
Waning of SARS-CoV-2 Vaccine Effectiveness in COPD Patients: Lessons from the Delta Variant
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Definitions
2.2. Statistical Analysis
3. Results
3.1. Patient and Population Characteristics
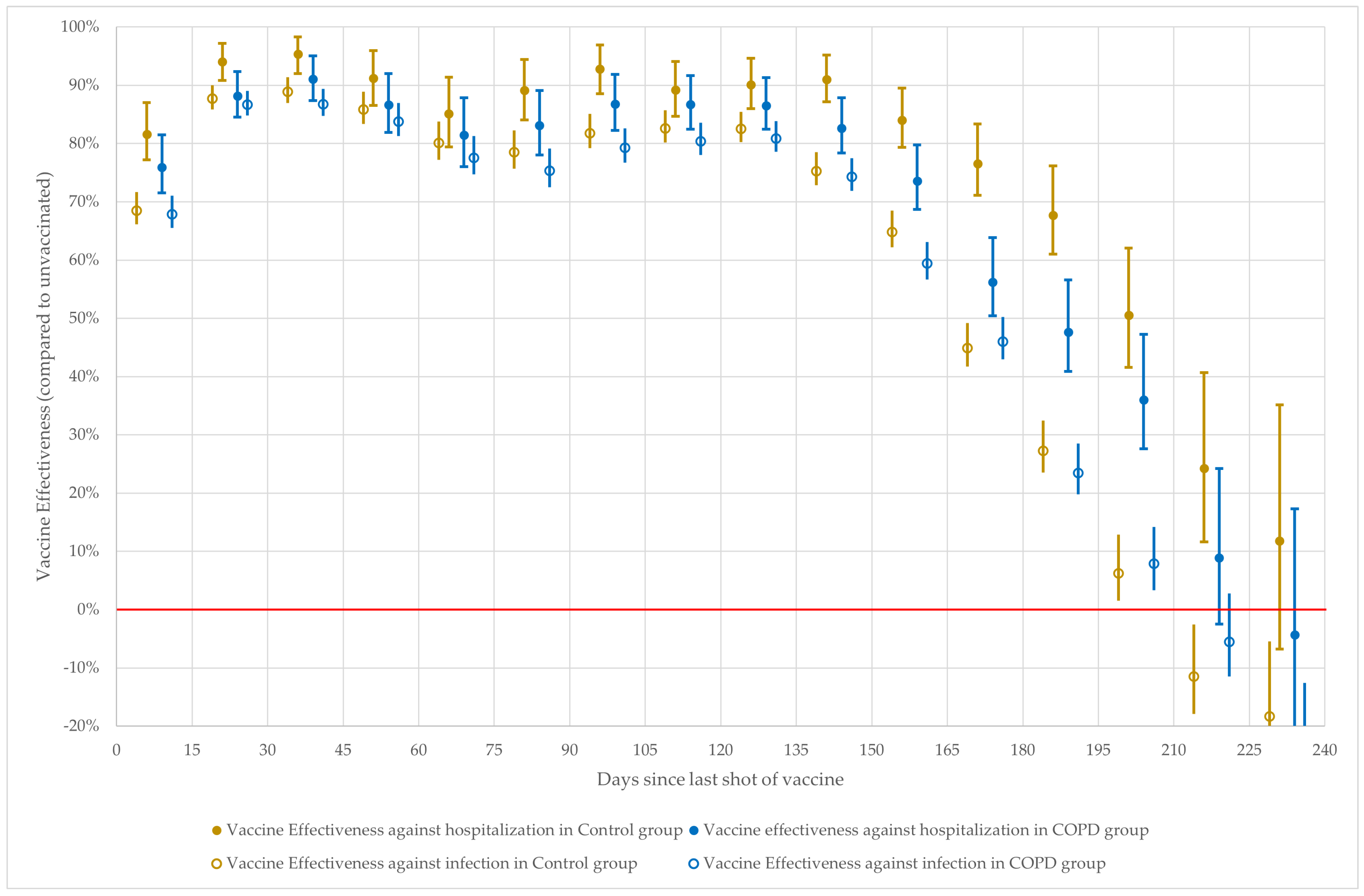
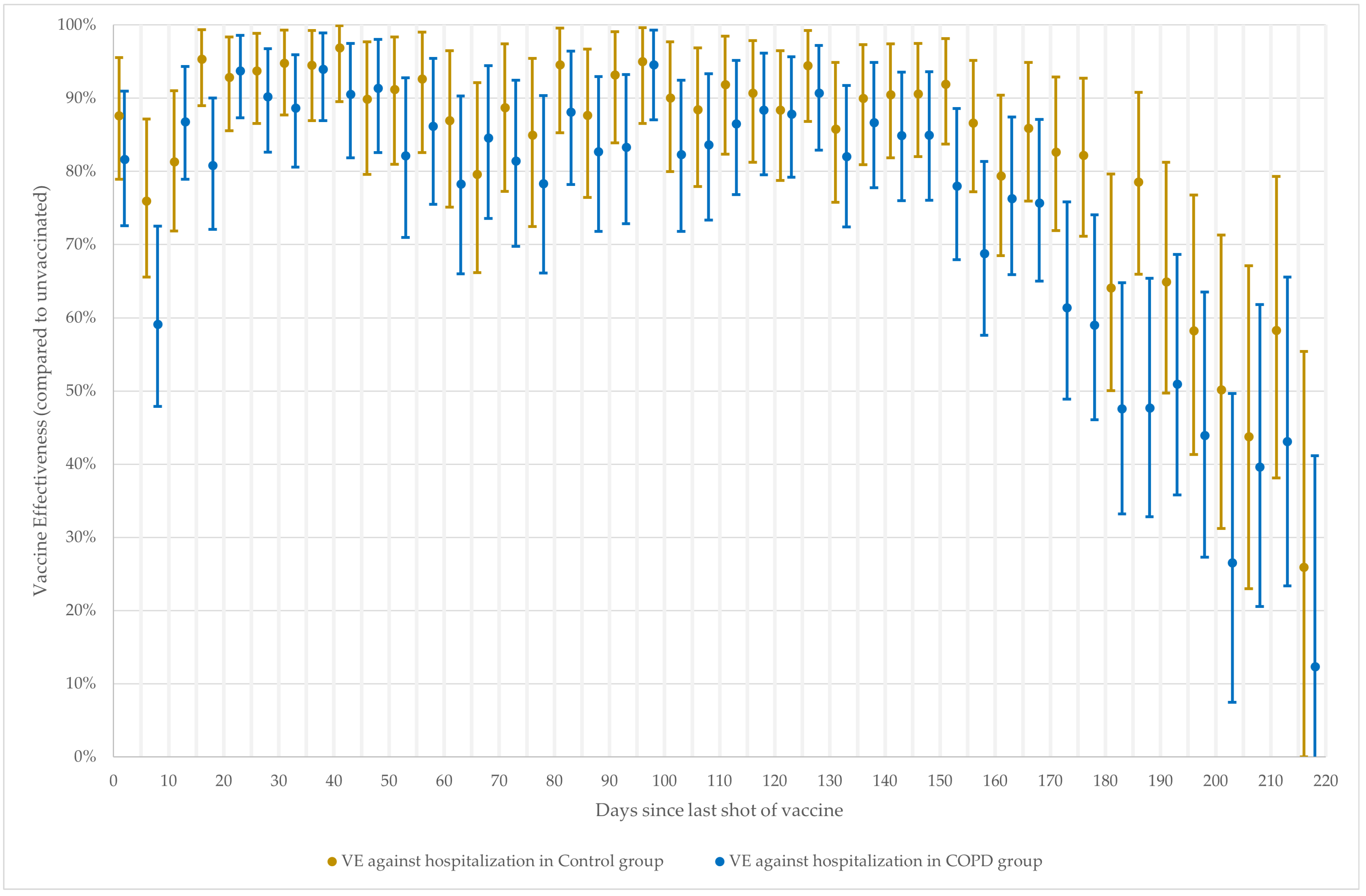
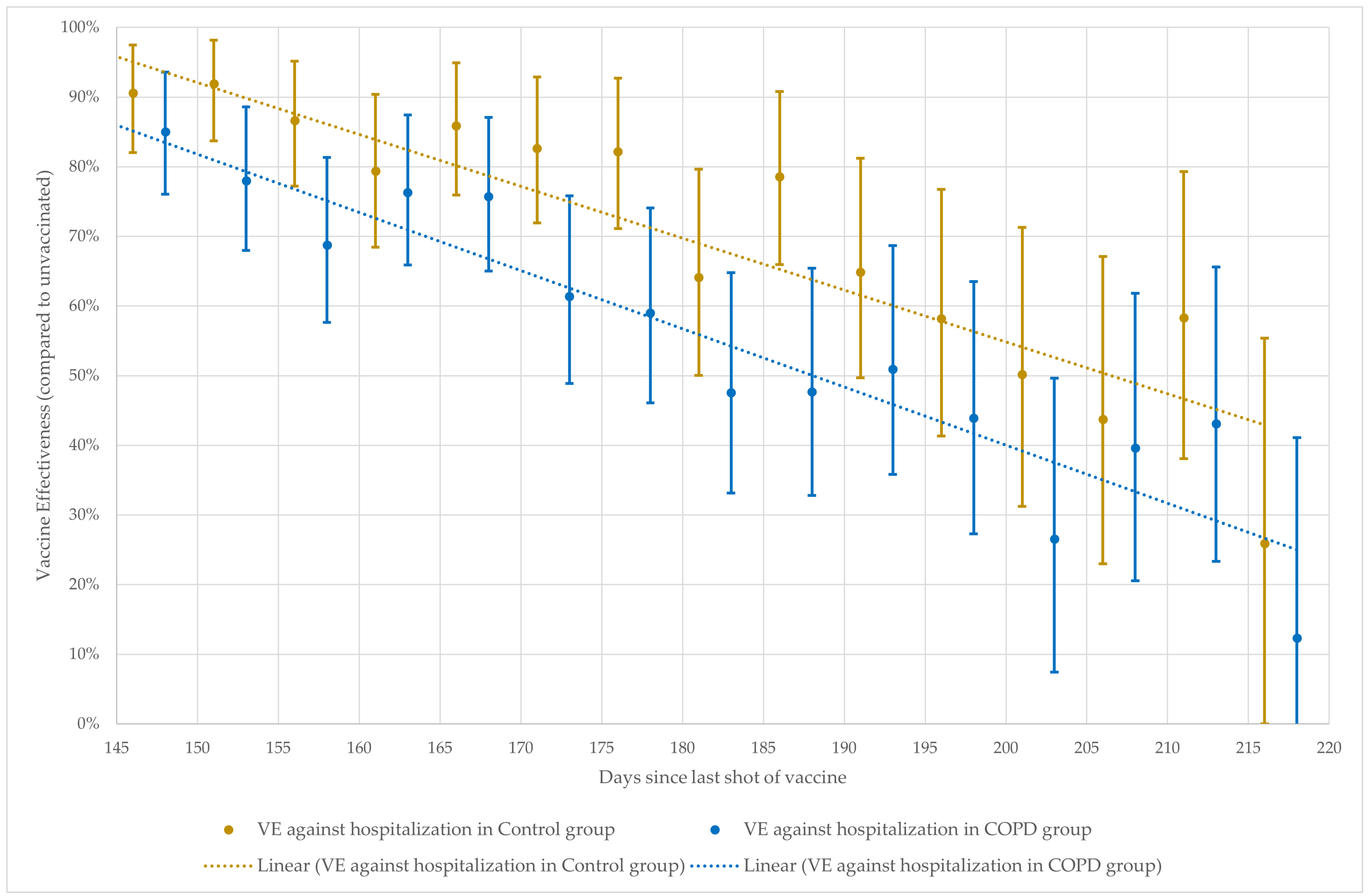
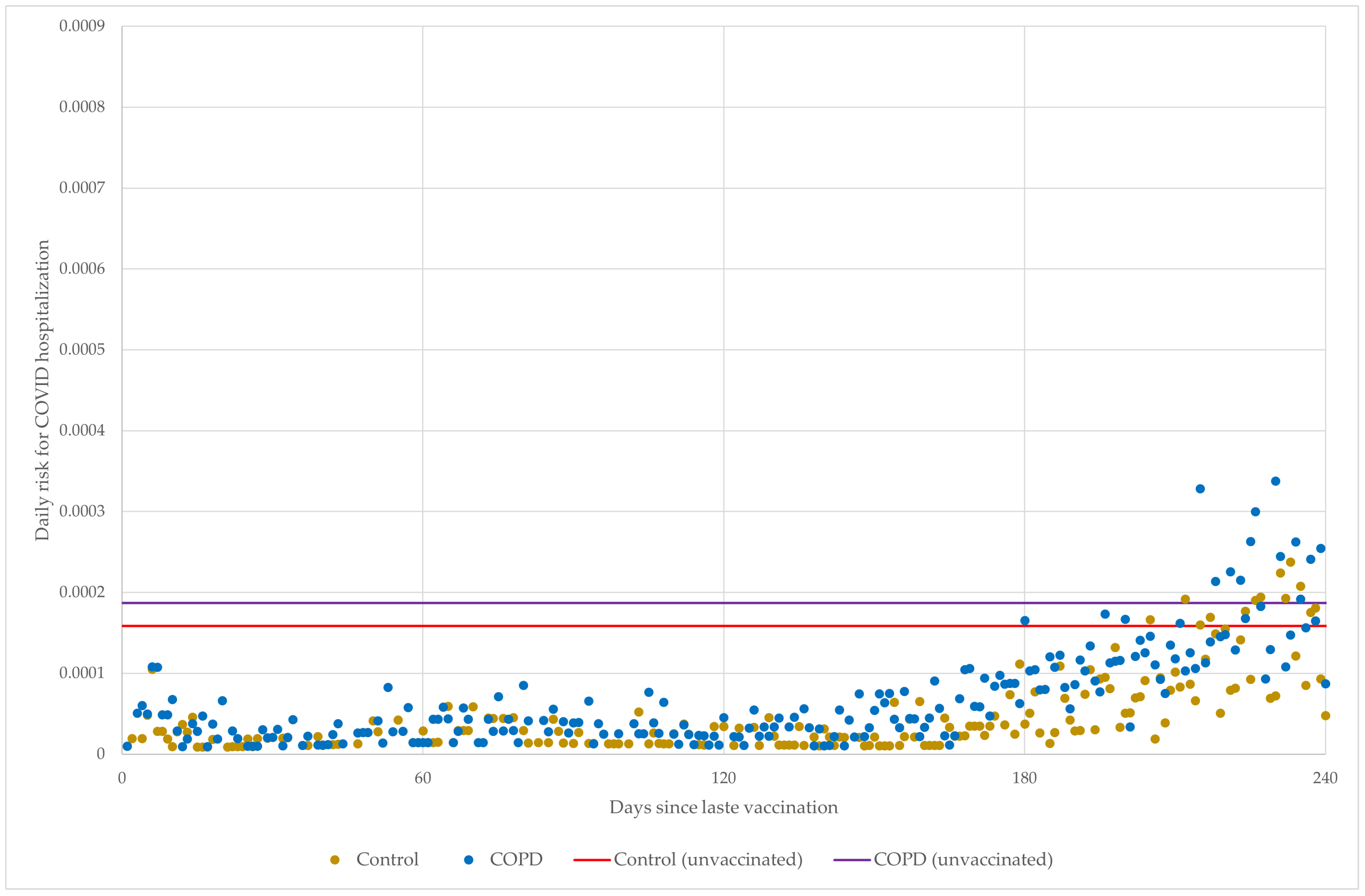
3.2. Assessment of Vaccine Effectiveness throughout the Delta VOC Wave
4. Discussion
4.1. Interpretation
4.2. Limitations and Special Approach
4.3. Use for the Results of the Study after the End of the Pandemic
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| COPD | Chronic obstructive pulmonary disease |
| VE | Vaccine effectiveness |
| VOC | Variant of concern |
| CI | Confidence interval |
| HR | Hazard ratio |
| mRNA | messenger ribonucleic acid |
| CDC | Center for Disease Control and Prevention |
| GOLD | Global Initiative for Chronic Obstructive Lung Disease |
| ICD-10 | International Classification of Diseases 10th Revision |
| NPHC | National Public Health Center of Hungary |
| SD | Standard deviation |
Appendix A


References
- Hall, E.; Wodi, P.A.; Hamborsky, J.; Morelli, V.; Schillie, S. Epidemiology and Prevention of Vaccine-Preventable Diseases; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Vokó, Z.; Kiss, Z.; Surján, G.; Surján, O.; Barcza, Z.; Wittmann, I.; Molnár, G.A.; Nagy, D.; Müller, V.; Bogos, K. Effectiveness and Waning of Protection with Different Sars-Cov-2 Primary and Booster Vaccines During the Delta Pandemic Wave in 2021 in Hungary (Hun-Ve 3 Study). Front. Immunol. 2022, 13, 919408. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, B.; Nuwarda, R.F.; Ramzan, I.; Kayser, V. A Narrative Review of Covid-19 Vaccines. Vaccines 2022, 10, 62. [Google Scholar] [CrossRef]
- Chen, X.; Huang, H.; Ju, J.; Sun, R.; Zhang, J. Impact of Vaccination on the Covid-19 Pandemic in Us States. Sci. Rep. 2022, 12, 1554. [Google Scholar] [CrossRef]
- WHO Official Site. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-unga-unsg-hosted-event---ending-the-pandemic-through-equitable-access-to-covid-19-vaccines--tests-and-treatments----23-september-2022 (accessed on 26 September 2023).
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H.; Bae, A.; Sin, D.D. Copd and the Risk of Poor Outcomes in Covid-19: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 33, 100789. [Google Scholar] [CrossRef] [PubMed]
- Valipour, A.; Aisanov, Z.; Avdeev, S.; Koblizek, V.; Kocan, I.; Kopitovic, I.; Lupkovics, G.; Man, M.; Bukovskis, M.; Tudoric, N. Recommendations for Copd Management in Central and Eastern Europe. Expert Rev. Respir. Med. 2022, 16, 221–234. [Google Scholar] [CrossRef]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: Gold Executive Summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- CDC Official Site. Available online: www.cdc.gov/vaccines/adults/rec-vac/health-conditions/lung-disease.html (accessed on 26 September 2023).
- Reyes, F.M.; Hache-Marliere, M.; Karamanis, D.; Berto, C.G.; Estrada, R.; Langston, M.; Ntaios, G.; Gulani, P.; Shah, C.D.; Palaiodimos, L. Assessment of the Association of Copd and Asthma with in-Hospital Mortality in Patients with Covid-19. A Systematic Review, Meta-Analysis, and Meta-Regression Analysis. J. Clin. Med. 2021, 10, 2087. [Google Scholar] [CrossRef]
- Gold 2022 Key Changes Summary. Available online: https://goldcopd.org/wp-content/uploads/2021/11/GOLD-2022-KEY-CHANGES-SUMMARY-4Nov2021.pdf (accessed on 26 September 2023).
- Simon, S.; Joean, O.; Welte, T.; Rademacher, J. The Role of Vaccination in Copd: Influenza, Sars-Cov-2, Pneumococcus, Pertussis, Rsv and Varicella Zoster Virus. Eur. Respir. Rev. 2023, 32, 230034. [Google Scholar] [CrossRef]
- Vokó, Z.; Kiss, Z.; Surján, G.; Surján, O.; Barcza, Z.; Pályi, B.; Formanek-Balku, E.; Molnár, G.A.; Herczeg, R.; Gyenesei, A. Nationwide Effectiveness of Five Sars-Cov-2 Vaccines in Hungary—the Hun-Ve Study. Clin. Microbiol. Infect. 2022, 28, 398–404. [Google Scholar] [CrossRef]
- Müller, V.; Polivka, L.; Valyi-Nagy, I.; Nagy, A.; Szekanecz, Z.; Bogos, K.; Vago, H.; Kamondi, A.; Fekete, F.; Szlavik, J. Booster Vaccination Decreases 28-Day All-Cause Mortality of the Elderly Hospitalized Due to Sars-Cov-2 Delta Variant. Vaccines 2022, 10, 986. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J. Scipy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- Graziani, D.; Soriano, J.; Morena, C.D.D.; DíAz, T.; Castillo, M.; Alonso, M.; Ancochea, J.; Lumbreras, S.; Izquierdo, J.L. Characteristics and Prognosis of Covid-19 in Patients with Copd. J. Clin. Med. 2020, 9, 3259. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T. Age and Smoking Predict Antibody Titres at 3 Months after the Second Dose of the Bnt162b2 Covid-19 Vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef] [PubMed]
- Fowlkes, A.; Gaglani, M.; Groover, K.; Thiese, M.S.; Tyner, H.; Ellingson, K.; HEROES-RECOVER Cohorts. Effectiveness of Covid-19 Vaccines in Preventing Sars-Cov-2 Infection among Frontline Workers before and During B. 1.617. 2 (Delta) Variant Predominance—Eight Us Locations, December 2020–August 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1167. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Baz, I.; Miqueleiz, A.; Casado, I.; Navascués, A.; Trobajo-Sanmartín, C.; Burgui, C.; Guevara, M.; Ezpeleta, C.; Castilla, J. Effectiveness of Covid-19 Vaccines in Preventing Sars-Cov-2 Infection and Hospitalisation, Navarre, Spain, January to April 2021. Eurosurveillance 2021, 26, 2100438. [Google Scholar] [CrossRef] [PubMed]
- Suah, J.L.; Husin, M.; Tok, P.S.K.; Tng, B.H.; Thevananthan, T.; Low, E.V.; Appannan, M.R.; Zin, F.M.; Zin, S.M.; Yahaya, H. Waning Covid-19 Vaccine Effectiveness for Bnt162b2 and Coronavac in Malaysia: An Observational Study. Int. J. Infect. Dis. 2022, 119, 69–76. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of Infection, Hospitalisation, and Death up to 9 Months after a Second Dose of Covid-19 Vaccine: A Retrospective, Total Population Cohort Study in Sweden. Lancet 2022, 399, 814–823. [Google Scholar] [CrossRef]
- Southworth, T.; Jackson, N.; Singh, D. Airway Immune Responses to Covid-19 Vaccination in Copd Patients and Healthy Subjects. Eur. Respir. J. 2022, 60, 2200497. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Protocol for a COVID-19 Vaccine Effectiveness Study Using Health Data Registries; ECDC: Stockholm, Sweden, 2023. [Google Scholar]
- Nainu, F.; Abidin, R.S.; Bahar, M.A.; Frediansyah, A.; Emran, T.B.; Rabaan, A.A.; Dhama, K.; Harapan, H. Sars-Cov-2 Reinfection and Implications for Vaccine Development. Hum. Vaccines Immunother. 2020, 16, 3061–3073. [Google Scholar] [CrossRef]
- Trombetta, C.M.; Kistner, O.; Montomoli, E.; Viviani, S.; Marchi, S. Influenza Viruses and Vaccines: The Role of Vaccine Effectiveness Studies for Evaluation of the Benefits of Influenza Vaccines. Vaccines 2022, 10, 714. [Google Scholar] [CrossRef]
- World Health Organization. Evaluation of Covid-19 Vaccine Effectiveness in a Changing Landscape of Covid-19 Epidemiology and Vaccination: Interim Guidance, 1 October 2022: Second Addendum to Evaluation of Covid-19 Vaccine Effectiveness: Interim Guidance; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y. A Bivalent Omicron-Containing Booster Vaccine against Covid-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Matched Control | COPD | |
|---|---|---|
| Sex | ||
| Female | 97,530 (52.2%) | 97,530 (52.2%) |
| Male | 89,451 (47.8%) | 89,451 (47.8%) |
| Age (years) average ± SD | 66.73 ± 12.67 * | 66.67 ± 12.66 * |
| Comorbidities | ||
| Heart failure | 18,485 (9.9%) | 18,485 (9.9%) |
| Acute myocardial infarct | 2219 (1.2%) | 2219 (1.2%) |
| Peripheral vascular disease | 22,108 (11.8%) | 22,108 (11.8%) |
| History of angina pectoris | 27,545 (14.7%) | 27,545 (14.7%) |
| History of stroke | 15,426 (8.3%) | 15,426 (8.3%) |
| Type 2 diabetes mellitus | 43,872 (23.5%) | 43,872 (23.5%) |
| Type 1 diabetes mellitus | 126 (0.1%) | 126 (0.1%) |
| Any malignancy | 28,249 (15.1%) | 28,249 (15.1%) |
| Immunosuppressed state | 12,198 (6.5%) | 12,198 (6.5%) |
| Chronic kidney disease | 10,356 (5.5%) | 10,356 (5.5%) |
| Immune status | ||
| Unvaccinated | 38,017 (20.3%) | 38,017 (20.3%) |
| Primary vaccination | 119,676 (64%) | 119,676 (64%) |
| Boost vaccination | 15,705 (8.4%) | 15,705 (8.4%) |
| Prior infection | 13,583 (7.3%) | 13,583 (7.3%) |
| Matched Control | COPD | p | |
|---|---|---|---|
| n = 186,981 | n = 186,981 | ||
| Infected | 7398 (4.0%) | 8025 (4.3%) | <0.001 |
| Unvaccinated | 2991 (40.4%) | 3095 (38.6%) | |
| Primary vaccinated | 3580 (48.4%) | 3921 (48.9%) | 0.031 |
| Boost vaccinated | 684 (9.2%) | 817 (10.2%) | |
| Had prior infection | 143 (1.9%) | 192 (2.4%) | 0.050 |
| Hospitalized (COVID-19 hospitalization) | 1278 (0.7%) | 1842 (1.0%) | <0.001 |
| Unvaccinated | 726 (56.8%) | 844 (45.8%) | |
| Primary vaccinated | 456 (35.7%) | 825 (44.8%) | <0.001 |
| Boost vaccinated | 88 (6.9%) | 152 (8.3%) | |
| Had prior infection | 8 (0.6%) | 21 (1.1%) | 0.141 |
| Primary Vaccinated | Boost Vaccinated | |||
|---|---|---|---|---|
| Matched Control | COPD | Matched Control | COPD | |
| VE against Infection | 46.78% | 45.58% | 86.11% | 83.6% |
| [43.48–49.94%] | [42.30–48.74%] | [84.65–87.50%] | [82.02–85.10%] | |
| VE against COVID-19 | 72.07% | 58.01% | 92.64% | 88.81% |
| Hospitalization | [67.51–76.22%] | [52.59–63.01%] | [90.45–94.54%] | [86.30–91.06%] |
| Average No. days since last vaccination at censoring time | 240.67 ± 57.82 | 239.06 ± 59.79 | 69.3 ± 45.16 | 69.89 ± 45.74 |
| Matched Control | COPD | |
|---|---|---|
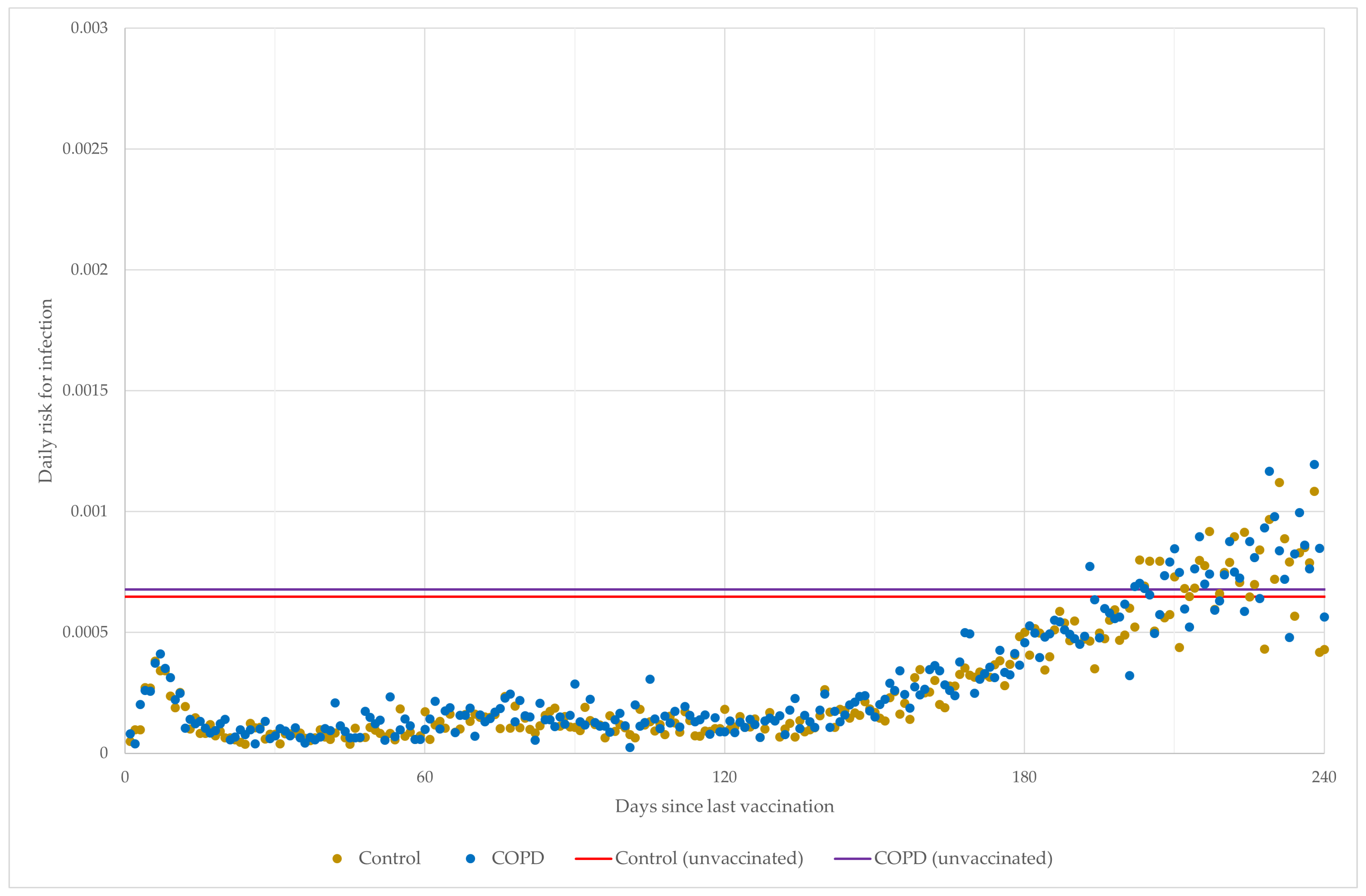
| Daily risk for infection | 64.71 [61.36–67.16]/100,000 | 67.73 [64.25–70.28]/100,000 |
| Daily risk for COVID-19 hospitalization | 15.84 [14.2–17.07]/100,000 | 18.66 [16.86–20.02]/100,000 |
| Infection | COVID-19 Hospitalization | |||
|---|---|---|---|---|
| HR | p | HR | p | |
| mRNA vaccine | 0.66 [0.619–0.703] | <0.001 | 0.809 [0.68–0.962] | 0.017 |
| Group COPD | 1.073 [1.008–1.142] | 0.028 | 1.867 [1.592–2.190] | <0.001 |
| Interaction | 1.034 [0.953–1.123] | 0.420 | 0.889 [0.724–1.093] | 0.266 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polivka, L.; Valyi-Nagy, I.; Szekanecz, Z.; Bogos, K.; Vago, H.; Kamondi, A.; Fekete, F.; Szlavik, J.; Surjan, G.; Surjan, O.; et al. Waning of SARS-CoV-2 Vaccine Effectiveness in COPD Patients: Lessons from the Delta Variant. Vaccines 2023, 11, 1786. https://doi.org/10.3390/vaccines11121786
Polivka L, Valyi-Nagy I, Szekanecz Z, Bogos K, Vago H, Kamondi A, Fekete F, Szlavik J, Surjan G, Surjan O, et al. Waning of SARS-CoV-2 Vaccine Effectiveness in COPD Patients: Lessons from the Delta Variant. Vaccines. 2023; 11(12):1786. https://doi.org/10.3390/vaccines11121786
Chicago/Turabian StylePolivka, Lörinc, Istvan Valyi-Nagy, Zoltan Szekanecz, Krisztina Bogos, Hajnalka Vago, Anita Kamondi, Ferenc Fekete, Janos Szlavik, György Surjan, Orsolya Surjan, and et al. 2023. "Waning of SARS-CoV-2 Vaccine Effectiveness in COPD Patients: Lessons from the Delta Variant" Vaccines 11, no. 12: 1786. https://doi.org/10.3390/vaccines11121786