Assessing Vaccination Delivery Strategies for Zero-Dose and Under-Immunized Children in the Fragile Context of Somalia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Setting
2.2. Study Design
2.3. Sampling
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Theme 1: Identification of Zero-Dose Children and Missed Communities
“There is insufficient data on the number of children under the age of one who reside even in the areas where health facilities are located because the routine immunization coverage reporting cannot be used to estimate the number of unvaccinated children as these children may have never been in contact with the health system. It is difficult to plan for population whose size and numbers are unknown. Large communities live in remote and inaccessible areas or places that cannot be visited due to insecurity”.(MoH official, KII)
“Zero dose children live everywhere in the country. The basis of my argument is related to the limited access to health services particularly immunization services in many places. If the mother does not have access to a health facility or immunization services (delivered as an outreach or mobile), it is highly likely that the (her) child will be zero dose. For instance, Bosaso city (which is the third most populous city in Somalia), we have conducted pre-registration (enumeration) to count the number of children under one year and under five years living in the city. The aim was to get a target denominator for Bossaso city before a new urban immunization strategy was implemented. The previous target denominator (before the registration) was 13,000 children but this time we obtained 28,000 under one-year children”.(Humanitarian health worker, KII)
“These [zero dose] children reside in rural regions, villages, remote areas, and IDP camps, but in order to find out how many there are in total, a census or survey must be conducted in the areas”.(MoH official, KII)
“In general, there are a large number of children in Somalia who are not vaccinated for a variety of reasons. The first group of people are those who live in rural areas or remote villages without a health centre where mobile teams are unable to travel. The second group consists of children who live in IDPs; many of these children have not had any vaccines even though they live in towns where most vaccinations are provided at facilities nearby. Some urban residents do not vaccinate their children particularly those with low socio-economic status while others refuse it on religious beliefs and cultural grounds”.(MoH official, KII)
3.1.1. Nomadic Populations
“We do not know how many of these children there are in the nomadic groups, let alone the percentage of immunized and un-immunized children. Regular routine immunization delivered through fixed sites does not offer convenient access to immunization for these communities and outreach programmes specifically designed for them are non-existent”.(MoH official, KII)
“Some of the challenges to expanding immunization services to rural areas [where nomadic populations reside] are related to resources and electricity, while others are related to security and geographic accessibility”.(MoH official, KII)
“We have not conducted specific surveys to estimate and identify these children in pastoralist communities. We classify the great majority of them as un-immunized not only because the data on these communities is limited but there are no immunization services for them that can report coverage data”.(MoH official, KII)
“I think if all the small villages across the country had primary health units which could provide routine immunization services, more children in the nomadic communities could get vaccinated. The outreach programmes do not offer routine immunization and only become popular response when there is an outbreak of measles, cholera or during polio national immunization days”.(Vaccinator, FGD)
3.1.2. Internally Displaced People (IDPs)
“The IDP population changes constantly. New arrivals are received daily in some towns of the country. Most of the IDPs live in overcrowded informal temporary settlements which face threats of eviction. We estimate the number of households in each camp through the data captured in the provision of humanitarian assistance [food and cash assistance] but the actual number of people and composition is not known, particularly the number of children in each household. Some IDPs move between camps in the same town or to other parts of the country. We identify the IDP children as under-immunized because most of them originate from areas [rural villages, nomadic areas and locations controlled by Al-shabaab] where there are not regular immunization services”.(NGO worker, KII)
“Many IDP camps have fixed health centres or are located in the vicinity of health facilities where they share with host communities. Despite, lack of disaggregation of the rate of coverage between IDP and host communities, it is possible to analyse the data from health centres in IDP camps”.(MoH official, KII)
“People who have been living in an IDP camp for a long time may vaccinate their children, but zero-dose children are often from families who migrate to a new city every month, and those who originate from inaccessible places in Somalia”.(Vaccinator, FGD)
“IDPs live in major cities where they earn their livelihood, where there are good health facilities. Their challenges stem from their livelihood. They are casual labourers (manual labour). They leave home early in the morning and come back in the evening sometimes late but the working hours of the health facilities (health workers) are between 7 a.m. to 2 p.m. therefore there is missed opportunity here which is very high. They take some of the children with them and leave others at home. The children who are left at home cannot be immunized during the outreach because of lack of parental consent. We cannot say that they have access to health services even though the health facilities are very close. For these families, immunization is not a priority for them, survival and earning an income (livelihood) is”.(Vaccinator, FGD)
3.1.3. Populations Living in Al-Shabaab-Controlled Areas
“Large areas of Galmudug are inaccessible due to insecurity, preventing the government and partners from reaching the people living in those areas and providing basic social services. The majority of these places are home to unvaccinated children, and they are in large numbers, with Al-Shabaab militants controlling roughly 40% or 50%”.(MoH officials, KII)
“Of course, reaching unvaccinated children is a priority (zero dose) for us but where they live is a challenge; in remote areas where the government has no control. There are genuine security concerns here as well. There have been reports of workers being kidnapped and held captive for months”.(MoH official, KII)
“There are numerous areas that cannot be visited due to security concerns. Children receive immunizations in locations from Bulo-Gadud to Kismayo town (small area), but beyond that, about 30 km from Bar-Sanguni (a nearby village to Kismayo), there are no vaccination facilities at all. The situation of the rural population is much worse, which is why there are so many outbreaks”.(Humanitarian health worker, KII)
“The immediate and most important aspect is to focus on security. Secondly, to secure the resources to reach these destinations. Opening a new health centre is not an easy task, so it is appropriate during the transition time to temporarily facilitate service delivery, such as using outreach programmes or mobile teams. Additionally, social media, community gatherings, and meetings will be used to raise awareness on immunizations”.(MoH official, KII)
3.1.4. Other Missed Subgroups
“It is not a choice for many poor parents to vaccinate their children or not. They have bigger and more urgent struggles in their life; finding work, earning livelihood, housing, ill-health and unlike IDPs, most of them do not get assistance from the humanitarian agencies. These groups are very diverse. They could be minority communities living together in deprived areas in towns and cities where there are no good health facilities or could be individual poor families spread across different quarters in towns and cities”.(MoH official, KII)
“Unvaccinated children can be found in a variety of settings, including cities, remote locations, and areas of conflict, particularly in areas where the government has little authority. The zero dose children may live in cities with parents who embrace inaccurate beliefs about vaccines, such as that immunizations result in infertility”.(Humanitarian health worker, KII)
“Some of the poor families in the neighbourhood of this health centre do not bring their children to the health facility for immunization. I talked to one family who said that they were not fully informed of the benefits of vaccination. Since their children were healthy, thanks to Allah, they did not think they needed to bring them to the health canter”.(Vaccinatr, FGD)
“I have recently visited the villages along the Indian Ocean in Karkaar and Gardafui regions (Puntland). I witnessed widespread deprivation and lack of basic health services for some of these communities, particularly the minority community in Garduush village. I have no doubt that the great majority of the children in these communities were not immunized”.(Humanitarian health worker, KII)
“I have not seen any study which was specifically done on immunization service delivery and uptake for marginalized groups but when we were discussing about urban immunization strategy, we looked into the existing barriers to immunization in major cities and towns such as Galkacyo, Burtinle, Garowe and Bosaso. We did not differentiate the barriers that had affected particular groups but daily stressors [livelihood circumstances, poverty, distance] and lack of education and awareness were noted as common impediments to access to immunization services”.(Humanitarian health worker, KII)
3.2. Theme 2: Reaching Zero-Dose Children and Missed Communities
3.2.1. Existing Immunization Policies and Strategies
“In reality, the focus of the national immunization policy is on vaccination in general. There is a brief mention of “missing doses” (p. 20) which does not fit with the scale and gravity of unvaccinated children in the country. I think there is no other way except to start with a separate strategy that focuses specifically on children who have not received any vaccine. Because there are more children who haven’t yet been vaccinated, this special strategy should chart how to identify and reach them, without interrupting the ongoing routine immunization activities”.(MoH official, KII)
“I do not know how we are going to do it, but a unique programme should be developed to reach areas where zero-dose children are detected, such as communities without a health centre, people in IDPs camps, and rural communities. Let’s have a look at how to vaccinate the newly displaced people. I believe these issues should be prioritized because vaccine-preventable diseases (VPDs) can spread from one child with a zero dose to another”.(MoH official, KII)
“In the strategy, there are components that ensure zero dose children are reached such as pre-immunization registration (head count of children) in order to set an accurate and actual target denominator. Thus, you can know the target children (number of children) to be vaccinated each month during the course of the year. This strategy was abandoned due to lack of funds”.(Immunization programme officer, KII)
3.2.2. Local Participation in Planning and Decision Making
“The Ministry of Health, WHO and UNICEF are at the forefront of planning and coordination. We are seen as the implementers. We take part in the health sector coordination meetings. We mainly contribute to discussions about community needs and service delivery issues but our leverage is limited when it comes to policy development and planning unless we are the ones paying for the work to formulate and implement such policies and plans”.(A senior official of a local NGO, KII)
“In these meetings, discussions are focused on the progress of the immunization activities per the workplans, analysing the data on vaccination coverage and the challenges that have been encountered. If the coverage is low, then the cause is investigated, and an action plan is agreed to improve the situation and increase the coverage. This information is rallied to the health canters where the vaccination programme is delivered”.(Community member and a former local NGO staff, FGD)
3.2.3. Immunization Service Delivery (Availability and Accessibility)
“Either you live a place close to health facility where routine immunization is available or you are covered by occasional outreach programme. There is no other way you can get your children vaccinated particularly if you live in a remote location or places where the government is not present”.(MoH official, KII)
“In Somalia, UN agencies manage resources [vaccines] from the point of purchase to the health centre where they are used, however, the government may be engaged in the planning. We, in Puntland, manage the central cold chain for the State, but UN agencies (WHO, UNICEF) provide all financial assistance, logistics, and personnel salaries. The government’s involvement is limited to planning, forecasting, and occasionally budgeting of operating costs, which they [UN] also manage [funds]”.(MoH official, KII)
“Everything came to standstill. Vaccine transportation has been halted due to flight restrictions. Our main vaccine store is in Nairobi, and there have been some delays, resulting in supply shortages. Additionally, the community’s connectivity was restricted, and people were advised to stay at home. As a result, vaccination uptake was extremely low because many people did not visit health centres or other locations where vaccinations were administered. It was really difficult time for us to conduct an immunization, supervision or any kind of work at the time”.(MoH official, KII)
“COVID-19 has impacted on all health services. Many people have been unable to come to the health centre for months, leading to a decrease in the number of people being served. The people themselves have been affected, and mothers refused to come and bring their children”.(MoH official, KII)
3.2.4. Resources and Capacities
“WHO and UNICEF support our vaccination programme. We are dedicated to promoting immunization across the country. Our partners have an interest to see that through. We have rough idea about the sort of communities where zero-dose children live but to be honest, we need adequate resources. Our capacity is limited but with resources, we can adapt strategies specifically targeting zero dose children and we can build our capacities to develop and implement effective plans and interventions”.(MoH official, KII)
“I hear that donors are providing lots of money to immunization services. Those of us at the FMS MoH level do not have information about the total amount of all that money. But we must have some kind of accountability and transparency. We can start with correcting the balance in decision making, implementation and oversight. Not only do we need an inclusive authority to coordinate and allocate the resources, we must have independent body to scrutinize the utilization of the resources”.(MoH official, KII)
“The immunization service should be equitably distributed. The health care professionals who perform immunization services and the communities should be consulted, and the few resources available should be allocated fairly and in accordance with the priorities and demands of each location”.(MoH official, KII)
“The biggest impact of COVID-19 happened in 2021 and 2022, when regular immunization was diverted and the focus was shifted to COVAX, resulting in a drop in coverage in the Banadir region. The lockdown and the fear of the infection forced many people not to go to the health centers. People were being advised to keep away from one another, resulting in low coverage, and employees who were expected to work in EPI were focused on the COVAX vaccine”.(MoH official, KII)
3.2.5. Integration with Other Health Programmes
“We all agree that it [immunization] is intertwined with other health services such as vitamin A administration and nutrition. A health card containing information about the different services given to the child such as immunization could be made mandatory to receive health services”.(MoH official, KII)
“It is absolutely essential to combine vaccination with other health services. For example, if a mother attends ANC, she is taught how to get her child vaccinated and the importance of vaccination. Besides that, the mother is given information about the health risks if the child is not vaccinated. As a result, other health services often help and increase the number of children reached. It is critical, and I advocate that other health services be linked to vaccination. As far as we can reveal, it is a good thing. If vaccination is not highlighted in all health service delivery, public and private, then the importance of vaccination will not be realized. If the mother of the sick child is informed of the advantages of the vaccine while she is receiving medical help, she will accept it and spread the message to others”.(MoH official, KII)
3.2.6. Community and Individual-Level Vaccine Uptake
“Communities participate in immunization, but it is not enough. The scholars participate, young women and educated people vaccinate their children but there is a lack of ownership, or a lack of direction and urgency for taking ownership of immunization. I think there is a need for government—community partnership. On the other hand, those who are misinformed, such as the Takfir religious group who believe that vaccines are not safe and question their permissibility in Islam, need a different approach, like active engagement and well-planned community led, religion-based strategy to fight misinformation”(Vaccinator, FGD)
“People have different views on vaccines. One-person next door to the MCH may reject them, while another may go a long distance to have their child vaccinated. Some people reject it for no obvious reasons, while others reject it because of incorrect information they have received from others or worries about harm on their children or they do not believe in its benefits. Perhaps those who refuse vaccination would listen to and share their private worries or reasons with people they trust such as midwives and other prominent people in the community”.
3.3. Theme 3: Monitoring and Measuring the Identification of Zero-Dose Children and the Progress of Immunization Interventions
“The MoH has a master list of all health facilities. Each health facility is designated to a catchment area and population. The population size of each area was calculated by adding the estimated data from the PESS 2014 with a 2.5% annual increment”.(MoH official, KII)
“All our sources of official data are poor. Civil registrations do not exist. The population estimate [PESS 2014] was conducted a long time ago, at a time when most of the South-Central Somalia was controlled by Alshabaab and the health and demographic survey [SHDS 2020] did not provide us concrete information about population sizes and compositions in different regions and communities. This is a cross-departmental issue and affects all basic social service delivery. However, we have now improved the reporting of health data including immunization coverage through our HMIS”.(MoJ official, KII)
“We report the number of children we immunized and the MoH calculate the coverage rate. To be candid about the immunization data, when we do not have accurate number of children in our area or who they are, we cannot measure performance and cannot set targets for increasing the uptake. Our immunization coverage rate is actually more of reporting requirement than useful tool for planning”.(Vaccinator, FGD)
“The target is children under nine (9) months old, and vaccination is planned based on centre needs. In addition to the lack of a specific target or precise microplan, the challenge arises from not having accurate statistics on vaccinated children due to continuous immigrant [IDPs, nomadic population] influx”.(MoH official, KII)
“If the Maternal and Child Health (MCH) clinic claims to have vaccinated 500 children, this information should be on the contact list, and their details [parent telephone numbers] should be in the registries. I’ve personally dialled random numbers to cross-check. There’s a system in place to verify the accuracy of the provided information”.(MoH official, KII)
“Vaccinated children from PENTA 1 and PENTA 3 are compared, assessing dropout rates and taking steps to understand access and utilization”.(Immunization programme officer, KII)
“Vaccination-related information is indeed utilized. Regular meetings, such as our technical working group meeting (TWG), occur alongside immunization meetings at district and regional levels. These sessions evaluate vaccine centre operations, administration, development, and community coverage. If coverage is low, the cause is identified, methods to enhance it are explored, and solutions are sought”.(MoH official, KII)
3.4. Theme 4: Engagement and Advocacy Approach for Reaching Zero-Dose Children
3.4.1. Political Leadership and Accountability
“We hold regular Health Cluster meetings. WHO, UNICEF, UNFPA and, to lesser extent, the International NGOs dominate this forum and set the agenda. Although the information about the meetings is publicly available, they are not more than progress updates and the cluster became a programming stage to prevent overlap of interventions among the UN and International organisations”.(MoH official, KII)
“We cannot judge commitment just by the occasional presence of top government officials in immunization events. We want them to make promoting immunization every day task which feature in all events. We want them to engage religious Sheikhs and raise awareness in the mosques. We want then to engage elders in the rural communities and propagate the messages in community gathering in the villages. And above all, we want them to hold the MoH and partner organizations accountable for this life-saving service”.(Vaccinator, FGD)
“All the immunization campaigns are launched by the ministries of health, and some instances by the FGS [Federal Government of Somalia] president and FMS [Federal Member States] presidents. This public show of support is very important for the immunization and underscore the leadership understanding and commitment for these preventative services”.(Community member, FGD)
“I think it would send a powerful signal of support if the top political, clan and religious leaders were seen taking their children to health facilities for immunization, not just a minister cutting ribbon or putting vaccine drops into a child’s mouth for the start of immunization campaign”.(Community member, FGD)
3.4.2. Partnership and Collaboration for Advocacy
“UNICEF and WHO wield huge influence because funds for the immunization programme are channelled through them and they have lots of experience and expertise at their disposal. With money, you can hire specialists and experts in the field”.(Humanitarian health worker, KII)
3.4.3. Community Engagement
“Each village has a Community Health Committee (CHC) that educates people and reports on community needs. In addition, throughout health projects, we use community health workers (CHWs) who connect the community and health centres and participate in areas where vaccinations are administered to bring people together. At times, such as World Immunization Day, the community members are called to meetings to educate them on the benefits of vaccination. CHC comprise of respected individuals in the community (scholars, midwives, and elders) in order to persuade the people of the importance of vaccination”.(MoH official, KII)
“The majority of advocates are young individuals, particularly females. It would be beneficial to involve other prominent and influential people in the community, such as elders so that they (social mobilizers) have better patronage to inform and persuade the community”.(Vaccinator, FGD)
“The MoH and implementing agencies need to understand that social mobilization and service delivery cannot be decoupled. The social mobilizers must be integrated with the health facilities and led by healthcare professionals who are respected in the local community. I think it would be helpful if local governors and community leaders sometimes deliver the messages”.(Community member, FGD)
“The people who work on raising awareness are very few in comparison to the community and size of the areas to be served. Awareness is the first and most important step to sensitize the community and promote acceptance. Hiring people who the community can trust and is willing to learn from them is very crucial if the awareness raising has to succeed”.(Vaccinator, FGD)
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMGF | Bill and Melinda Gates Foundation |
| DTP | Diphtheria, Tetanus, and Pertussis |
| EPHS | Essential Packages of Health Services |
| EPI | Expanded Programme on Immunization |
| FGS | Federal Government of Somalia |
| FMS | Federal Member States |
| GBD | Global Burden of Diseases |
| HSSP | Health Sector Strategic Plan |
| IDP | Internally Displaced Persons |
| LSHTM | London School of Tropical Medicine |
| MoH | Ministry of Health |
| NGO | Non-governmental organization |
| PENTA | Pentavalent Vaccine (diphtheria, tetanus, whooping cough (pertussis), polio and Hib disease (Haemophilus influenzae type b)) |
| PESS | Population Estimate Survey of Somalia |
| SHDS | Somalia Health and Demographic Survey |
| SIDRA | Somali Institute for Development Research and Analysis |
| UN | United Nations |
| UNFPA | United National Population Fund |
| UNICEF | United Nations Children’s Fund |
| WHO | World Health Organization |
References
- United Nations Children’s Fund. The State of the World’s Children 2023: For Every Child, Vaccination; UNICEF Innocenti—Global Office of Research and Foresight: Florence, Italy, 2023; Available online: https://www.unicef.org/media/108161/file/SOWC-2023-full-report-English.pdf (accessed on 11 September 2023).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030 (accessed on 11 September 2023).
- Carter, A.; Msemburi, W.; Sim, S.Y.; Gaythorpe, K.A.; Lambach, P.; Lindstrand, A.; Hutubessy, R. Modeling the impact of vaccination for the immunization Agenda 2030: Deaths averted due to vaccination against 14 pathogens in 194 countries from 2021 to 2030. Vaccine 2023. [Google Scholar] [CrossRef]
- Galles, N.C.; Liu, P.Y.; Updike, R.L.; Fullman, N.; Nguyen, J.; Rolfe, S.; Sbarra, A.N.; Schipp, M.F.; Marks, A.; Abady, G.G.; et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980–2019: A systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021, 398, 503–521. [Google Scholar] [CrossRef]
- UNICEF. Somalia Key Demographics Indicators. Available online: https://data.unicef.org/country/som/ (accessed on 12 November 2023).
- Wigley, A.; Lorin, J.; Hogan, D.; Utazi, C.E.; Hagedorn, B.; Dansereau, E.; Tatem, A.J.; Tejedor-Garavito, N. Estimates of the number and distribution of zero-dose and under-immunised children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLoS Glob. Public Health 2022, 2, e0001126. [Google Scholar] [CrossRef]
- Somalia Health Sector Strategic Plan 2022–2026 (HSSP III); Ministry of Health and Human Services, Federal Government of Somalia: Mogadishu, Somalia, 2021. Available online: https://moh.gov.so/so/wp-content/uploads/2022/11/Health-Sector-Strategy-Plan-III.pdf (accessed on 22 August 2023).
- Warsame, A.; Frison, S.; Checchi, F. Drought, armed conflict and population mortality in Somalia, 2014–2018: A statistical analysis. PLoS Glob Public Health 2023, 3, e0001136. [Google Scholar] [CrossRef]
- Nagata, J.M.; Epstein, A.; Ganson, K.T.; Benmarhnia, T.; Weiser, S.D. Drought and child vaccination coverage in 22 countries in sub-Saharan Africa: A retrospective analysis of national survey data from 2011 to 2019. PLoS Med. 2021, 18, e1003678. [Google Scholar] [CrossRef]
- Bellizzi, S.; Lane, C.; Elhakim, M.; Nabeth, P. Health consequences of drought in the WHO Eastern Mediterranean Region: Hotspot areas and needed actions. Environ. Health 2020, 19, 114. [Google Scholar] [CrossRef] [PubMed]
- Population Estimation Survey of Somalia 2014; The Ministry of Planning, Federal Government of Somalia and UNFPA, Somalia Country Office: Mogadishu, Somalia, 2014. Available online: https://somalia.unfpa.org/sites/default/files/pub-pdf/Population-Estimation-Survey-of-Somalia-PESS-2013-2014.pdf (accessed on 12 September 2023).
- WHO; UNICEF. Somalia: Estimates of Immunization Coverage: 2022 Revision. 2022. Available online: https://data.unicef.org/wp-content/uploads/cp/immunisation/som.pdf (accessed on 28 October 2023).
- Somalia Health and Demographic Survey, 2020; The Directorate of National Statistics, Ministry of Planning, Investment and Economic Development, Federal Government of Somalia: Mogadishu, Somalia, 2020. Available online: https://microdata.nbs.gov.so/index.php/catalog/50 (accessed on 14 September 2023).
- Somali Immunization Policy 2020; Ministry of Health and Human Services, Federal Government of Somalia: Mogadishu, Somalia, 2020. Available online: https://somalimedicalarchives.org/media/attachments/2021/08/29/somalia_immunization_policy-1.pdf (accessed on 12 December 2023).
- WHO Immunization Dashboard, Somalia. Available online: https://immunizationdata.who.int/pages/profiles/som.html (accessed on 2 October 2023).
- LSHTM RAISE Project. Assessing Governance, Including Decision-Making and Financing, and Delivery of Vaccines for Children in Humanitarian Settings, London School of Hygiene and Tropical Medicine. Available online: https://www.lshtm.ac.uk/research/centres-projects-groups/raise (accessed on 18 October 2023).
- Gavi, The Vaccine Alliance, Reaching Zero-Dose Children. IRMMA Framework. Available online: https://www.gavi.org/our-alliance/strategy/phase-5-2021-2025/equity-goal/zero-dose-children-missed-communities (accessed on 16 July 2023).
- Somalia National Bureau of Statistics; Federal Government of Somalia. Somali Health and Demographic Survey—Galmudug Report. 2021. Available online: https://somalia.unfpa.org/sites/default/files/pub-pdf/galmudug_report_2021_.pdf (accessed on 6 December 2023).
- Somalia National Bureau of Statistics; Federal Government of Somalia. Somali Health and Demographic Survey—Jubaland Report. 2021. Available online: https://somalia.unfpa.org/sites/default/files/pub-pdf/jlhds_report_2021_29dec_2.pdf (accessed on 6 December 2023).
- Britten, N. Qualitative Interviews. In Qualitative Research in Health Care; Pope, C., Mays, N., Eds.; Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2006; pp. 1–11. [Google Scholar] [CrossRef]
- Jenny Kitzinger, J. Focus groups. In Qualitative Research in Health Care; Pope, C., Mays, N., Eds.; Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2006; pp. 12–20. [Google Scholar] [CrossRef]
- Hogan, D.; Gupta, A. Why Reaching Zero-Dose Children Holds the Key to Achieving the Sustainable Development Goals. Vaccines 2023, 11, 781. [Google Scholar] [CrossRef] [PubMed]
- Rampin, R.; Rampin, V. Taguette: Open-source qualitative data analyses. J. Open-Source Softw. 2021, 6, 3522. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, H.; Della Rosa, F.; Russell, C.; Muiruri, F. Evaluation of Social Mobilization Network (SM Net): Final Evaluation Report; Kimetrica: Nairobi, Keyna, 2017; Available online: https://media.kimetrica.com/media/uploads/files/pdf/Kimetrica_SM_Net_Final_Evaluation_Report__final_1_August.pdf (accessed on 10 July 2023).
- Abdullahi, M.F.; Stewart, W.J.; Sahlèn, K.-G.; Bile, K.; Kinsman, J. Factors contributing to the uptake of childhood vaccination in Galkayo District, Puntland, Somalia. Glob. Health Action 2020, 13, 1803543. [Google Scholar] [CrossRef] [PubMed]
- Jama, A.A. Determinants of complete immunization coverage among children aged 11–24 months in Somalia. Int. J. Paediatr. 2020, 2020, 5827074. [Google Scholar] [CrossRef]
- Sheik-Mohamed, A.; Velema, J.P. Where health care has no access: The nomadic populations of sub-Saharan Africa. Trop. Med. Int. Health 1999, 4, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Pertet, A.M.; Kaseje, D.; Otieno-Odawa, C.F.; Kirika, L.; Wanjala, C.; Ochieng, J.; Jaoko, M.; Otieno, W.; Odindo, D. Under vaccination of children among Maasai nomadic pastoralists in Kenya: Is the issue geographic mobility, social demographics or missed opportunities? BMC Public Health. 2018, 18, 1389. [Google Scholar] [CrossRef] [PubMed]
- Gammino, V.M.; Diaz, M.R.; Pallas, S.W.; Greenleaf, A.R.; Kurnit, M.R. Health services uptake among nomadic pastoralist populations in Africa: A systematic review of the literature. PLoS Neglected Trop. Dis. 2020, 14, e0008474. [Google Scholar] [CrossRef] [PubMed]
- Dao, M.Y.; Brieger, W.R. Immunization for the migrant Fulani: Identifying an under-served population in southwestern Nigeria. Int. Q. Community Health Educ. 1994, 15, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Bomoi, I.M.; Waziri, N.E.; Nguku, P.; Tsofo, A. Integrated human and animal vaccination delivery to Nomadic Fulani communities in Northern Nigeria 2015. Int. J. Infect. Dis. 2016, 45, 22. [Google Scholar] [CrossRef]
- Kamadjeu, R.; Mulugeta, A.; Gupta, D.; Hirsi, A.A.; Belayneh, A.; Clark-Hattingh, M.; Adams, C.; Abed, P.; Kyeyune, B.; Ahmed, T.; et al. Immunizing nomadic children and livestock—Experience in North East Zone of Somalia. Hum. Vaccine Immunother. 2015, 11, 2637–2639. [Google Scholar] [CrossRef] [PubMed]
- Schelling, E.; Bechir, M.; Ahmed, M.A.; Wyss, K.; Randolph, T.F.; Zinsstag, J. Human and Animal Vaccination Delivery to Remote Nomadic Families, Chad. Emerg. Infect. Dis. 2007, 13, 373–379. [Google Scholar] [CrossRef] [PubMed]
- IOM. Displacement in Somalia Reaches Record High 3.8 Million. 2023. Available online: https://www.iom.int/news/displacement-somalia-reaches-record-high-38-million-iom-deputy-director-general-calls-sustainable-solutions (accessed on 30 September 2023).
- Jelle, M.; Seal, A.J.; Mohamed, H.; Mohamed, H.; Omar, M.S.; Mohamed, S.; Mohamed, A.; Morrison, J. Understanding multilevel barriers to childhood vaccination uptake among Internally Displaced Populations (IDPs) in Mogadishu, Somalia: A qualitative study. BMC Public Health 2023, 23, 2018. [Google Scholar] [CrossRef]
- Sheffel, A.; Karp, C.; Creanga, A.A. Use of Service Provision Assessments and Service Availability and Readiness Assessments for monitoring quality of maternal and newborn health services in low-income and middle-income countries. BMJ Glob. Health 2018, 3, e001011. [Google Scholar] [CrossRef]
- Majid, N.; Jelle, M.; Adan, G.; Daar, A.; Abdirahman, K.; Hailey, P.; Balfour, N.; Seal, A.; Maxwell, D. Another Humanitarian (and Political) Crisis in Somalia in 2022; Feinstein International Center, Tufts University: Boston, MA, USA, 2022; Available online: https://fic.tufts.edu/publication-item/another-humanitarian-and-political-crisis-in-somalia-in-2022/ (accessed on 10 August 2023).
- Ameyaw, E.K.; Kareem, Y.O.; Ahinkorah, B.O.; Seidu, A.-A.; Yaya, S. Decomposing the rural-urban gap in factors associated with childhood immunisation in sub-Saharan Africa: Evidence from surveys in 23 countries. BMJ Global Health 2021, 6, e003773. [Google Scholar] [CrossRef]
- Ngo, N.V.; Pemunta, N.V.; Muluh, N.E.; Adedze, M.; Basil, N.; Agwale, S. Armed conflict, a neglected determinant of childhood vaccination: Some children are left behind. Hum. Vaccines Immunother. 2020, 16, 1454–1463. [Google Scholar] [CrossRef]
- Ali, H.A.; Hartner, A.M.; Echeverria-Londono, S.; Roth, J.; Li, X.; Abbas, K.; Portnoy, A.; Vynnycky, E.; Woodruff, K.; Ferguson, N.M.; et al. Vaccine equity in low- and middle-income countries: A systematic review and meta-analysis. Int. J. Equity Health 2022, 21, 82. [Google Scholar] [CrossRef]
- Wendt, A.; Santos, T.M.; Cata-Preta, B.O.; Costa, J.C.; Mengistu, T.; Hogan, D.R.; Victora, C.G.; Barros, A.J.D. Children of more empowered women are less likely to be left without vaccination in low- and middle-income countries: A global analysis of 50 DHS surveys. J. Glob. Health 2022, 12, 04022. [Google Scholar] [CrossRef] [PubMed]
- Johns, N.E.; Hosseinpoor, A.R.; Chisema, M.; Danovaro-Holliday, M.C.; Kirkby, K.; Schlotheuber, A.; Shibeshi, M.; Sodha, S.V.; Zimba, B. Association between childhood immunisation coverage and proximity to health facilities in rural settings: A cross-sectional analysis of Service Provision Assessment 2013–2014 facility data and Demographic and Health Survey 2015–2016 individual data in Malawi. BMJ Open 2022, 12, e061346. [Google Scholar] [CrossRef] [PubMed]
- Hayir, T.M.M.; Magan, M.A.; Mohamed, L.M.; Mohamud, M.A.; Muse, A.A. Barriers for full immunization coverage among under 5 years children in Mogadishu, Somalia. J. Fam. Med. Prim. Care 2020, 9, 2664. [Google Scholar] [CrossRef] [PubMed]
- Ikilezi, G.; Augusto, O.J.; Sbarra, A.; Sherr, K.; Dieleman, J.L.; Lim, S.S. Determinants of geographical inequalities for DTP3 vaccine coverage in sub-Saharan Africa. Vaccine 2020, 16, 3447–3454. [Google Scholar] [CrossRef] [PubMed]
- Cherian, T.; Mantel, C. National immunization programmes. Bundesgesundheitsbl 2020, 63, 16–24. [Google Scholar] [CrossRef] [PubMed]
- The Essential Package of Health Services 2020 (EPHS); The Ministry of Health and Human Services, Federal Government of Somalia: Mogadishu, Somalia, 2020. Available online: https://reliefweb.int/report/somalia/essential-package-health-services-ephs-somalia-2020 (accessed on 20 July 2023).


{kind=link}
| Step | Description |
|---|---|
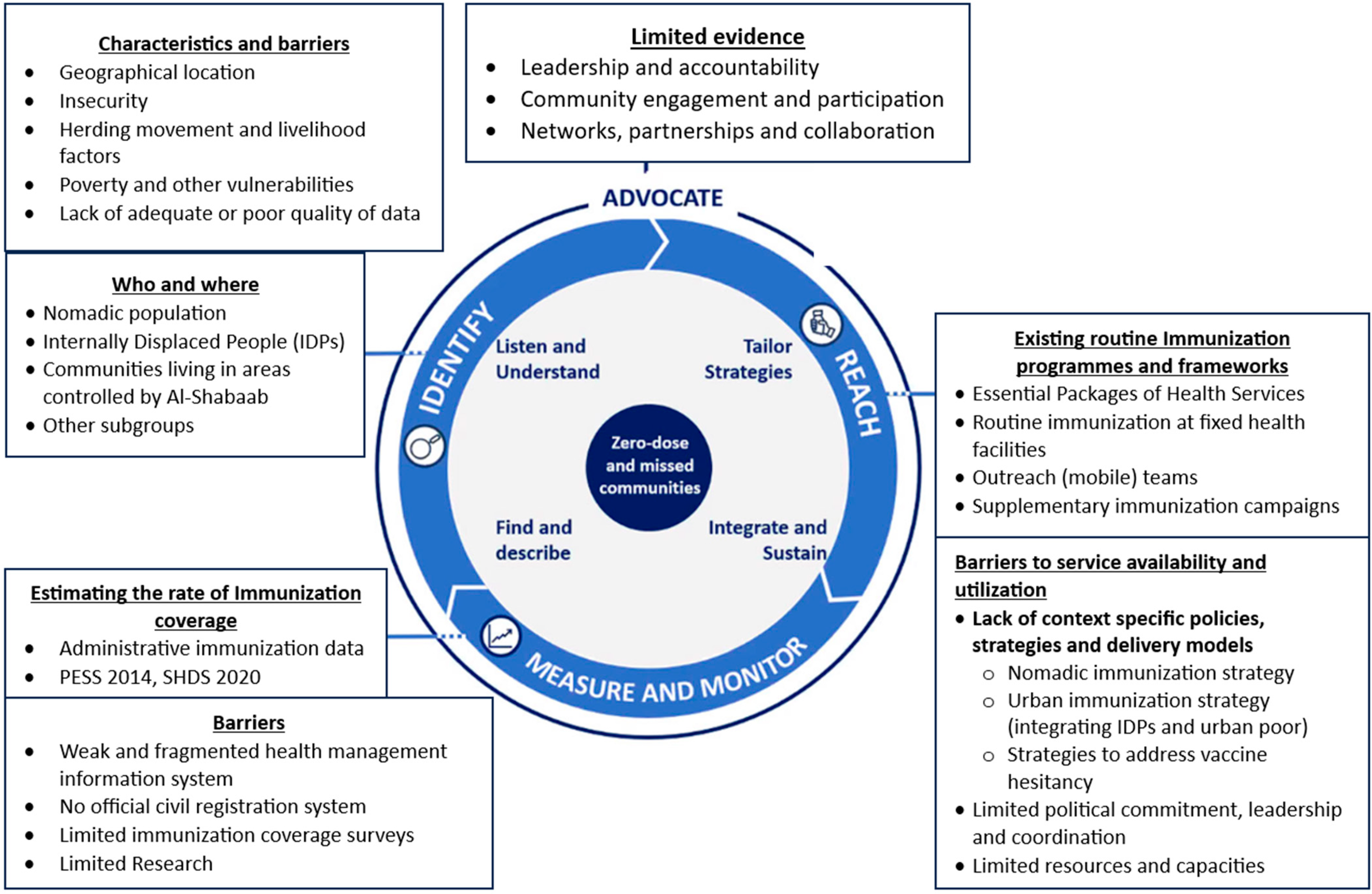
| Identify | This first step describes the strategies and methods to gain a “clear understanding of which, where, why, and how many zero-dose children and missed communities have not been reached”, including how they were identified (data sources) and the barriers that prevent these children from getting vaccinated [17]. |
| Reach | The second step outlines the whole health system and primary healthcare approaches that countries can adopt, using a wide range of data and evidence, to design context-specific, tailored and sustainable delivery strategies and models which address the main barriers to service availability and service utilization for zero-dose and under-immunized children. |
| Monitor/Measure | The third and fourth steps describe the importance of effective monitoring and evaluation mechanisms to track and review progress in a timely manner and gain a better understanding of the extent to which the strategies and programmes are implemented in order to enable learning, course corrections and validation of the integrity of the implementation. |
| Advocate | The fifth step sets out approaches that governments can raise the profile of immunization, engage with affected communities and establish strong networks and partnerships in order to mobilize and prioritize resources towards zero-dose children and missed communities. |
| Variables | Number (n) | Percentage | ||
|---|---|---|---|---|
| Age Groups | 19–29 | 5 | 29% | |
| 30–40 | 10 | 59% | ||
| 40+ | 2 | 12% | ||
| Gender | Male | 17 | 100% | |
| Female | 0 | 0% | ||
| Agency | Federal MoH | 3 | 18% | |
| State MoH | Puntland | 3 | 18% | |
| Galmudug | 2 | 12% | ||
| Jubbaland | 3 | 18% | ||
| UNICEF | 1 | 6% | ||
| INGOs | 3 | 18% | ||
| Local NGO | 2 | 12% | ||
| MoH Level | Vaccinators | Community | Total FGD |
|---|---|---|---|
| Puntland | 1 (2 male, 9 female) | 0 | 1 (11) |
| Galmudug | 1 (3 male, 9 female) | 1 (2 male, 6 female) | 2 (20) |
| Jubaland | 1 (1 male, 11 female) | 1 (1 male, 8 female) | 2 (21) |
| Total | 3 (6 male, 29 female) | 2 (3 male, 14 female) | 5 (52) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bile, A.S.; Ali-Salad, M.A.; Mahmoud, A.J.; Singh, N.S.; Abdelmagid, N.; Sabahelzain, M.M.; Checchi, F.; Mounier-Jack, S.; Nor, B. Assessing Vaccination Delivery Strategies for Zero-Dose and Under-Immunized Children in the Fragile Context of Somalia. Vaccines 2024, 12, 154. https://doi.org/10.3390/vaccines12020154
Bile AS, Ali-Salad MA, Mahmoud AJ, Singh NS, Abdelmagid N, Sabahelzain MM, Checchi F, Mounier-Jack S, Nor B. Assessing Vaccination Delivery Strategies for Zero-Dose and Under-Immunized Children in the Fragile Context of Somalia. Vaccines. 2024; 12(2):154. https://doi.org/10.3390/vaccines12020154
Chicago/Turabian StyleBile, Ahmed Said, Mohamed A. Ali-Salad, Amina J. Mahmoud, Neha S. Singh, Nada Abdelmagid, Majdi M. Sabahelzain, Francesco Checchi, Sandra Mounier-Jack, and Barni Nor. 2024. "Assessing Vaccination Delivery Strategies for Zero-Dose and Under-Immunized Children in the Fragile Context of Somalia" Vaccines 12, no. 2: 154. https://doi.org/10.3390/vaccines12020154