
Post-Marketing Active Surveillance of Adverse Reactions Following Influenza Cell-Based Quadrivalent Vaccine: An Italian Prospective Observational Study


 and
and
Abstract
:1. Introduction
2. Material and Methods
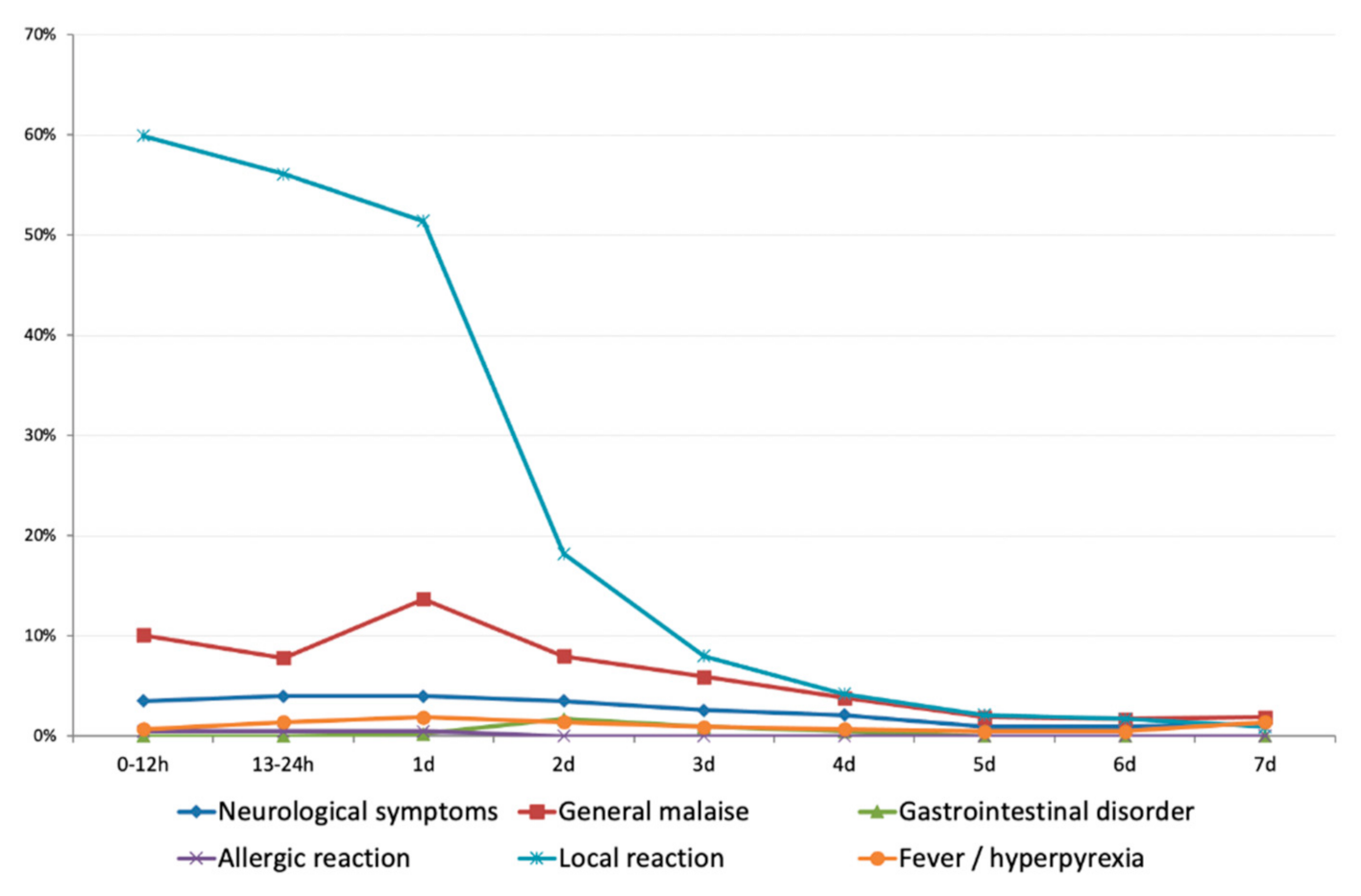
- Local reactions (pain, redness, swelling, induration at the injection site)
- Allergic reaction (anaphylaxis, allergic/urticarial reaction)
- Gastrointestinal symptoms (nausea, vomiting, diarrhea)
- General malaise (asthenia, myalgia, malaise, drowsiness/insomnia
- Neurological symptoms (irritability, nervousness, headache)
- Fever/hyperpyrexia.
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC (Center for Disease Control and Prevention). Recommended Vaccines for Healthcare Workers. Available online: https://www.cdc.gov/vaccines/adults/rec-vac/hcw.html (accessed on 13 March 2021).
- Black, C.L.; Yue, X.; Ball, S.W.; Fink, R.V.; de Perio, M.A.; Laney, A.S.; Williams, W.W.; Graitcer, S.B.; Fiebelkorn, A.P.; Lu, P.J.; et al. Influenza Vaccination Coverage Among Health Care Personnel-United States, 2017–2018 Influenza Season. MMWR Morb. Mortal Wkly. Rep. 2018, 67, 1050–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Government Legislative Decree No. 81/2008. Unique Text on Health and Safety at Work. Available online: https://www.ispettorato.gov.it/it-it/Documenti-Norme/Documents/Testo-Unico-Dlgs-81-08-edizione-di-luglio-2018.pdf (accessed on 15 March 2021).
- Italian Ministry of Health. Prevention and Control of Influenza: Recommendations for the 2019–2020 Season. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=74451&parte=1%20&serie=null (accessed on 7 March 2021).
- Prato, R.; Tafuri, S.; Fortunato, F.; Martinelli, D. Vaccination in healthcare workers: An Italian perspective. Expert Rev. Vaccines 2010, 9, 277–283. [Google Scholar] [CrossRef] [PubMed]
- CDC. Cell-Based Flu Vaccines. Available online: https://www.cdc.gov/flu/prevent/cell-based.htm (accessed on 2 March 2021).
- European Medicines Agency. Flucelvax Tetra. Influenza Vaccine (Surface Antigen, Inactivated, Prepared in Cell Cultures). Available online: https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-flucelvax-tetra_en.pdf (accessed on 12 March 2021).
- European Commission. Summary of the Decisions of the European Union Relating to Authorizations for the Marketing of Medicinal Products from 1 December 2018 to 31 December 2018. Available online: https://eur-lex.europa.eu/legal-content/IT/TXT/PDF/?uri=CELEX:52019XC0125(05)&qid=1560959699946&from=IT (accessed on 12 March 2021).
- U.S. National Library. Clinical Trial.gov. Safety and Immunogenicity of Three Influenza Vaccines Adults Ages 18 and Older. December 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT01992094 (accessed on 12 March 2021).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, M.R.; Braun, M.M.; Bart, K.J. What should an ideal vaccine postlicensure safety system be? Am. J. Public Health 2009, 99, S345–S350. [Google Scholar] [CrossRef] [PubMed]
- Stefanizzi, P.; De Nitto, S.; Patano, F.; Bianchi, F.P.; Ferorelli, D.; Stella, P.; Ancona, D.; Bavaro, V.; Tafuri, S. Post-marketing surveillance of adverse events following measles, mumps, rubella and varicella (MMRV) vaccine: Retrospecive study in apulia region (ITALY), 2009–2017. Hum. Vaccines Immunother. 2020, 16, 1875–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Addendum ‘Guidance on Enhanced Safety Surveillance for Seasonal Influenza Vaccines in the EU’. April 2014. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/interim-guidance-enhanced-safety-surveillance-seasonal-influenza-vaccines-eu_en.pdf (accessed on 15 March 2021).
- Vimercati, L.; Bianchi, F.P.; Mansi, F.; Ranieri, B.; Stefanizzi, P.; De Nitto, S.; Tafuri, S. Influenza vaccination in health-care workers: An evaluation of an on-site vaccination strategy to increase vaccination uptake in HCWs of a South Italy Hospital. Hum. Vaccines Immunother. 2019, 15, 2927–2932. [Google Scholar] [CrossRef] [PubMed]
- WHO. Causality Assessment of an Adverse Event Following Immunization (AEFI). User Manual for the Revised WHO Classification. January 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/259959/9789241513654-eng.pdf?sequence=1&isAllowed=y (accessed on 2 March 2021).
- AIFA. Guida alla Valutazione delle Reazioni Avverse Osservabili dopo Vaccinazione. Available online: http://www.aifa.gov.it/sites/default/files/Guida_valutazione_reazioni_avverse_osservabili_dopo_vaccinazione_2.pdf (accessed on 3 March 2021).
- Stefanizzi, P.; Stella, P.; Ancona, D.; Malcangi, K.N.; Bianchi, F.P.; De Nitto, S.; Ferorelli, D.; Germinario, C.A.; Tafuri, S. Adverse Events Following Measles-Mumps-Rubella-Varicella Vaccination and the Case of Seizures: A Post Marketing Active Surveillance in Puglia Italian Region, 2017–2018. Vaccines 2019, 7, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spila Alegiani, S.; Alfonsi, V.; Appelgren, E.C.; Ferrara, L.; Gallo, T.; Alicino, C.; Pascucci, M.G.; Aquilani, S.; Spadea, A.; Tafuri, S.; et al. Active surveillance for safety monitoring of seasonal influenza vaccines in Italy, 2015/2016 season. BMC Public Health 2018, 18, 1401. [Google Scholar] [CrossRef] [PubMed]
- Pillsbury, A.; Cashman, P.; Leeb, A.; Regan, A.; Westphal, D.; Snelling, T.; Blyth, C.; Crawford, N.; Wood, N.; Macartney, K.; et al. Real-time safety surveillance of seasonal influenza vaccines in children, Australia, 2015. Eurosurveillance 2015, 20, 30050. [Google Scholar] [CrossRef] [PubMed]
- Newes-Adeyi, G.; Greece, J.; Bozeman, S.; Walker, D.K.; Lewis, F.; Gidudu, J. Active surveillance for influenza vaccine adverse events: The integrated vaccine surveillance system. Vaccine 2012, 30, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Danova, J.; Kocourkova, A.; Celko, A.M. Active surveillance study of adverse events following immunisation of children in the Czech Republic. BMC Public Health 2017, 17, 167. [Google Scholar]
- Márquez, E.J.; Chung, C.H.; Marches, R.; Rossi, R.J.; Nehar-Belaid, D.; Eroglu, A.; Mellert, D.J.; Kuchel, G.A.; Banchereau, J.; Ucar, D. Sexual-dimorphism in human immune system aging. Nat. Commun. 2020, 11, 751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurici, M.; Arigliani, M.; Dugo, V.; Leo, C.; Pettinicchio, V.; Arigliani, R.; Franco, E. Empathy in vaccination counselling: A survey on the impact of a three-day residential course. Hum. Vaccines Immunother. 2019, 15, 631–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regan, A.; Blyth, C.; Tracey, L.; Mak, D.; Richmond, P.; Effler, P. Comparison of text-messaging to voice telephone interviews for active surveillance of adverse events following immunisation. Vaccine 2015, 33, 3689–3694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorelli, C.; Odone, A.; Conversano, M.; Bonanni, P. Deaths after Fluad flu vaccine and the epidemic of panic in Italy. BMJ 2015, 350, h116. [Google Scholar]
- Bianchi, F.P.; Vimercati, L.; Mansi, F.; De Nitto, S.; Stefanizzi, P.; Rizzo, L.A.; Fragnelli, G.R.; Cannone, E.S.S.; De Maria, L.; Larocca, A.M.V.; et al. Compliance with immunization and a biological risk assessment of health care workers as part of an occupational health surveillance program: The experience of a university hospital in southern Italy. Am. J. Infect. Control 2020, 48, 368–374. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AEFI | n | % | Reporting Rate (95%CI) × 100 Enrolled |
|---|---|---|---|
| Local reaction | 378 | 87.8 | 51.0 (47.3–54.7) |
| General malaise | 114 | 26.5 | 15.4 (12.9–18.2) |
| Neurological symptoms | 36 | 8.4 | 4.9 (3.4–6.7) |
| Fever/hyperpyrexia | 21 | 4.8 | 2.8 (1.8–4.3) |
| Gastrointestinal disorder | 9 | 2.1 | 1.2 (0.6–2.3) |
| Allergic reaction | 2 | 0.4 | 0.27 (0.03–0.97) |
| At least one AEFI | 430 | 100.0 | 58.0 (54.4–61.6) |
| AEFI (Only Local Reaction) | n | % | Reporting Rate (95%CI) × 100 Enrolled |
|---|---|---|---|
| Pain at injection site | 357 | 94.4 | 48.2 (44.5–51.8) |
| Induration of injection site | 81 | 21.4 | 10.9 (8.8–13.4) |
| Swelling | 28 | 7.4 | 5.1 (2.5–5.4) |
| Redness | 21 | 5.5 | 2.8 (1.8–4.3) |
| Females (n = 412) | Males (n = 369) | p-Value | |||
|---|---|---|---|---|---|
| AEFI | n | Reporting Rate (95%CI) × 100 Enrolled | n | Reporting Rate (95%CI) × 100 Enrolled | |
| Local reaction | 240 | 58.3 (53.3–63.1) | 138 | 41.9 (36.6–47.5) | <0.0001 |
| General malaise | 79 | 19.2 (15.5–23.3) | 35 | 10.6 (7.5–14.5) | 0.001 |
| Neurological symptoms | 23 | 5.6 (3.6–8.3) | 13 | 4.0 (2.1–6.7) | 0.305 |
| Fever/hyperpyrexia | 16 | 3.9 (2.2–6.2) | 5 | 1.5 (0.5–3.5) | 0.054 |
| Gastrointestinal disorder | 6 | 1.5 (0.5–3.1) | 3 | 0.5 (0.2–2.6) | 0.501 |
| Allergic reaction | 1 | 0.2 (0.0–1.3) | 1 | 0.3 (0.0–1.7) | 0.873 |
| At least one AEFI | 270 | 65.5 (60.7–70.1) | 160 | 48.6 (43.1–54.2) | <0.0001 |
| <40 Years Old (n = 380) | ≥40 Years Old (n = 361) | p-Value | |||
|---|---|---|---|---|---|
| AEFI | n | Reporting Rate (95%CI) × 100 Enrolled | n | Reporting Rate (95%CI) × 100 Enrolled | |
| Local reaction | 229 | 60.2 (55.1–65.2) | 149 | 41.3 (36.1–46.5) | <0.0001 |
| General malaise | 64 | 16.8 (13.2–21.0) | 50 | 13.9 (10.5–17.8) | 0.259 |
| Neurological symptoms | 20 | 5.3 (3.2–8.0) | 16 | 4.4 (2.6–7.1) | 0.599 |
| Fever/hyperpyrexia | 15 | 3.9 (2.2–6.4) | 6 | 1.7 (0.6–3.6) | 0.061 |
| Gastrointestinal disorder | 1 | 0.3 (0.0–1.5) | 8 | 2.2 (1.0–4.3) | 0.015 |
| Allergic reaction | 2 | 0.5 (0.1–1.9) | 0 | 0.0 (0.0–1.0) | 0.168 |
| At least one AEFI | 251 | 66.1 (61.0–70.8) | 179 | 49.6 (44.3–54.9) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanizzi, P.; De Nitto, S.; Spinelli, G.; Lattanzio, S.; Stella, P.; Ancona, D.; Dell'Aera, M.; Padovano, M.; Soldano, S.; Tafuri, S.; et al. Post-Marketing Active Surveillance of Adverse Reactions Following Influenza Cell-Based Quadrivalent Vaccine: An Italian Prospective Observational Study. Vaccines 2021, 9, 456. https://doi.org/10.3390/vaccines9050456
Stefanizzi P, De Nitto S, Spinelli G, Lattanzio S, Stella P, Ancona D, Dell'Aera M, Padovano M, Soldano S, Tafuri S, et al. Post-Marketing Active Surveillance of Adverse Reactions Following Influenza Cell-Based Quadrivalent Vaccine: An Italian Prospective Observational Study. Vaccines. 2021; 9(5):456. https://doi.org/10.3390/vaccines9050456
Chicago/Turabian StyleStefanizzi, Pasquale, Sara De Nitto, Giuseppe Spinelli, Sabrina Lattanzio, Paolo Stella, Domenica Ancona, Maria Dell'Aera, Margherita Padovano, Savino Soldano, Silvio Tafuri, and et al. 2021. "Post-Marketing Active Surveillance of Adverse Reactions Following Influenza Cell-Based Quadrivalent Vaccine: An Italian Prospective Observational Study" Vaccines 9, no. 5: 456. https://doi.org/10.3390/vaccines9050456