
An Immune Response to Heterologous ChAdOx1/BNT162b2 Vaccination against COVID-19: Evaluation of the anti-RBD Specific IgG Antibodies Titers and Interferon Gamma Release Assay (IGRA) Test Results
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
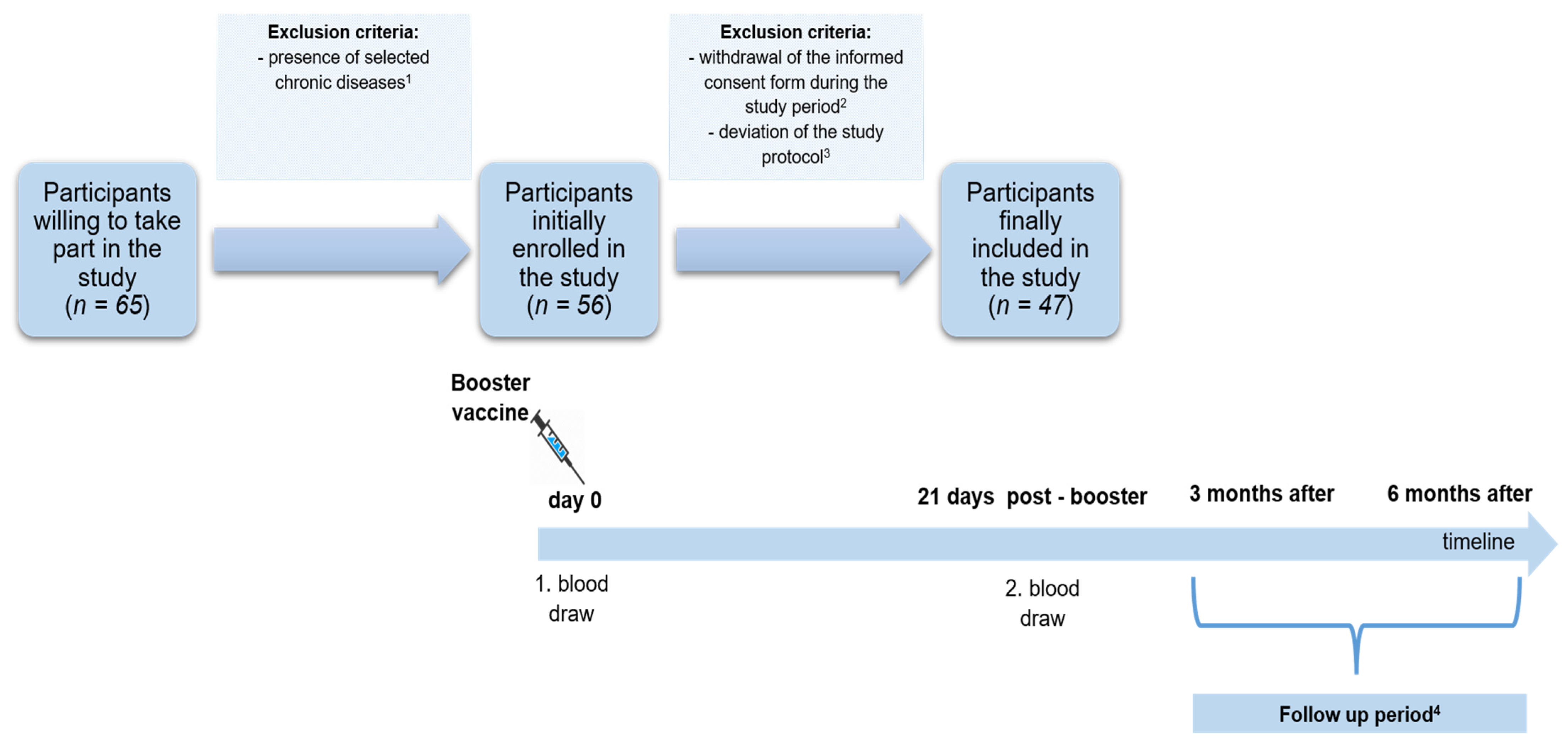
2.1. The Study Group
2.2. Laboratory Tests
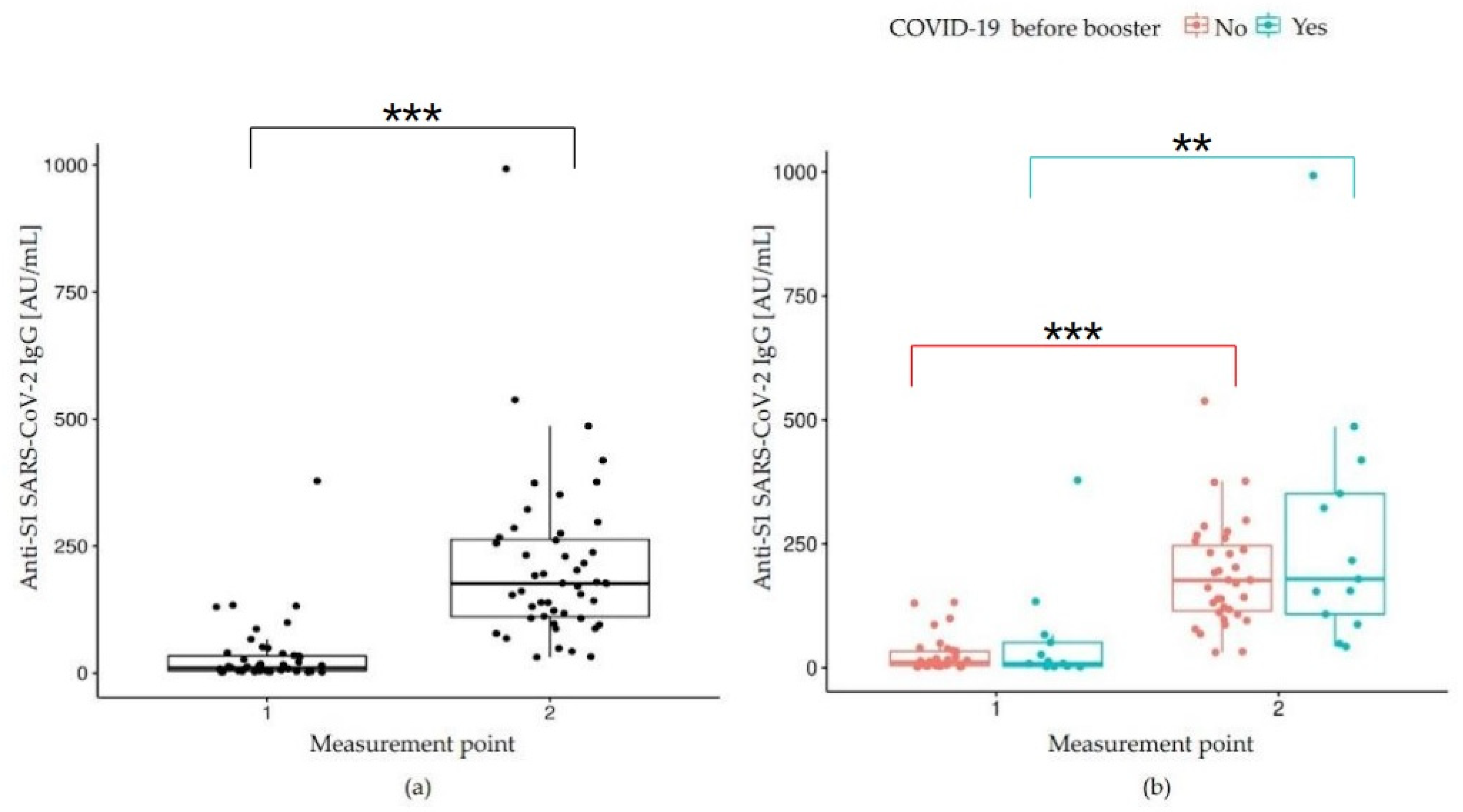
2.2.1. Humoral Immune Response: Anti-SARS-CoV-2 IgG Measurement
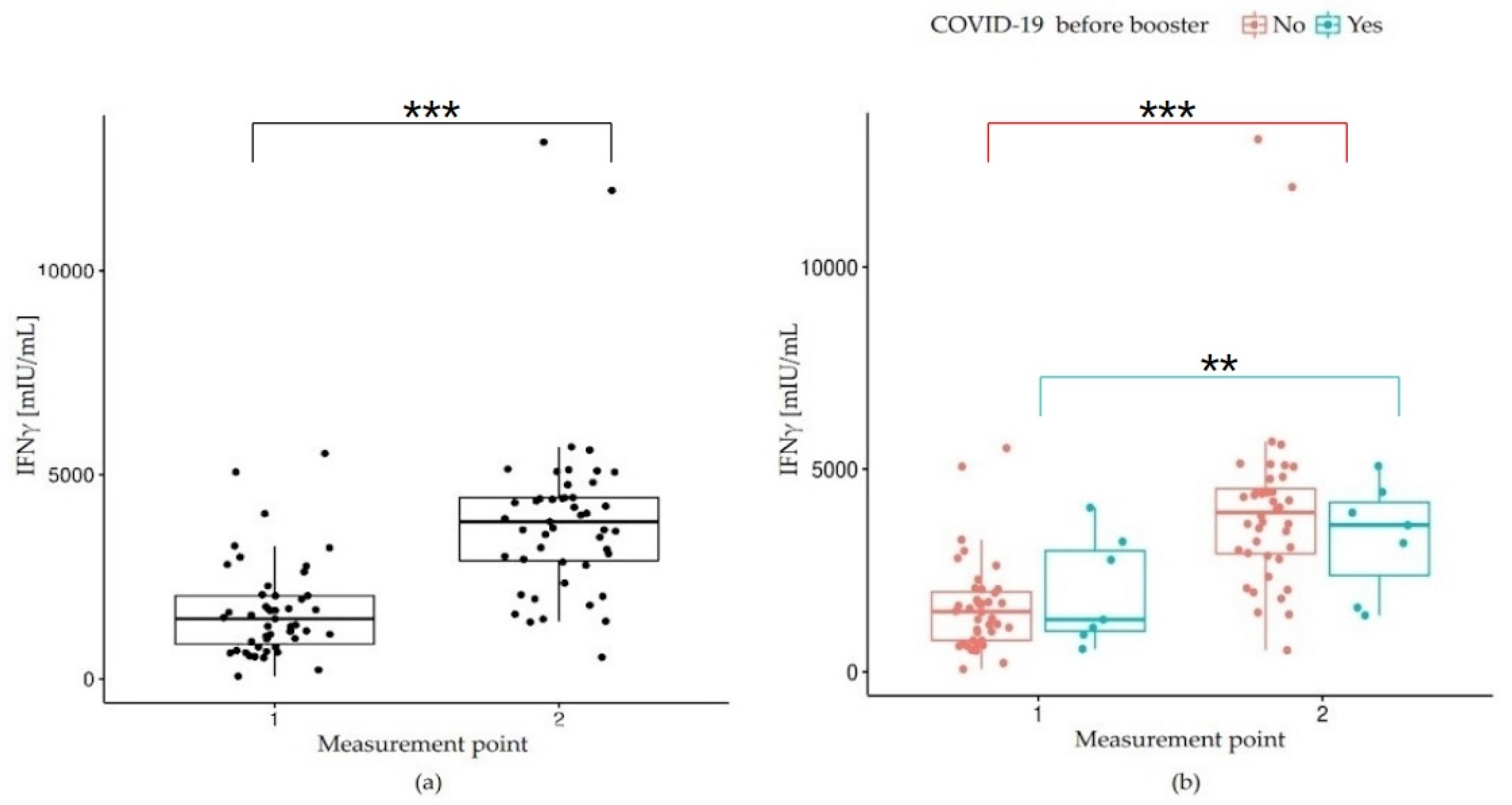
2.2.2. Cellular Immune Response: Quantitative Determination of IFN-γ Release by SARS-CoV-2-Specific T Cells
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Study limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- World Health Organization website: Origin of SARS-CoV-2. Available online: https://apps.who.int/iris/bitstream/handle/10665/332197/WHO-2019-nCoV-FAQ-Virus_origin-2020.1-eng.pdf (accessed on 26 March 2020).
- World Health Organization website: WHO Director-General’s Opening Remarks at the Media Briefing on COVID19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 2 May 2021).
- World Health Organization Website: WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 8 September 2022).
- Sacco, P.L.; De Domenico, M. Public Health Challenges and Opportunities after COVID-19. Bull. World Health Organ. 2021, 99, 529–535. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control: COVID-19. Situation Updates on COVID-19. SARS-CoV-2 Variants of Concern. 28 July 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 29 July 2022).
- Loconsole, D.; Centrone, F.; Morcavallo, C.; Campanella, S.; Accogli, M.; Sallustio, A.; Peccarisi, D.; Stufano, A.; Lovreglio, P.; Chironna, M. Changing Features of COVID-19: Characteristics of Infections with the SARS-CoV-2 Delta (B.1.617.2) and Alpha (B.1.1.7) Variants in Southern Italy. Vaccines 2021, 9, 1354. [Google Scholar] [CrossRef]
- Shehata, M.M.; Mahmoud, S.H.; Tarek, M.; Al-Karmalawy, A.A.; Mahmoud, A.; Mostafa, A.; Elhefnawi, M.; Ali, M.A. In Silico and In Vivo Evaluation of SARS-CoV-2 Predicted Epitopes-Based Candidate Vaccine. Molecules 2021, 26, 6182. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Napoli, R.D. Features, Evaluation, and Treatment of Coronavirus (COVID-19) StatPearles. Treasure Island (FL): StatPearls Publishing January 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554776/#_NBK554776_pubdet_ (accessed on 30 June 2022).
- Fiske, A.; Schönweitz, F.; Eichinger, J.; Zimmermann, B.; Hangel, N.; Sierawska, A.; McLennan, S.; Buyx, A. The COVID-19 Vaccine: Trust, Doubt, and Hope for a Future beyond the Pandemic in Germany. PLoS ONE 2022, 17, e0266659. [Google Scholar] [CrossRef]
- Paul, K.T.; Zimmermann, B.M.; Corsico, P.; Fiske, A.; Geiger, S.; Johnson, S.; Kuiper, J.M.L.; Lievevrouw, E.; Marelli, L.; Prainsack, B.; et al. Anticipating Hopes, Fears and Expectations towards COVID-19 Vaccines: A Qualitative Interview Study in Seven European Countries. SSM—Qual. Res. Health 2022, 2, 100035. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 3099, 1293–1302. [Google Scholar] [CrossRef]
- COVID-19 Vaccine AstraZeneca. Product Information as Approved by the CHMP on 29 January 2021, Pending Endorsement by the European Commission. Available online: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-astrazeneca-product-information-approved-chmp-29-january-2021-pending-endorsement_en.pdf (accessed on 29 March 2022).
- GOV UK. Available online: https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for-covid-19/summary-of-product-characteristics-for-covid-19-vaccine-pfizerbiontech (accessed on 7 July 2022).
- Centers for Disease Control and Prevention. Moderna COVID-19 Vaccine (also Known as Spikevax): Overview and Safety. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Moderna.html. (accessed on 14 July 2022).
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the ChAdOx1 NCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning immune humoral response to BNT162b2 COVID-19 vaccine over 6 months. N. Engl. J. Med. 2021, 285, e84. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, 24.e85. [Google Scholar] [CrossRef] [PubMed]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of Effectiveness of Vaccines against SARS-CoV-2 Infection and COVID-19 Disease: Results of a Systematic Review and Meta-Regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after Covid-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 2534–2535. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, R.A.; Qamar, M.A.; Gilani, J.A.; Irfan, O.; Waqar, U.; Sajid, M.I.; Mahmood, S.F. The Mystery of COVID-19 Reinfections: A Global Systematic Review and Meta-Analysis. Ann. Med. Surg. 2021, 72, 103130. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Wang, W.; Ma, J.; Wu, S.; Sun, F. Reinfection Rates among Patients Previously Infected by SARS-CoV-2: Systematic Review and Meta-Analysis. Chin. Med. J. 2022, 135, 145–152. [Google Scholar] [CrossRef]
- University of Birmingham: Study Shows Low or Undetectable Immune Response to Double COVID-19 in Patients with Impaired Immune System. Preliminary Results of The OCTAVE Study. Available online: https://www.birmingham.ac.uk/news/2021/study-shows-low-or-undetectable-immune-response-to-double-covid-19-vaccination-in-patients-with-impaired-immune-systems-1 (accessed on 24 August 2021).
- Falahi, S.; Kenarkoohi, A. Host Factors and Vaccine Efficacy: Implications for COVID-19 Vaccines. J. Med. Virol. 2022, 94, 1330–1335. [Google Scholar] [CrossRef]
- Madison, A.A.; Shrout, M.R.; Renna, M.E.; Kiecolt-Glaser, J.K. Psychological and Behavioral Predictors of Vaccine Efficacy: Considerations for COVID-19. Perspect. Psychol. Sci. 2021, 16, 191–203. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention: COVID-19 Vaccine Boosters. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 20 July 2022).
- European Center for Disease Control and Prevention: Vaccines. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/vaccines (accessed on 21 January 2022).
- World Health Organization Website: Interim Statement on the Use of Additional Booster Doses of Mergency Use Listed mRNA Vaacines Against COVID-19. Available online: https://www.who.int/news/item/17-05-2022-interim-statement-on-the-use-of-additional-booster-doses-of-emergency-use-listed-mrna-vaccines-against-covid-19 (accessed on 17 May 2022).
- World Health Organization website: Corrigenda for the WHO SAGE Roadmap for Prioritizing Uses of COVID-19 Vaccines. Available online: https://www.who.int/publications/m/item/corrigenda-for-the-who-sage-roadmap-for-prioritizing-uses-of-covid-19-vaccines (accessed on 31 January 2022).
- European Medicines Agency Heterologous Primary and Booster COVID-19 Vaccination Evidence Based Regulatory Considerations. Available online: https://www.ema.europa.eu/en/documents/report/heterologous-primary-booster-covid-19-vaccination-evidence-based-regulatory-considerations_en.pdf (accessed on 2 August 2022).
- Borobia, A.M.; Carcas, A.J.; Pérez-Olmeda, M.; Castaño, L.; Bertran, M.J.; García-Pérez, J.; Campins, M.; Portolés, A.; González-Pérez, M.; García Morales, M.T.; et al. Immunogenicity and Reactogenicity of BNT162b2 Booster in ChAdOx1-S-Primed Participants (CombiVacS): A Multicentre, Open-Label, Randomised, Controlled, Phase 2 Trial. Lancet 2021, 398, 121–130. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu-Omar, A.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and Reactogenicity of Heterologous ChAdOx1 NCoV-19/MRNA Vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef]
- Chiu, N.C.; Chi, H.; Tu, Y.K.; Huang, Y.N.; Tai, Y.L.; Weng, S.L.; Chang, L.; Huang, D.T.N.; Huang, F.Y.; Lin, C.Y. To Mix or Not to Mix? A Rapid Systematic Review of Heterologous Prime–Boost Covid-19 Vaccination. Expert Rev. Vaccines 2021, 20, 1211–1220. [Google Scholar] [CrossRef]
- Voysey, M.; Costa Clemens, S.A.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Single-Dose Administration and the Influence of the Timing of the Booster Dose on Immunogenicity and Efficacy of ChAdOx1 NCoV-19 (AZD1222) Vaccine: A Pooled Analysis of Four Randomised Trials. Lancet 2021, 397, 881–891. [Google Scholar] [CrossRef]
- Van Gils, M.J.; Lavell, A.; van der Straten, K.; Appelman, B.; Bontjer, I.; Poniman, M.; Burger, J.A.; Oomen, M.; Bouhuijs, J.H.; van Vught, L.A.; et al. Antibody Responses against SARS-CoV-2 Variants Induced by Four Different SARS-CoV-2 Vaccines in Health Care Workers in the Netherlands: A Prospective Cohort Study. PLoS Med. 2022, 19, e1003991. [Google Scholar] [CrossRef] [PubMed]
- Al-Karmalawy, A.A.; Soltane, R.; Abo Elmaaty, A.; Tantawy, M.A.; Antar, S.A.; Yahya, G.; Chrouda, A.; Pashameah, R.A.; Mustafa, M.; Abu Mraheil, M.; et al. Coronavirus Disease (COVID-19) Control between Drug Repurposing and Vaccination: A Comprehensive Overview. Vaccines 2021, 9, 1317. [Google Scholar] [CrossRef] [PubMed]
- Ashour, N.A.; Elmaaty, A.A.; Sarhan, A.A.; Elkaeed, E.B.; Moussa, A.M.; Erfan, I.A.; Al-Karmalawy, A.A. A Systematic Review of the Global Intervention for SARS-CoV-2 Combating: From Drugs Repurposing to Molnupiravir Approval. Drug Des. Devel. Ther. 2022, 16, 685. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 Vaccine and Correlates of Humoral Immune Responses and Dynamics: A Prospective, Single-Centre, Longitudinal Cohort Study in Health-Care Workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Lange, A.; Borowik, A.; Bocheńska, J.; Rossowska, J.; Jaskuła, E. Immune Response to Covid-19 Mrna Vaccine—a Pilot Study. Vaccines 2021, 9, 2–9. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the MRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Tretyn, A.; Szczepanek, J.; Skorupa, M.; Jarkiewicz-Tretyn, J.; Sandomierz, D.; Dejewska, J.; Ciechanowska, K.; Jarkiewicz-Tretyn, A.; Koper, W.; Pałgan, K. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-Covid-19 Recovery or Post-Vaccination. Cells 2021, 10, 1952. [Google Scholar] [CrossRef]
- Zheng, J.; Deng, Y.; Zhao, Z.; Mao, B.; Lu, M.; Lin, Y.; Huang, A. Characterization of SARS-CoV-2-specific humoral immunity and its potential applications and therapeutic prospects. Cell. Mol. Immunol. 2022, 19, 150–157. [Google Scholar] [CrossRef]
- Woldemeskel, B.A.; Kwaa, A.K.; Garliss, C.C.; Laeyendecker, O.; Ray, S.C.; Blankson, J.N. Healthy Donor T Cell Responses to Common Cold Coronaviruses and SARS-CoV-2. J. Clin. Investig. 2020, 130, 6631–6638. [Google Scholar] [CrossRef]
- Technology Networks Immunology & Microbioloby: EUROIMMUN Launches SARS-CoV-2 Test System to Detect T-Cell Response. Available online: https://www.technologynetworks.com/immunology/product-news/euroimmun-launches-sars-cov-2-test-system-to-detect-t-cell-response-344589 (accessed on 2 August 2022).
- ACCESS SARS-CoV-2 IgG—Instructions for Use (Ref. no. C58961). Available online: https://www.fda.gov/media/139627/download (accessed on 2 March 2022).
- Quan-T-Cell SARS-CoV-2 & Quan-T-Cell ELISA. EUROIMMUN, Medizinische Labordiagnostika AG, Lübeck, Germany. Available online: https://www.coronavirusdiagnostics.com/documents/Indications/Infections/Coronavirus/ET_2606_D_UK_A.pdf (accessed on 1 August 2022).
- RStudio Team. RStudio: Integrated Development for R. RStudio, PBC, Boston, 2020. Available online: http://www.rstudio.com/ (accessed on 1 July 2022).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; p. 2. [Google Scholar]
- Painter, S.D.; Ovsyannikova, I.G.; Poland, G.A. The weight of obesity on the human immune response to vaccination. HHS Public Access. Vaccine 2015, 33, 4422–4429. [Google Scholar] [CrossRef] [Green Version]
- Golec, M.; Fronczek, M.; Zembala-John, J.; Chrapiec, M.; Konka, A.; Wystyrk, K.; Botor, H.; Brzoza, Z.; Kasperczyk, S.; Bułdak, R.J. Early and Longitudinal Humoral Response to the SARS-CoV-2 MRNA BNT162b2 Vaccine in Healthcare Workers: Significance of BMI, Adipose Tissue and Muscle Mass on Long-Lasting Post-Vaccinal Immunity. Viruses 2022, 14, 868. [Google Scholar] [CrossRef] [PubMed]
- Soegiarto, G.; Wulandari, L.; Purnomosari, D.; Fahmita, K.D.; Gautama, H.I.; Hadmoko, S.; Prasetyo, M.E.; Mahdi, B.A.; Arafah, N.; Prasetyaningtyas, D.; et al. Hypertension Is Associated with Antibody Response and Breakthrough Infection in Health Care Workers Following Vaccination with Inactivated SARS-CoV-2. Vaccine 2022, 40, 4046–4056. [Google Scholar] [CrossRef] [PubMed]
- Strzelak, A.; Ratajczak, A.; Adamiec, A.; Feleszko, W. Tobacco Smoke Induces and Alters Immune Responses in the Lung Triggering Inflammation, Allergy, Asthma and Other Lung Diseases: A Mechanistic Review. Int. J. Environ. Res. Public Health 2018, 15, 1033. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Gianfredi, V.; Tomaselli, V.; Polosa, R. The Effect of Smoking on Humoral Response to COVID-19 Vaccines: A Systematic Review of Epidemiological Studies. Vaccines 2022, 10, 303. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 w Polsce, 2022. Available online: https://sarswpolsce (accessed on 13 May 2022).
- Sette, A.; Crotty, S. Adaptive Immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef] [PubMed]
- Jakóbisiak, M. Główne Komponenty i Zasadnicze Cechy Odpowiedzi Immunologicznej. Immunologia; Gołąb, J., Jakóbisiak, M., Lasek, W., Stokłosa, T., Eds.; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2009; pp. 3–5. [Google Scholar]
- Brand, I.; Gilberg, L.; Bruger, J.; Garí, M.; Wieser, A.; Eser, T.M.; Frese, J.; Ahmed, M.I.M.; Rubio-Acero, R.; Guggenbuehl Noller, J.M.; et al. Broad T Cell Targeting of Structural Proteins After SARS-CoV-2 Infection: High Throughput Assessment of T Cell Reactivity Using an Automated Interferon Gamma Release Assay. Front. Immunol. 2021, 12, 688436. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Raza, H.A.; Sen, P.; Bhatti, O.A.; Gupta, L. Sex hormones, autoimmunity and gender disparity in COVID-19. Rheumatol. Int. 2021, 41, 1375–1386. [Google Scholar] [CrossRef]
- Barin, B.; Kasap, U.; Selçuk, F.; Volkan, E.; Uluçkan, Ö. Comparison of SARS-CoV-2 anti-spike receptor binding domain IgG antibody responses after CoronaVac, BNT162b2, ChAdOx1 COVID-19 vaccines, and a single booster dose: A prospective, longitudinal population-based study. Lancet Microbe 2022, 3, e274–e283. [Google Scholar] [CrossRef]
- Chen, Z.; Wherry, E.J. T cell responses in patients with COVID-19. Nat. Rev. Immunol. 2020, 20, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Schiffner, J.; Backhaus, I.; Rimmele, J.; Schulz, S.; Möhlenkamp, T.; Klemens, J.M.; Zapf, D.; Solbach, W.; Mischnik, A. Long-Term Course of Humoral and Cellular Immune Responses in Outpatients After SARS-CoV-2 Infection. Front. Public Health 2021, 9, 1378. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, A.; Marchevsky, N.; Jenkin, D.; Aboagye, J.; Aley, P.; Angus, B.; Belij-Rammerstorfer, S.; Bibi, S.; Bittaye, M.; Cappuccini, F.; et al. Reactogenicity and immunogenicity after a late second dose or a third dose of chadox1 ncov-19 in the uk: A substudy of two randomised controlled trials (cov001 and cov002). Lancet 2021, 398, 981–990. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and Immunogenicity of Seven COVID-19 Vaccines as a Third Dose (Booster) Following Two Doses of ChAdOx1 NCov-19 or BNT162b2 in the UK (COV-BOOST): A Blinded, Multicentre, Randomised, Controlled, Phase 2 Trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Hasan, A.; Al-Ozairi, E.; Al-Baqsumi, Z.; Ahmad, R.; Al-Mulla, F. Cellular and Humoral Immune Responses in Covid-19 and Immunotherapeutic Approaches. Immunotargets Ther. 2021, 10, 63–85. [Google Scholar] [CrossRef]
- Danese, E.; Montagnana, M.; Salvagno, G.L.; Gelati, M.; Peserico, D.; Pighi, L.; De Nitto, S.; Henry, B.M.; Porru, S.; Lippi, G. Comparison of Five Commercial Anti-Sars-Cov-2 Total Antibodies and Igg Immunoassays after Vaccination with Bnt162b2 Mrna. J. Med. Biochem. 2021, 40, 335–340. [Google Scholar] [CrossRef]
- Šimánek, V.; Pecen, L.; Krátká, Z.; Fürst, T.; Řezáčková, H.; Topolčan, O.; Fajfrlík, K.; Sedláček, D.; Šín, R.; Pazdiora, P.; et al. Five Commercial Immunoassays for Sars-Cov-2 Antibody Determination and Their Comparison and Correlation with the Virus Neutralization Test. Diagnostics 2021, 11, 593. [Google Scholar] [CrossRef]
- Ju, B.; Zhang, Q.; Ge, J.; Wang, R.; Sun, J.; Ge, X.; Yu, J.; Shan, S.; Zhou, B.; Song, S.; et al. Human Neutralizing Antibodies Elicited by SARS-CoV-2 Infection. Nature 2020, 584, 115–119. [Google Scholar] [CrossRef]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and Decay of Human Antibody Responses to the Receptor Binding Domain of SARS-CoV-2 Spike Protein in COVID-19 Patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Website. Science Brief: COVID-19 Vaccines and Vaccination. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/fully-vaccinated-people.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fmore%2Ffully-vaccinated-people.html (accessed on 15 September 2021).
- Centers’ for Disease Control and Prevention Website. Science Brief: SARS-CoV-2 Infection-Induced and Vaccine-Induced Immunity. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/vaccine-induced-immunity.html (accessed on 29 October 2021).
- Pérez-Alós, L.; Armenteros, J.J.A.; Madsen, J.R.; Hansen, C.B.; Jarlhelt, I.; Hamm, S.R.; Heftdal, L.D.; Pries-Heje, M.M.; Møller, D.L.; Fogh, K.; et al. Modeling of Waning Immunity after SARS-CoV-2 Vaccination and Influencing Factors. Nat. Commun. 2022, 13, 1–11. [Google Scholar] [CrossRef]
- Rode, O.D.; Bodulić, K.; Zember, S.; Balent, N.C.; da Novokmet, A.; Čulo, M.; Rašić, Ž.; Mikulić, R.; Markotić, A. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines 2022, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-Antibody Waning after Second Dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef]
- United Nations Medical Directors Recommendations for Additional Vaccine and Booster Doses for COVID-19 Vaccinations. Updated 8 July, 2022. Available online: https://www.un.org/sites/un2.un.org/files/unmd_recommendations_for_additional_vaccine_and_booster_doses_covid-19_vaccination.pdf (accessed on 2 August 2022).
- Jeong, S.; Lee, N.; Lee, S.K.; Cho, E.-J.; Hyun, J.; Park, M.-J.; Song, W.; Kim, H.S. Humoral and Cellular Responses to BNT162b2 as a Booster Following Two Doses of ChAdOx1 NCov-19 Determined Using Three SARS-CoV-2 Antibody Assays and an Interferon-Gamma Release Assay: A Prospective Longitudinal Study in Healthcare Workers. Front. Immunol. 2022, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Imperial College London. Available online: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-49-omicron/ (accessed on 16 December 2021).
- Edara, V.V.; Manning, K.E.; Ellis, M.; Lai, L.; Moore, K.M.; Foster, S.L.; Floyd, K.; Davis-Gardner, M.E.; Mantus, G.; Nyhoff, L.E.; et al. MRNA-1273 and BNT162b2 MRNA Vaccines Have Reduced Neutralizing Activity against the SARS-CoV-2 Omicron Variant. Cell Rep. Med. 2022, 3, 100529. [Google Scholar]
- Chang, C.; Vlad, G.; Vasilescu, E.R.; Li, P.; Husain, S.A.; Silvia, E.; Cohen, D.J.; Ratner, L.E.; Sun, W.Z.; Mohan, S.; et al. Previous SARS-CoV-2 infection or a third dose of vaccine elicited cross-variant neutralising antibodies in vaccinated solid-organ transplant recipients. Clin. Transl. Immunol. 2022, 11, e1411. [Google Scholar] [CrossRef]
- Demonbreuna, A.R.; Sancilioc, A.; Veleza, M.P.; Ryan, D.T.; Saber, R.; Vaught, L.A.; Reisera, N.L.; Hsieha, R.R.; D’Aquilaf, R.T.; Mustanskie, B.; et al. Comparison of IgG and neutralizing antibody responses after one or two doses of COVID-19 mRNA vaccine in previously infected and uninfected individuals. EClinicalMedicine 2021, 38, 101018. [Google Scholar]
- Jagannathan, P.; Wang, T.T. Immunity after SARS-CoV-2 infections. Nat. Immunol. 2021, 22, 539–540. [Google Scholar]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; van Osch, J.A.T.; Dijkhuizen, E.; et al. SARS-CoV-2 Variants of Concern Partially Escape Humoral but Not T-Cell Responses in COVID-19 Convalescent Donors and Vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar]
- Tan, A.T.; Linster, M.; Tan, C.W.; Le Bert, N.; Chia, W.N.; Kunasegaran, K.; Zhuang, Y.; Tham, C.Y.L.; Chia, A.; Smith, G.J.D.; et al. Early Induction of Functional SARS-CoV-2-Specific T Cells Associates with Rapid Viral Clearance and Mild Disease in COVID-19 Patients. Cell Rep. 2021, 34I, 108728. [Google Scholar]
- Seraceni, S.; Zocca, E.; Cervone, T.E.; Tomassetti, F.; Polidori, I.; Valisi, M.; Broccolo, F.; Calugi, G.; Bernardini, S.; Pieri, M. T-Cell Assay after COVID-19 Vaccination Could Be a Useful Tool? A Pilot Study on Interferon-Gamma Release Assay in Healthcare Workers. Diseases 2022, 10, 49. [Google Scholar] [CrossRef]
- Nguyen, T.H.O.; Cohen, C.A.; Rowntree, L.C.; Bull, M.B.; Hachim, A.; Kedzierska, K.; Valkenburg, S.A. T Cells Targeting SARS-CoV-2: By Infection, Vaccination, and Against Future Variants. Front. Med. 2021, 8, 793102. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 28, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, P.S.; Wimmers, F.; Mok, C.K.P.; Perera, R.A.; Scott, M.; Hagan, T.; Sigal, N.; Feng, Y.; Bristow, L.; Tak-Yin Tsang, O.; et al. Systems biological assessment of immunity to mild versus severe COVID-19 infection in humans. Science 2020, 369, 1210–1220. [Google Scholar] [CrossRef] [PubMed]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, 6515. [Google Scholar] [CrossRef]
- Laing, A.G.; Lorenc, A.; del Molino del Barrio, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2020, 26, 1623–1635. [Google Scholar] [CrossRef]
- Aid, M.; Busman-Sahay, K.; Vidal, S.J.; Maliga, Z.; Bondoc, S.; Starke, C.; Terry, M.; Jacobson, C.A.; Wrijil, L.; Ducat, S.; et al. Vascular Disease and Thrombosis in SARS-CoV-2-Infected Rhesus Macaques. Cell 2020, 25, 1354–1366. [Google Scholar] [CrossRef]
- Kuri-Cervantes, L.; Pampena, M.B.; Meng, W.; Rosenfeld, A.M.; Ittner, C.A.G.; Weisman, A.R.; Agyekum, R.S.; Mathew, D.; Baxter, A.E.; Vella, L.A.; et al. Comprehensive mapping of immune perturbations associated with severe COVID-19. Sci. Immunol. 2020, 15, 49.eabd7114. [Google Scholar] [CrossRef]
- Li, S.; Jiang, L.; Li, X.; Lin, F.; Wang, Y.; Li, B.; Jiang, T.; An, W.; Liu, S.; Liu, H.; et al. Clinical and pathological investigation of patients with severe COVID-19. JCI Insight 2020, 5, 12. [Google Scholar] [CrossRef]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Eun Oh, J.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef]
- Radermecker, C.; Detrembleur, N.; Guiot, J.; Cavalier, E.; Henket, M.; d’Emal, C.; Vanwinge, C.; Cataldo, D.; Oury, C.; Delvenne, P.; et al. Neutrophil extracellular traps infiltrate the lung airway, interstitial, and vascular compartments in severe COVID-19. J. Exp. Med. 2020, 217, 12. [Google Scholar] [CrossRef]
- Schurink, B.; Roos, E.; Radonic, T.; Barbe, E.; Bouman, C.S.C.; de Boer, H.H.; de Bree, G.J.; Bulle, E.B.; Aronica, E.M.; Florquin, S.; et al. Viral presence and immunopathology in patients with lethal COVID-19: A prospective autopsy cohort study. Lancet Microbe. 2020, 1, e290–e299. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Bastard, P.; Liu, Z.; Le Pen, J.; Moncada-Velez, M.; Chen, J.; Ogishi, M.; Sabli, I.K.D.; Hodeib, S.; Korol, C.; et al. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 2020, 370, eabd4570. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, J.; Fischer, B.; Becher, H.; Becker, A.K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Cellular and Humoral Immune Response to a Third Dose of BNT162b2 COVID-19 Vaccine—A Prospective Observational Study. Front. Immunol. 2022, 13, 896151. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n | % | |
|---|---|---|---|
| Sex | male | 6 | 12.77 |
| female | 41 | 87.23 | |
| Age (years) | <60 | 42 | 89.36 |
| ≥60 | 5 | 10.64 | |
| BMI | underweight (<18.50) | 1 | 2.13 |
| normal body mass (18.50–24.99) | 30 | 63.82 | |
| overweight (25.00–29.99) | 10 | 21.28 | |
| obesity (≥30.00) | 6 | 12.77 | |
| Smoking | yes | 6 | 12.77 |
| no | 41 | 87.23 | |
| COVID-19 before a booster dose | yes | 13 | 27.66 |
| no | 34 | 72.34 | |
| COVID-19 after a booster dose | yes | 7 | 14.89 |
| no | 40 | 85.11 | |
| Parameter | Range | n (%) 47 (100.00%) | Mean ± SD | Median (Q1; Q3) | p-Value |
|---|---|---|---|---|---|
| IgG before a booster (AU/mL) | <10.00 | 24 (51.06) | 33.06 ± 61.90 | 10.38 (4.35; 34.34) | p < 0.001 |
| ≥10.00 | 23 (48.94) | ||||
| IgG after a booster (AU/mL) | <10.00 | 0 (0.00) | 211.41 ± 162.96 | 176.65 (110.00; 264.45) | |
| ≥10.00 | 47 (100.00) | ||||
| IFNγ before a booster (mIU/mL) | <100.00 | 1 (2.13) | 1664.16 ± 1158.19 | 1472.43 (777.76; 2037.33) | p < 0.001 |
| 100.00–200.00 | 0 (0.00) | ||||
| >200.00 | 46 (97.87) | ||||
| IFNγ after a booster (mIU/mL) | <100.00 | 0 (0.00) | 3975.47 ± 2198.65 | 3890.92 (2897.18; 4601.09) | |
| 100.00–200.00 | 0 (0.00) | ||||
| >200.00 | 47 (100.00) |
| SARS-CoV-2 Infection before a Booster Dose | ||||
|---|---|---|---|---|
| Yes n = 13 (27.66%) | No n = 34 (72.34%) | Yes Vs. No | ||
| Parameter | Estimation point | Median (Q1; Q3) | Median (Q1; Q3) | p-value ** |
| IgG (AU/mL) | Before a booster (1) | 8.62 (3.05; 51.25) | 11.22 (4.50; 33.81) | p > 0.05 |
| After a booster (2) | 179.05 (108.22; 351.25) | 176.40 (111.77; 255.47) | p > 0.05 | |
| p-value * | p = 0.002 | p < 0.001 | ||
| IFNγ (mIU/mL) | Before a booster (1) | 1673.92 (1093.17; 2622.30) | 1291.26 (696.22; 1951.83) | p > 0.05 |
| After a booster (2) | 4414.46 (4231.84; 5095.95) | 3540.81 (2347.16; 4426.45) | p = 0.348 | |
| p-value * | p = 0.001 | p < 0.001 | ||
| Follow-Up Period | |||
|---|---|---|---|
| Follow-Up Outcomes | Early FU (<21 Days) | Intermediate FU (≥21 Days–3 Months) | Late FU (≥3–6 Months) |
| SARS-CoV-2 infection n (%) | 1 (2.13) | 6 (12.77) | 0 (0.00) |
| death n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zalewska, M.; Fus, W.; Konka, A.; Wystyrk, K.; Bochenek, A.; Botor, H.; Fronczek, M.; Zembala-John, J.; Adamek, B. An Immune Response to Heterologous ChAdOx1/BNT162b2 Vaccination against COVID-19: Evaluation of the anti-RBD Specific IgG Antibodies Titers and Interferon Gamma Release Assay (IGRA) Test Results. Vaccines 2022, 10, 1546. https://doi.org/10.3390/vaccines10091546
Zalewska M, Fus W, Konka A, Wystyrk K, Bochenek A, Botor H, Fronczek M, Zembala-John J, Adamek B. An Immune Response to Heterologous ChAdOx1/BNT162b2 Vaccination against COVID-19: Evaluation of the anti-RBD Specific IgG Antibodies Titers and Interferon Gamma Release Assay (IGRA) Test Results. Vaccines. 2022; 10(9):1546. https://doi.org/10.3390/vaccines10091546
Chicago/Turabian StyleZalewska, Marzena, Wiktoria Fus, Adam Konka, Karolina Wystyrk, Aneta Bochenek, Hanna Botor, Martyna Fronczek, Joanna Zembala-John, and Brygida Adamek. 2022. "An Immune Response to Heterologous ChAdOx1/BNT162b2 Vaccination against COVID-19: Evaluation of the anti-RBD Specific IgG Antibodies Titers and Interferon Gamma Release Assay (IGRA) Test Results" Vaccines 10, no. 9: 1546. https://doi.org/10.3390/vaccines10091546