
The Assessment of the Reliability and Validity of the Polish Version of the Adult Vaccine Hesitancy Scale (PL-aVHS) in the Context of Attitudes toward COVID-19 Vaccination


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Questionnaire
2.3. Cultural Adaptation of aVHS (PL-aVHS)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Internal Consistency
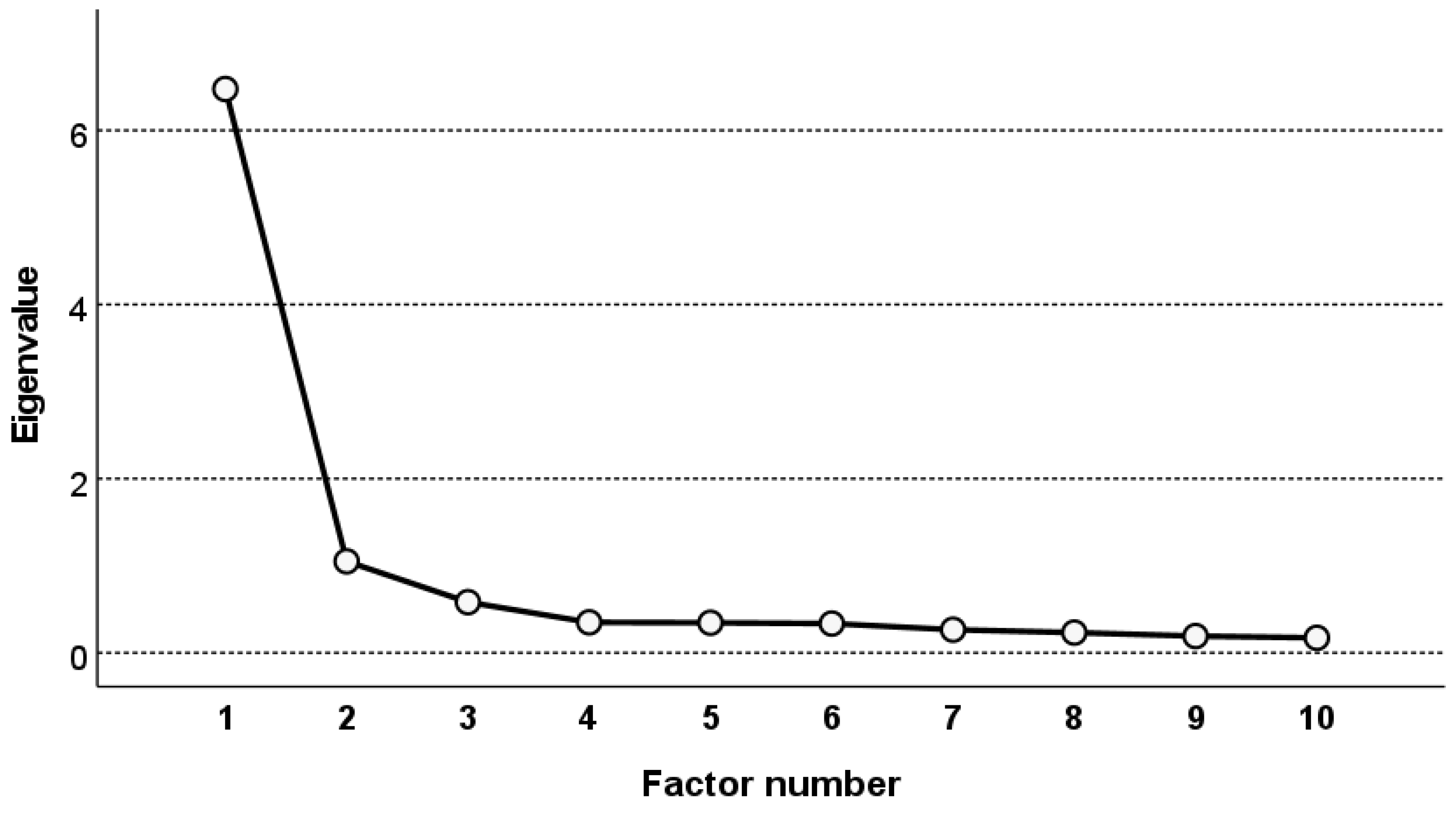
3.3. Exploratory Factor Analysis
3.4. Hypotheses Testing
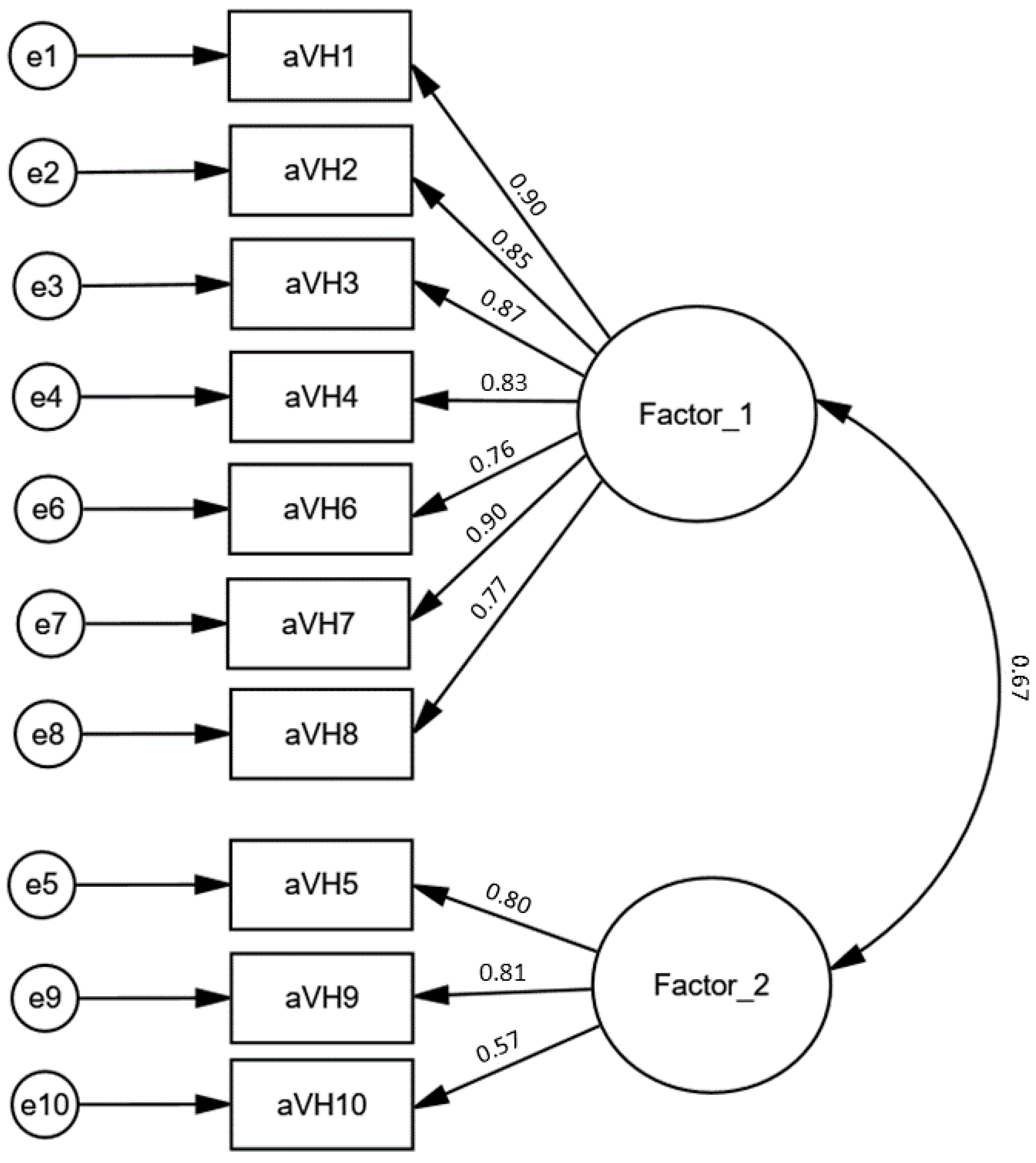
3.5. Confirmatory Factor Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; de Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A Practical Taxonomy for the Determinants of Vaccine Uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [Green Version]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of Vaccination Readiness. Eur. J. Psychol. Assess. 2021, 38, 261–269. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Zhou, C.; Catz, S.; Myaing, M.; Mangione-Smith, R. The Relationship between Parent Attitudes about Childhood Vaccines Survey Scores and Future Child Immunization Status: A Validation Study. JAMA Pediatr. 2013, 167, 1065–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilkey, M.B.; Magnus, B.E.; Reiter, P.L.; McRee, A.L.; Dempsey, A.F.; Brewer, N.T. The Vaccination Confidence Scale: A Brief Measure of Parents’ Vaccination Beliefs. Vaccine 2014, 32, 6259–6265. [Google Scholar] [CrossRef] [Green Version]
- Sarathchandra, D.; Navin, M.C.; Largent, M.A.; McCright, A.M. A Survey Instrument for Measuring Vaccine Acceptance. Prev. Med. 2018, 109, 1–7. [Google Scholar] [CrossRef]
- Frew, P.M.; Murden, R.; Mehta, C.C.; Chamberlain, A.T.; Hinman, A.R.; Nowak, G.; Mendel, J.; Aikin, A.; Randall, L.A.; Hargreaves, A.L.; et al. Development of a US Trust Measure to Assess and Monitor Parental Confidence in the Vaccine System. Vaccine 2019, 37, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.K.; Tatar, O.; Dube, E.; Amsel, R.; Knauper, B.; Naz, A.; Perez, S.; Rosberger, Z. The Vaccine Hesitancy Scale: Psychometric Properties and Validation. Vaccine 2018, 36, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond Confidence: Development of a Measure Assessing the 5C Psychological Antecedents of Vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; Eskola, J.; et al. Measuring Vaccine Hesitancy: The Development of a Survey Tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luyten, J.; Bruyneel, L.; van Hoek, A.J. Assessing Vaccine Hesitancy in the UK Population Using a Generalized Vaccine Hesitancy Survey Instrument. Vaccine 2019, 37, 2494–2501. [Google Scholar] [CrossRef]
- Akel, K.B.; Masters, N.B.; Shih, S.F.; Lu, Y.; Wagner, A.L. Modification of a Vaccine Hesitancy Scale for Use in Adult Vaccinations in the United States and China. Hum. Vaccines Immunother. 2021, 17, 2639–2646. [Google Scholar] [CrossRef]
- Ledda, C.; Costantino, C.; Liberti, G.; Rapisarda, V. The Italian Version of the Adult Vaccine Hesitancy Scale (AVHS) for the Working-Age Population: Cross-Cultural Adaptation, Reliability, and Validity. Vaccines 2022, 10, 224. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.S.; Gurfinkel, D.; Saville, A.W.; Vangala, S.; Rice, J.D.; Helmkamp, L.; Zimet, G.D.; Valderrama, R.; Breck, A.; et al. Prevalence and Characteristics of HPV Vaccine Hesitancy among Parents of Adolescents across the US. Vaccine 2020, 38, 6027–6037. [Google Scholar] [CrossRef] [PubMed]
- Nour, R.; Powell, L.; Alnakhi, W.K.; Mamdouh, H.; Zidoun, Y.; Hussain, H.Y.; Al Suwaidi, H.; Zary, N. Adult Vaccine Hesitancy Scale in Arabic and French: Protocol for Translation and Validation in the World Health Organization Eastern Mediterranean Region. JMIR Res. Protoc. 2022, 11, e36928. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Ogólnopolski Panel Badawczy, Sp. z o.o. Available online: https://panelariadna.pl/contact (accessed on 10 July 2022).
- Ariadna Ogólnopolski Panel Badawczy. Available online: https://panelariadna.pl/ (accessed on 2 July 2022).
- Gumiński, M.; Guzowski, W.; Huet, M.; Mariola, K.; Mordan, P.; Orczykowska, M. Information Society in Poland in 2021; Statistics Poland: Warsaw, Poland, 2022. [Google Scholar]
- HLS-EU Consortium. The European Health Literacy Project Comparative Report on Health Literacy in Eight EU Member States—The European Health Literacy Survey HLS-EU; HLS-EU Consortium: Maastricht, The Netherlands, 2012. [Google Scholar]
- Duplaga, M.; Sobecka, K.; Wójcik, S. The Reliability and Validity of the Telephone-Based and Online Polish Ehealth Literacy Scale Based on Two Nationally Representative Samples. Int. J. Environ. Res. Public Health 2019, 16, 3216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelikan, J.M.; Röthlin, F.; Ganahl, K. Measuring Comprehensive Health Literacy in General Populations: Validation of Instrument, Indices and Scales of the HLS-EU Study. In Proceedings of the 6th Annual Health Literacy Research Conference, Bethesda, MD, USA, 3–4 November 2014. [Google Scholar]
- World Health Organization. Process of Translation and Adaptation of Instruments; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Hutcheson, G.; Sofroniou, N. The Multivariate Social Scientist: Introductory Statistics Using Generalized Linear Models; Sage Publications: Thousand Oaks, CA, USA, 1999; ISBN 9780761952008. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 4th ed.; SAGE: London, UK, 2013. [Google Scholar]
- Child, D. The Essentials of Factor Analysis, 3rd ed.; Continuum: New York, NY, USA, 2006. [Google Scholar]
- Guadagnoli, E.; Velicer, W.F. Relation of Sample Size to the Stability of Component Patterns. Psychol. Bull. 1988, 103, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L. Figuring out Factors: The Use and Misuse of Factor Analysis. Can. J. Psychiatry 1994, 39, 135–140. [Google Scholar] [CrossRef]
- Domek, G.J.; O’Leary, S.T.; Bull, S.; Bronsert, M.; Contreras-Roldan, I.L.; Bolaños Ventura, G.A.; Kempe, A.; Asturias, E.J. Measuring Vaccine Hesitancy: Field Testing the WHO SAGE Working Group on Vaccine Hesitancy Survey Tool in Guatemala. Vaccine 2018, 36, 5273–5281. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hatcher, L.; O’Rourke, N. A Step-by-Step Approach to Using SAS for Factor Analysis and Structural Equation Modeling, 2nd ed.; SAS Institute Inc.: Cary, NC, USA, 2013; ISBN 978-1599942308. [Google Scholar]
- Tennant, A.; Pallant, J. The Root Mean Square Error of Approximation (RMSEA). Rasch Meas. Trans. 2012, 25, 1348–1349. [Google Scholar]
- Babyak, M.A.; Green, S.B. Confirmatory Factor Analysis: An Introduction for Psychosomatic Medicine Researchers. Psychosom. Med. 2010, 72, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-Square for Model Fit in Confirmatory Factor Analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [Green Version]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Sowa, P.; Kiszkiel, Ł.; Laskowski, P.P.; Alimowski, M.; Szczerbiński, Ł.; Paniczko, M.; Moniuszko-Malinowska, A.; Kamiński, K. COVID-19 Vaccine Hesitancy in Poland—Multifactorial Impact Trajectories. Vaccines 2021, 9, 876. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Issa, J.; Hussain, S.; Tanasiewicz, M.; Wojtyczka, R.; Kubina, R.; Konwinska, M.D.; Riad, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Professionals and Students in Poland: Cross-Sectional Survey-Based Study. Front. Public Health 2022, 10, 2391. [Google Scholar] [CrossRef] [PubMed]
- Kuciel, N.; Mazurek, J.; Hap, K.; Marciniak, D.; Biernat, K.; Sutkowska, E. COVID-19 Vaccine Acceptance in Pregnant and Lactating Women and Mothers of Young Children in Poland. Int. J. Womens Health 2022, 14, 415–424. [Google Scholar] [CrossRef]
- Jastrzẹbska, A.; Saden, G.; Knysz, B.; Pondel, M.; Siennicka, A. The Relationship between Knowledge about the Pandemic and Willingness to Get Vaccinated against SARS-CoV-2 in Medical Students in Poland: A Cross-Sectional Survey. Front. Public Health 2022, 10, 2778. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Variable Categories | All Respondents (n = 2189) | Subset 1 (n = 1082) | Subset 2 (n = 1107) | |||
|---|---|---|---|---|---|---|---|
| % | n | % | n | % | n | ||
| Gender | Female | 51.2 | 1121 | 51.7 | 559 | 50.8 | 562 |
| Male | 48.8 | 1068 | 48.3 | 523 | 49.2 | 545 | |
| Place of residence | Rural | 37.87 | 829 | 36.9 | 399 | 38.8 | 430 |
| urban below 20,000 inhabitants | 12.84 | 281 | 14.1 | 153 | 11.6 | 128 | |
| urban 20,000–100,000 inhabitants | 20.15 | 441 | 20.1 | 217 | 20.2 | 224 | |
| urban 100,000–200,000 inhabitants | 8.59 | 188 | 9.2 | 100 | 7.9 | 88 | |
| urban 200,000–500,000 inhabitants | 8.73 | 191 | 7.9 | 86 | 9.5 | 105 | |
| urban above 500,000 inhabitants | 11.83 | 259 | 11.7 | 127 | 11.9 | 132 | |
| Education | lower than secondary | 13.8 | 301 | 13.2 | 143 | 14.3 | 158 |
| secondary vocational | 24.4 | 535 | 23.5 | 254 | 25.4 | 281 | |
| Secondary | 35.7 | 781 | 38.5 | 417 | 32.9 | 364 | |
| University | 26.1 | 572 | 24.8 | 268 | 27.5 | 304 | |
| Net monthly household income | not more than 500 PLN | 1.74 | 38 | 2.0 | 22 | 1.4 | 16 |
| 501–1000 PLN | 5.25 | 115 | 5.3 | 57 | 5.2 | 58 | |
| 1001–1500 PLN | 8.77 | 192 | 9.2 | 100 | 8.3 | 92 | |
| 1501–2000 PLN | 14.80 | 324 | 15.5 | 168 | 14.1 | 156 | |
| 2001–3000 PLN | 21.52 | 471 | 21.3 | 231 | 21.7 | 240 | |
| 3001–4000 PLN | 12.97 | 284 | 13.4 | 145 | 12.6 | 139 | |
| more than 4000 PLN | 13.57 | 297 | 12.9 | 140 | 14.2 | 157 | |
| not revealed | 21.38 | 468 | 20.2 | 219 | 22.5 | 249 | |
| Vocational status | employee | 50.43 | 1104 | 50.8 | 550 | 50.0 | 554 |
| self-employed or farmer | 7.26 | 159 | 6.2 | 67 | 8.3 | 92 | |
| retired or on a disability pension | 21.06 | 461 | 20.8 | 225 | 21.3 | 236 | |
| high school or university student | 4.80 | 105 | 5.4 | 58 | 4.2 | 47 | |
| vocationally passive incl. unemployed | 9.82 | 215 | 10.0 | 108 | 9.7 | 107 | |
| a part-time job or other | 6.62 | 145 | 6.8 | 74 | 6.4 | 71 | |
| Marital status | single | 22.70 | 497 | 23.1 | 250 | 22.3 | 247 |
| married | 53.86 | 1179 | 52.9 | 572 | 54.8 | 607 | |
| in partnership | 1.23 | 27 | 13.0 | 141 | 12.7 | 141 | |
| widowed | 3.97 | 87 | 3.6 | 39 | 4.3 | 48 | |
| divorced or separated | 6.58 | 144 | 13.80 | 80 | 14.30 | 64 | |
| Item | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 |
|---|---|---|---|---|---|---|---|---|---|
| item 2 | 0.791 | ||||||||
| item 3 | 0.810 | 0.774 | |||||||
| item 4 | 0.769 | 0.737 | 0.749 | ||||||
| item 5 | 0.479 | 0.512 | 0.479 | 0.451 | |||||
| item 6 | 0.688 | 0.687 | 0.685 | 0.653 | 0.486 | ||||
| item 7 | 0.806 | 0.799 | 0.772 | 0.783 | 0.525 | 0.681 | |||
| item 8 | 0.695 | 0.690 | 0.715 | 0.699 | 0.428 | 0.652 | 0.712 | ||
| item 9 | 0.459 | 0.487 | 0.478 | 0.447 | 0.661 | 0.475 | 0.483 | 0.401 | |
| item 10 | 0.544 | 0.500 | 0.498 | 0.490 | 0.512 | 0.391 | 0.512 | 0.420 | 0.496 |
| Item | Mean after Removing an Item | The Variance of the Scale after Removing an Item | Item-Factor Correlation | Squared Item-Factor Correlation | Cronbach α after Removing an Item | Initial Communalities |
|---|---|---|---|---|---|---|
| item 1 | 22.57 | 56.080 | 0.843 | 0.776 | 0.924 | 0.776 |
| item 2 | 22.48 | 56.132 | 0.834 | 0.737 | 0.924 | 0.737 |
| item 3 | 22.57 | 55.870 | 0.830 | 0.744 | 0.924 | 0.744 |
| item 4 | 22.52 | 56.870 | 0.802 | 0.702 | 0.926 | 0.702 |
| item 5 | 21.91 | 58.342 | 0.625 | 0.520 | 0.935 | 0.520 |
| item 6 | 22.21 | 57.423 | 0.745 | 0.593 | 0.929 | 0.593 |
| item 7 | 22.55 | 55.654 | 0.848 | 0.768 | 0.923 | 0.768 |
| item 8 | 22.55 | 57.911 | 0.746 | 0.616 | 0.929 | 0.616 |
| item 9 | 21.76 | 57.791 | 0.600 | 0.497 | 0.937 | 0.497 |
| item 10 | 22.30 | 58.822 | 0.596 | 0.410 | 0.936 | 0.410 |
| Factor | Initial Eigenvalues | Sum of Squared Loading after Extraction | Sums of Squared Loadings after Rotation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulated % of Variance | Total | % of Variance | Cumulated % of Variance | Total | % of Variance | Cumulated % of Variance | |
| 1 | 6.48 | 64.75 | 64.75 | 6.17 | 61.74 | 61.74 | 4.68 | 46.83 | 46.83 |
| 2 | 1.05 | 10.51 | 75.26 | 0.72 | 7.17 | 68.90 | 2.21 | 22.08 | 68.90 |
| 3 | 0.58 | 5.82 | 81.07 | ||||||
| 4 | 0.35 | 3.50 | 84.57 | ||||||
| 5 | 0.35 | 3.45 | 88.02 | ||||||
| 6 | 0.34 | 3.36 | 91.38 | ||||||
| 7 | 0.27 | 2.65 | 94.04 | ||||||
| 8 | 0.23 | 2.32 | 96.36 | ||||||
| 9 | 0.19 | 1.92 | 98.28 | ||||||
| 10 | 0.17 | 1.72 | 100.00 | ||||||
| Item | Factor 1 | Factor 2 |
|---|---|---|
| item 1 | 0.844 | 0.318 |
| item 2 | 0.798 | 0.366 |
| item 3 | 0.820 | 0.327 |
| item 4 | 0.804 | 0.299 |
| item 5 | 0.277 | 0.790 |
| item 6 | 0.684 | 0.366 |
| item 7 | 0.818 | 0.365 |
| item 8 | 0.750 | 0.272 |
| item 9 | 0.271 | 0.746 |
| item 10 | 0.407 | 0.503 |
| Grouping Variable | Number of Respondents | ‘Confidence’ Subscore Mean (SD) | K-W Test H Statistic (p-Value) | ‘Risks’ Subscore Mean (SD) | K-W Test H Statistic (p-Value) | Total PL-aVHS Score Mean (SD) | K-W Test H Statistic (p-Value) |
|---|---|---|---|---|---|---|---|
| Status of vaccination against COVID-19 | |||||||
| subgroup 1 | 724 | 13.75 (4.78) 2,3,4 | 397.21 (<0.001) | 7.46 (2.53) 2,3,4 | 316.34 (<0.001) | 21.21 (6.47) 2,3,4 | 443.63 (<0.001) |
| subgroup 2 | 66 | 17.68 (4.00) 1,3,4 | 9.61 (1.76) 1,4 | 27.29 (4.80) 1,4 | |||
| subgroup 3 | 73 | 20.32 (3.61) 1,2 | 10.29 (1.55) 1 | 30.60 (4.02) 1 | |||
| subgroup 4 | 208 | 23.18 (5.89) 1,2 | 11.07 (2.30) 1,2 | 34.25 (7.15) 1,2 | |||
| Category of HL | |||||||
| subgroup 1 | 49 | 18.98 (7.29) 3 | 18.31 (<0.001) | 9.53 (2.87) 3 | 12.37 (0.002) | 28.51 (9.46) 2,3 | 18.73 (<0.001) |
| subgroup 2 | 450 | 16.36 (5.88) 3 | 8.66 (2.59) 3 | 25.02 (7.79) 1,3 | |||
| subgroup 3 | 402 | 15.33 (6.29) 1,2 | 8.18 (3.05) 1,2 | 23.51 (8.68) 1,2 | |||
| Indexes | Threshold Index Levels | One Factor Model (10 Items) | One Factor Model (9 Items) | Two-Factor Model (10 Items) | Two-Factor Model (9 Items without Item 10) |
|---|---|---|---|---|---|
| CDFR | <2.0 (p > 0.05) | 17.016 (<0.001) | 18.077 (<0.001) | 5.47 (<0.001) | 4.187 (<0.001) |
| NFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.927 | 0.937 | 0.977 | 0.986 |
| GFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.904 | 0.917 | 0.966 | 0.979 |
| AGFI | Acceptable: ≥0.90 to <0.95, good: ≥0.95 | 0.849 | 0.861 | 0.946 | 0.964 |
| CFI | Acceptable: 0.90–0.95, good: >0.95 | 0.931 | 0.940 | 0.981 | 0.989 |
| TLI | Acceptable: 0.90–0.95, good: >0.95 | 0.911 | 0.920 | 0.975 | 0.985 |
| RMSEA (90%CI) | Acceptable: <0.08 to 0.05, good: <0.05 | 0.120 (0.112–129) | 0.124 (0.115–0.134) | 0.064 (0.055–0.073) | 0.054 (0.043–0.064) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duplaga, M.; Zwierczyk, U.; Kowalska-Duplaga, K. The Assessment of the Reliability and Validity of the Polish Version of the Adult Vaccine Hesitancy Scale (PL-aVHS) in the Context of Attitudes toward COVID-19 Vaccination. Vaccines 2022, 10, 1666. https://doi.org/10.3390/vaccines10101666
Duplaga M, Zwierczyk U, Kowalska-Duplaga K. The Assessment of the Reliability and Validity of the Polish Version of the Adult Vaccine Hesitancy Scale (PL-aVHS) in the Context of Attitudes toward COVID-19 Vaccination. Vaccines. 2022; 10(10):1666. https://doi.org/10.3390/vaccines10101666
Chicago/Turabian StyleDuplaga, Mariusz, Urszula Zwierczyk, and Kinga Kowalska-Duplaga. 2022. "The Assessment of the Reliability and Validity of the Polish Version of the Adult Vaccine Hesitancy Scale (PL-aVHS) in the Context of Attitudes toward COVID-19 Vaccination" Vaccines 10, no. 10: 1666. https://doi.org/10.3390/vaccines10101666