | 0.881 | 62.9 | 15 | 0.031 | 0.015 | 0.061 | 0 | |||
| mRNA-based | 4 | 0.995 | 0.980 | 0.999 | 0.0 | 4 | 0.016 | 0.007 | 0.035 | 0 | |||
| Side Effect | Vaccine Type | Phase | Odds Ratio (95% CI) | Included Study | Heterogeneity Test, I-Squared |
|---|---|---|---|---|---|
| Site pain | mRNA-based | 2/3 | 83.06 (37.05–186.1) | 5 | 81.33 |
| 1/2 | 28.26 (16.18–49.35) | 17 | 0 | ||
| Adenovirus-based | 2/3 | 13.64 (8.39–22.17) | 2 | 0 | |
| 1/2 | 3.2 (2.7–4) | 2 | 0 | ||
| Inactivated | 2/3 | 1.73 (0.667–4.5) | 6 | 46.64 | |
| 1/2 | 3.19 (1.3–7.6) | 10 | 52.14 | ||
| Pro-Subunit | 2/3 | 2.14 (1.01–4.5) | 4 | 48.55 | |
| 1/2 | 2.29 (0.48–10.8) | 2 | 29.93 | ||
| Swelling | Adenovirus-based | 1/2/3 | 1.21 (0.77–1.89) | 2 | 0 |
| Inactivated | 1/2/3 | 0.402 (0.056–2.90) | 2 | 0 | |
| Pro-Subunit | 1/2/3 | 6.48 (3.09–13.67) | 5 | 0 | |
| mRNA-based | 1/2/3 | 18.79 (4.87–72.40) | 3 | 59.08 | |
| Redness | Adenovirus-based | 1/2/3 | 1.35 (0.815–2.25) | 4 | 0 |
| Pro-Subunit | 1/2/3 | 7.29 (3.70–14.38) | 6 | 0 | |
| mRNA-based | 1/2/3 | 24.40 (18.73–31.77) | 1 | 0 | |
| Itch | Adenovirus-based | 1/2 | 3.10 (1.96–4.89) | 1 | 0 |
| Inactivated | 1/2 | 0.32 (0.02–5.3) | 1 | 0 | |
| Pro-Subunit | 1/2 | 25.44 (7.85–82.40) | 6 | 0 | |
| Cough | Adenovirus-based | 1/2/3 | 1.76 (1.20–2.58) | 3 | 0 |
| Fever | Adenovirus-based | 1/2/3 | 1.73 (0.57–5.66) | 3 | 90.5 |
| Inactivated | 1/2/3 | 0.27 (0.09–0.76) | 5 | 0 | |
| Pro-Subunit | 1/2/3 | 1.17 (0.73–1.86) | 4 | 0 | |
| mRNA-based | 1/2/3 | 36.90 (12.34–105.21) | 3 | 43.31 | |
| Headache | mRNA-based | 3 | 4.63 (4.4–4.86) | 1 | 0 |
| 2 | 2.32 (1.28–4.19) | 4 | 69.20 | ||
| 1/2 | 5.13 (2.32–11.31) | 5 | 63.02 | ||
| Adenovirus-based | 2 | 2.54 (1.65–3.91) | 2 | 0 | |
| 1/2 | 3.01 (2.35–3.87) | 1 | 0 | ||
| 3 | 0.58 (0.49–0.68) | 1 | 0 | ||
| Inactivated | 2 | 0.18 (0.02–1.14) | 2 | 0 | |
| Pro-Subunit | 2 | 1.25 (0.33–4.7) | 2 | 0 | |
| 1/2 | 1.99 (1.21–3.26) | 14 | 0 | ||
| Fatigue | Adenovirus-based | 1/2 | 2.72 (2.2–3.37) | 3 | 0 |
| Inactivated | 1/2 | 0.39 (0.18–0.82) | 7 | 0 | |
| Pro-Subunit | 1/2 | 2.7 (1.01–7.16) | 4 | 37.2 | |
| mRNA-based | 1/2 | 5.0 (3.42–7.33) | 24 | 48.23 | |
| 2–3 | 4.87 (4.65–5.09) | 1 | 0 | ||
| 3 | 6.16 (5.86–6.48) | 1 | 0 | ||
| Induration | Adenovirus-based | 1/2 | 0.16 (0.05–0.49) | 2 | 46.44 |
| Inactivated | 1/2 | 0.18 (0.06–0.58) | 4 | 0 | |
| Pro-Subunit | 1/2 | 2.62 (1.23–5.58) | 2 | 0 | |
| mRNA-based | 1/2 | 17.5 (1.96–155.58) | 1 | 0 | |
| Vomiting | Adenovirus-based | 1/2 | 2.75 (1.99–3.82) | 3 | 0 |
| Inactivated | 1/2 | 0.32 (0.02–5.38) | 1 | 0 | |
| mRNA-based | 1/2 | 8.71 (4.38–17.34) | 8 | 0 | |
| 2–3 | 4.87 (4.65–5.09) | 1 | 0 | ||
| 3 | 6.16 (5.86–6.48) | 1 | 0 | ||
| Diarrhea | Adenovirus-based | 1/2 | 2.51 (1.12–5.63) | 2 | 0 |
| Inactivated | 1/2 | 0.60 (0.13–2.83) | 3 | 0 | |
| mRNA-based | 1/2 | 0.54 (0.27–1.10) | 5 | 0 | |
| Myalgia | Adenovirus-based | 1/2 | 4.59 (3.58–5.89) | 3 | 0 |
| Inactivated | 1/2 | 1.43 (0.25–8.08) | 2 | 0 | |
| Pro-Subunit | 2.92 (0.57–8.75) | 8 | 53.30 | ||
| mRNA-based | 1/2 | 10.71 (6.51–17.60) | 10 | 33.74 | |
| 2/3 | 7.0 (6.57–7.47) | 1 | 0 | ||
| 3 | 1.43 (0.25–8.08) | 1 | 0 | ||
| Arthralgia | Adenovirus-based | 2/3 | 4.06 (2.99–5.57) | 3 | 0 |
| Pro-Subunit | 2/3 | 1.34 (0.47–3.83) | 4 | 4.833 | |
| mRNA-based | 2/3 | 9.67 (1.27–76.90) | 3 | 67.97 | |
| Chills | Adenovirus-based | 2/3 | 10.61 (7.60–14.83) | 1 | 0 |
| mRNA-based | 2/3 | 13.11 (7.19–23.89) | 8 | 3.82 | |
| Pruritus | Adenovirus-based | 2/3 | 0.54 (0.23–1.25) | 2 | 0 |
| mRNA-based | 2/3 | 17.50 (1.98–155.58) | 1 | 0 |
| Side Effect | Adjuvant Type | Phase | Odds Ratio (95% CI) | Included Study | Heterogeneity Test, I-Squared | |
|---|---|---|---|---|---|---|
| Systemic | Fatigue | Alum | 2/3 | 0.392 (0.18–0.82) | 7 | 0 |
| Matrix-M1 | 2/3 | 3.70 (1.36–10.02) | 3 | 24.81 | ||
| No adjuvant | 2/3 | 4.43 (2.62–7.49) | 6 | 54.08 | ||
| Vomiting | Alum | 2/3 | 0.325 (0.02–5.30) | 1 | 0 | |
| No adjuvant | 2/3 | 3.46 (1.45–8.26) | 7 | 0 | ||
| Fever | Alum | 2/3 | 0.85 (0.51–1.43) | 9 | 20.78 | |
| No adjuvant | 2/3 | 2.96 (1.22–7.17) | 2 | 68.19 | ||
| Myalgia | Alum | 2/3 | 1.43 (0.25–8.0) | 2 | 0 | |
| AS03 | 2/3 | 14.331 (3.39–60.56) | 3 | 0 | ||
| CpG/Alum | 2/3 | 2.42 (0.13–44.50) | 1 | 0 | ||
| Matrix-M1 | 2/3 | 1.57 (0.26–9.4) | 3 | 67.96 | ||
| No adjuvant | 2/3 | 9.66 (3.97–23.47) | 8 | 49.99 | ||
| Diarrhea | Alum | 2/3 | 0.608 (0.13–2.87) | 3 | 0 | |
| No adjuvant | 2/3 | 0.89 (0.40–1.97) | 6 | 50.47 | ||
| Local | Injection site pain | Alum | 2/3 | 2.40 (1.51–3.83) | 22 | 44.55 |
| No adjuvant | 2/3 | 25.61 (13.31–49.30) | 7 | 36.60 | ||
| Itch | Alum | 2/3 | 13.20 (3.23–53.90) | 7 | 40.58 | |
| Swelling | Alum | 2/3 | 3.83 (1.52–9.64) | 7 | 37.52 | |
| Redness | Alum | 2/3 | 7.29 (3.7–14.39) | 6 | 0 | |
| No adjuvant | 2/3 | 0.923 (0.23–3.6) | 2 | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. https://doi.org/10.3390/vaccines9050467
Pormohammad A, Zarei M, Ghorbani S, Mohammadi M, Razizadeh MH, Turner DL, Turner RJ. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines. 2021; 9(5):467. https://doi.org/10.3390/vaccines9050467
Chicago/Turabian StylePormohammad, Ali, Mohammad Zarei, Saied Ghorbani, Mehdi Mohammadi, Mohammad Hossein Razizadeh, Diana L. Turner, and Raymond J. Turner. 2021. "Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" Vaccines 9, no. 5: 467. https://doi.org/10.3390/vaccines9050467