
Orogenital Human Papillomavirus Infection and Vaccines: A Survey of High- and Low-Risk Genotypes Not Included in Vaccines

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Samples Collection
2.2. Samples Processing and HPV-DNA Extraction, Detection and Genotyping
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caltabiano, M.; Castiglioni, M.; De-Rose, A. Changes in the sexual behaviour of young people: Introduction. Genus 2020, 76, 38. [Google Scholar] [CrossRef]
- Candotto, V.; Lauritano, D.; Nardone, M.; Baggi, L.; Arcuri, C.; Gatto, R.; Gaudio, R.M.; Spadari, F.; Carinci, F. HPV Infection in the Oral Cavity: Epidemiology, Clinical Manifestations and Relationship with Oral Cancer. Oral Implantol. 2017, 10, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Fatone, L.; Montenegro, V.; De Vito, D.; Pettini, F.; Crincoli, V.; Antelmi, A.; Romita, P.; Rapone, B.; et al. Transmission of Nonviral Sexually Transmitted Infections and Oral Sex. J. Sex. Med. 2012, 9, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Herbenick, D.; Bowling, J.; Fu, T.-C.; Dodge, B.; Guerra-Reyes, L.; Sanders, S. Sexual diversity in the United States: Results from a nationally representative probability sample of adult women and men. PLoS ONE 2017, 12, e0181198. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.; Clark, A.; Sherman, C.; Heitzeg, M.M.; Hicks, B.M. Age, sex, and other demographic trends in sexual behavior in the United States: Initial findings of the sexual behaviors, internet use, and psychological adjustment survey. PLoS ONE 2021, 16, e0255371. [Google Scholar] [CrossRef] [PubMed]
- CENSIS. Rapporto Censis-Bayer Sui Nuovi Comportamenti Sessuali Degli Italiani n.d. Available online: https://www.censis.it/welfare-e-salute/il-sesso-degli-italiani-più-frequente-più-vario-con-più-partner (accessed on 9 May 2023).
- Queirós, C.; Borges, J. Oral Transmission of Sexually Transmissable Infections: A Narrative Review. Acta Med. Port. 2019, 32, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Fasciana, T.; Capra, G.; Di Carlo, P.; Calà, C.; Vella, M.; Pistone, G.; Colomba, C.; Giammanco, A. Socio-Demographic Characteristics and Sexual Behavioral Factors of Patients with Sexually Transmitted Infections Attending a Hospital in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 4722. [Google Scholar] [CrossRef] [PubMed]
- Fasciana, T.; Capra, G.; Lipari, D.; Firenze, A.; Giammanco, A. Sexually Transmitted Diseases: Diagnosis and Control. Int. J. Environ. Res. Public Health 2022, 19, 5293. [Google Scholar] [CrossRef]
- Kombe, A.J.K.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.-A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front. Public Health 2021, 8, 552028. [Google Scholar] [CrossRef]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The Estimated Lifetime Probability of Acquiring Human Papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Radley, D.; Saah, A.; Stanley, M. Persistent infection with human papillomavirus 16 or 18 is strongly linked with high-grade cervical disease. Hum. Vaccines Immunother. 2015, 12, 768–772. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Monographs on the Evaluation of Carcinogenic Risks to Humans. In Some Antineoplastic and Immunosuppressive Agents; Biological Agents, Human Papillomaviruses; International Agency for Research on Cancer (IARC): Lyon, France, 1998; Volume 100B, pp. 255–295. [Google Scholar]
- Capra, G.; Notari, T.; Buttà, M.; Serra, N.; Rizzo, G.; Bosco, L. Human Papillomavirus (HPV) Infection and Its Impact on Male Infertility. Life 2022, 12, 1919. [Google Scholar] [CrossRef] [PubMed]
- Javier, R.T.; Butel, J.S. The History of Tumor Virology. Cancer Res. 2008, 68, 7693–7706. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 92. [Google Scholar] [CrossRef]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K. Beyond Cervical Cancer: Burden of Other HPV-Related Cancers Among Men and Women. J. Adolesc. Health 2010, 46, S20–S26. [Google Scholar] [CrossRef]
- Vidotti, L.R.; Vidal, F.C.B.; Monteiro, S.C.M.; Nunes, J.D.; Salgado, J.V.; Brito, L.M.O.; Lopes, F.F. Association between oral DNA-HPV and genital DNA-HPV. J. Oral Pathol. Med. 2014, 43, 289–292. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). Cancers Associated with Human Papillomavirus, United States—2015–2019; UCSC Data Br; Centers for Disease Control and Prevention; US Department of Health and Human Services: Atlanta, GA, USA, 2022; p. 32.
- Syrjanen, S.; Termine, N.; Capra, G.; Paderni, C.; Panzarella, V.; Campisi, G. Oral HPV Infection: Current Strategies for Prevention and Therapy. Curr. Pharm. Des. 2012, 18, 5452–5469. [Google Scholar] [CrossRef]
- Wierzbicka, M.; Giorgi, M.R.M.S.; Dikkers, F.G. Transmission and clearance of human papillomavirus infection in the oral cavity and its role in oropharyngeal carcinoma—A review. Rev. Med. Virol. 2022, 33, e2337. [Google Scholar] [CrossRef]
- Oliveira, L.H.S.; Santos, L.S.; Silva, C.O.; Augusto, E.F.; Neves, F.P.G. Papillomavirus infections in the oral and genital mucosa of asymptomatic women. Braz. J. Infect. Dis. 2017, 21, 88–91. [Google Scholar] [CrossRef]
- Wierzbicka, M.; Klussmann, J.P.; Giorgi, M.R.S.; Wuerdemann, N.; Dikkers, F.G. Oral and laryngeal HPV infection: Incidence, prevalence and risk factors, with special regard to concurrent infection in head, neck and genitals. Vaccine 2021, 39, 2344–2350. [Google Scholar] [CrossRef] [PubMed]
- Sias, C.; Salichos, L.; Lapa, D.; Del Nonno, F.; Baiocchini, A.; Capobianchi, M.R.; Garbuglia, A.R. Alpha, Beta, gamma human PapillomaViruses (HPV) detection with a different sets of primers in oropharyngeal swabs, anal and cervical samples. Virol. J. 2019, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Perino, A.; Consiglio, P.; Maranto, M.; De Franciscis, P.; Marci, R.; Restivo, V.; Manzone, M.; Capra, G.; Cucinella, G.; Calagna, G. Impact of a new carrageenan-based vaginal microbicide in a female population with genital HPV-infection: First experimental results. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 6744–6752. [Google Scholar] [CrossRef] [PubMed]
- Calagna, G.; Maranto, M.; Paola, C.; Capra, G.; Perino, A.; Chiantera, V.; Cucinella, G. ‘Secondary prevention’ against female HPV infection: Literature review of the role of carrageenan. Expert Rev. Anti Infect. Ther. 2020, 18, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Capra, G.; Giovannelli, L.; Matranga, D.; Bellavia, C.; Guarneri, M.F.; Fasciana, T.; Scaduto, G.; Firenze, A.; Vassiliadis, A.; Perino, A. Potential impact of a nonavalent HPV vaccine on HPV related low-and high-grade cervical intraepithelial lesions: A referral hospital-based study in Sicily. Hum. Vaccines Immunother. 2017, 13, 1839–1843. [Google Scholar] [CrossRef] [PubMed]
- Hillman, R.J.; Giuliano, A.R.; Palefsky, J.M.; Goldstone, S.; Moreira, E.D.; Vardas, E.; Aranda, C.; Jessen, H.; Ferris, D.G.; Coutlee, F.; et al. Immunogenicity of the Quadrivalent Human Papillomavirus (Type 6/11/16/18) Vaccine in Males 16 to 26 Years Old. Clin. Vaccine Immunol. 2012, 19, 261–267. [Google Scholar] [CrossRef]
- Luxembourg, A.; Moeller, E. 9-Valent human papillomavirus vaccine: A review of the clinical development program. Expert Rev. Vaccines 2017, 16, 1119–1139. [Google Scholar] [CrossRef]
- Bosco, L.; Serra, N.; Fasciana, T.; Pistoia, D.; Vella, M.; Di Gregorio, L.; Schillaci, R.; Perino, A.; Calagna, G.; Firenze, A.; et al. Potential impact of a nonavalent anti HPV vaccine in Italian men with and without clinical manifestations. Sci. Rep. 2021, 11, 4096. [Google Scholar] [CrossRef]
- Nielsen, K.J.; Jakobsen, K.K.; Jensen, J.S.; Grønhøj, C.; Von Buchwald, C. The Effect of Prophylactic HPV Vaccines on Oral and Oropharyngeal HPV Infection—A Systematic Review. Viruses 2021, 13, 1339. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Wilkin, T.; Bautista, O.M.; Cheon, K.; Connor, L.; Dubey, S.; Luxembourg, A.; Rawat, S.; Shaw, A.; Velicer, C.; et al. Design of a phase III efficacy, immunogenicity, and safety study of 9-valent human papillomavirus vaccine in prevention of oral persistent infection in men. Contemp. Clin. Trials 2022, 115, 106592. [Google Scholar] [CrossRef] [PubMed]
- Takes, R.P.; Wierzbicka, M.; D’souza, G.; Jackowska, J.; Silver, C.E.; Rodrigo, J.P.; Dikkers, F.G.; Olsen, K.D.; Rinaldo, A.; Brakenhoff, R.H.; et al. HPV vaccination to prevent oropharyngeal carcinoma: What can be learned from anogenital vaccination programs? Oral Oncol. 2015, 51, 1057–1060. [Google Scholar] [CrossRef] [PubMed]
- de Sanjosé, S.; Serrano, B.; Tous, S.; Alejo, M.; Lloveras, B.; Quirós, B.; Clavero, O.; Vidal, A.; Ferrándiz-Pulido, C.; Pavón, M.; et al. Burden of Human Papillomavirus (HPV)-Related Cancers Attributable to HPVs 6/11/16/18/31/33/45/52 and 58. JNCI Cancer Spectr. 2018, 2, pky045. [Google Scholar] [CrossRef] [PubMed]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef] [PubMed]
- Haws, A.L.F.; He, Q.; Rady, P.L.; Zhang, L.; Grady, J.; Hughes, T.K.; Stisser, K.; Konig, R.; Tyring, S.K. Nested PCR with the PGMY09/11 and GP5+/6+ primer sets improves detection of HPV DNA in cervical samples. J. Virol. Methods 2004, 122, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.P.; Saha, S.; Kraninger, J.L.; Swick, A.D.; Yu, M.; Lambert, P.F.; Kimple, R.J. Prevalence of Human Papillomavirus in Oropharyngeal Cancer. Cancer J. 2015, 21, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Langevin, S.M.; Eliot, M.; Nelson, H.H.; Pawlita, M.; McClean, M.D.; Kelsey, K.T. High-risk HPV types and head and neck cancer. Int. J. Cancer 2014, 135, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Donà, M.G.; Rollo, F.; Pichi, B.; Spriano, G.; Moretto, S.; Covello, R.; Pellini, R.; Benevolo, M. Evolving Profile of HPV-Driven Oropharyngeal Squamous Cell Carcinoma in a National Cancer Institute in Italy: A 10-Year Retrospective Study. Microorganisms 2020, 8, 1498. [Google Scholar] [CrossRef]
- Herzum, A.; Ciccarese, G.; Drago, F.; Pastorino, A.; Dezzana, M.; Mavilia, M.G.; Sola, S.; Copello, F.; Parodi, A. Cervical, oral and anal Human papillomavirus infection in women attending the Dermatology Unit of a regional reference hospital in Genoa, Italy: A prevalence study. J. Prev. Med. Hyg. 2022, 63, E415–E419. [Google Scholar] [CrossRef]
- Syrjänen, S. Oral manifestations of human papillomavirus infections. Eur. J. Oral Sci. 2018, 126, 49–66. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Graubard, B.I.; Broutian, T.; Pickard, R.K.; Tong, Z.-Y.; Xiao, W.; Kahle, L.; Gillison, M.L. NHANES 2009–2012 Findings: Association of Sexual Behaviors with Higher Prevalence of Oral Oncogenic Human Papillomavirus Infections in U.S. Men. Cancer Res. 2015, 75, 2468–2477. [Google Scholar] [CrossRef] [PubMed]
- Klein, S. The effects of hormones on sex differences in infection: From genes to behavior. Neurosci. Biobehav. Rev. 2000, 24, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Custer, J.; Patel, R.; Delclos, G.L.; DeSantis, S.M. Concurrent and Concordant Oral and Genital High-Risk Human Papillomavirus in the United States: Results from the National Health and Nutrition Examination Survey. J. Infect. Dis. 2021, 223, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Gravitt, P.E. Unraveling the Epidemiology of Oral Human Papillomavirus Infection. Ann. Intern. Med. 2017, 167, 748–749. [Google Scholar] [CrossRef] [PubMed]
- Kedarisetty, S.; Orosco, R.K.; Hecht, A.S.; Chang, D.C.; Weissbrod, P.A.; Coffey, C.S. Concordant Oral and Vaginal Human Papillomavirus Infection in the United States. JAMA Otolaryngol. Neck Surg. 2016, 142, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Patel, E.U.; Rositch, A.F.; Gravitt, P.E.; Tobian, A.A.R. Concordance of Penile and Oral Human Papillomavirus Infections Among Men in the United States. J. Infect. Dis. 2017, 215, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.T.; Boemi, S.; Caruso, G.; Sgalambro, F.; Ferlito, S.; Cavallaro, A.; Sudano, M.C.; Palumbo, M. Oral HPV Infection in Women with HPV-Positive Cervix Is Closely Related to Oral Sex. Diagnostics 2023, 13, 2096. [Google Scholar] [CrossRef] [PubMed]
- Steinau, M.; Hariri, S.; Gillison, M.L.; Broutian, T.R.; Dunne, E.F.; Tong, Z.-Y.; Markowitz, L.E.; Unger, E.R. Prevalence of Cervical and Oral Human Papillomavirus Infections Among US Women. J. Infect. Dis. 2014, 209, 1739–1743. [Google Scholar] [CrossRef]
- Shen, Y.; Huang, Y.; Wang, W.; Zhang, J.; Chen, X.; Zhang, L.; Huang, X.; Ge, Y. Prevalence and genotype distribution of HPV infection among women in Xiamen, China. Front. Microbiol. 2023, 14, 1130226. [Google Scholar] [CrossRef]
- Wang, T.; Luan, L.; Deng, J.; Liu, N.; Wu, Q.; Gong, T.; Zhu, J.; Zhang, Z.; Zhang, J. Prevalence and human papillomavirus (HPV) genotype distribution in Suzhou, China. Hum. Vaccines Immunother. 2023, 19, 2241309. [Google Scholar] [CrossRef]
- Liu, Y.; Li, Z.; Yuan, L.; Liu, F.; Wu, K.; Xiao, X.; Zhu, C. Human papillomavirus genotypic characteristics of 60,685 subjects under age-expansion vaccination of the nine-valent human papillomavirus vaccine: A cross-sectional study. J. Infect. Public Heal. 2023, 16, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Cheng, C.; Liang, R.; Zhu, Q.; Xue, F.; Xu, L.; Shi, Y.; Luo, H.; Yu, S.; He, J. Epidemiological analysis of HPV in Sichuan during 2014–2021. Cancer Epidemiol. 2023, 84, 102360. [Google Scholar] [CrossRef] [PubMed]
- Zhong, F.; Li, Z.; Sun, Y.; Xiao, Y.; Li, J.; Zhou, X.; Cong, Q.; Sui, L.; Tao, X.; Zhao, C. HPV genotyping of cervical histologic specimens of 61, 422 patients from the largest women hospital in China. Front. Oncol. 2023, 13, 1161631. [Google Scholar] [CrossRef]
- Chen, S.-F.; Yang, F.; Wang, W.-H.; Xu, C.; Zheng, L.-Y. High-risk HPV prevalence and genotype distribution among women in Liaocheng, Shandong Province, China from 2016 to 2022. Front. Public Health 2023, 11, 1145396. [Google Scholar] [CrossRef]
- Serretiello, E.; Corrado, F.; Santella, B.; Chianese, A.; Iervolino, D.; Coppola, A.; Grimaldi, E.; Galdiero, M.; Franci, G. Prevalence and Distribution of High- and Low- Risk HPV Genotypes in Women Living in the Metropolitan Area of Naples: A Recent Update. Asian Pac. J. Cancer Prev. 2023, 24, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Kiwerska, K.; Jozefiak, A.; Markowska, J.; Kedzia, W.; Jackowska, J.; Wierzbicka, M. Oral-genital human papillomavirus infection in Polish couples: Frequent detection of HPV 42. BMC Infect. Dis. 2019, 19, 122. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Total (n = 337) | Females (n = 281) | Males (n = 56) |
|---|---|---|---|
| Age | |||
| Mean (SD) | 33.7 (10.2) | 32.4 (9.2) | 38.2 (11.9) |
| Median (IQR) | 31 (25.9–40) | 30.3 (25.5–37.1) | 38.2(29.7–45.4) |
| HPV+ | |||
| Genital | 73.6% (248/337) | 73.7% (207/281) | 73.2 (41/56) |
| Oral | 10.1% (34/337) | 7.1% (20/281) | 25% (14/56) |
| HrHPV (including lrHPV/hrHPV infections) | |||
| Genital | 86.7% (215/248) | 87% (180/207) | 82.9% (34/41) |
| Oral | 70.6% (24/34) | 65% (13/20) | 78.6% (11/14) |
| Single infections | |||
| Genital | 62.1% (154/248) | 67.1% (139/207) | 36.6% (15/41) |
| Oral | 91.2% (31/34) | 95% (19/20) | 85.7% (12/14) |
| Multiple infections | |||
| Genital | 37.9% (94/248) | 32.9% (68/207) | 63.4% (26/41) |
| Oral | 8.8% (3/34) | 5% (1/20) | 14.3% (2/14) |
| Concurrence | 12.5% (31/248) | 9.2% (19/207) | 29.3% (12/41) |
| hr-concordance | 61.3% (19/31) | 57.9% (11/19) | 66.7% (8/12) |
| lr-concordance | 12.9% (4/31) | 15.8% (3/19) | 8.3% (1/12) |
| Type-concordance | 25.8% (10/31) | 31.6% (6/19) | 33.3% (4/12) |
| Genotype included in the quadrivalent vaccine | |||
| Genital | 35.1% (87/248) | 31.9% (66/207) | 51.2% (21/41) |
| Oral | 35.3% (12/34) | 30% (6/20) | 42.9% (6/14) |
| Genotype included in the nonavalent vaccine | |||
| Genital | 61.7% (153/248) | 59.4% (123/207) | 73.2% (30/41) |
| Oral | 44.1% (15/34) | 40% (8/20) | 50% (7/14) |
| HPV+ (Oral) (n = 34) | HPV+ (Genital) (n = 248) | |||
|---|---|---|---|---|
| Genotypes Not Included in Quadrivalent or Nonavalent Vaccine | % (n) | L/H Risk | % (n) | L/H Risk |
| 3 | 2.9 (1) | LR | - | |
| 7 | 2.9 (1) | LR | - | |
| 10 | 2.9 (1) | LR | - | |
| 35 | - | - | 2.0 (5) | HR |
| 39 | - | - | 3.2 (8) | HR |
| 40 | - | - | 0.8 (2) | LR |
| 42 | - | - | 8.9 (22) * | LR |
| 44 | - | - | 3.6 (9) | LR |
| 51 | 8.8 (3) | HR | 9.3 (23) * | HR |
| 53 | 5.9 (2) | HR | 11.3 (28) * | HR |
| 54 | 2.9 (1) | LR | 3.2 (8) | LR |
| 55 | - | - | 0.4 (1) | LR |
| 56 | 5.9 (2) | HR | 4.8 (12) | HR |
| 59 | 2.9 (1) | HR | 3.6 (9) | HR |
| 61 | 2.9 (1) | LR | 2.0 (5) | LR |
| 62 | 2.9 (1) | LR | 2.8 (7) | LR |
| 64 | - | - | 0.4 (1) | HR |
| 66 | 8.8 (3) | HR | 12.9 (32) * | HR |
| 67 | - | - | 1.6 (4) | HR |
| 68 | - | - | 6.0 (15) * | HR |
| 69 | - | - | 0.4 (1) | HR |
| 70 | - | - | 3.2 (8) | HR |
| 72 | - | - | 0.8 (2) | LR |
| 73 | - | - | 4.0 (10) | HR |
| 74 | - | - | 1.2 (3) | LR |
| 81 | - | - | 2.4 (6) | LR |
| 82 | - | - | 0.8 (2) | HR |
| 83 | 2.9 (1) | LR | 2.0 (5) | LR |
| 84 | - | - | 2.8 (7) | LR |
| 87 | - | - | 0.4 (1) | LR |
| 89 | - | - | 2.8 (7) | LR |
| 107 | 5.9 (2) | LR | - | - |
| HPV+ (Oral) (n = 34) | HPV+ (Genital) (n = 248) | |||
|---|---|---|---|---|
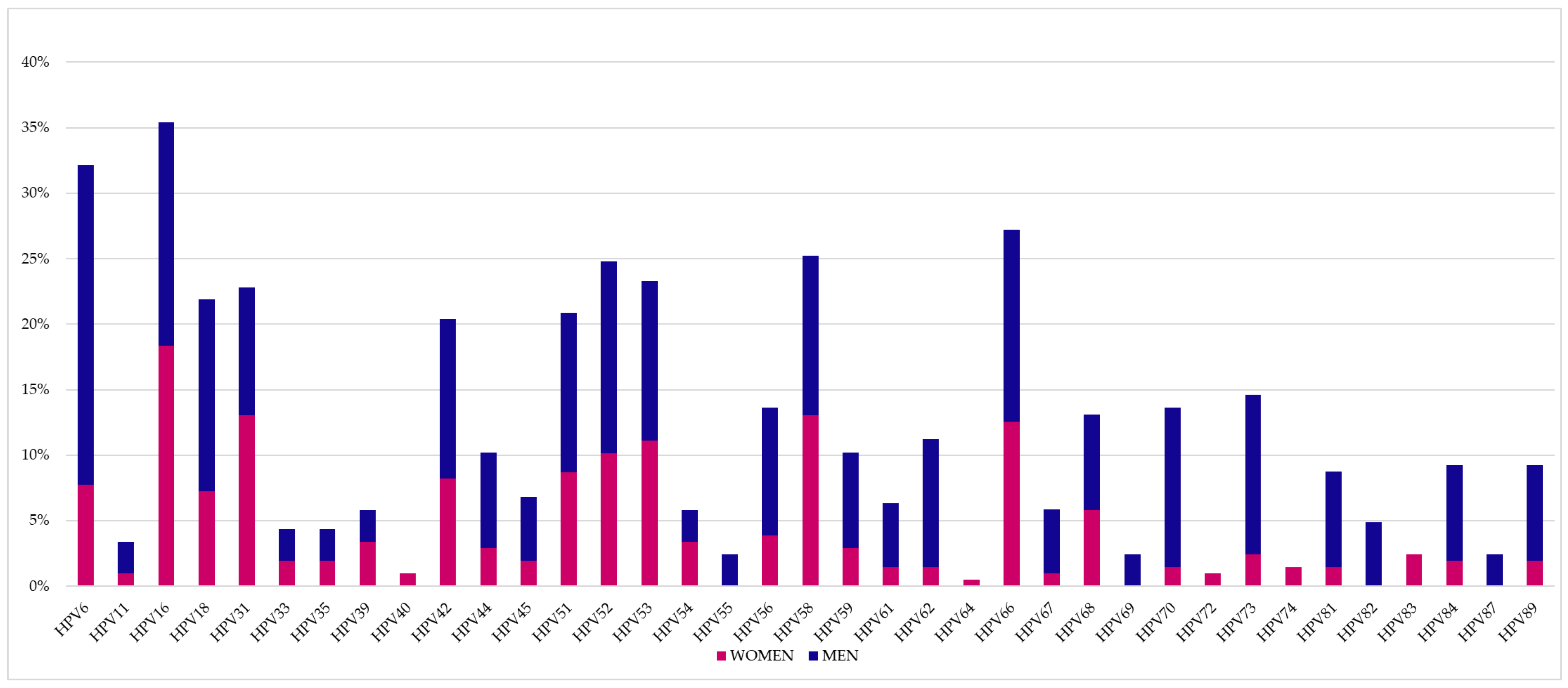
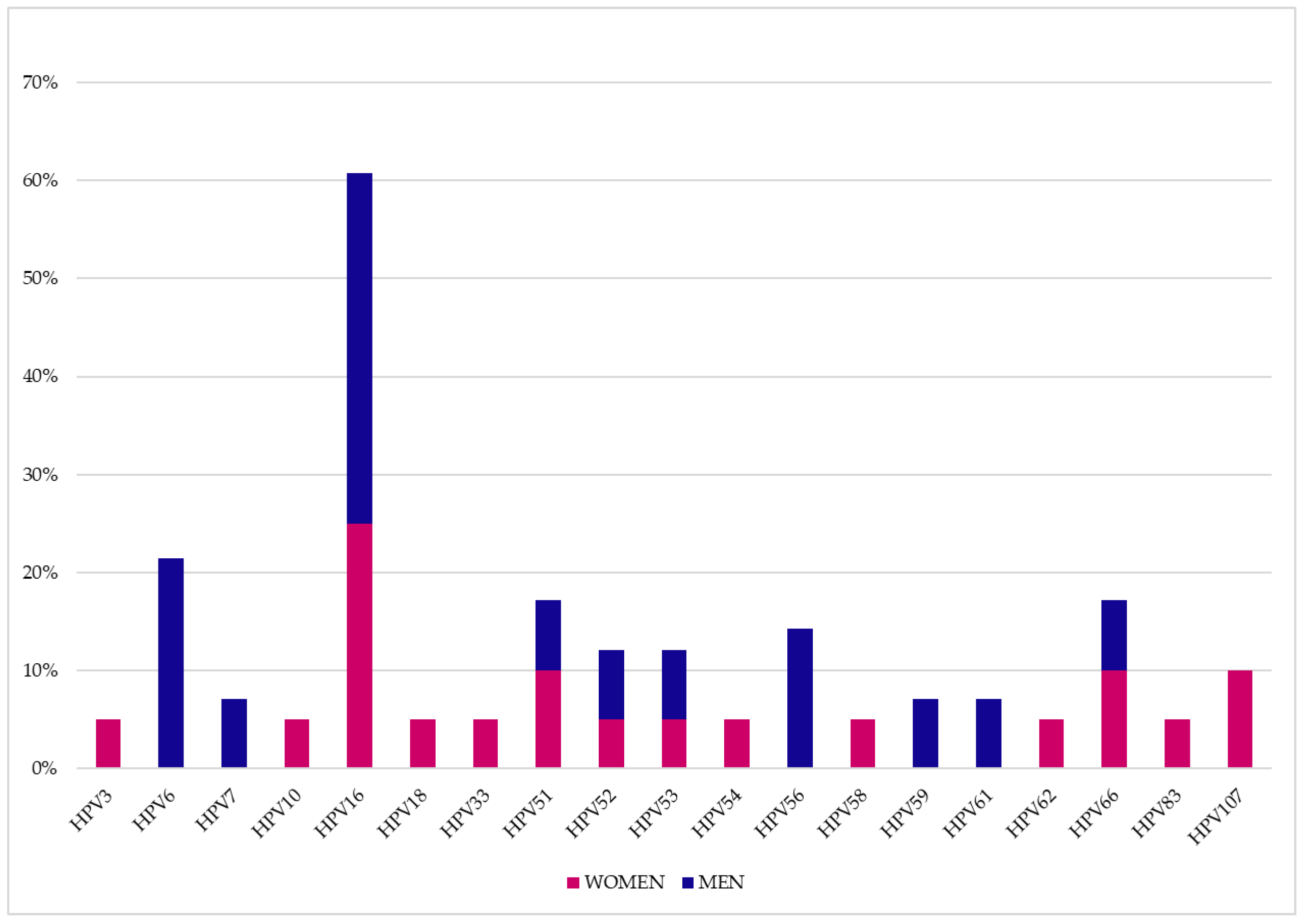
| Genotypes Not Included in Quadrivalent or Nonvalent Vaccine | Males (14) % (n) | Females (n = 20) % (n) | Males (n = 41) % (n) | Females (n = 207) % (n) |
| 3 | - | 5.0 (1) | - | - |
| 7 | 7.1 (1) | - | - | - |
| 10 | - | 5.0 (1) | - | - |
| 35 | - | - | 2.4 (1) | 1.9 (4) |
| 39 | - | - | 2.4 (1) | 3.4 (7) |
| 40 | - | - | - | 1.0 (2) |
| 42 | - | - | 12.2 (5) * | 8.2 (17) * |
| 44 | - | - | 7.3 (3) | 2.9 (6) |
| 51 | 7.1 (1) | 10.0 (2) | 12.2 (5) * | 8.7 (18) * |
| 53 | 7.1 (1) | 5.0 (1) | 12.2 (5) * | 11.1 (23) * |
| 54 | - | 5.0 (1) | 2.4 (1) | 3.4 (7) |
| 55 | - | - | 2.4 (1) | - |
| 56 | 14.3 (2) | - | 9.8 (4) | 3.9 (8) |
| 59 | 7.1 (1) | - | 7.3 (3) | 2.9 (6) |
| 61 | 7.1 (1) | - | 4.9 (2) | 1.4 (3) |
| 62 | - | 5.0 (1) | 9.8 (4) | 1.4 (3) |
| 64 | - | - | - | 0.5 (1) |
| 66 | 7.1 (1) | 10.0 (2) | 14.6 (6) * | 12.6 (26) * |
| 67 | - | - | 4.9 (2) | 1.0 (2) |
| 68 | - | - | 7.3 (3) | 5.6 (12) * |
| 69 | - | - | 2.4 (1) | - |
| 70 | - | - | 12.2 (5) * | 1.4 (3) |
| 72 | - | - | - | 1.0 (2) |
| 73 | - | - | 12.2 (5) * | 2.4 (5) |
| 74 | - | - | - | 1.4 (3) |
| 81 | - | - | 7.3 (3) | 1.4 (3) |
| 82 | - | - | 4.9 (2) | - |
| 83 | - | 5.0 (1) | - | 2.4 (5) |
| 84 | - | - | 7.3 (3) | 1.9 (4) |
| 87 | - | - | 2.4 (1) | - |
| 89 | - | - | 7.3 (3) | 1.9 (4) |
| 107 | - | 10.0 (2) | - | - |
| Parameters | HPV+ (Oral) (n = 34) | HPV+ (Genital) (n = 248) | HPV+ (Oral) vs. HPV+ (Genital) |
|---|---|---|---|
| Age | |||
| Mean (SD) | 37.1 (11.7) | 33.6 (10.2) | |
| Median (IQR) | 36 (28.5, 46.5) | 31 (25.75, 40) | 0.09 (MW) |
| Shapiro–Wilk test | p = 0.0025, rN | p < 0.0001, rN | |
| Gender | |||
| Male | 41.2% (14) | 16.5% (41) | 0.0007 * (C) |
| Female | 58.8% (20) | 85.5% (207) | |
| hrHPV (including lrHPV/hrHPV infections) | 70.6% (24) | 86.7% (215) | |
| lrHPV | 29.4% (10) | 13.3% (33) | 0.0143 * (C) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buttà, M.; Serra, N.; Panzarella, V.; Fasciana, T.M.A.; Campisi, G.; Capra, G. Orogenital Human Papillomavirus Infection and Vaccines: A Survey of High- and Low-Risk Genotypes Not Included in Vaccines. Vaccines 2023, 11, 1466. https://doi.org/10.3390/vaccines11091466
Buttà M, Serra N, Panzarella V, Fasciana TMA, Campisi G, Capra G. Orogenital Human Papillomavirus Infection and Vaccines: A Survey of High- and Low-Risk Genotypes Not Included in Vaccines. Vaccines. 2023; 11(9):1466. https://doi.org/10.3390/vaccines11091466
Chicago/Turabian StyleButtà, Michela, Nicola Serra, Vera Panzarella, Teresa Maria Assunta Fasciana, Giuseppina Campisi, and Giuseppina Capra. 2023. "Orogenital Human Papillomavirus Infection and Vaccines: A Survey of High- and Low-Risk Genotypes Not Included in Vaccines" Vaccines 11, no. 9: 1466. https://doi.org/10.3390/vaccines11091466