
Adverse Maternal Outcomes in Pregnant Women Affected by Severe-Critical COVID-19 Illness: Correlation with Vaccination Status in the Time of Different Viral Strains’ Dominancy

 , , ,
, , ,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Prevalence of Severe-Critical Maternal Outcomes and Possible Correlation with the Pandemic Waves and Viral Strains
3.2. Comparison between the SARS-CoV-2 Variants, the Specific Pandemic Wave (Wild, Alpha, Delta, Omicron Dominant), and the Severe-Critical Adverse Maternal Outcomes
3.3. Comparison between Vaccinated vs. Non-Vaccinated Patients during the Fourth Wave
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volpe, N.; Schera, G.B.L.; Frusca, T. COVID-19 in pregnancy: Italian experience. Perinat. J. 2020, 28, 149–153. [Google Scholar] [CrossRef]
- National_Institutes_of_Health. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 15 November 2022).
- Adhikari, E.H.; Moreno, W.; Zofkie, A.C.; MacDonald, L.; McIntire, D.D.; Collins, R.R.J.; Spong, C.Y. Pregnancy Outcomes Among Women with and without Severe Acute Respiratory Syndrome Coronavirus 2 Infection. JAMA Netw Open 2020, 3, e2029256. [Google Scholar] [CrossRef]
- Wong, Y.P.; Khong, T.Y.; Tan, G.C. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Resta, L.; Vimercati, A.; Cazzato, G.; Mazzia, G.; Cicinelli, E.; Colagrande, A.; Fanelli, M.; Scarcella, S.V.; Ceci, O.; Rossi, R. SARS-CoV-2 and Placenta: New Insights and Perspectives. Viruses 2021, 13, 723. [Google Scholar] [CrossRef]
- Resta, L.; Vimercati, A.; Sablone, S.; Marzullo, A.; Cazzato, G.; Ingravallo, G.; Mazzia, G.; Arezzo, F.; Colagrande, A.; Rossi, R. Is the First of the Two Born Saved? A Rare and Dramatic Case of Double Placental Damage from SARS-CoV-2. Viruses 2021, 13, 995. [Google Scholar] [CrossRef] [PubMed]
- Edlow, A.G.; Li, J.Z.; Collier, A.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw Open 2020, 3, e2030455. [Google Scholar] [CrossRef] [PubMed]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased Fetal Movements: A Sign of Placental SARS-CoV-2 Infection with Perinatal Brain Injury. Viruses 2021, 13, 2517. [Google Scholar] [CrossRef]
- Shook, L.L.; Sullivan, E.L.; Lo, J.O.; Perlis, R.H.; Edlow, A.G. COVID-19 in pregnancy: Implications for fetal brain development. Trends Mol. Med. 2022, 28, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.A.; O’Reilly, D.P.; Edebiri, O.; Donnelly, J.C.; McCallion, N.; Drew, R.J.; Ferguson, W. The Effect of COVID-19 Infection During Pregnancy; Evaluating Neonatal Outcomes and the Impact of the B.1.1.7. Variant. Pediatr. Infect. Dis. J. 2021, 40, e475–e481. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, E.H.; SoRelle, J.A.; McIntire, D.D.; Spong, C.Y. Increasing severity of COVID-19 in pregnancy with Delta (B.1.617.2) variant surge. Am. J. Obstet. Gynecol. 2022, 226, 149–151. [Google Scholar] [CrossRef]
- DeSisto, C.L.; Wallace, B.; Simeone, R.M.; Polen, K.; Ko, J.Y.; Meaney-Delman, D.; Ellington, S.R. Risk for stillbirth among women with and without COVID-19 at delivery hospitalization—United States, March 2020–September 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1640. [Google Scholar] [CrossRef] [PubMed]
- Vousden, N.; Ramakrishnan, R.; Bunch, K.; Morris, E.; Simpson, N.A.B.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; et al. Severity of maternal infection and perinatal outcomes during periods of SARS-CoV-2 wildtype, alpha, and delta variant dominance in the UK: Prospective cohort study. BMJ Med. 2022, 1. [Google Scholar] [CrossRef]
- Donati, S.; Corsi, E.; Maraschini, A.; Salvatore, M.A.; the ItOSS-COVID-19 Working Group. SARS-CoV-2 infection among hospitalised pregnant women and impact of different viral strains on COVID-19 severity in Italy: A national prospective population-based cohort study. BJOG 2022, 129, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland. Nat. Med. 2022, 28, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic review and meta-analysis of the effectiveness and perinatal outcomes of COVID-19 vaccination in pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef] [PubMed]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. Am. J. Obs. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Bookstein Peretz, S.; Regev, N.; Novick, L.; Nachshol, M.; Goffer, E.; Ben-David, A.; Asraf, K.; Doolman, R.; Levin, E.G.; Regev Yochay, G.; et al. Short-term outcome of pregnant women vaccinated with BNT162b2 mRNA COVID-19 vaccine. Ultrasound Obs. Gynecol. 2021, 58, 450–456. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Biron-Shental, T.; Makov-Assif, M.; Key, C.; Kohane, I.S.; Hernan, M.A.; Lipsitch, M.; Hernandez-Diaz, S.; Reis, B.Y.; et al. Effectiveness of the BNT162b2 mRNA COVID-19 vaccine in pregnancy. Nat. Med. 2021, 27, 1693–1695. [Google Scholar] [CrossRef]
- Loconsole, D.; Centrone, F.; Morcavallo, C.; Campanella, S.; Sallustio, A.; Accogli, M.; Fortunato, F.; Parisi, A.; Chironna, M. Rapid spread of the SARS-CoV-2 variant of concern 202012/01 in Southern Italy (December 2020–March 2021). Int. J. Environ. Res. Public Health 2021, 18, 4766. [Google Scholar] [CrossRef]
- Glick, I.; Kadish, E.; Rottenstreich, M. Management of Pregnancy in Women of Advanced Maternal Age: Improving Outcomes for Mother and Baby. Int. J. Womens Health 2021, 13, 751–759. [Google Scholar] [CrossRef]
- Johansson, S.A.-O.; Sandström, A.; Cnattingius, S. Maternal overweight and obesity increase the risk of fetal acidosis during labor. J. Perinatol. 2018, 38, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Vimercati, A.; De Nola, R.; Trerotoli, P.; Metta, M.E.; Cazzato, G.; Resta, L.; Malvasi, A.; Lepera, A.; Ricci, I.; Capozza, M.; et al. COVID-19 Infection in Pregnancy: Obstetrical Risk Factors and Neonatal Outcomes— A Monocentric, Single-Cohort Study. Vaccines 2022, 10, 166. [Google Scholar]
- Thornton, J.G. SARS-CoV-2 infection among hospitalised pregnant women and impact of different viral strains on COVID-19 disease severity in Italy. BJOG 2022, 129, 232. [Google Scholar] [CrossRef]
- Loconsole, D.; Bisceglia, L.; Centrone, F.; Sallustio, A.; Accogli, M.; Dalfino, L.; Brienza, N.; Chironna, M. Autochthonous Outbreak of SARS-CoV-2 Omicron Variant in Booster-Vaccinated (3 Doses) Healthcare Workers in Southern Italy: Just the Tip of the Iceberg? Vaccines 2022, 10, 283. [Google Scholar] [CrossRef]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., 3rd; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status-United States, 22 January 22–3 October 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1641. [Google Scholar] [CrossRef]
- Audit, I. ICNARC report on COVID-19 in critical care. ICNARC 2020, 10, 1–26. [Google Scholar]
- Gurzenda, S.; Castro, M.C. COVID-19 poses alarming pregnancy and postpartum mortality risk in Brazil. EClin. Med. 2021, 36, 30. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef]
- Male, V. SARS-CoV-2 infection and COVID-19 vaccination in pregnancy. Nat. Rev. Immunol. 2022, 22, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Kosovali, B.D.; Tezcan, B.; Mutlu, N.M. Effects of SARS-CoV-2 Variants on Maternal Infection and Severity: A Single-Center Experience. Cureus 2022, 14, e24201. [Google Scholar] [CrossRef]
- Shukla, V.V.; Rahman, A.F.; Shen, X.; Black, A.; Nakhmani, A.; Ambalavanan, N.; Carlo, W.A. Trends in Maternal Outcomes During the COVID-19 Pandemic in Alabama From 2016 to 2021. JAMA Netw. Open 2022, 5, e222681. [Google Scholar] [CrossRef] [PubMed]
- Mupanomunda, M.; Fakih, M.G.; Miller, C.; Ottenbacher, A.; Winegar, A.L.; Roberts, P.; Kimathi, M.; Gianopoulos, J.G.; Cahill, A.G.; Cacchione, J.G.; et al. Comparison of Severe Maternal Morbidities Associated With Delivery During Periods of Circulation of Specific SARS-CoV-2 Variants. JAMA Netw. Open 2022, 5, e2226436. [Google Scholar] [CrossRef] [PubMed]
- ISS. Italian Case-Based Surveillance System. Available online: https://www.epicentro.iss.it/en/vaccines/covid-19-pregnancy-breastfeeding (accessed on 29 June 2022).
- SIGO-AOGOI-AGUI-AGITE-SIN. Position Paper ad Interim. VACCINAZIONE ANTI-COVID19 e GRAVIDANZA. 2021. Available online: https://www.sigo.it/wp-content/uploads/2021/01/VaccinoCovid19eGravidanza-SIGO-AOGOI-AGUI-AGITE-SIN_02-01-2021.pdf (accessed on 15 November 2022).
- ItOSS. Documento ItOSS su Vaccino ANTI Covid-19 in Gravidanza e Allattamento_9 Gennaio. 2021. Available online: https://www.iss.it/documents/20126/0/Documento+ItOSS+su+vaccino+ANTI+covid-19+in+gravidanza+e+allattamento_9+gennaio.pdf/5f6c170c-3d37-d6b5-a1e7-b0b728dc1ba6?t=1610194643183 (accessed on 15 November 2022).
- SIGO. PositionPaper_Gravidanza_Vaccinazione_anti_COVID. 2021. Available online: https://www.sigo.it/wp-content/uploads/2021/05/PositionPaper_Gravidanza_Vaccinazione_anti_COVID_05.05.2021.pdf (accessed on 15 November 2022).
- The U.S. Food and Drug Administration. FDA Authorizes Booster Dose of Pfizer-BioNTech COVID-19 Vaccine for Certain Populations. U.S. Food and Drug Administration. FDA Authorizes Booster Dose of Pfizer-BioNTech COVID-19 Vaccine for Certain Populations. Available online: https://www.fda.gov/ news-events/press-announcements/fda-authorizes-boosterdose-pfizer-biontech-covid-19-vaccine-certain-populations (accessed on 23 November 2021).
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obs. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef] [PubMed]
- ISS. Indicazioni ad interim su. Vaccinazione contro il COVID-19 in gravidanza e allattamento. Aggiornamento del 22 settembre 2021. 2021. Available online: https://www.iss.it/documents/20126/0/Aggiornamento+indicazioni+ISS+su+vaccino+in+grav_+e+allatt_2021+%281%29.pdf/a4469f15-3fb4-e11f-8a10-5103b451b138?t=1632477934377 (accessed on 15 November 2022).
- Raccomandazioni Sulla Vaccinazione Anti SARS-CoV-2/COVID-19 in Gravidanza. 2021. Available online: https://www.siml.it/post/circolare-del-ministero-della-salute-n-43293-del-24-09-2021-recante-le-raccomandazioni-sulla-vaccinazione-anti-sars-cov-2-covid-19-in-gravidanza-e-allattamento (accessed on 15 November 2022).
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association Between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 326, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Yasuhara, J.; Iwagami, M.; Miyamoto, Y.; Yamada, Y.; Suzuki, Y.; Takagi, H.; Kuno, T. Peripartum Outcomes Associated With COVID-19 Vaccination During Pregnancy: A Systematic Review and Meta-analysis. AMA Pediatr. 2022, 176, 1098–1106. [Google Scholar] [CrossRef] [PubMed]
- Kugelman, N.; Nahshon, C.; Shaked-Mishan, P.; Cohen, N.; Sher, M.L.; Gruber, M.; Marom, I.; Zolotarevsky, A.; Lavie, O.; Damti, A. Maternal and neonatal SARS-CoV-2 immunoglobulin G antibody levels at delivery after receipt of the BNT162b2 messenger RNA COVID-19 vaccine during the second trimester of pregnancy. JAMA Pediatr. 2022, 176, 290–295. [Google Scholar] [CrossRef]
- Badell, M.L.; Dude, C.M.; Rasmussen, S.A.; Jamieson, D.J. Covid-19 vaccination in pregnancy. BMJ 2022, 378, e069741. [Google Scholar] [CrossRef]
- RCOG; RCM. Coronavirus (COVID-19) Infection in Pregnancy. Version 15: Published Monday 7 March 2022. 2022. Available online: https://www.rcog.org.uk/guidance/coronavirus-covid-19-pregnancy-and-women-s-health/coronavirus-covid-19-infection-in-pregnancy/ (accessed on 15 November 2022).
- Franchini, M.; Prefumo, F.; Grisolia, G.; Bergamini, V.; Glingani, C.; Pisello, M.; Presti, F.; Zaffanello, M. Convalescent Plasma for Pregnant Women with COVID-19: A Systematic Literature Review. Viruses 2021, 13, 1194. [Google Scholar] [CrossRef]
- AIFA. Sotrovimab_Allegato1_Informativa_hcp.pdf. 2021. Available online: https://www.aifa.gov.it/documents/20142/1307084/sotrovimab_Allegato1_Informativa_hcp.pdf (accessed on 23 November 2021).



{kind=link}
{kind=link}
| Age (years) | <30 | 31.15% |
| 30–40 | 62.30% | |
| >40 | 5.74% | |
| Missing | 0.82% | |
| BMI | <25 normal and under weight | 16.39% |
| 25–30 overweight | 56.56% | |
| >30 obese | 20.49% | |
| missing | 6.56% | |
| Ethnicity | Caucasian | 95.08% |
| African | 4.10% | |
| Asian | 0.82% | |
| Comorbidities | hypertension/pre-eclampsia | 1.64% |
| diabetes/gestational diabetes | 9.84% | |
| Others | 23.77% | |
| Healthy | 64.75% | |
| Missing | 0.82% | |
| Parity | Nulliparous | 40.98% |
| Multiparous | 59.02% | |
| G.A. at Covid diagnosis | 1° trimester | 0.00% |
| 2° trimester | 1.64% | |
| 3° trimester | 98.36% | |
| COVID-19 SYMPTOMS | 1 none | 60.66% |
| 2A few | 19.67% | |
| 2B mild | 14.75% | |
| 3 severe-critical | 4.10% | |
| Missing | 0.82% |
| AGE | 37.5 [4.5] * | |
| BMI | 30 [4.6] * | |
| COMORBITIDY | 100% none | |
| ETHNICITY | 100% Caucasic | |
| SARS-CoV2 vaccination | 0% | |
| SARS-CoV2 variant | Wild Alpha Delta Omicron | 25% 25% 50% 0% |
| Epidemic wave | I II III IV | 25% 25% 50% 0% |
| COVID-19 detection | 100% nasopharyngeal swab, RT-PCR analysis | |
| Step-up days stay | 13.50 [7.75] * days | |
| Overall OTI | 57% | |
| Overall BiPAP | 75% | |
| Hyperimmune plasma adm. | 62% | |
| Remdesivir adm. | 12% | |
| Antibiotics adm. | 62% | |
| Heparin adm. | 88% | |
| Mode of delivery | 100% CS | |
| Primigravida | 50% | |
| Twin pregnancy | 25% | |
| G.A. | 34.9 [3.72] * | |
| Neonatal weight | 2570 [1115] * g | |
| Neonatal weight percentile | 56.5 [34] * | |
| Neonatal step-down | 27% | |
| Neonatal step-up | 18% | |
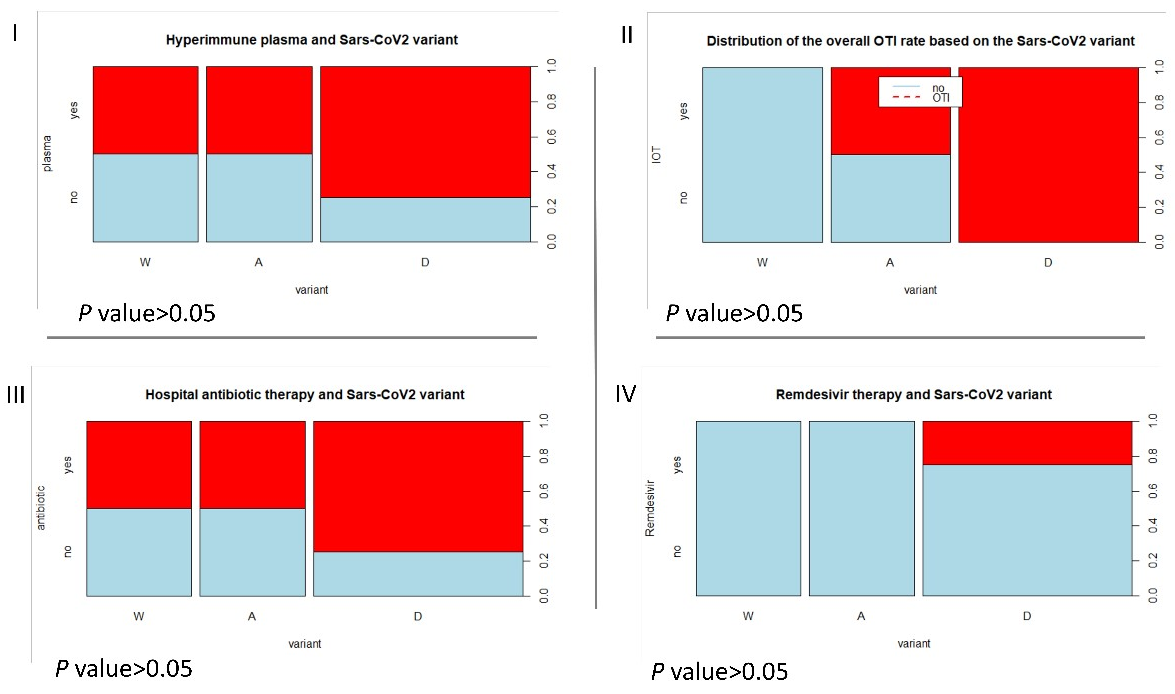
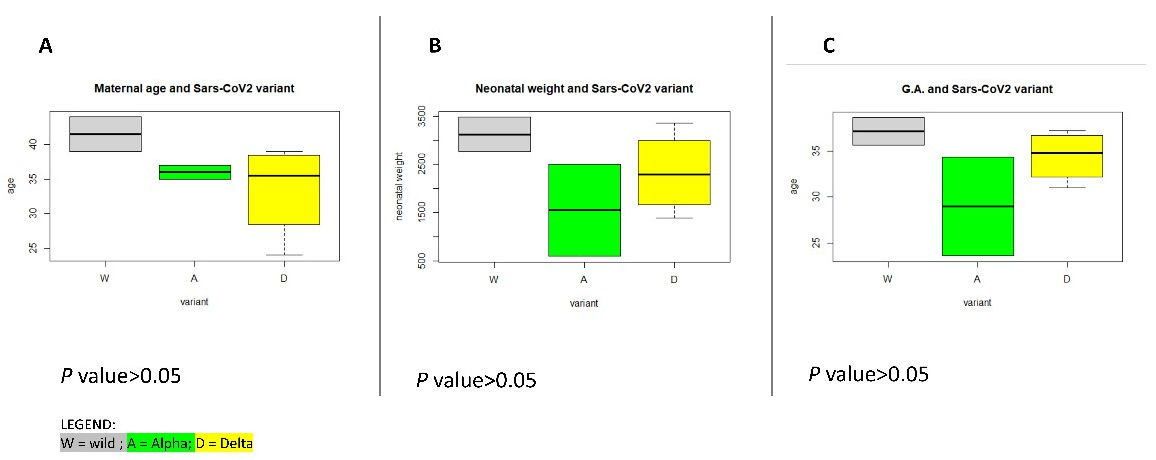
| Wild | Alpha | Delta | |
|---|---|---|---|
| AGE | 41.5 [2.5] * yrs | 36 [1] * yrs | 35.5 [7.5] * yrs |
| Overall OTI | 0% | 50% | 100% |
| Hyperimm. plasma | 50% | 50% | 75% |
| Remdesivir | 0% | 0% | 33% |
| Antibiotic therapy | 50% | 50% | 75% |
| Neonatal weight | 3125 [355] * g | 1145 [955] * g | 2290 [1017.5] * g |
| G.A. | 37.1 [1.5] * wks, ds | 28.9 [5.35] * wks, ds | 34.7 [3.72] * wks, ds |
| Variant | No ICU Admission | ICU Admission | Odds for ICU Admission | Risk Ratio (95% CI) |
|---|---|---|---|---|
| W | 78 | 2 | 0.02 | 0.78 (0.11–5.33) |
| A | 61 | 2 | 0.03 | 1.00 |
| D | 16 | 4 | 0.25 | 6.30 |
| O | 124 | 0 | 0.00 | 0.00 |
| Groups compared in rx2 tables | p-value of the risk ratio comparison | |||
| W vs. A | 0.8 | |||
| W vs. D | 0.01 | |||
| W vs. O | 0.08 | |||
| A vs. D | 0.01 | |||
| A vs. O | 0.05 | |||
| D vs. O | <0.001 | |||
| Vaccine | No ICU Admission | ICU Admission | Odds for ICU Admission | Risk Ratio (95% CI) |
|---|---|---|---|---|
| Yes | 87 | 0 | 0.00 | 1.00 |
| No | 192 | 8 | 0.04 | 0.00 |
| Groups compared in rx2 tables | p-value of the risk ratio comparison | |||
| Vaccinated vs. Non-vaccinated | 0.06 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vimercati, A.; De Nola, R.; Battaglia, S.; Di Mussi, R.; Cazzato, G.; Resta, L.; Chironna, M.; Loconsole, D.; Vinci, L.; Chiarello, G.; et al. Adverse Maternal Outcomes in Pregnant Women Affected by Severe-Critical COVID-19 Illness: Correlation with Vaccination Status in the Time of Different Viral Strains’ Dominancy. Vaccines 2022, 10, 2061. https://doi.org/10.3390/vaccines10122061
Vimercati A, De Nola R, Battaglia S, Di Mussi R, Cazzato G, Resta L, Chironna M, Loconsole D, Vinci L, Chiarello G, et al. Adverse Maternal Outcomes in Pregnant Women Affected by Severe-Critical COVID-19 Illness: Correlation with Vaccination Status in the Time of Different Viral Strains’ Dominancy. Vaccines. 2022; 10(12):2061. https://doi.org/10.3390/vaccines10122061
Chicago/Turabian StyleVimercati, Antonella, Rosalba De Nola, Stefano Battaglia, Rossella Di Mussi, Gerardo Cazzato, Leonardo Resta, Maria Chironna, Daniela Loconsole, Lorenzo Vinci, Giulia Chiarello, and et al. 2022. "Adverse Maternal Outcomes in Pregnant Women Affected by Severe-Critical COVID-19 Illness: Correlation with Vaccination Status in the Time of Different Viral Strains’ Dominancy" Vaccines 10, no. 12: 2061. https://doi.org/10.3390/vaccines10122061