
Immune Response after mRNA COVID-19 Vaccination in Lung Transplant Recipients: A 6-Month Follow-Up

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Sample Collection
3. Anti-SARS-CoV-2 Testing
4. Peptides
5. IFN-γ ELISpot Assay
6. Statistical Analysis
7. Results
7.1. Patient Characteristics
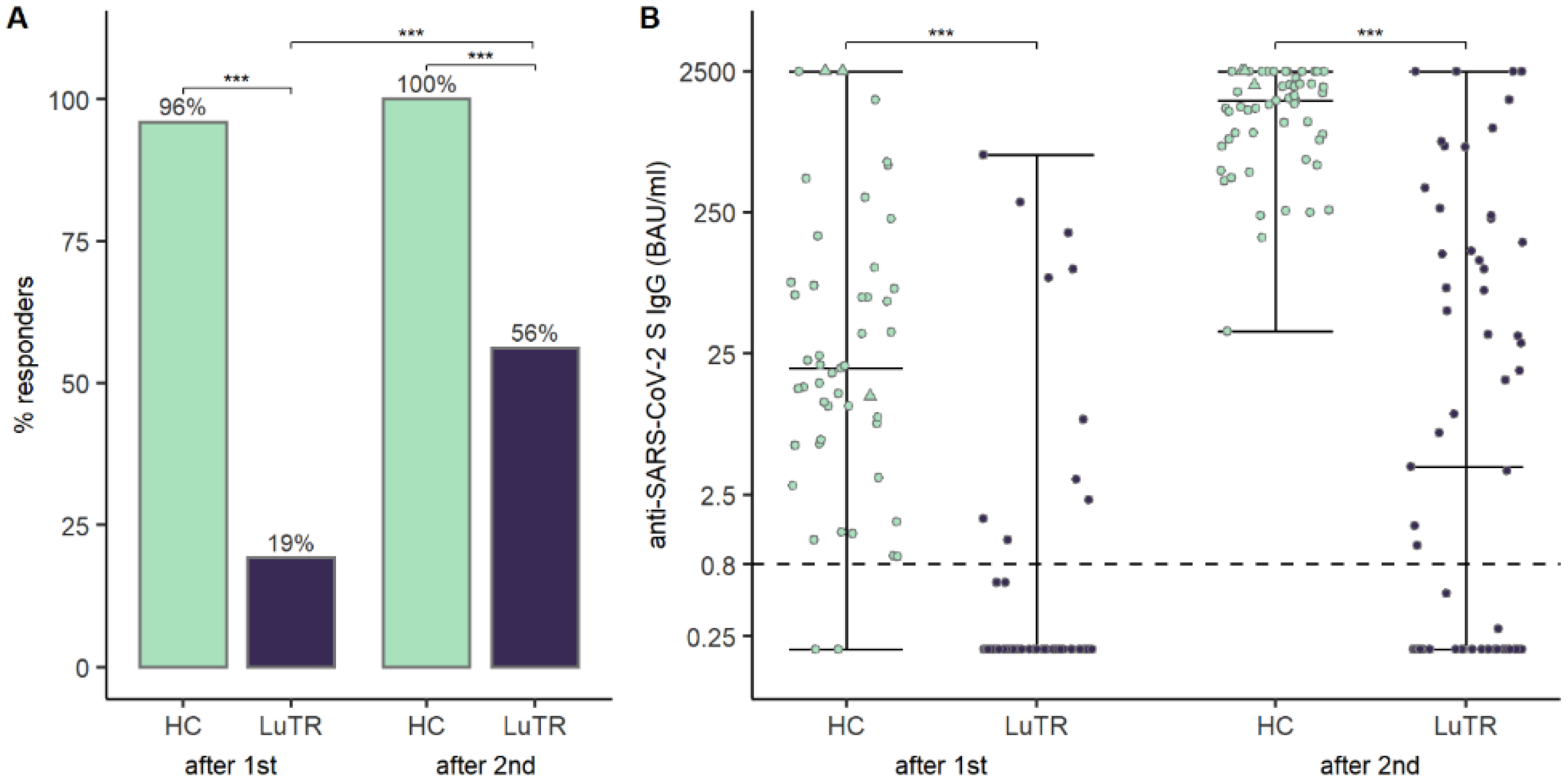
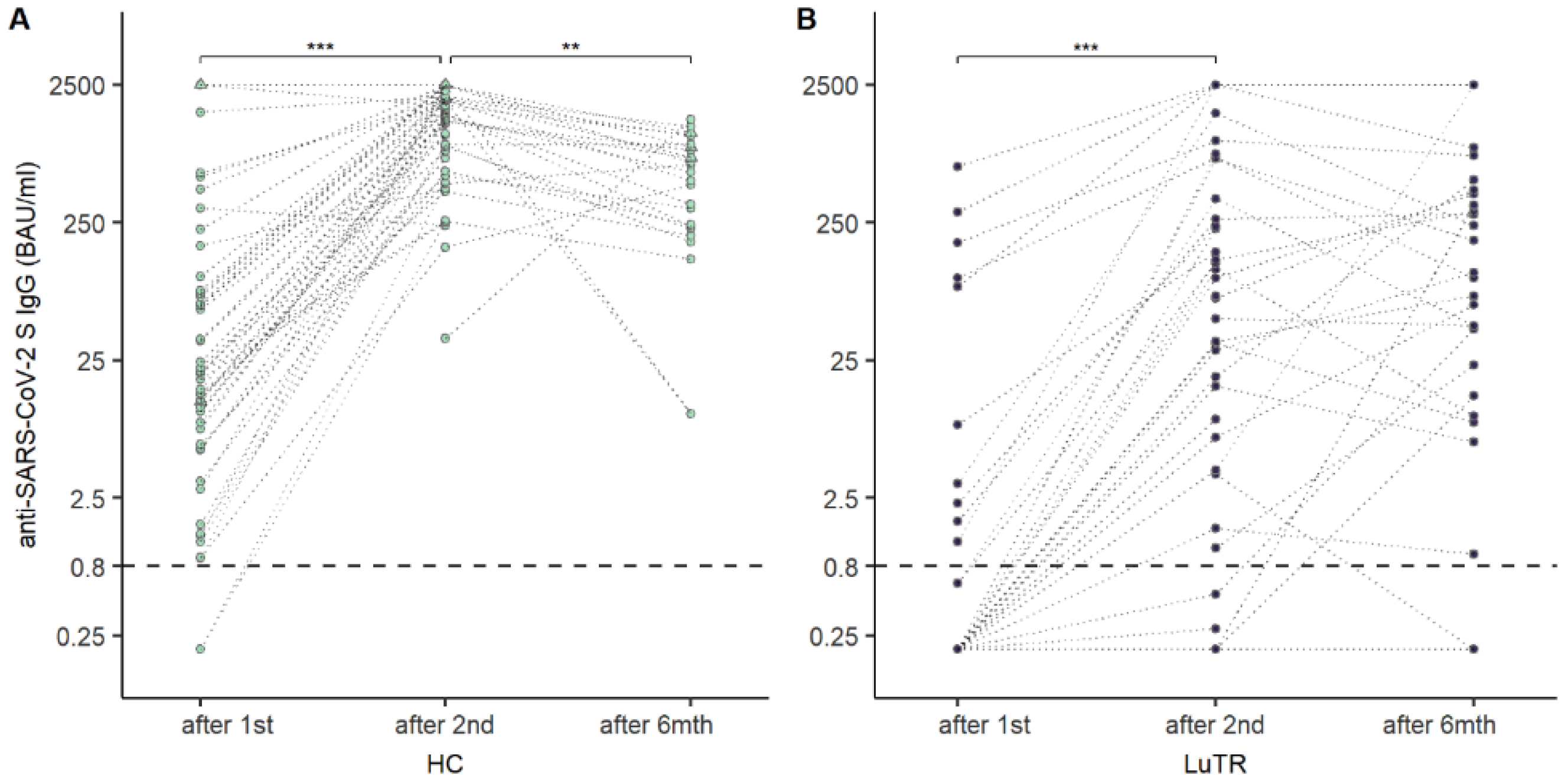
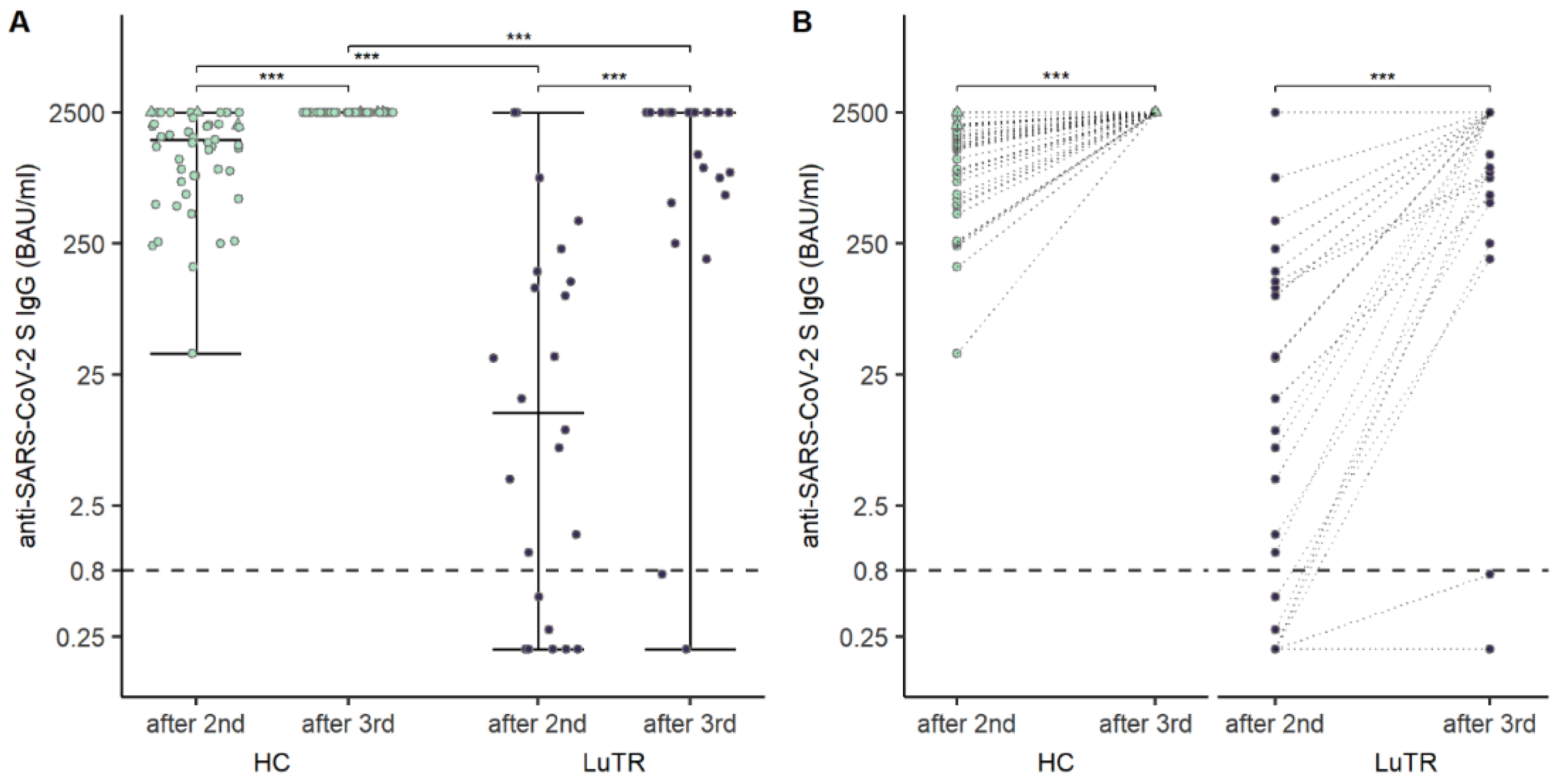
7.2. Humoral Response after COVID-19 mRNA Vaccine
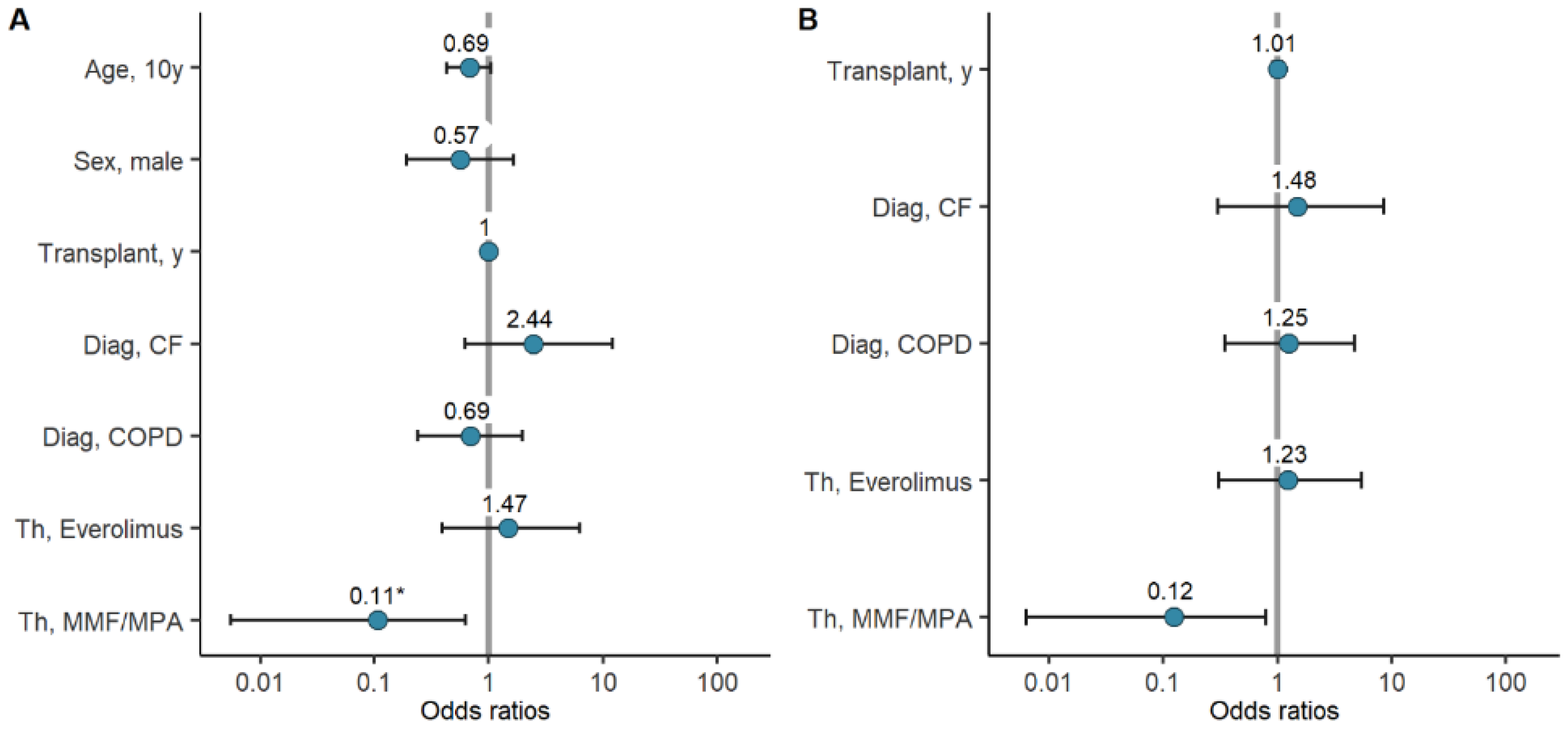
7.3. Factors Associated with Seroconversion Rates and Antibody Titers
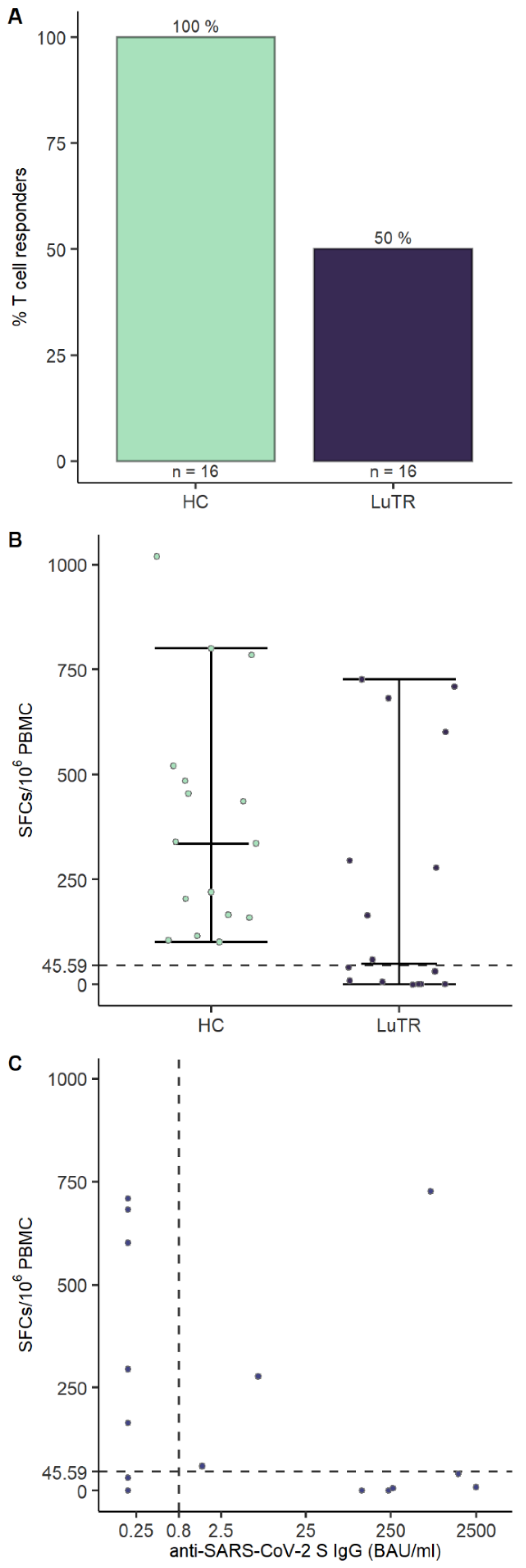
7.4. Cellular Response to SARS-CoV-2 after the Second Dose of mRNA Vaccine
7.5. Adverse Events
8. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fung, M.; Babik, J.M. COVID-19 in Immunocompromised Hosts: What We Know So Far. Clin. Infect. Dis. 2021, 72, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Robinson, P.C.; Uldrick, T.S.; Ljungman, P. COVID-19 in immunocompromised populations: Implications for prognosis and repurposing of immunotherapies. J. Immunother. Cancer 2021, 9, e002630. [Google Scholar] [CrossRef]
- Gergen, A.K.; Madsen, H.J.; Tilva, K.R.; Smith, J.B.; Weyant, M.J. Coronavirus Disease 2019 in Lung Transplant Recipients. Ann. Thorac. Surg. 2021, 111, e343–e345. [Google Scholar] [CrossRef]
- Myers, C.N.; Scott, J.H.; Criner, G.J.; Cordova, F.C.; Mamary, A.J.; Marchetti, N.; Shenoy, K.V.; Galli, J.A.; Mulhall, P.D.; Brown, J.C.; et al. COVID-19 in lung transplant recipients. Transpl. Infect. Dis. 2020, 22, e13364. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Mrak, D.; Tobudic, S.; Koblischke, M.; Graninger, M.; Radner, H.; Sieghart, D.; Hofer, P.; Perkmann, T.; Haslacher, H.; Thalhammer, R.; et al. SARS-CoV-2 vaccination in rituximab-treated patients: B cells promote humoral immune responses in the presence of T-cell-mediated immunity. Ann. Rheum. Dis. 2021, 80, 1345–1350. [Google Scholar] [CrossRef]
- Havlin, J.; Svorcova, M.; Dvorackova, E.; Lastovicka, J.; Lischke, R.; Kalina, T.; Hubacek, P. Immunogenicity of BNT162b2 mRNA COVID-19 vaccine and SARS-CoV-2 infection in lung transplant recipients. J. Heart Lung Transplant. 2021, 40, 754–758. [Google Scholar] [CrossRef]
- Hallett, A.M.; Greenberg, R.S.; Boyarsky, B.J.; Shah, P.D.; Ou, M.T.; Teles, A.T.; Krach, M.R.; López, J.I.; Werbel, W.A.; Avery, R.K.; et al. SARS-CoV-2 messenger RNA vaccine antibody response and reactogenicity in heart and lung transplant recipients. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2021, 40, 1579–1588. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Barbur, I.; Chiang, T.P.; Ou, M.T.; Greenberg, R.S.; Teles, A.T.; Krach, M.R.; López, J.I.; Garonzik-Wang, J.M.; Avery, R.K.; et al. SARS-CoV-2 Messenger RNA Vaccine Immunogenicity in Solid Organ Transplant Recipients with Prior COVID-19. Transplantation 2021, 105, e270–e271. [Google Scholar] [CrossRef] [PubMed]
- Svorcova, M.; Novysedlak, R.; Lischke, R.; Vachtenheim, J., Jr.; Strizova, Z. Vaccination Against SARS-CoV-2 in Lung Transplant Recipients: Immunogenicity, Efficacy and Safety. Front. Immunol. 2022, 13, 906225. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 June 2022).
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Kumar, D.; Ferreira, V.H.; Hall, V.G.; Hu, Q.; Samson, R.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Tomlinson, G.; Gingras, A.C.; et al. Neutralization of SARS-CoV-2 Variants in Transplant Recipients After Two and Three Doses of mRNA-1273 Vaccine: Secondary Analysis of a Randomized Trial. Ann. Intern. Med. 2022, 175, 226–233. [Google Scholar] [CrossRef]
- Haslacher, H.; Gerner, M.; Hofer, P.; Jurkowitsch, A.; Hainfellner, J.; Kain, R.; Wagner, O.F.; Perkmann, T. Usage Data and Scientific Impact of the Prospectively Established Fluid Bioresources at the Hospital-Based MedUni Wien Biobank. Biopreserv. Biobank. 2018, 16, 477–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, V.; Fabros, A.; Kulasingam, V. Quantitative Measurement of Anti-SARS-CoV-2 Antibodies: Analytical and Clinical Evaluation. J. Clin. Microbiol. 2021, 59, e03149-20. [Google Scholar] [CrossRef]
- Simon, D.; Tascilar, K.; Fagni, F.; Krönke, G.; Kleyer, A.; Meder, C.; Atreya, R.; Leppkes, M.; Kremer, A.E.; Ramming, A.; et al. SARS-CoV-2 vaccination responses in untreated, conventionally treated and anticytokine-treated patients with immune-mediated inflammatory diseases. Ann. Rheum. Dis. 2021, 80, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Cordero, E.; Manuel, O. Influenza vaccination in solid-organ transplant recipients. Curr. Opin. Organ Transplant. 2012, 17, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Cucchiari, D.; Egri, N.; Bodro, M.; Herrera, S.; Del Risco-Zevallos, J.; Casals-Urquiza, J.; Cofan, F.; Moreno, A.; Rovira, J.; Banon-Maneus, E.; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Am. J. Transplant. 2021, 21, 2727–2739. [Google Scholar] [CrossRef]
- Cassaniti, I.; Gregorini, M.; Bergami, F.; Arena, F.; Sammartino, J.C.; Percivalle, E.; Soleymaninejadian, E.; Abelli, M.; Ticozzelli, E.; Nocco, A.; et al. Effect of a Third Dose of SARS-CoV-2 mRNA BNT162b2 Vaccine on Humoral and Cellular Responses and Serum Anti-HLA Antibodies in Kidney Transplant Recipients. Vaccines 2022, 10, 921. [Google Scholar] [CrossRef]
- Morishita, T.; Sakai, A.; Matsunami, H. Seroconversions After Withdrawal From Mycophenolate Mofetil in Solid Organ Transplant Recipients without a Third Dose of BNT162b2 mRNA Coronavirus Disease 2019 Vaccine. Transplantation 2022, 106, e238–e239. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Havlin, J.; Skotnicova, A.; Dvorackova, E.; Hubacek, P.; Svorcova, M.; Lastovicka, J.; Sediva, A.; Kalina, T.; Lischke, R. Impaired Humoral Response to Third Dose of BNT162b2 mRNA COVID-19 Vaccine Despite Detectable Spike Protein-specific T cells in Lung Transplant Recipients. Transplantation 2021, 106, e183–e184. [Google Scholar] [CrossRef]
- Hoffman, T.W.; Meek, B.; Rijkers, G.T.; van Kessel, D.A. Serologic response to a third dose of an mRNA-based SARS-CoV-2 vaccine in lung transplant recipients. Transpl. Immunol. 2022, 72, 101599. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LuTRs (n = 57) | (n = 57) | |
|---|---|---|
| Age, median (IQR) | 55.5 (46.5–58.25) | 55 (44.0–64.00) |
| Sex, female n (%) | 35 (61) | 34 (60) |
| Time in years between lung organ transplantation and vaccination, median (IQR) | 7 (4–11) | NA |
| Immunosuppressive therapy including prednisone (n, %) | 57 (100) | NA |
| Immunosuppressive therapy including tacrolimus (n, %) | 56 (100) | NA |
| Immunosuppressive therapy including MMF/MPA n (%) | 47 (83) | NA |
| Immunosuppressive therapy including everolimus n (%) | 11 (19) | NA |
| Immunosuppressive therapy including ciclosporine n (%) | 1 (2) | NA |
| Therapy combination (n, %): | ||
| Tacrolimus, MMF/MPA, prednisone | 39 (68) | NA |
| Everolimus, tacrolimus, MMF/MPA, prednisone | 7 (12) | NA |
| Tacrolimus, prednisone | 6 (11) | NA |
| Everolimus, tacrolimus, prednisone | 3 (5) | NA |
| Everolimus, tacrolimus | 1 (2) | NA |
| Ciclosporine, MMF/MPA/prednisone | 1 (2) | NA |
| Therapy number n (%): | NA | |
| 2 Agents | 7 (12) | NA |
| 3 Agents | 43 (75) | NA |
| 4 Agents | 7 (12) | NA |
| Drug levels (median, IQR): | ||
| Ciclosporine (n = 1) | 120 | NA |
| Everolimus (n = 8) | 3.4 (2.7–3.6) | NA |
| Tacrolimus (n = 52) | 5.6 (4.3–6.8) | NA |
| Dose prednisone (median, IQR, n = 56) | 5 (5–5) | NA |
| Vaccine n (%) 2 doses n (%) | 57 (100) | 57 (100) |
| mRNA-1273 | 2 (4) | 0 (0) |
| BNT162b2 | 55 (96) | 57 (100) |
| Vaccine n (%) 3 doses n (%) | 24 (42) | 53 (93) |
| mRNA-1273 | 2 (8) | 2 (4) |
| BNT162b2 | 19 (80) | 51 (96) |
| ChAdOx1 nCoV-19 | 2 (8) | 0 (0) |
| Ad26.COV2.S | 1 (4) | 0 (0) |
| Univariate Logistic Regression | Multivariate Logistic Regression § | |||
|---|---|---|---|---|
| OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | |
| Age, ten years | 0.69 (0.43–1.04) | 0.088 | — | — |
| Sex, male | 0.6 (0.2–1.74) | 0.345 | — | — |
| Years since transplant | 1 (0.92–1.1) | 0.985 | 1.01 (0.92–1.12) | 0.793 |
| Diagnosis, CF | 2.05 (0.5–10.43) | 0.337 | 0.81 (0.13–5.38) | 0.820 |
| Diagnosis, COPD | 0.69 (0.24–1.98) | 0.495 | 1.49 (0.4–6.03) | 0.563 |
| Therapy, everolimus | 1.47 (0.39–6.26) | 0.578 | 1.28 (0.32–5.69) | 0.729 |
| Therapy, MMF/MPA | 0.11 (0.01–0.63) | 0.041 | 0.12 (0.01–0.78) | 0.059 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tobudic, S.; Benazzo, A.; Koblischke, M.; Schneider, L.; Blüml, S.; Winkler, F.; Schmidt, H.; Vorlen, S.; Haslacher, H.; Perkmann, T.; et al. Immune Response after mRNA COVID-19 Vaccination in Lung Transplant Recipients: A 6-Month Follow-Up. Vaccines 2022, 10, 1130. https://doi.org/10.3390/vaccines10071130
Tobudic S, Benazzo A, Koblischke M, Schneider L, Blüml S, Winkler F, Schmidt H, Vorlen S, Haslacher H, Perkmann T, et al. Immune Response after mRNA COVID-19 Vaccination in Lung Transplant Recipients: A 6-Month Follow-Up. Vaccines. 2022; 10(7):1130. https://doi.org/10.3390/vaccines10071130
Chicago/Turabian StyleTobudic, Selma, Alberto Benazzo, Maximilian Koblischke, Lisa Schneider, Stephan Blüml, Florian Winkler, Hannah Schmidt, Stefan Vorlen, Helmuth Haslacher, Thomas Perkmann, and et al. 2022. "Immune Response after mRNA COVID-19 Vaccination in Lung Transplant Recipients: A 6-Month Follow-Up" Vaccines 10, no. 7: 1130. https://doi.org/10.3390/vaccines10071130