
Modelling SARS-CoV-2 Binding Antibody Waning 8 Months after BNT162b2 Vaccination

 , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Vaccination of Health Care Workers
2.2. Serological Tests
2.3. Statistical Analysis
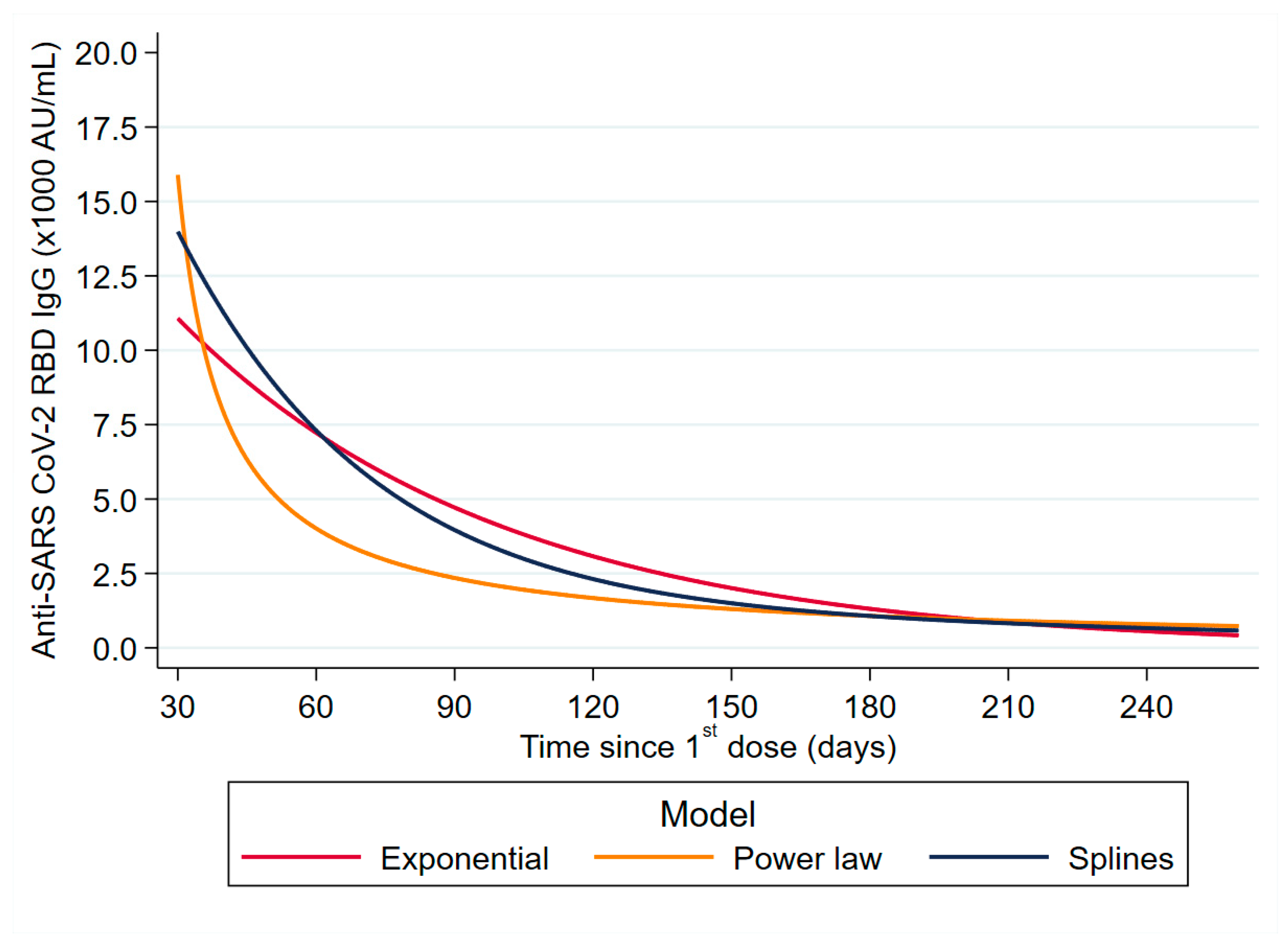
2.3.1. Exponential Model (EM)
2.3.2. Power-Law Model (PLM)
2.3.3. Restricted Cubic Splines Model (RCSM)
2.3.4. Model Selection
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feikin, D.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.; Huppert, A.; O’Brien, K.; Smith, P.G. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. 2021. preprint. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J. Efficacy of the mRNA-1273 SARS-CoV-2 vaccine at completion of blinded phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine through 6 months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines in US Veterans. N. Engl. J. Med. 2021, 386, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nat. Med. 2021, 27, 2136–2143. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z. Waning of BNT162b2 vaccine protection against SARS-CoV-2 infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning immunity after the BNT162b2 vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G. Effectiveness of Covid-19 vaccines against the B. 1.617. 2 (Delta) variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A. Waning immune humoral response to BNT162b2 Covid-19 vaccine over 6 months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health-Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C. Antibody persistence through 6 months after the second dose of mRNA-1273 vaccine for COVID-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Pegu, A.; O’Connell, S.E.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Anderson, E.; Bennett, H.; Corbett, K.S. Durability of mRNA-1273 vaccine–induced antibodies against SARS-CoV-2 variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef]
- Falsey, A.R.; Frenck Jr, R.W.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X. SARS-CoV-2 neutralization with BNT162b2 vaccine dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Bayart, J.-L.; Douxfils, J.; Gillot, C.; David, C.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Gerin, V. Waning of IgG, total and neutralizing antibodies 6 months post-vaccination with BNT162b2 in healthcare workers. Vaccines 2021, 9, 1092. [Google Scholar] [CrossRef]
- Collier, A.-r.Y.; Yu, J.; McMahan, K.; Liu, J.; Chandrashekar, A.; Maron, J.S.; Atyeo, C.; Martinez, D.R.; Ansel, J.L.; Aguayo, R. Differential kinetics of immune responses elicited by COVID-19 vaccines. N. Engl. J. Med. 2021, 385, 2010–2012. [Google Scholar] [CrossRef]
- Psichogiou, M.; Karabinis, A.; Poulakou, G.; Antoniadou, A.; Kotanidou, A.; Degiannis, D.; Pavlopoulou, I.D.; Chaidaroglou, A.; Roussos, S.; Mastrogianni, E. Comparative Immunogenicity of BNT162b2 mRNA Vaccine with Natural SARS-CoV-2 Infection. Vaccines 2021, 9, 1017. [Google Scholar] [CrossRef]
- Kageyama, T.; Ikeda, K.; Tanaka, S.; Taniguchi, T.; Igari, H.; Onouchi, Y.; Kaneda, A.; Matsushita, K.; Hanaoka, H.; Nakada, T.-A. Antibody responses to BNT162b2 mRNA COVID-19 vaccine and their predictors among healthcare workers in a tertiary referral hospital in Japan. Clin. Microbiol. Infect. 2021, 27, 1861-e1. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Elmer, A.; Kingston, N. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Oyebanji, O.A.; Wilson, B.; Keresztesy, D.; Carias, L.; Wilk, D.; Payne, M.; Aung, H.; Denis, K.S.; Lam, E.C.; Rowley, C.F. Does a lack of vaccine side effects correlate with reduced BNT162b2 mRNA vaccine response among healthcare workers and nursing home residents? Aging Clin. Exp. Res. 2021, 33, 3151–3160. [Google Scholar] [CrossRef]
- Aldridge, R.W.; Yavlinsky, A.; Nguyen, V.; Eyre, M.T.; Shrotri, M.; Navaratnam, A.M.; Beale, S.; Braithwaite, I.; Byrne, T.; Kovar, J. Waning of SARS-CoV-2 antibodies targeting the Spike protein in individuals post second dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and risk of breakthrough infections: Analysis of the Virus Watch community cohort. medRxiv 2021. [Google Scholar]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A. BNT162b2 vaccine induces neutralizing antibodies and poly-specific T cells in humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef]
- SARS-CoV-2 Immunoassay | Abbott Core Laboratory. Available online: https://www.corelaboratory.abbott/us/en/offerings/segments/infectious-disease/sars-cov-2 (accessed on 15 December 2021).
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Gelfand, A.E.; Hills, S.E.; Racine-Poon, A.; Smith, A.F. Illustration of Bayesian inference in normal data models using Gibbs sampling. J. Am. Stat. Assoc. 1990, 85, 972–985. [Google Scholar] [CrossRef]
- Mallon, P.W.; Brunet, L.; Hsu, R.K.; Fusco, J.S.; Mounzer, K.C.; Prajapati, G.; Beyer, A.P.; Wohlfeiler, M.B.; Fusco, G.P. Weight gain before and after switch from TDF to TAF in a US cohort study. J. Int. AIDS Soc. 2021, 24, e25702. [Google Scholar] [CrossRef] [PubMed]
- Antia, A.; Ahmed, H.; Handel, A.; Carlson, N.E.; Amanna, I.J.; Antia, R.; Slifka, M. Heterogeneity and longevity of antibody memory to viruses and vaccines. PLoS Biol. 2018, 16, e2006601. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, Z.; Wei, F.-X.; Huang, S.-J.; Tan, Z.; Fang, Y.; Zhu, F.-C.; Wu, T.; Zhang, J.; Xia, N.-S. Modeling the long-term antibody response of a hepatitis E vaccine. Vaccine 2015, 33, 4124–4129. [Google Scholar] [CrossRef]
- Korn, E.L.; Graubard, B.I. Analysis of Health Surveys; John Wiley & Sons: Hoboken, NJ, USA, 1999. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; T.S.L.: College Station, TX, USA, 2013. [Google Scholar]
- McMahan, K.; Yu, J.; Mercado, N.B.; Loos, C.; Tostanoski, L.H.; Chandrashekar, A.; Liu, J.; Peter, L.; Atyeo, C.; Zhu, A. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature 2021, 590, 630–634. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Addetia, A.; Crawford, K.H.; Dingens, A.; Zhu, H.; Roychoudhury, P.; Huang, M.-L.; Jerome, K.R.; Bloom, J.D.; Greninger, A.L. Neutralizing antibodies correlate with protection from SARS-CoV-2 in humans during a fishery vessel outbreak with a high attack rate. J. Clin. Microbiol. 2020, 58, e02107–e02120. [Google Scholar] [CrossRef]
- Corbett Kizzmekia, S.; Nason Martha, C.; Flach Britta, G.M.; O’Connell Sarah, J.T.S. Immune correlates of protection by mRNA-1273 vaccine against SARS-CoV-2 in nonhuman primates. Science 2021, 373, 6561. [Google Scholar]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 variants—Clinical, public health, and vaccine implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Orenstein, W.; Offit, P.A.; Edwards, K.M. Plotkin’s Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Zhong, D.; Xiao, S.; Debes, A.K.; Egbert, E.R.; Caturegli, P.; Colantuoni, E.; Milstone, A.M. Durability of Antibody Levels after Vaccination with mRNA SARS-CoV-2 Vaccine in Individuals with or without Prior Infection. JAMA 2021, 326, 2524–2526. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; Al Kanaani, Z. Association of prior SARS-CoV-2 infection with risk of breakthrough infection following mRNA vaccination in Qatar. JAMA 2021, 326, 1930–1939. [Google Scholar] [CrossRef]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.-H.; Barnes, C.O.; Cipolla, M.; Ramos, V. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.; Vogels, C.B.; Yildirim, I.; Rothman, J.E.; Lu, P.; Monteiro, V.; Gehlhausen, J.R.; Campbell, M.; Silva, J.; Tabachnikova, A. Impact of circulating SARS-CoV-2 variants on mRNA vaccine-induced immunity. Nature 2021, 600, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.; Weisblum, Y.; Rutkowska, M.; Poston, D.; DaSilva, J.; Zhang, F.; Bednarski, E.; Cho, A.; Schaefer-Babajew, D.J.; Gaebler, C. High genetic barrier to SARS-CoV-2 polyclonal neutralizing antibody escape. Nature 2021, 600, 512–516. [Google Scholar] [CrossRef]
- Schmidt, F.; Muecksch, F.; Weisblum, Y.; Da Silva, J.; Bednarski, E.; Cho, A.; Wang, Z.; Gaebler, C.; Caskey, M.; Nussenzweig, M. Plasma neutralization properties of the SARS-CoV-2 Omicron variant. medRxiv 2021. [Google Scholar]
- Doria-Rose, N.; Shen, X.; Schmidt, S.D.; O’Dell, S.; McDanal, C.; Feng, W.; Tong, J.; Eaton, A.; Maglinao, M.; Tang, H. Booster of mRNA-1273 Vaccine Reduces SARS-CoV-2 Omicron Escape from Neutralizing Antibodies. medRxiv 2021. [Google Scholar]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
- Roessler, A.; Riepler, L.; Bante, D.; von Laer, D.; Kimpel, J. SARS-CoV-2 B. 1.1. 529 variant (Omicron) evades neutralization by sera from vaccinated and convalescent individuals. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.12.08.21267491v1 (accessed on 15 December 2021).
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. MedRxiv 2021, 73, 2065–2072. [Google Scholar]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection against COVID-19 by BNT162b2 booster across age groups. N. Engl. J. Med. 2021, 385, 2421–2430. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef]
- Andreano, E.; Paciello, I.; Piccini, G.; Manganaro, N.; Pileri, P.; Hyseni, I.; Leonardi, M.; Pantano, E.; Abbiento, V.; Benincasa, L. Hybrid immunity improves B cells and antibodies against SARS-CoV-2 variants. Nature 2021, 600, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Cromer, D.; Steain, M.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Kent, S.J.; Triccas, J.A.; Khoury, D.S.; Davenport, M.P. Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: A meta-analysis. Lancet Microbe 2021, 3, E52–E61. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Covariate | Total n = 97 | Total n = 774 | p-Value |
|---|---|---|---|
| Gender, n (%) | 0.090 1 | ||
| Male | 43 (44.3) | 275 (35.5) | |
| Female | 54 (55.7) | 499 (64.5) | |
| Age (years), mean (SD) | 50.3 (9.4) | 47.4 (10.4) | 0.011 2 |
| Age (years), median (25th–75th) | 50.1 (46.1–56.6) | 48.9 (39.2–55.2) | 0.019 3 |
| Age (years), n (%) | 0.349 1 | ||
| [18–50) | 47 (48.4) | 414 (53.5) | |
| [50–68) | 50 (51.6) | 360 (46.5) | |
| Country of birth, n (%) | 0.555 1 | ||
| Greece | 91 (93.8) | 713 (92.1) | |
| Other | 6 (6.2) | 61 (7.9) | |
| Body mass index (BMI) (kg/m2), mean (SD) | 26.4 (5.5) | 26.2 (4.8) | 0.653 2 |
| Body mass index (BMI) (kg/m2), median (25th–75th) | 25.6 (22.9–29.1) | 25.7 (22.8–29.0) | 0.988 3 |
| Body mass index (BMI) (kg/m2), n (%) | 0.770 1 | ||
| Under/Normal weight: <25 | 41 (42.3) | 342 (44.2) | |
| Overweight: 25–30 | 35 (36.1) | 288 (37.2) | |
| Obesity: ≥30 | 21 (21.6) | 144 (18.6) | |
| Education, n (%) | 0.136 1 | ||
| High school or below | 28 (28.9) | 179 (23.2) | |
| University | 30 (30.9) | 319 (41.3) | |
| MSc-Ph.D. | 39 (40.2) | 275 (35.6) | |
| Health care workers, n (%) | <0.001 1 | ||
| Yes | 65 (67.0) | 644 (83.2) | |
| No | 32 (33.0) | 130 (16.8) | |
| Risk factors for severe COVID-19 illness, n (%) | 0.960 1 | ||
| Yes | 15 (15.5) | 119 (15.7) | |
| No | 82 (84.5) | 641 (84.3) | |
| Side effects of vaccination, n (%) | 0.626 1 | ||
| Yes | 53 (54.6) | 443 (57.2) | |
| No | 44 (45.4) | 331 (42.8) |
| Covariate | Study Day 30 | Study Day 125 | Study Day 183 | Study Day 251 | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | Geometric Mean (95% CI) | p 1 | Geometric Mean (95% CI) | p 1 | Geometric Mean (95% CI) | p 1 | Geometric Mean (95% CI) | p 1 | |
| Overall | 97 | 13,674 (11,164–16,749) | 2112 (1716–2601) | 1036 (834–1288) | 617 (490–778) | ||||
| Gender | 0.135 | 0.743 | 0.918 | 0.856 | |||||
| Male | 43 | 11,520 (7974–16,641) | 2032 (1400–2950) | 1023 (696–1504) | 632 (424–942) | ||||
| Female | 54 | 15,674 (12,558–19,564) | 2179 (1716–2767) | 1047 (812–1350) | 606 (458–801) | ||||
| Age (y) | 0.258 | 0.577 | 0.355 | 0.359 | |||||
| [18─50) | 47 | 15,413 (10,917–21,763) | 2245 (1609–3131) | 1151 (817–1622) | 690 (483–984) | ||||
| [50─68) | 50 | 12,218 (9696–15,396) | 1995 (1530–2602) | 939 (708–1245) | 556 (409–757) | ||||
| Risk factors for severe COVID-19 illness | 0.072 | 0.181 | 0.158 | 0.133 | |||||
| Yes | 15 | 8894 (3493–22,647) | 1520 (588–3928) | 721 (278–1871) | 410 (154–1092) | ||||
| No | 82 | 14,793 (12,362–17,702) | 2243 (1859–2707) | 1107 (905–1355) | 666 (536–827) | ||||
| Adverse effects of vaccination | 0.003 | 0.042 | 0.043 | 0.042 | |||||
| Yes | 53 | 17,983 (14,111–22,918) | 2563 (1950–3368) | 1268 (952–1689) | 765 (568–1032) | ||||
| No | 44 | 9831 (7125–13,565) | 1674 (1219–2299) | 813 (584–1131) | 477 (333–682) | ||||
| History of COVID-19 infection up to the 2nd dose | 0.912 | 0.071 | 0.044 | 0.036 | |||||
| Yes | 7 | 14,246 (2396–84,696) | 4166 (525–33,070) | 2283 (254–20,538) | 1478 (154–14,173) | ||||
| No | 90 | 13,631 (11,247–16,519) | 2004 (1667–2409) | 974 (806–1179) | 577 (470–708) |
| Model | Ν | Log-Likelihood | df | AIC | Study Day of t1/2 | 95% CI |
|---|---|---|---|---|---|---|
| Exponential | 97 | −71.9 | 6 | 155.8 | 78.7 | 76.1–81.4 |
| Power-Law | 97 | −23.3 | 6 | 58.5 | 39.8 | 39.0–40.6 |
| Restricted cubic spline | 97 | 112.2 | 11 | −202.4 | 62.0 | 59.9–64.5 |
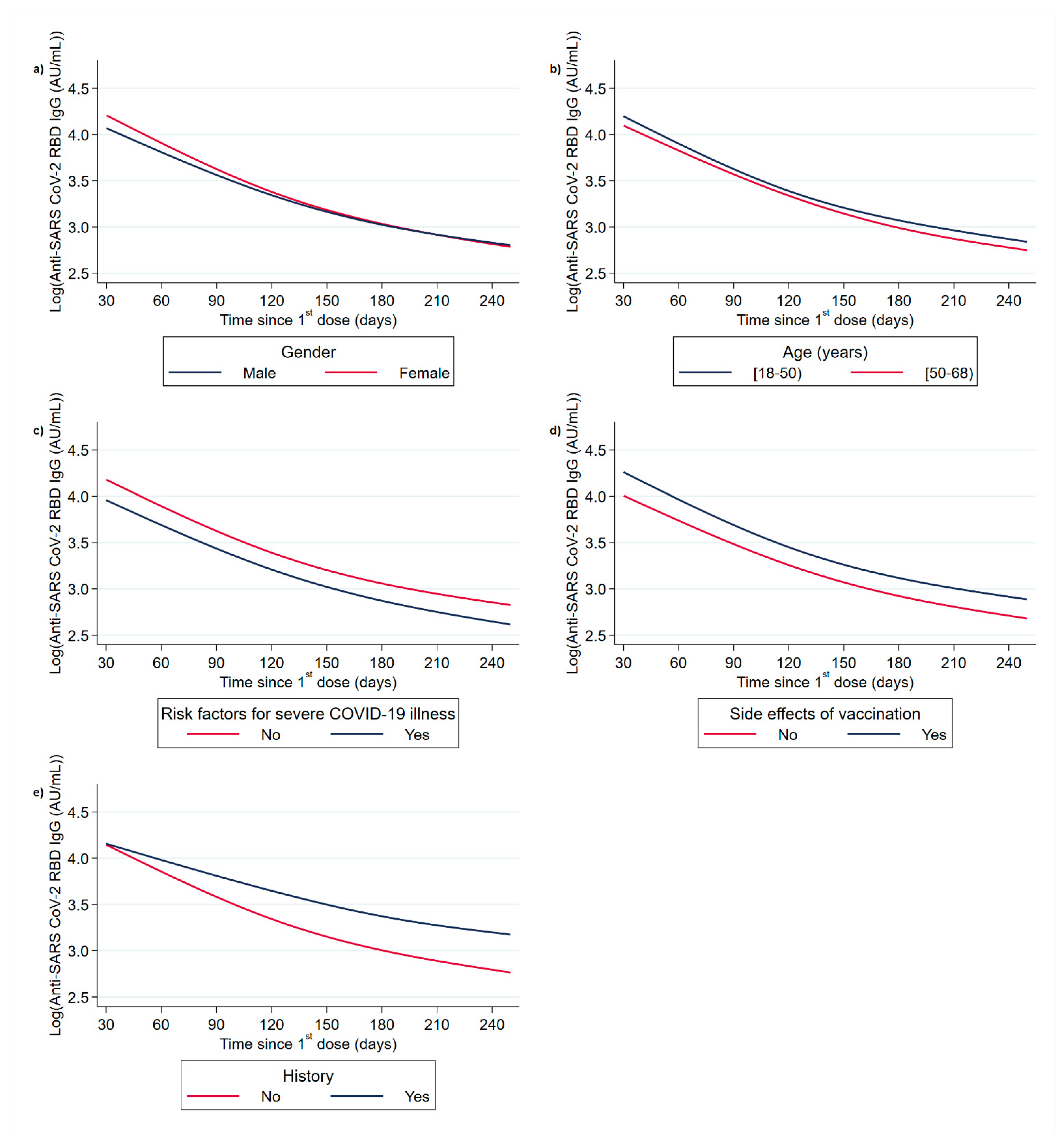
| Univariable | Multivariable | ||||||
|---|---|---|---|---|---|---|---|
| Covariate | N | % Difference | 95% CI | p-Value | % Difference | 95% CI | p-Value |
| Gender 1 | |||||||
| Male | 43 | Ref. | |||||
| Female | 54 | 26.1% | −13.7–84.4% | 0.230 | |||
| Age (y) 2 | |||||||
| [18–50) | 47 | Ref. | |||||
| [50–68) | 50 | −16.2% | −42.6–22.3% | 0.360 | |||
| Risk factors for severe COVID-19 illness 3 | |||||||
| No | 82 | Ref. | Ref. | ||||
| Yes | 15 | −36.6% | −62.2–6.3% | 0.084 | −43.6% | −66.6–−5.1% | 0.031 |
| Side effects of vaccination 4 | |||||||
| Yes | 53 | Ref. | Ref. | ||||
| No | 44 | −40.4% | −58.8–−14.0% | 0.006 | −38.6% | −57.2–−11.9% | 0.001 |
| History of COVID-19 infection 5 | |||||||
| No | 90 | Ref. | Ref. | ||||
| Yes (at 29 days) | 7 | 1.6% | −52.9–119.2% | 0.968 | 20.3% | −44.0–158.4% | 0.635 |
| Yes (at 125 days) | 106.2% | -4.1–343.3% | 0.064 | 144.4% | 13.0–428.3% | 0.023 | |
| Yes (at 183 days) | 134.0% | 3.4–429.7% | 0.041 | 177.2% | 21.8–530.5% | 0.015 | |
| Yes (at 253 days) | 158.0% | 9.5–508.1% | 0.030 | 205.8% | 30.1–618.6% | 0.010 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatzakis, A.; Karabinis, A.; Roussos, S.; Pantazis, N.; Degiannis, D.; Chaidaroglou, A.; Petsios, K.; Pavlopoulou, I.; Tsiodras, S.; Paraskevis, D.; et al. Modelling SARS-CoV-2 Binding Antibody Waning 8 Months after BNT162b2 Vaccination. Vaccines 2022, 10, 285. https://doi.org/10.3390/vaccines10020285
Hatzakis A, Karabinis A, Roussos S, Pantazis N, Degiannis D, Chaidaroglou A, Petsios K, Pavlopoulou I, Tsiodras S, Paraskevis D, et al. Modelling SARS-CoV-2 Binding Antibody Waning 8 Months after BNT162b2 Vaccination. Vaccines. 2022; 10(2):285. https://doi.org/10.3390/vaccines10020285
Chicago/Turabian StyleHatzakis, Angelos, Andreas Karabinis, Sotirios Roussos, Nikos Pantazis, Dimitrios Degiannis, Antigoni Chaidaroglou, Konstantinos Petsios, Ioanna Pavlopoulou, Sotirios Tsiodras, Dimitrios Paraskevis, and et al. 2022. "Modelling SARS-CoV-2 Binding Antibody Waning 8 Months after BNT162b2 Vaccination" Vaccines 10, no. 2: 285. https://doi.org/10.3390/vaccines10020285