
A Placebo-Controlled, Double-Blind Randomized (Phase IIB) Trial of Oral Administration with HPV16 E7-Expressing Lactobacillus, GLBL101c, for the Treatment of Cervical Intraepithelial Neoplasia Grade 2 (CIN2)

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Study Design
2.3. Composition of the Vaccine
2.4. Collection and Processing of Cervical Specimens
2.5. Safety and Tolerability
2.6. Immunological Responses to HPV16 E7
2.7. Statistical Analysis
3. Results
3.1. Study Population and Adverse Events
3.2. Clinical Responses to Administration
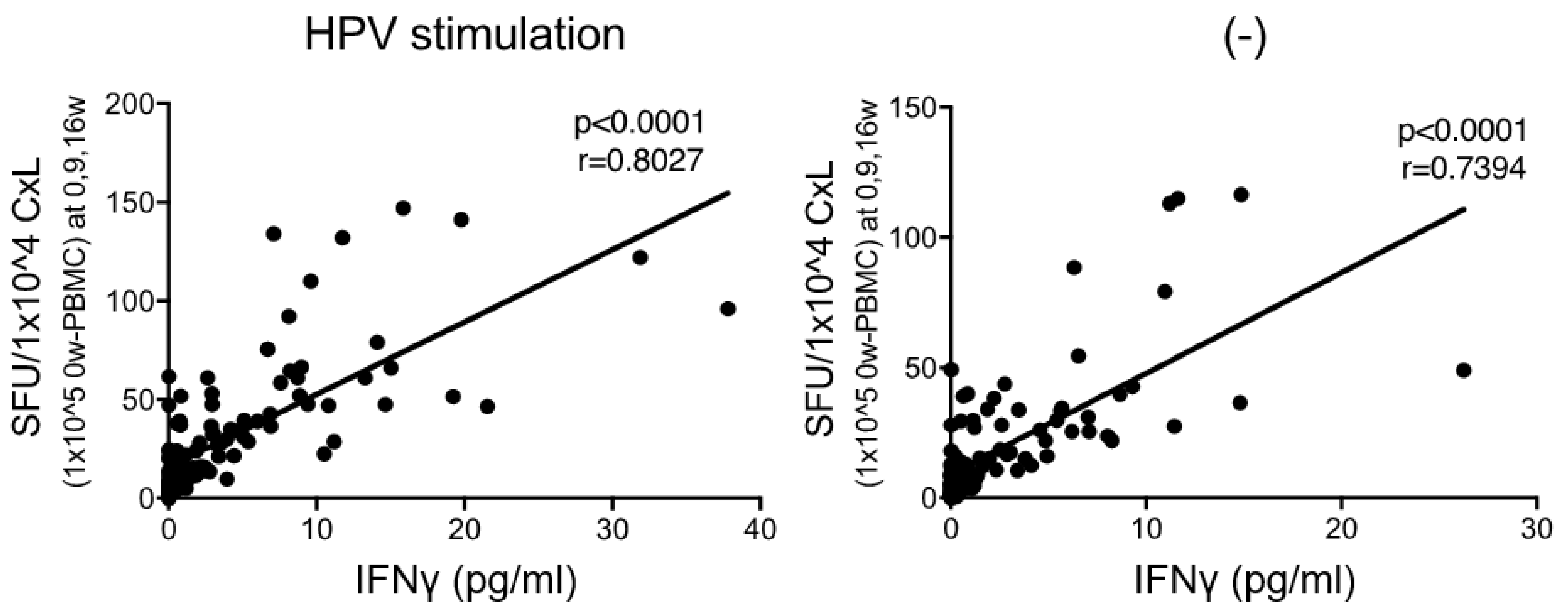
3.3. Correlation between E7-Specific IFNγ-Producing Cells and IFNγ Secretion
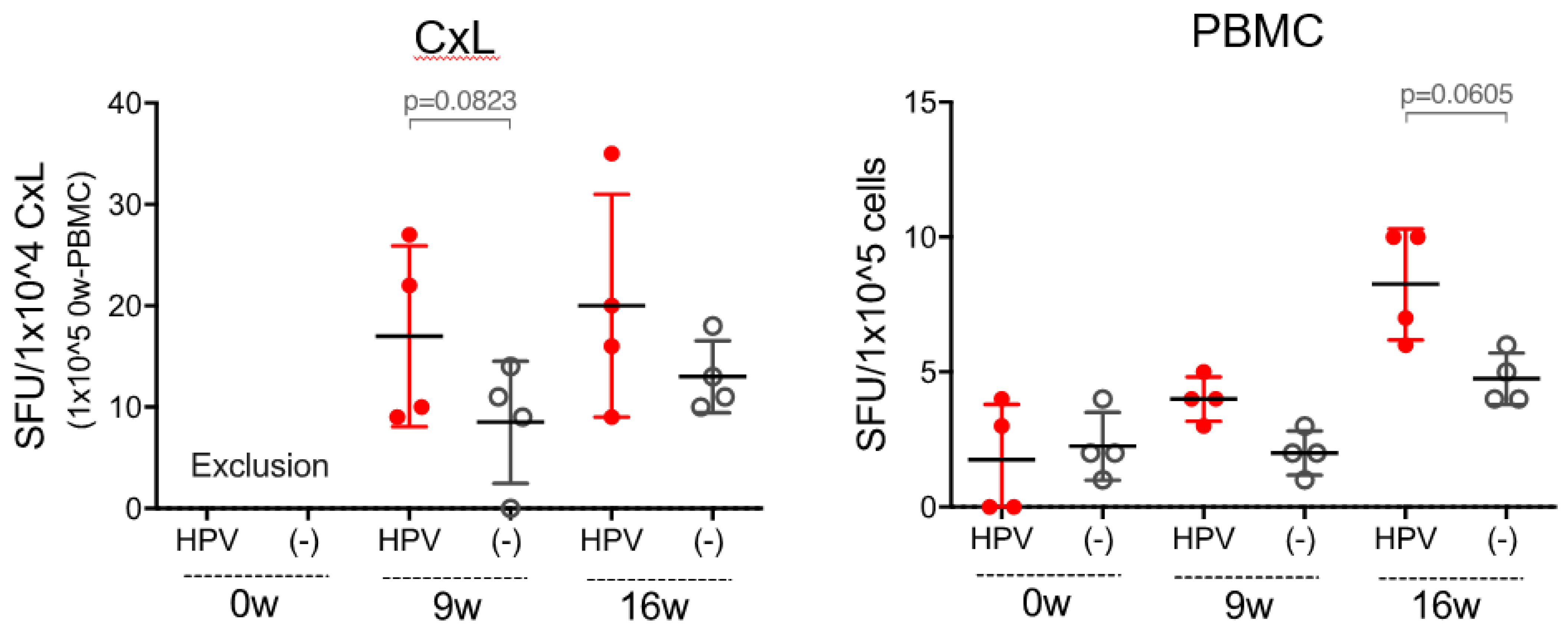
3.4. E7-Specific Th1 Immune Responses to Administration
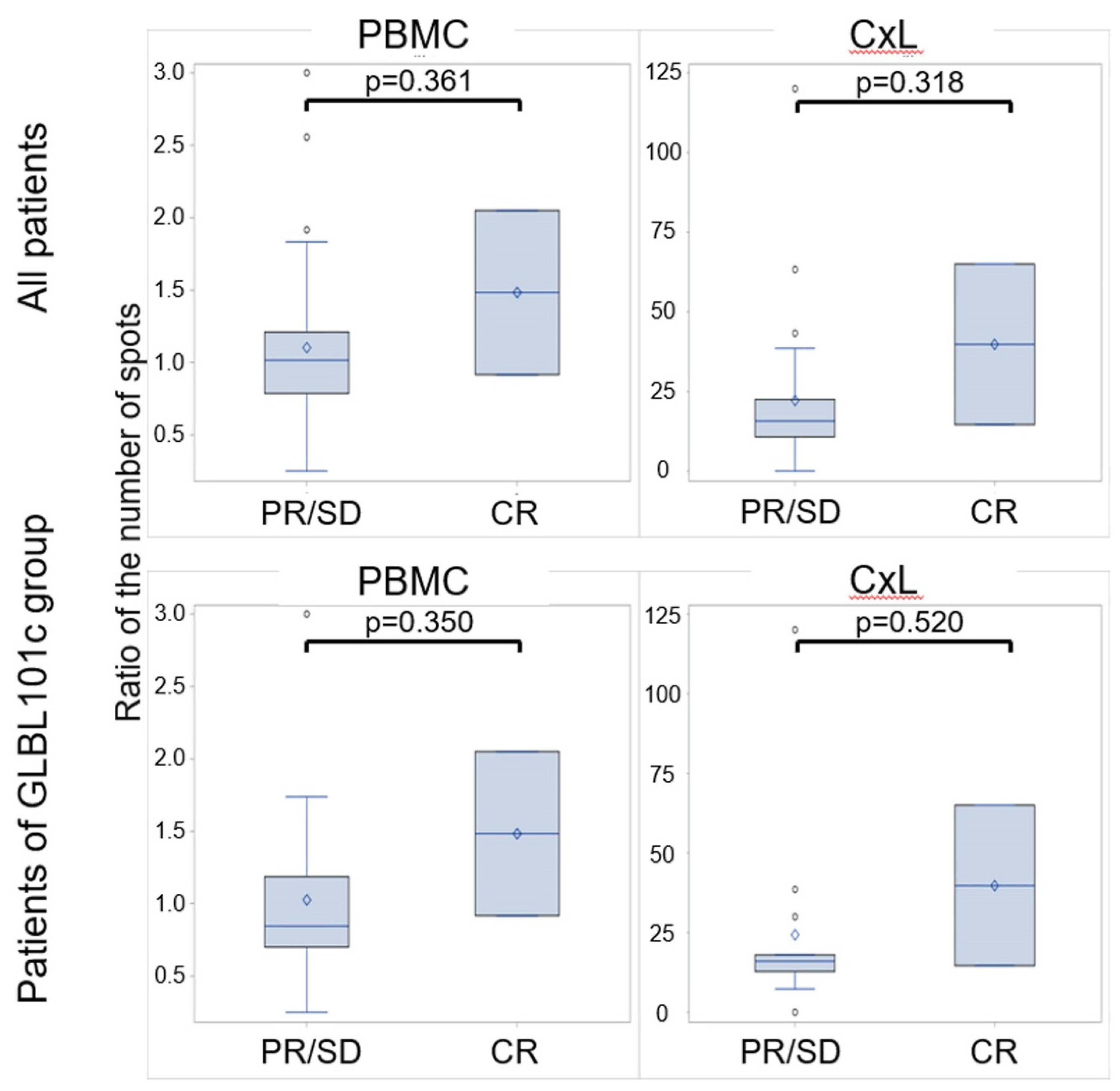
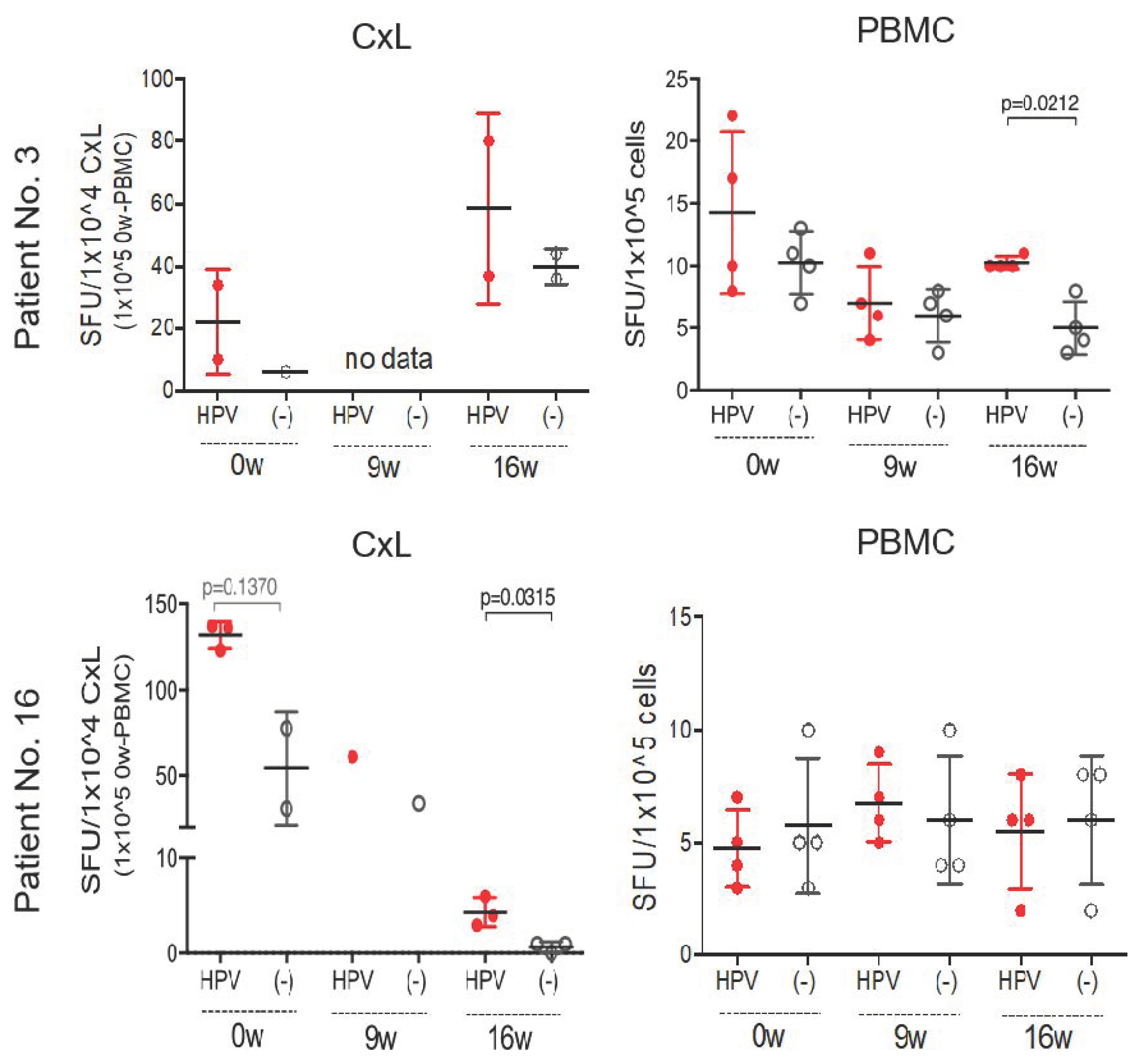
3.5. Characteristics of Patients with Rapid Regression to Normal
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Clinical Trial Registration
Conflicts of Interest
References
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Bosch, F.X.; de Sanjose, S. Chapter 1: Human papillomavirus and cervical cancer—Burden and assessment of causality. J. Natl. Cancer Inst. Monogr. 2003, 2003, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, E.F.; Unger, E.R.; Sternberg, M.; McQuillan, G.; Swan, D.C.; Patel, S.S.; Markowitz, L.E. Prevalence of hpv infection among females in the united states. JAMA 2007, 297, 813–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferenczy, A.; Franco, E. Persistent human papillomavirus infection and cervical neoplasia. Lancet Oncol. 2002, 3, 11–16. [Google Scholar] [CrossRef]
- Bogani, G.; Raspagliesi, F.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Simoncini, T.; Petrillo, M.; Plotti, F.; Lopez, S.; Casarin, J.; et al. Assessing the long-term role of vaccination against hpv after loop electrosurgical excision procedure (leep): A propensity-score matched comparison. Vaccines 2020, 8, 717. [Google Scholar] [CrossRef]
- Bogani, G.; Di Donato, V.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. Recurrence rate after loop electrosurgical excision procedure (leep) and laser conization: A 5-year follow-up study. Gynecol. Oncol. 2020, 159, 636–641. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Athanasiou, A.; Kalliala, I.E.J.; Paraskevaidi, M.; Mitra, A.; Martin-Hirsch, P.P.; Arbyn, M.; Bennett, P.; Paraskevaidis, E. Obstetric outcomes after conservative treatment for cervical intraepithelial lesions and early invasive disease. Cochrane Database Syst. Rev. 2017, 11, CD012847. [Google Scholar] [CrossRef]
- Matsumoto, K.; Oki, A.; Furuta, R.; Maeda, H.; Yasugi, T.; Takatsuka, N.; Mitsuhashi, A.; Fujii, T.; Hirai, Y.; Iwasaka, T.; et al. Predicting the progression of cervical precursor lesions by human papillomavirus genotyping: A prospective cohort study. Int. J. Cancer 2011, 128, 2898–2910. [Google Scholar] [CrossRef]
- Holowaty, P.; Miller, A.B.; Rohan, T.; To, T. Natural history of dysplasia of the uterine cervix. J. Natl. Cancer Inst. 1999, 91, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Kawana, K.; Yasugi, T.; Taketani, Y. Human papillomavirus vaccines: Current issues & future. Indian J. Med. Res. 2009, 130, 341–347. [Google Scholar]
- Trimble, C.L.; Morrow, M.P.; Kraynyak, K.A.; Shen, X.; Dallas, M.; Yan, J.; Edwards, L.; Parker, R.L.; Denny, L.; Giffear, M.; et al. Safety, efficacy, and immunogenicity of vgx-3100, a therapeutic synthetic DNA vaccine targeting human papillomavirus 16 and 18 e6 and e7 proteins for cervical intraepithelial neoplasia 2/3: A randomised, double-blind, placebo-controlled phase 2b trial. Lancet 2015, 386, 2078–2088. [Google Scholar] [CrossRef] [Green Version]
- Kojima, S.; Kawana, K.; Fujii, T.; Yokoyama, T.; Miura, S.; Tomio, K.; Tomio, A.; Yamashita, A.; Adachi, K.; Sato, H.; et al. Characterization of gut-derived intraepithelial lymphocyte (iel) residing in human papillomavirus (hpv)-infected intraepithelial neoplastic lesions. Am. J. Reprod. Immunol. 2011, 66, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Adachi, K.; Kawana, K.; Yokoyama, T.; Fujii, T.; Tomio, A.; Miura, S.; Tomio, K.; Kojima, S.; Oda, K.; Sewaki, T.; et al. Oral immunization with a lactobacillus casei vaccine expressing human papillomavirus (hpv) type 16 e7 is an effective strategy to induce mucosal cytotoxic lymphocytes against hpv16 e7. Vaccine 2010, 28, 2810–2817. [Google Scholar] [CrossRef] [PubMed]
- Poo, H.; Pyo, H.M.; Lee, T.Y.; Yoon, S.W.; Lee, J.S.; Kim, C.J.; Sung, M.H.; Lee, S.H. Oral administration of human papillomavirus type 16 e7 displayed on lactobacillus casei induces e7-specific antitumor effects in c57/bl6 mice. Int. J. Cancer 2006, 119, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Kawana, K.; Adachi, K.; Kojima, S.; Taguchi, A.; Tomio, K.; Yamashita, A.; Nishida, H.; Nagasaka, K.; Arimoto, T.; Yokoyama, T.; et al. Oral vaccination against hpv e7 for treatment of cervical intraepithelial neoplasia grade 3 (cin3) elicits e7-specific mucosal immunity in the cervix of cin3 patients. Vaccine 2014, 32, 6233–6239. [Google Scholar] [CrossRef]
- Buckley, C.H.; Butler, E.B.; Fox, H. Cervical intraepithelial neoplasia. J. Clin. Pathol. 1982, 35, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Einstein, M.H.; Kadish, A.S.; Burk, R.D.; Kim, M.Y.; Wadler, S.; Streicher, H.; Goldberg, G.L.; Runowicz, C.D. Heat shock fusion protein-based immunotherapy for treatment of cervical intraepithelial neoplasia iii. Gynecol. Oncol. 2007, 106, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Han, C.; Kawana-Tachikawa, A.; Shimizu, A.; Zhu, D.; Nakamura, H.; Adachi, E.; Kikuchi, T.; Koga, M.; Koibuchi, T.; Gao, G.F.; et al. Switching and emergence of ctl epitopes in hiv-1 infection. Retrovirology 2014, 11, 38. [Google Scholar] [CrossRef] [Green Version]
- Ressler, S.; Scheiden, R.; Dreier, K.; Laich, A.; Muller-Holzner, E.; Pircher, H.; Morandell, D.; Stein, I.; Viertler, H.P.; Santer, F.R.; et al. High-risk human papillomavirus e7 oncoprotein detection in cervical squamous cell carcinoma. Clin. Cancer Res. 2007, 13, 7067–7072. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.; Xiao, X.; Lou, H.; Liu, P.; Song, S.; Liu, M.; Xu, T.; Zhang, Y.; Li, C.; Guan, R.; et al. Analysis of the role of the human papillomavirus 16/18 e7 protein assay in screening for cervical intraepithelial neoplasia: A case control study. BMC Cancer 2020, 20, 999. [Google Scholar]
- Liu, S.; Minaguchi, T.; Lachkar, B.; Zhang, S.; Xu, C.; Tenjimbayashi, Y.; Shikama, A.; Tasaka, N.; Akiyama, A.; Sakurai, M.; et al. Separate analysis of human papillomavirus e6 and e7 messenger rnas to predict cervical neoplasia progression. PLoS ONE 2018, 13, e0193061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang-Johanning, F.; Lu, D.W.; Wang, Y.; Johnson, M.R.; Johanning, G.L. Quantitation of human papillomavirus 16 e6 and e7 DNA and rna in residual material from thinprep papanicolaou tests using real-time polymerase chain reaction analysis. Cancer 2002, 94, 2199–2210. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, A.; Igimi, S.; Kawana, K. Optimization of human papillomavirus (hpv) type 16 e7-expressing lactobacillus-based vaccine for induction of mucosal e7-specific ifngamma-producing cells. Vaccine 2018, 36, 3423–3426. [Google Scholar] [CrossRef]
- Ikeda, Y.; Uemura, Y.; Asai-Sato, M.; Nakao, T.; Nakajima, T.; Iwata, T.; Akiyama, A.; Satoh, T.; Yahata, H.; Kato, K.; et al. Safety and efficacy of mucosal immunotherapy using human papillomavirus (hpv) type 16 e7-expressing lactobacillus-based vaccine for the treatment of high-grade squamous intraepithelial lesion (hsil): The study protocol of a randomized placebo-controlled clinical trial (milacle study). Jpn. J. Clin. Oncol 2019, 49, 877–880. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | GLBL-101c | Placebo |
|---|---|---|
| Number of patients | 20 | 20 |
| Age | ||
| <30 | 5 | 3 |
| ≥30 | 15 | 17 |
| Height | 158.6 | 161.2 |
| Weight (Median) | 50.2 | 51.6 |
| Initial blood pressure (Median) | ||
| Max | 115.4 | 112.4 |
| Min | 72.4 | 72.6 |
| History of chlamydia infection | 3 | 5 |
| Current chlamydia infection | 0 | 0 |
| HIV antibody positive | 0 | 0 |
| Cytological finding | ||
| NILM | 1 | 4 |
| LSIL | 2 | 1 |
| HSIL | 11 | 13 |
| N/A | 6 | 2 |
| * History of previous treatment | ||
| YES | 2 | 5 |
| NO | 17 | 15 |
| N/A | 1 | 0 |
| Follow up duration | ||
| <3years | 14 | 15 |
| ≥3years | 6 | 5 |
| Events | GLBL101c (N = 20) | Placebo (N = 20) | |||||
|---|---|---|---|---|---|---|---|
| No. of Patients | (%) | No. of Events | No. of Patients | (%) | No. of Events | * p-Value | |
| Constipation | 0 | 0 | 0 | 0 | 0 | 0 | - |
| Abdominal pain | 2 | 10 | 2 | 3 | 15 | 3 | 1.000 |
| Nausea | 1 | 5 | 1 | 0 | 0 | 0 | 1.000 |
| Palpitation | 0 | 0 | 0 | 0 | 0 | 0 | - |
| Headache | 4 | 20 | 6 | 1 | 5 | 1 | 0.342 |
| Peripheral neuropathy | 0 | 0 | 0 | 1 | 5 | 1 | 1.000 |
| Itch | 1 | 5 | 1 | 0 | 0 | 0 | 1.000 |
| Skin rash | 2 | 10 | 2 | 0 | 0 | 0 | 0.487 |
| The others | 7 | 35 | 13 | 6 | 30 | 12 | 1.000 |
| Total | 17 | 85 | 25 | 11 | 55 | 17 | 0.082 |
| Characteristics | Outcome (No. of Patients) | Total | p-Value | |||
|---|---|---|---|---|---|---|
| Histology at Week 16 | CR | PR | SD | PD | ||
| GLBL101c | 2 | 2 | 12 | 3 | 19 | 0.344 * |
| Placebo | 0 | 7 | 12 | 0 | 19 | |
| Cytology at week 16 | NILM | LSIL | HSIL | SCC | ||
| GLBL101c | 3 | 2 | 12 | 0 | 17 | 0.236 * |
| Placebo | 7 | 1 | 10 | 0 | 18 | |
| E7-specific immune response | Positive (9 weeks, 16 weeks) | Negative | ||||
| GLBL101c | 10 (4, 6) | 9 | 19 | 0.514 ** | ||
| Placebo | 7 (3, 4) | 12 | 19 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, Y.; Adachi, K.; Tomio, K.; Eguchi-Kojima, S.; Tsuruga, T.; Uchino-Mori, M.; Taguchi, A.; Komatsu, A.; Nagamatsu, T.; Oda, K.; et al. A Placebo-Controlled, Double-Blind Randomized (Phase IIB) Trial of Oral Administration with HPV16 E7-Expressing Lactobacillus, GLBL101c, for the Treatment of Cervical Intraepithelial Neoplasia Grade 2 (CIN2). Vaccines 2021, 9, 329. https://doi.org/10.3390/vaccines9040329
Ikeda Y, Adachi K, Tomio K, Eguchi-Kojima S, Tsuruga T, Uchino-Mori M, Taguchi A, Komatsu A, Nagamatsu T, Oda K, et al. A Placebo-Controlled, Double-Blind Randomized (Phase IIB) Trial of Oral Administration with HPV16 E7-Expressing Lactobacillus, GLBL101c, for the Treatment of Cervical Intraepithelial Neoplasia Grade 2 (CIN2). Vaccines. 2021; 9(4):329. https://doi.org/10.3390/vaccines9040329
Chicago/Turabian StyleIkeda, Yuji, Katsuyuki Adachi, Kensuke Tomio, Satoko Eguchi-Kojima, Tetsushi Tsuruga, Mayuyo Uchino-Mori, Ayumi Taguchi, Atsushi Komatsu, Takeshi Nagamatsu, Katsutoshi Oda, and et al. 2021. "A Placebo-Controlled, Double-Blind Randomized (Phase IIB) Trial of Oral Administration with HPV16 E7-Expressing Lactobacillus, GLBL101c, for the Treatment of Cervical Intraepithelial Neoplasia Grade 2 (CIN2)" Vaccines 9, no. 4: 329. https://doi.org/10.3390/vaccines9040329