
The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Sampling
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Comparison of Acceptance and Preferences for COVID-19 Vaccination between Two Phases
3.3. Influencing Factors of Vaccination Acceptance
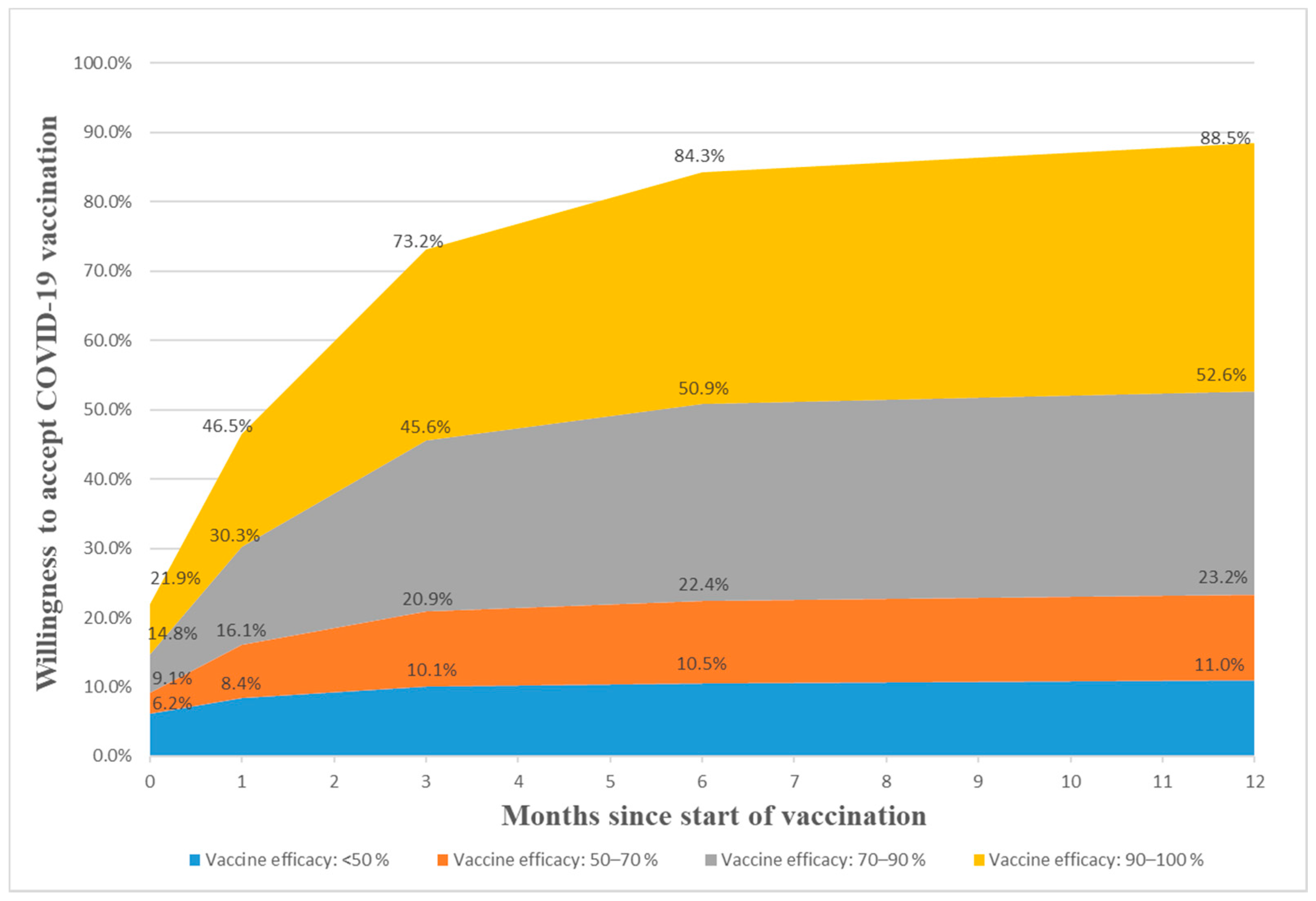
3.4. Public Preferences for COVID-19 Vaccines and Vaccination and Possible Ranges of Acceptance over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Items | Longitudinal Sample (n = 791) | Cross-Sectional Sample | |||
|---|---|---|---|---|---|
| Mar 2020 (Severe epidemic Phase) | Nov–Dec 2020 (Well-contained Phase) | Mar 2020 (Severe epidemic Phase) (n = 2058) | Nov–Dec 2020 (Well-contained Phase) (n = 2013) | ||
| N (%) | N (%) | N (%) | N (%) | ||
| Age group | |||||
| 18–25 | 119 (15.0) | 119 (15.0) | 475 (23.1) | 332 (16.5) | |
| 26–30 | 173 (21.9) | 173 (21.9) | 400 (19.4) | 434 (21.6) | |
| 31–40 | 260 (32.9) | 260 (32.9) | 523 (25.4) | 717 (35.6) | |
| 41–50 | 178 (22.5) | 178 (22.5) | 510 (24.8) | 360 (17.9) | |
| 51 and above | 61 (7.7) | 61 (7.7) | 150 (7.3) | 170 (8.4) | |
| Gender | |||||
| Female | 420 (53.1) | 420 (53.1) | 1115 (54.2) | 987 (49.0) | |
| Male | 371 (46.9) | 371 (46.9) | 943 (45.8) | 1026 (51.0) | |
| Highest level of education | |||||
| Middle school and below | 27 (3.4) | 27 (3.4) | 123 (6.0) | 111 (5.5) | |
| High school | 234 (29.6) | 234 (29.6) | 663 (32.2) | 585 (29.1) | |
| Associate or bachelor | 479 (60.6) | 479 (60.6) | 1140 (55.4) | 1214 (60.3) | |
| Master and above | 51 (6.5) | 51 (6.5) | 132 (6.4) | 103 (5.1) | |
| Marriage status | |||||
| Married | 592 (74.8) | 609 (77.0) | 1385 (67.3) | 1456 (72.3) | |
| Others (single, divorced or widowed) | 199 (25.2) | 182 (23.0) | 673 (32.7) | 557 (27.7) | |
| Location | |||||
| Central | 154 (19.5) | 136 (17.2) | 531 (25.8) | 409 (20.3) | |
| East | 536 (67.8) | 563 (71.2) | 1195 (58.1) | 1311 (65.1) | |
| West | 101 (12.8) | 92 (11.6) | 332 (16.1) | 293 (14.6) | |
| Region | |||||
| Rural | 113 (14.3) | 83 (10.5) | 420 (20.4) | 333 (16.5) | |
| Urban | 678 (85.7) | 708 (89.5) | 1638 (79.6) | 1680 (83.5) | |
| Employment status | |||||
| Employed | 695 (87.8) | 678 (85.7) | 1651 (80.2) | 1714 (85.1) | |
| Unemployed | 96 (12.2) | 113 (14.3) | 407 (19.8) | 299 (14.9) | |
| Health status | |||||
| Good and above (good, very good) | 594 (75.1) | 552 (69.8) | 1527 (74.2) | 1366 (67.9) | |
| Fair or below (fair, poor, very poor) | 197 (24.9) | 239 (30.2) | 531 (25.8) | 647 (32.1) | |
| Total annual family income in 2019 | |||||
| ≤CNY 50,000 (USD 7246) | 56 (7.1) | 56 (7.1) | 277 (13.4) | 207 (10.3) | |
| CNY 50,000–100,000 (USD 7246–14,492) | 139 (17.6) | 139 (17.6) | 548 (26.6) | 490 (24.3) | |
| CNY 100,000–150,000 (USD 14,492–21,739) | 191 (24.2) | 191 (24.2) | 506 (24.6) | 489 (24.3) | |
| CNY 150,000–200,000 (USD 21,739–28,986) | 181 (22.9) | 181 (22.9) | 352 (17.1) | 395 (19.6) | |
| CNY 200,000–300,000 (USD 28,986–43,478) | 139 (17.6) | 139 (17.6) | 239 (11.7) | 284 (14.1) | |
| ≥CNY 300,000 (USD 43,478) | 85 (10.7) | 85 (10.7) | 136 (6.6) | 148 (7.4) | |
| There are confirmed or suspected cases in the county | |||||
| Yes | 618 (78.1) | 518 (65.5) | 1538 (74.7) | 1282 (63.7) | |
| No or not clear | 173 (21.9) | 273 (34.5) | 520 (25.3) | 731 (36.3) | |
| Perceived risk of infection | |||||
| High or very high | 104 (13.2) | 206 (26.0) | 251 (12.2) | 498 (24.8) | |
| Fair | 238 (30.1) | 256 (32.4) | 575 (27.9) | 589 (29.3) | |
| Low or very low | 449 (56.8) | 329 (41.6) | 1232 (59.9) | 926 (46.0) | |
| Pandemic impact on daily life | |||||
| Large or very large | 550 (69.5) | 318 (40.2) | 1368 (66.5) | 844 (41.9) | |
| Fair | 173 (21.9) | 269 (34.0) | 497 (24.1) | 651 (32.3) | |
| Small or very small | 68 (8.6) | 204 (25.8) | 193 (9.4) | 518 (25.7) | |
| Pandemic impact on work | |||||
| Large or very large | 533 (67.4) | 318 (40.2) | 1326 (64.4) | 828 (41.1) | |
| Fair | 145 (18.3) | 244 (30.8) | 402 (19.5) | 583 (29.0) | |
| Small or very small | 72 (9.1) | 174 (22.0) | 191 (9.3) | 445 (22.1) | |
| Missing | 41 (5.2) | 55 (6.9) | 139 (6.8) | 157 (7.8) | |
| Pandemic impact on income | |||||
| Large or very large | 388 (49.1) | 263 (33.2) | 905 (44.0) | 753 (37.4) | |
| Fair | 203 (25.6) | 252 (31.9) | 467 (22.7) | 567 (28.2) | |
| Small or very small | 129 (16.3) | 191 (24.1) | 325 (15.8) | 458 (22.8) | |
| Missing | 71 (9.0) | 85 (10.8) | 361 (17.5) | 235 (11.7) | |
| Refused vaccination of a certain type of vaccine in the past | |||||
| Yes | 183 (23.1) | 183 (23.1) | 459 (22.3) | 437 (21.7) | |
| No | 608 (76.9) | 608 (76.9) | 1599 (77.7) | 1576 (78.3) | |
| Doctor’s recommendation is an important factor in vaccination decision-making | |||||
| Yes | 659 (83.3) | 645 (81.5) | 1659 (80.6) | 1625 (80.7) | |
| No | 132 (16.7) | 146 (18.5) | 399 (19.4) | 388 (19.3) | |
| Vaccination convenience (vaccination method, frequency, distance to vaccination sites, etc.) is an important factor in vaccination decision-making | |||||
| Yes | 577 (72.9) | 564 (71.3) | 1558 (75.7) | 1432(71.1) | |
| No | 214 (27.1) | 227 (28.7) | 500 (23.3) | 581 (28.9) | |
| Vaccine price is an important factor in vaccination decision-making | |||||
| Yes | 452 (57.1) | 444 (56.1) | 1233 (59.9) | 1197 (59.5) | |
| No | 339 (42.9) | 347 (43.9) | 825 (40.1) | 816 (40.5) | |
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 26 January 2021).
- WHO. Overview of the COVID-19 Pandemic. Available online: https://www.who.int/docs/default-source/coronaviruse/risk-comms-updates/epi-win-update40-overview-of-the-pandemic.pdf?sfvrsn=8d355bcd_4 (accessed on 16 January 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg 2020, 78, 185–193. [Google Scholar] [CrossRef]
- VOX, CEPR Policy Portal. Economics in the Time of COVID-19. Available online: https://www.incae.edu/sites/default/files/covid-19.pdf#page=52 (accessed on 24 December 2020).
- WHO. Update on COVID-19 Vaccine Development. Available online: https://www.who.int/docs/default-source/coronaviruse/risk-comms-updates/update45-vaccines-developement.pdf?sfvrsn=13098bfc_5 (accessed on 5 January 2021).
- WHO. Draft Landscape and Tracker of COVID-19 Candidate Vaccines. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 18 February 2021).
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e8961. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J.; Ayre, J.; Batcup, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Graffigna, G.; Palamenghi, L.; Boccia, S.; Barello, S. Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis. Vaccines 2020, 8, 576. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8. [Google Scholar] [CrossRef]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.; Robinson, E. Willingness to vaccinate against COVID-19 in the US: Longitudinal evidence from a nationally representative sample of adults from April–October 2020. medRxiv 2020, 2011–2020. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and Vaccine Hesitancy: A Longitudinal Study. SSRN 2020. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. National Trends in the US Public’s Likelihood of Getting a COVID-19 Vaccine—April 1 to December 8, 2020. JAMA 2020, 325, 396–398. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Dubé, E.; MacDonald, N.E. Chapter 26—Vaccine Acceptance: Barriers, Perceived Risks, Benefits, and Irrational Beliefs. In The Vaccine Book, 2nd ed.; Bloom, B.R., Lambert, P., Eds.; Academic Press: Cambridge, MA, USA, 2016; pp. 507–528. [Google Scholar]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- WHO. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf?ua=1 (accessed on 20 December 2020).
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Fressard, L.; Beck, F.; Legleye, S.; L’Haridon, O.; et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Dube, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef]
- Brown, K.F.; Long, S.J.; Ramsay, M.; Hudson, M.J.; Green, J.; Vincent, C.A.; Kroll, J.S.; Fraser, G.; Sevdalis, N. UK parents’ decision-making about measles–mumps–rubella (MMR) vaccine 10 years after the MMR-autism controversy: A qualitative analysis. Vaccine 2012, 30, 1855–1864. [Google Scholar] [CrossRef]
- Cottrell, S.; Roberts, R.J. Measles outbreak in Europe. BMJ 2011, 342, d3724. [Google Scholar] [CrossRef] [PubMed]
- Jansen, V.A.A. Measles Outbreaks in a Population with Declining Vaccine Uptake. Science 2003, 301, 804. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Wang, Z.; Chang, R.; Wang, H.; Xu, C.; Yu, X.; Tsamlag, L.; Dong, Y.; Wang, H.; Cai, Y. COVID-19 containment: China provides important lessons for global response. Front. Med. 2020, 14, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Xu, T.; Ao, M.; Zhou, X.; Zhu, W.; Nie, H.; Fang, J.; Sun, X.; Zheng, B.; Chen, X. China’s practice to prevent and control COVID-19 in the context of large population movement. Infect. Dis. Poverty 2020, 9. [Google Scholar] [CrossRef]
- Chen, S.; Yang, J.; Yang, W.; Wang, C.; Barnighausen, T. COVID-19 control in China during mass population movements at New Year. Lancet 2020, 395, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Yue, X.; Tchounwou, P.B. Response to the COVID-19 Epidemic: The Chinese Experience and Implications for Other Countries. Int. J. Environ. Res. Public Health 2020, 17, 2304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burki, T. China’s successful control of COVID-19. Lancet Infect. Dis. 2020, 20, 1240–1241. [Google Scholar] [CrossRef]
- Press Conference of the Joint Prevention and Control Mechanism of the State Council on March 12, 2020. Available online: http://www.gov.cn/xinwen/gwylflkjz54/index.htm (accessed on 18 December 2020).
- China: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/wpro/country/cn/ (accessed on 16 January 2021).
- Press Conference of the Joint Prevention and Control Mechanism of the State Council on December 31, 2020. Available online: http://www.gov.cn/xinwen/gwylflkjz143/index.htm (accessed on 1 January 2021).
- Press Conference of the Joint Prevention and Control Mechanism of the State Council on January 13, 2021. Available online: http://www.gov.cn/xinwen/gwylflkjz145/index.htm (accessed on 14 January 2021).
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021. [Google Scholar] [CrossRef]
- Maddux, J.E.; Rogers, R.W. Protection motivation and self-efficacy: A revised theory of fear appeals and attitude change. J. Exp. Soc. Psychol. 1983, 19, 469–479. [Google Scholar] [CrossRef]
- Maurer, J.; Harris, K.M.; Parker, A.; Lurie, N. Does receipt of seasonal influenza vaccine predict intention to receive novel H1N1 vaccine: Evidence from a nationally representative survey of U.S. adults. Vaccine 2009, 27, 5732–5734. [Google Scholar] [CrossRef] [Green Version]
- Eastwood, K.; Durrheim, D.N.; Jones, A.; Butler, M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med. J. Aust. 2010, 192, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Sypsa, V.; Livanios, T.; Psichogiou, M.; Malliori, M.; Tsiodras, S.; Nikolakopoulos, I.; Hatzakis, A. Public perceptions in relation to intention to receive pandemic influenza vaccination in a random population sample: Evidence from a cross-sectional telephone survey. Eurosurveillance 2009, 14, 19437. [Google Scholar] [CrossRef] [PubMed]
- Henrich, N.; Holmes, B. The public’s acceptance of novel vaccines during a pandemic: A focus group study and its application to influenza H1N1. Emerg. Health Threat. J. 2009, 2, e8. [Google Scholar] [CrossRef]
- Determann, D.; Korfage, I.J.; Lambooij, M.S.; Bliemer, M.; Richardus, J.H.; Steyerberg, E.W.; de Bekker-Grob, E.W. Acceptance of Vaccinations in Pandemic Outbreaks: A Discrete Choice Experiment. PLoS ONE 2014, 9, e102505. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Development and Licensure of Vaccines to Prevent COVID-19. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/development-and-licensure-vaccines-prevent-covid-19 (accessed on 15 January 2021).
- National Medical Products Administration. Guidelines for Clinical Evaluation of the COVID-19 Vaccine (in Trial). Available online: http://www.gov.cn/xinwen/2020-08/15/content_5535069.htm (accessed on 18 December 2020).
- WHO. WHO Target Product Profiles for COVID-19 Vaccines. Available online: https://www.who.int/publications/m/item/who-target-product-profiles-for-covid-19-vaccines (accessed on 23 December 2020).
- Kwok, K.O.; Lai, F.; Wei, W.I.; Wong, S.Y.S.; Tang, J.W.T. Herd immunity—Estimating the level required to halt the COVID-19 epidemics in affected countries. J. Infect. 2020, 80, e32–e33. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Xu, R.H.; Wong, E.L.Y.; Hung, C.T.; Feng, D.; Feng, Z.; Yeoh, E.K.; Wong, S.Y.S. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef] [PubMed]
- Press Conference of the Joint Prevention and Control Mechanism of the State Council on December 19, 2020. Available online: http://www.gov.cn/xinwen/gwylflkjz140/index.htm (accessed on 20 December 2020).
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.M.; Romero, J.R.; Bell, B.P. Postapproval Vaccine Safety Surveillance for COVID-19 Vaccines in the US. JAMA 2020, 324, 1937–1938. [Google Scholar] [CrossRef]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e4206. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Casuccio, A.; Restivo, V. Vaccination and Vaccine Effectiveness: A Commentary of Special Issue Editors. Vaccines 2020, 8, 545. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Building Vaccine Confidence Through Community Engagement. Available online: https://www.apa.org/topics/covid-19/equity-resources/building-vaccine-confidence.pdf (accessed on 18 February 2021).
- Building Confidence in COVID-19 Vaccines. Available online: https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence.html (accessed on 18 February 2021).
- Dhanda, S.; Osborne, V.; Lynn, E.; Shakir, S. Postmarketing studies: Can they provide a safety net for COVID-19 vaccines in the UK? BMJ Evid. Based Med. 2020, 111507. [Google Scholar] [CrossRef]
- Johansen, K.; Nicoll, A.; Ciancio, B.C.; Kramarz, P. Pandemic influenza A(H1N1) 2009 vaccines in the European Union. Eurosurveillance 2009, 14, 19361. [Google Scholar] [CrossRef]
- Piot, P.; Larson, H.J.; O. Brien, K.L.; N. Kengasong, J.; Ng, E.; Sow, S.; Kampmann, B. Immunization: Vital progress, unfinished agenda. Nature 2019, 575, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Items | Longitudinal Sample | Cross-Sectional Samples | ||||
|---|---|---|---|---|---|---|
| Mar 2020 (Severe epidemic Phase) | Nov–Dec 2020 (Well-contained Phase) | Mar 2020 (Severe epidemic Phase) | Nov–Dec 2020 (Well-contained Phase) | |||
| N (%) | N (%) | p-value | N (%) | N (%) | p-value | |
| Overall respondents | 791 (100) | 791 (100) | 2058 (100) | 2013 (100) | ||
| COVID-19 vaccination is an effective way to prevent and control COVID-19 | ||||||
| Yes | 718 (90.8) | 746 (94.3) | 1842 (89.5) | 1874 (93.1) | ||
| No | 73 (9.2) | 45 (5.7) | 0.007 | 216 (10.5) | 139 (6.9) | <0.001 |
| Accept vaccination if the COVID-19 vaccine is successfully developed and approved for listing in the future | ||||||
| Yes | 727 (91.9) | 701 (88.6) | 1879 (91.3) | 1782 (88.5) | ||
| No | 64 (8.1) | 90 (11.4) | 0.03 | 179 (8.7) | 231 (11.5) | 0.003 |
| Vaccine accept group | 727 (100) | 701 (100) | 1879 (100) | 1782 (100) | ||
| Want to receive vaccination as soon as possible when the vaccine is available | ||||||
| Yes, as soon as possible | 424 (58.3) | 161 (23.0) | 980 (52.2) | 441 (24.7) | ||
| No, delay vaccination until I confirmed the vaccine safety | 303 (41.7) | 540 (77.0) | <0.001 | 899 (47.8) | 1341 (75.3) | <0.001 |
| Prefer which kind of immunization schedules of the COVID-19 vaccination | ||||||
| Routine immunization | 333 (45.8) | 340 (48.5) | 928 (49.4) | 904 (50.7) | ||
| Emergency vaccination | 79 (10.9) | 94 (13.4) | 169 (9.0) | 223 (12.5) | ||
| Both are acceptable | 315 (43.3) | 267 (38.1) | 0.09 | 782 (41.6) | 655 (36.8) | <0.001 |
| Prefer which type of COVID-19 vaccines | ||||||
| Domestic vaccine | 235 (32.3) | 338 (48.2) | 611 (32.5) | 975 (54.7) | ||
| Imported vaccine | 30 (4.1) | 24 (3.4) | 62 (3.3) | 59 (3.3) | ||
| Both are acceptable | 462 (63.6) | 339 (48.4) | <0.001 | 1206 (64.2) | 748 (42.0) | <0.001 |
| Characteristics | Longitudinal Sample | Pooled Cross-Sectional Sample | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | SE | p-Value | 95% CI | OR | SE | p-Value | 95% CI | |||
| Phase | ||||||||||
| Severe epidemic phase | Ref | Ref | ||||||||
| Well-contained phase | 0.12 | 0.02 | <0.001 | (0.08, 0.18) | 0.19 | 0.03 | <0.001 | (0.14, 0.25) | ||
| Age group | ||||||||||
| 18~25 | Ref | Ref | ||||||||
| 26~30 | 1.19 | 0.36 | 0.58 | (0.65, 2.15) | 1.13 | 0.20 | 0.50 | (0.80, 1.59) | ||
| 31~40 | 1.35 | 0.41 | 0.32 | (0.74, 2.47) | 1.07 | 0.20 | 0.71 | (0.75, 1.53) | ||
| 41~50 | 1.39 | 0.44 | 0.31 | (0.74, 2.59) | 1.06 | 0.20 | 0.77 | (0.73, 1.53) | ||
| >51 | 1.79 | 0.79 | 0.19 | (0.75, 4.27) | 1.14 | 0.28 | 0.59 | (0.70, 1.86) | ||
| Gender | ||||||||||
| Female | Ref | Ref | ||||||||
| Male | 1.15 | 0.18 | 0.37 | (0.85, 1.55) | 1.29 | 0.12 | 0.01 | (1.07, 1.54) | ||
| Highest level of education | ||||||||||
| Middle school and below | Ref | Ref | ||||||||
| High school | 1.71 | 0.79 | 0.25 | (0.69, 4.25) | 0.92 | 0.19 | 0.67 | (0.61, 1.38) | ||
| Associate or Bachelor | 1.45 | 0.69 | 0.43 | (0.57, 3.67) | 0.85 | 0.18 | 0.45 | (0.56, 1.29) | ||
| Master and above | 1.08 | 0.61 | 0.89 | (0.36, 3.24) | 0.79 | 0.22 | 0.39 | (0.45, 1.36) | ||
| Marriage status | ||||||||||
| Others (Single, Divorced or Widowed) | Ref | Ref | ||||||||
| Married | 1.48 | 0.33 | 0.08 | (0.95, 2.30) | 1.78 | 0.25 | <0.001 | (1.35, 2.35) | ||
| Location | ||||||||||
| Central | Ref | Ref | ||||||||
| East | 0.65 | 0.13 | 0.03 | (0.44, 0.96) | 0.85 | 0.09 | 0.13 | (0.68, 1.05) | ||
| West | 0.64 | 0.17 | 0.10 | (0.37, 1.09) | 0.94 | 0.14 | 0.67 | (0.71, 1.25) | ||
| Region | ||||||||||
| Rural | Ref | Ref | ||||||||
| Urban | 0.53 | 0.12 | 0.01 | (0.34, 0.84) | 0.85 | 0.10 | 0.18 | (0.67, 1.08) | ||
| Employment status | ||||||||||
| Unemployed | Ref | Ref | ||||||||
| Employed | 0.99 | 0.76 | 0.99 | (0.22, 4.44) | 0.74 | 0.31 | 0.48 | (0.33, 1.69) | ||
| Health status | ||||||||||
| Fair or below (fair, poor, very poor) | Ref | Ref | ||||||||
| Good and above (good, very good) | 1.18 | 0.21 | 0.33 | (0.84, 1.66) | 1.13 | 0.12 | 0.23 | (0.92, 1.38) | ||
| Total family income in 2019 | ||||||||||
| ≤CNY 50,000 | Ref | Ref | ||||||||
| CNY 50,000–100,000 | 0.90 | 0.31 | 0.76 | (0.46, 1.75) | 0.66 | 0.11 | 0.01 | (0.48, 0.91) | ||
| CNY 100,000–150,000 | 0.96 | 0.33 | 0.90 | (0.49, 1.87) | 0.61 | 0.10 | <0.001 | (0.44, 0.86) | ||
| CNY 150,000–200,000 | 0.69 | 0.25 | 0.30 | (0.34, 1.39) | 0.66 | 0.12 | 0.02 | (0.46, 0.95) | ||
| CNY 200,000–300,000 | 1.25 | 0.48 | 0.55 | (0.60, 2.64) | 0.76 | 0.15 | 0.18 | (0.51, 1.13) | ||
| ≥CNY 300,000 | 1.61 | 0.67 | 0.25 | (0.71, 3.64) | 1.03 | 0.24 | 0.90 | (0.66, 1.62) | ||
| Refused vaccination of a certain type of vaccine in the past | ||||||||||
| No | Ref | Ref | ||||||||
| Yes | 0.57 | 0.10 | <0.001 | (0.40, 0.82) | 0.78 | 0.09 | 0.03 | (0.63, 0.97) | ||
| There are confirmed or suspected cases in the county | ||||||||||
| No or not clear | Ref | Ref | ||||||||
| Yes | 0.69 | 0.12 | 0.03 | (0.49, 0.96) | 0.76 | 0.08 | 0.01 | (0.62, 0.92) | ||
| Perceived risk of infection | ||||||||||
| Fair | Ref | Ref | ||||||||
| High or very high | 1.59 | 0.33 | 0.03 | (1.06, 2.40) | 1.83 | 0.25 | <0.001 | (1.41, 2.38) | ||
| Low or very low | 0.87 | 0.15 | 0.43 | (0.63, 1.22) | 1.06 | 0.11 | 0.58 | (0.86, 1.30) | ||
| Pandemic impact on daily life | ||||||||||
| Fair | Ref | Ref | ||||||||
| Large or very large | 0.93 | 0.17 | 0.70 | (0.65, 1.33) | 1.05 | 0.12 | 0.64 | (0.85, 1.31) | ||
| Small or very small | 0.95 | 0.24 | 0.85 | (0.58, 1.56) | 0.89 | 0.14 | 0.47 | (0.66, 1.21) | ||
| Pandemic impact on work | ||||||||||
| Fair | Ref | Ref | ||||||||
| Large or very large | 0.94 | 0.19 | 0.77 | (0.64, 1.39) | 1.12 | 0.14 | 0.35 | (0.88, 1.43) | ||
| Small or very small | 0.77 | 0.20 | 0.33 | (0.46, 1.30) | 0.99 | 0.17 | 0.96 | (0.71, 1.38) | ||
| Pandemic impact on income | ||||||||||
| Fair | Ref | Ref | ||||||||
| Large or very large | 1.05 | 0.19 | 0.79 | (0.73, 1.51) | 1.00 | 0.12 | 0.98 | (0.79, 1.26) | ||
| Small or very small | 0.80 | 0.18 | 0.31 | (0.51, 1.24) | 0.79 | 0.11 | 0.10 | (0.59, 1.05) | ||
| COVID-19 vaccination is an effective way to prevent and control COVID-19 | ||||||||||
| No | Ref | Ref | ||||||||
| Yes | 2.07 | 0.69 | 0.03 | (1.07, 3.99) | 1.89 | 0.36 | <0.001 | (1.30, 2.74) | ||
| Doctor’s recommendation is an important factor in vaccination decision-making | ||||||||||
| No | Ref | Ref | ||||||||
| Yes | 3.13 | 0.75 | <0.001 | (1.96, 5.01) | 2.72 | 0.39 | <0.001 | (2.06, 3.59) | ||
| Vaccination convenience is an important factor in vaccination decision-making | ||||||||||
| No | Ref | Ref | ||||||||
| Yes | 0.64 | 0.11 | 0.01 | (0.46, 0.91) | 0.59 | 0.07 | <0.001 | (0.47, 0.74) | ||
| Vaccine price is an important factor in vaccination decision-making | ||||||||||
| No | Ref | Ref | ||||||||
| Yes | 0.54 | 0.09 | <0.001 | (0.40, 0.74) | 0.53 | 0.05 | <0.001 | (0.44, 0.65) | ||
| Items | N (%) |
|---|---|
| Vaccine accept group | 1782 (100) |
| Prefer when to get vaccinated (weekday/weekend) | |
| Weekday (Monday to Friday) | 150(8.4) |
| Weekend (Saturday or Sunday) | 761(42.7) |
| Both are acceptable | 871(48.9) |
| Prefer when to get vaccinated (day/night time) | |
| Day time | 1102 (61.8) |
| Night time | 34 (1.9) |
| Both are acceptable | 646 (36.3) |
| Prefer where to get vaccinated | |
| Secondary/ Tertiary hospital | 597 (33.5) |
| Primary hospital | 353 (19.8) |
| Local centers for disease control and prevention | 524 (29.4) |
| Temporary vaccination sites (e.g., set in workplace or school) | 208 (11.7) |
| Residents’ committee/ Villagers’ committees | 94 (5.3) |
| Private hospital | 6 (0.3) |
| Willing to accept vaccination at what level of vaccine efficacy | |
| Willing to accept vaccination at any level | 135 (7.6) |
| At least 30% | 87 (4.9) |
| At least 50% | 246 (13.8) |
| At least 70% | 591 (33.2) |
| At least 90% | 723 (40.6) |
| Vaccine delay group | 1341 (100) |
| The duration of delaying vaccination to see the vaccine safety | |
| At least 1 month | 495 (36.9) |
| At least 3 months | 537 (40.0) |
| At least 6 months | 224 (16.7) |
| At least 1 year | 85 (6.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Lu, X.; Lai, X.; Lyu, Y.; Zhang, H.; Fenghuang, Y.; Jing, R.; Li, L.; Yu, W.; Fang, H. The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study. Vaccines 2021, 9, 191. https://doi.org/10.3390/vaccines9030191
Wang J, Lu X, Lai X, Lyu Y, Zhang H, Fenghuang Y, Jing R, Li L, Yu W, Fang H. The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study. Vaccines. 2021; 9(3):191. https://doi.org/10.3390/vaccines9030191
Chicago/Turabian StyleWang, Jiahao, Xinran Lu, Xiaozhen Lai, Yun Lyu, Haijun Zhang, Yufei Fenghuang, Rize Jing, Li Li, Wenzhou Yu, and Hai Fang. 2021. "The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study" Vaccines 9, no. 3: 191. https://doi.org/10.3390/vaccines9030191