
COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
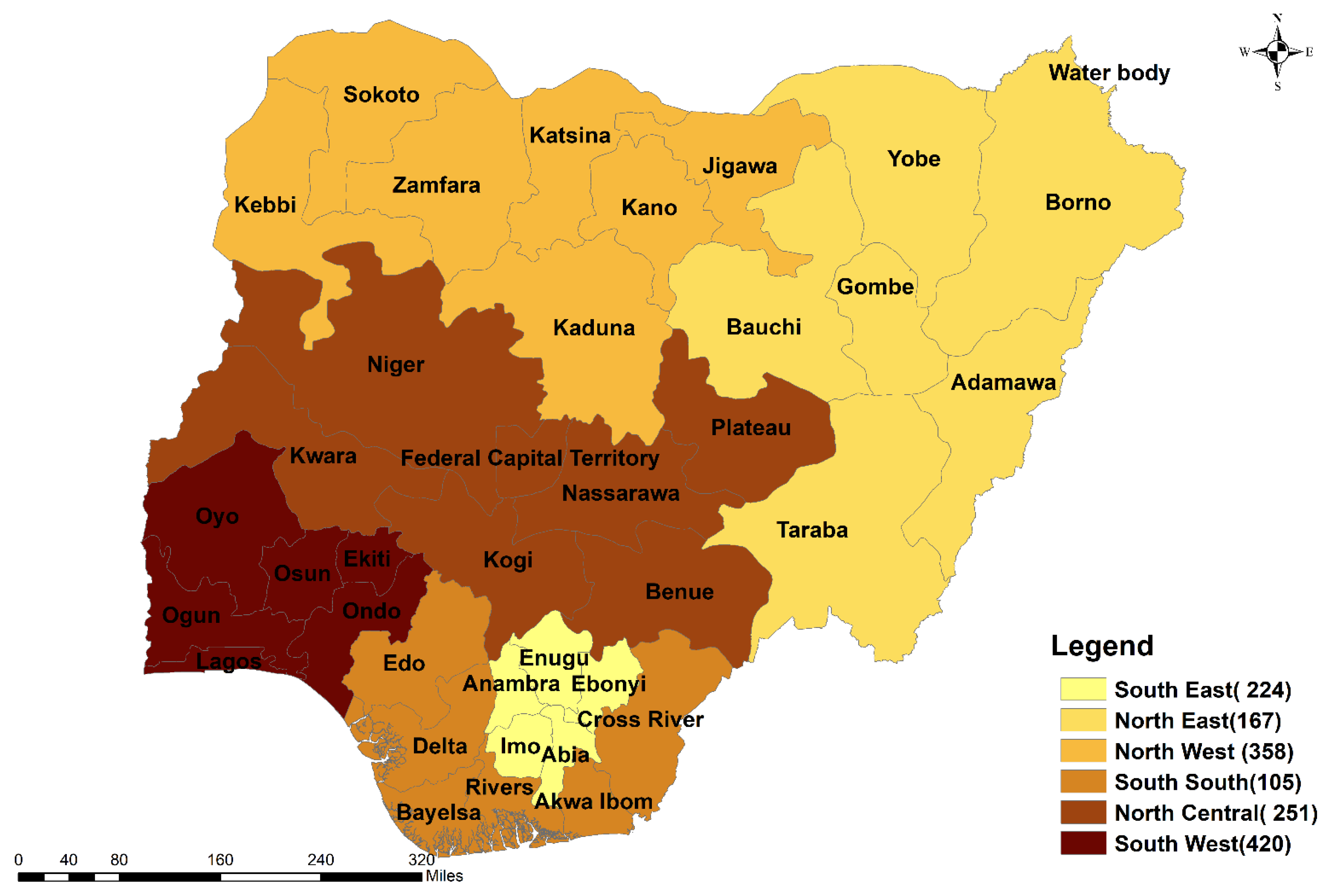
2.1. Study Area
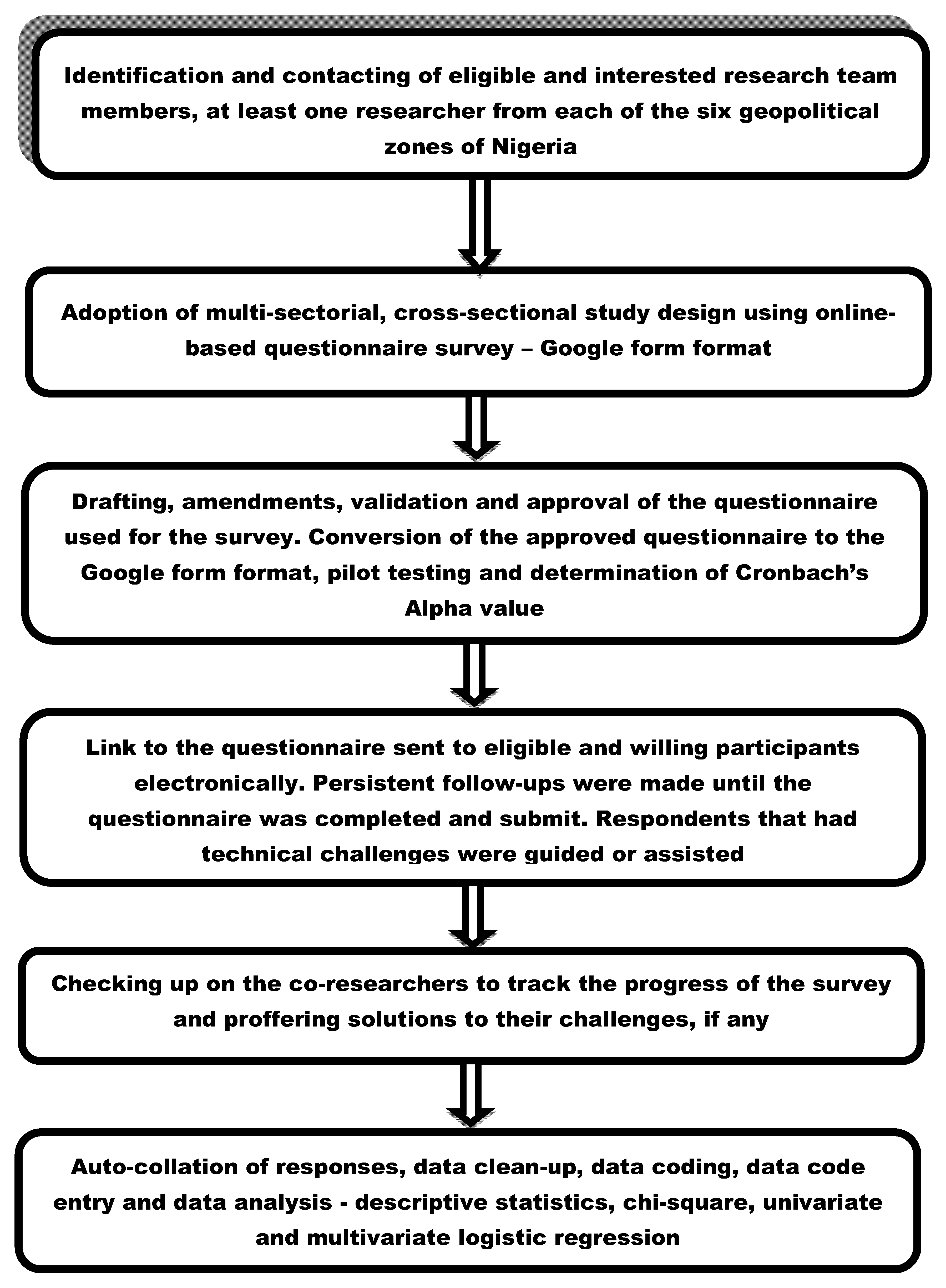
2.2. Study Design, Study Population and Sample Size Determination
2.3. Questionnaire Design, Validation, and Pilot Testing
2.4. Sampling Procedure
2.5. Ethical and Informed Consent Considerations
2.6. Data Analyses
3. Results
3.1. Percentage Response Rate
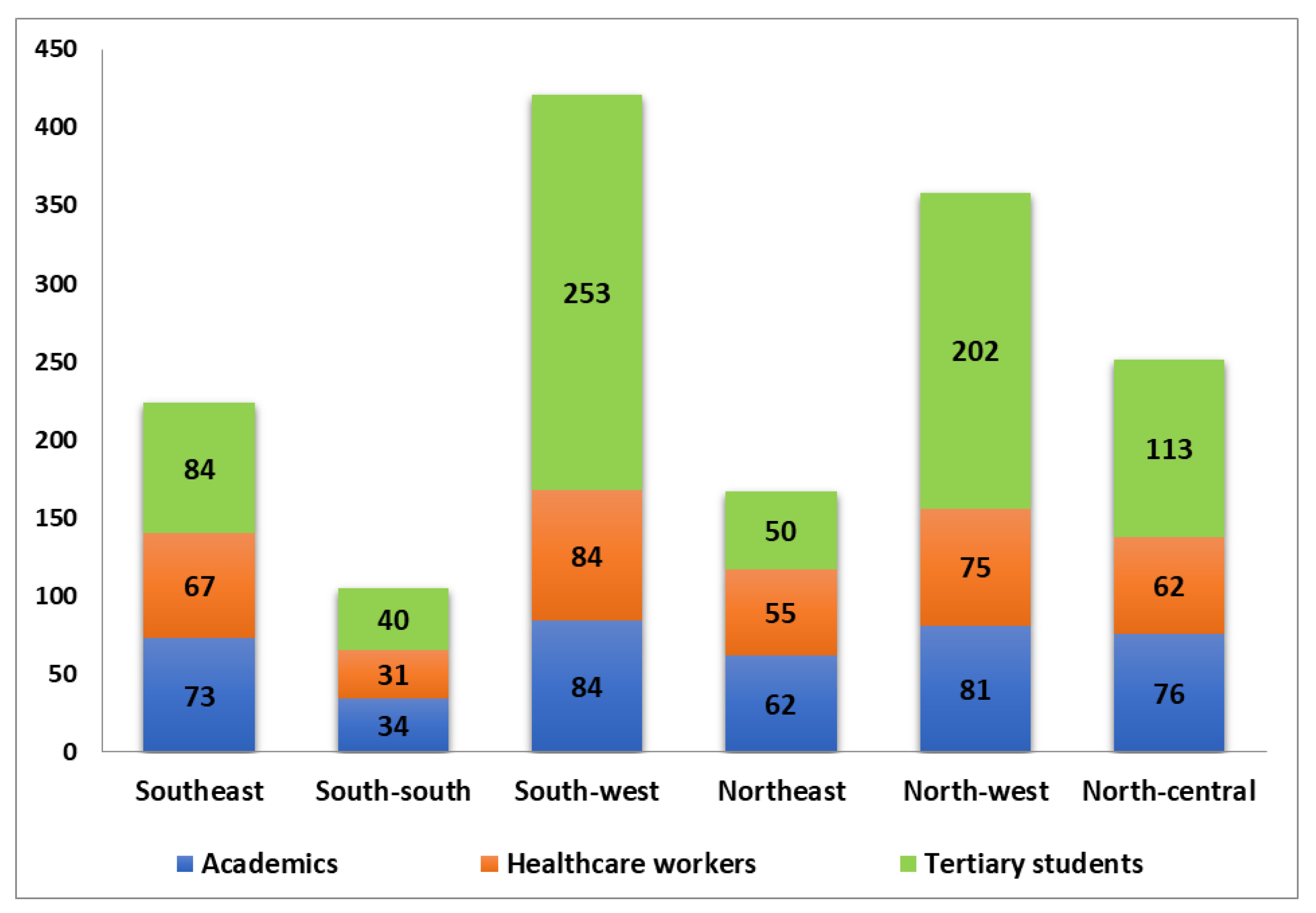
3.2. Socio-Demographics
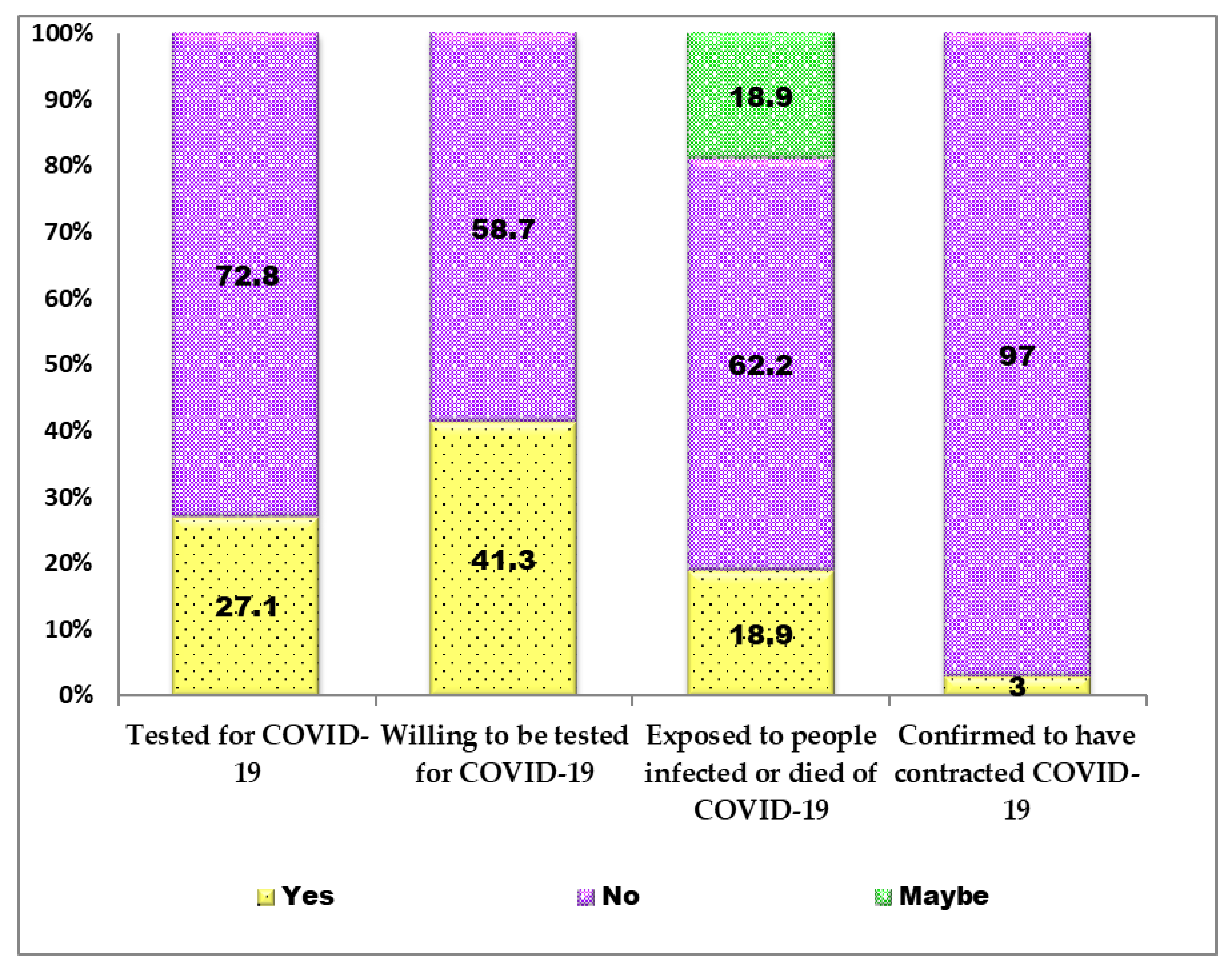
3.3. SARS-CoV-2 Testing and Infection Status of Respondents
3.4. COIVD-19 Vaccine Availability, Accessibility, Acceptance, and VH
3.5. COVID-19 VH and Measures to Improve Its Availability and Acceptance in Nigeria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 22 January 2022).
- NCDC. COVID-19 Nigeria 2022. Available online: https://covid19.ncdc.gov.ng/ (accessed on 14 March 2022).
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [Green Version]
- WHO. Achieving 70% COVID-19 Immunization Coverage by Mid-2022. 2022. Available online: https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022 (accessed on 16 December 2021).
- Adigwe, O.P. COVID-19 vaccine hesitancy and willingness to pay: Emergent factors from a cross-sectional study in Nigeria. Vaccine X 2021, 9, 100112. [Google Scholar] [CrossRef]
- Eze, U.A.; Ndoh, K.I.; Ibisola, B.A.; Onwuliri, C.D.; Osiyemi, A.; Ude, N.; Chime, A.A.; Ogbor, E.O.; Alao, A.O.; Abdullahi, A. Determinants for Acceptance of COVID-19 Vaccine in Nigeria. Cureus 2021, 13, e19801. [Google Scholar] [CrossRef]
- Josiah, B.O.; Kantaris, M. Perception of Covid-19 and acceptance of vaccination in Delta State Nigeria. Niger. Health J. 2021, 21, 60–86. [Google Scholar]
- Uzochukwu, I.C.; Eleje, G.U.; Nwankwo, C.H.; Chukwuma, G.O.; Uzuke, C.A.; Uzochukwu, C.E.; Mathias, B.A.; Okunna, C.S.; Asomugha, L.A.; Esimone, C.O. COVID-19 vaccine hesitancy among staff and students in a Nigerian tertiary educational institution. Ther. Adv. Infect. Dis. 2021, 8. [Google Scholar] [CrossRef]
- Bolarinwa, O.A. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger. Postgrad. Med. J. 2015, 22, 195. [Google Scholar] [CrossRef] [Green Version]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.-R. Design and implementation content validity study: Development of an instrument for measuring patient-centered communication. J. Caring Sci. 2015, 4, 165. [Google Scholar] [CrossRef]
- Al-Janabi, H.; Flynn, T.N.; Peters, T.J.; Bryan, S.; Coast, J. Test–retest reliability of capability measurement in the UK general population. Health Econ. 2015, 24, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e132. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afolabi, M.O.; Wariri, O.; Saidu, Y.; Otu, A.; Omoleke, S.A.; Ebenso, B.; Adebiyi, A.; Ooko, M.; Ahinkorah, B.O.; Ameyaw, E.K.; et al. Tracking the uptake and trajectory of COVID-19 vaccination coverage in 15 West African countries: An interim analysis. BMJ Glob. Health 2021, 6, e007518. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Infectious, D. The COVID-19 infodemic. Lancet Infect. Dis. 2020, 20, 875. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Personal. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Ghinai, I.; Willott, C.; Dadari, I.; Larson, H.J. Listening to the rumours: What the northern Nigeria polio vaccine boycott can tell us ten years on. Glob. Public Health 2013, 8, 1138–1150. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Progress toward poliomyelitis eradication—Nigeria, January 2009–June 2010. MMWR Morb Mortal Wkly Rep. 2010, 59, 802–807. [Google Scholar]
- Blazar, D.; Kraft, M.A. Teacher and teaching effects on students’ attitudes and behaviors. Educ. Eval. Policy Anal. 2017, 39, 146–170. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Rosa, S.S.; Prazeres, D.M.F.; Azevedo, A.M.; Marques, M.P.C. mRNA vaccines manufacturing: Challenges and bottlenecks. Vaccine 2021, 39, 2190–2200. [Google Scholar] [CrossRef]
- Worldometer. Nigeria Population 2022. Available online: http://www.worldometers.info/world-population/nigeriapopulation (accessed on 12 February 2022).
- Mlaba, K. Why Are African Countries Throwing Away COVID-19 Vaccines? Available online: https://www.globalcitizen.org/en/content/african-countries-throwing-away-covid-19-vaccines/ (accessed on 6 February 2022).
- Mohamed, N.A.; Solehan, H.M.; Mohd Rani, M.D.; Ithnin, M.; Che Isahak, C.I. Knowledge, acceptance and perception on COVID-19 vaccine among Malaysians: A web-based survey. PLoS ONE 2021, 16, e0256110. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.; Jasny, E.; Schmidt, K.E.; Petsch, B. New vaccine technologies to combat outbreak situations. Front. Immunol. 2018, 9, 1963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, J. COVID-19 and mRNA vaccines—first large test for a new approach. JAMA 2020, 324, 1125–1127. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low-and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- OECD. OECD Policy Responses to Coronavirus (COVID-19)—Testing for COVID-19: A Way to Lift Confinement Restrictions 2021. Available online: https://www.oecd.org/coronavirus/en/policy-responses (accessed on 21 January 2022).
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B. 1.617. 2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2022, 22, 183–195. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern 2022. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 12 February 2022).
- Mallapaty, S. Researchers fear growing COVID vaccine hesitancy in developing nations. Nature 2021, 601, 174–175. [Google Scholar] [CrossRef]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef]
- Chen, P.-L.; Lee, N.-Y.; Cia, C.-T.; Ko, W.-C.; Hsueh, P.-R. A review of treatment of coronavirus disease 2019 (COVID-19): Therapeutic repurposing and unmet clinical needs. Front. Pharmacol. 2020, 11, 1782. [Google Scholar] [CrossRef] [PubMed]
- El Bairi, K.; Trapani, D.; Petrillo, A.; Le Page, C.; Zbakh, H.; Daniele, B.; Belbaraka, R.; Curigliano, G.; Afqir, S. Repurposing anticancer drugs for the management of COVID-19. Eur. J. Cancer 2020, 141, 40–61. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Plotkin, S.A. Impact of vaccines; health, economic and social perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef] [PubMed]
- Sunohara, S.; Asakura, T.; Kimura, T.; Ozawa, S.; Oshima, S.; Yamauchi, D.; Tamakoshi, A. Effective vaccine allocation strategies, balancing economy with infection control against COVID-19 in Japan. PLoS ONE 2021, 16, e0257107. [Google Scholar] [CrossRef]
- Boschiero, N. COVID-19 Vaccines as Global Common Goods: An Integrated Approach of Ethical, Economic Policy and Intellectual Property Management. Glob. Jurist 2021. [Google Scholar] [CrossRef]
- Shivaram, D. A Man Died from Rabies in Illinois. Here’s Why That’s So Unusual in the U.S. 2021. Available online: https://www.npr.org/2021/09/29/1041457232/rabies-illinois-man-death-rare-public-health (accessed on 16 December 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographics | Variables | Proportion | χ2-Value | p-Value |
|---|---|---|---|---|
| EVER TESTED FOR SARS-CoV-2 | ||||
| Gender | Male | 67.6% (1031/1525) | 0.371 | 0.543 |
| Female | 32.4% (494/1525) | |||
| Job description | Healthcare worker | 24.5% (373/1525) | 16.82 | 0.002 * |
| Academic | 26.9% (410/1525) | |||
| Tertiary student | 48.7% (742/1525) | |||
| Age categories (years) | 16–30 | 52% (793/1525) | 149.1 | <0.001 * |
| 31–45 | 34.3% (523/1525) | |||
| ≥46 | 13.7% (209/1525) | |||
| Marital status | Single | 52.4% (799/1525) | 7.347 | 0.007 * |
| Married/divorced | 47.6% (726/1525) | |||
| Religion | Christianity | 59.3% (905/1525) | 1.484 | 0.223 |
| Islam/others | 40.7% (620/1525) | |||
| Educational level | Postgraduate | 35.7% (545/1525) | 13.27 | 0.001 * |
| Graduate | 29.1% (443/1525) | |||
| Undergraduate | 35.2% (537/1525) | |||
| Location | South-west | 6.9% (105/1525) | 19.46 | 0.0006 * |
| South-south | 14.7% (224/1525) | |||
| Southeast | 11.0% (167/1525) | |||
| Northeast | 23.5% (358/1525) | |||
| North-west | 16.5% (251/1525) | |||
| North-central | 6.9% (105/1525) | |||
| VACCINATION AGAINST COVID-19 | ||||
| Gender | Male | 67.6% (1031/1525) | 1.299 | 0.254 |
| Female | 32.4% (494/1525) | |||
| Job description | Healthcare worker | 24.5% (373/1525) | 34.43 | 0.000 * |
| Academic | 26.9% (410/1525) | |||
| Tertiary student | 48.7% (742/1525) | |||
| Age categories (years) | 16–30 | 52% (793/1525) | 151.4 | <0.001 * |
| 31–45 | 34.3% (523/1525) | |||
| ≥46 | 13.7% (209/1525) | |||
| Marital status | Single | 52.4% (799/1525) | 0.881 | 0.348 |
| Married/divorced | 47.6% (726/1525) | |||
| Religion | Christianity | 59.3% (905/1525) | 2.337 | 0.126 |
| Islam/others | 40.7% (620/1525) | |||
| Educational level | Postgraduate | 35.7% (545/1525) | 16.17 | 0.003 * |
| Graduate | 29.1% (443/1525) | |||
| Undergraduate | 35.2% (537/1525) | |||
| Location | South-west | 6.9% (105/1525) | 24.94 | <0.001 * |
| South-south | 14.7% (224/1525) | |||
| Southeast | 11.0% (167/1525) | |||
| Northeast | 23.5% (358/1525) | |||
| North-west | 16.5% (251/1525) | |||
| North-central | 6.9% (105/1525) | |||
| S/No | Questions Asked or Information Required | Number of Respondents (%) |
|---|---|---|
| 1. | * Reasons for non-vaccination among unvaccinated respondents (n = 1079) | |
| COVID-19 vaccination registration protocol is difficult | 633 (58.7) | |
| Suspicion/doubts on safety of novel vaccines | 43 (4.0) | |
| COVID-19 is a hoax | 183 (17.0) | |
| The vaccines are not available/accessible in my locality | 57 (5.3) | |
| Herbal medicines/home remedies are effective for cure/management of COVID-19 | 65 (6.0) | |
| Influence from anti-COVID-19-vaccine movements | 40 (3.7) | |
| Vaccination is against my religious beliefs or personal ideology | 495 (45.9) | |
| Concerns about long term health/side effects | 296 (27.4) | |
| Scepticism about the vaccine due to hasty production/roll out | 159 (14.7) | |
| Preventive measures are enough to protect against COVID-19 | 323 (30.0) | |
| Bad feelings towards the vaccines due to negative social media reports/rumours | 633 (58.7) | |
| Others | 37 (3.4) | |
| 2. | * Some health concerns that prevented unvaccinated respondents (n = 1079) from getting vaccinated | |
| Blood clot issues among women | 266 (24.7) | |
| Allergic reactions | 307 (28.5) | |
| Innate immunity concerns | 345 (32.0) | |
| New or worsening muscle/joint pains | 107 (10.0) | |
| Myocardial infarction | 180 (16.7) | |
| Others | 41 (3.8) | |
| 3. | * Fears against COVID-19 vaccine among unvaccinated respondents (n = 1079) | |
| The vaccines may be unsafe due to its hasty production and or roll out | 674 (62.9) | |
| The vaccine may contain ‘hidden chip’ that may be a mark of the anti-Christ | 208 (19.3) | |
| It may limiting procreation and fertility and hence a population control strategy | 206 (19.9) | |
| The vaccine may cause deaths as one certain vaccine did in Kano State, Nigeria | 132 (12.2) | |
| The vaccine may cause adverse immunological problem as mRNA vaccine are relatively new and sufficient time is needed to proof their safety and efficacy | 613 (56.8) | |
| Others | 22 (2.0) | |
| 4. | * Ways to improve COVID-19 vaccine availability and acceptance in Nigeria (n = 1525) | |
| More COVID-19 vaccine donations from developed to developing countries | 519 (34.0) | |
| Increased funding to the Nigerian health and education/research sectors | 727(47.7) | |
| More public enlightenment campaigns/grass-root health education to the populace | 955 (62.6) | |
| Procurement of more COVID-19 vaccines | 379 (24.8) | |
| Commencement of indigenous COVID-19 vaccine production | 505 (33.1) | |
| Provision of COVID-19 vaccine storage and distribution facilities | 453 (29.7) | |
| Increased remuneration and provision of incentives to healthcare workers | 437 (28.7) | |
| Developed countries should halt 3rd COVID-19 booster vaccination to increase the availability of the vaccines in developing countries | 211 (13.8) | |
| Univariable Analysis | Multivariable Model | |||||
|---|---|---|---|---|---|---|
| Variables | Categories | Proportions | OR (95% CI) | p-Value | AOR (95% CI) | p-Value |
| Gender | Male | 67.6% (1031/1525) | Referent | Referent | Referent | Referent |
| Female | 32.4% (494/1525) | 1.28 (1.03–1.60) | 0.026 | 1.13 (0.88–1.45) | 0.30 | |
| State | South West | 27.5% (422/1525) | Referent | Referent | Referent | Referent |
| South-South | 6.9% (105/1525) | 1.03 (0.67–1.61) | 0.90 | 1.12 (0.71–1.79) | 0.60 | |
| South East | 14.7% (224/1525) | 1.42 (1.01–2.01) | 0.044 | 1.60 (1.11–2.32) | 0.012 | |
| North East | 11.0% (167/1525) | 1.24 (0.86–1.81) | 0.30 | 2.40 (1.51–3.87) | <0.001 | |
| North West | 23.5% (358/1525) | 0.61 (0.46–0.81) | <0.001 | 1.31 (0.88–1.95) | 0.20 | |
| North Central | 16.5% (251/1525) | 0.89 (0.65–1.22) | 0.50 | 1.28 (0.91–1.80) | 0.20 | |
| Job description | Healthcare worker | 24.5% (373/1525) | Referent | Referent | Referent | Referent |
| Academic | 26.9% (410/1525) | 1.05 (0.82–1.35) | 0.70 | 1.19 (0.85–1.67 | 0.3 | |
| Tertiary student | 48.7% (742/1525) | 0.86 (0.67–1.10) | 0.20 | 1.73 (1.13–2.65) | 0.012 | |
| Age categories (years) | 16–30 | 52.0% (793/1525) | Referent | Referent | Referent | Referent |
| 31–45 | 34.3% (523/1525) | 0.68 (0.55–0.86) | <0.001 | 0.75 (0.51–1.10) | 0.15 | |
| ≥46 | 13.7 (209/1525) | 0.64 (0.47–0.88) | 0.005 | 0.63 (0.37–1.05) | 0.078 | |
| Marital status | Single | 52.4% (799/1525) | Referent | Referent | Referent | Referent |
| Married/divorced | 47.6% (726/1525) | 0.76 (0.62–0.93) | 0.009 | 1.13 (0.78–1.62) | 0.50 | |
| Religion | Christian | 59.3% (905/1525) | Referent | Referent | Referent | Referent |
| Non-Christian | 40.7% (602/1525) | 0.56 (0.45–0.69) | <0.001 | |||
| Highest educational level attained | Postgraduate | 35.7% (545/1525) | Referent | Referent | Referent | Referent |
| Graduate | 29.0% (443/1525) | 1.05 (0.81–1.35) | 0.70 | 1.19 (0.85–1.67) | 0.3 | |
| Undergraduate | 35.0% (537/1525) | 1.51 (1.19–1.94) | <0.001 | 1.73 (1.13–2.65) | 0.012 | |
| Tested against COVID-19 | Yes (1) | 26.3% (401/1525) | Referent | Referent | Referent | Referent |
| No (0) | 73.7% (1124/1525) | 2.43 (1.90–3.13) | <0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Njoga, E.O.; Mshelbwala, P.P.; Abah, K.O.; Awoyomi, O.J.; Wangdi, K.; Pewan, S.B.; Oyeleye, F.A.; Galadima, H.B.; Alhassan, S.A.; Okoli, C.E.; et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines 2022, 10, 626. https://doi.org/10.3390/vaccines10040626
Njoga EO, Mshelbwala PP, Abah KO, Awoyomi OJ, Wangdi K, Pewan SB, Oyeleye FA, Galadima HB, Alhassan SA, Okoli CE, et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines. 2022; 10(4):626. https://doi.org/10.3390/vaccines10040626
Chicago/Turabian StyleNjoga, Emmanuel O., Philip P. Mshelbwala, Kenneth O. Abah, Olajoju J. Awoyomi, Kinley Wangdi, Shedrach B. Pewan, Felix A. Oyeleye, Haruna B. Galadima, Salisu A. Alhassan, Chinwe E. Okoli, and et al. 2022. "COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria" Vaccines 10, no. 4: 626. https://doi.org/10.3390/vaccines10040626