
Diabetes Mellitus and Its Association with Adverse In-Hospital Outcomes in Patients with COVID-19—A Nationwide Study
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Study Oversight, Support, and Ethical Statement
2.3. Coding of Diagnoses, Procedures, and Definitions
2.4. Study Outcomes and Adverse In-Hospital Events
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison Regarding Patient Characteristics of COVID-19 Inpatients with and without Diabetes Mellitus
3.3. Comparison Regarding Respiratory Manifestation of COVID-19 Inpatients with and without Diabetes Mellitus
3.4. Comparison Regarding Treatment Approaches in COVID-19 Inpatients with and without Diabetes Mellitus
3.5. Comparison Regarding Outcomes of COVID-19 Inpatients with and without Diabetes Mellitus
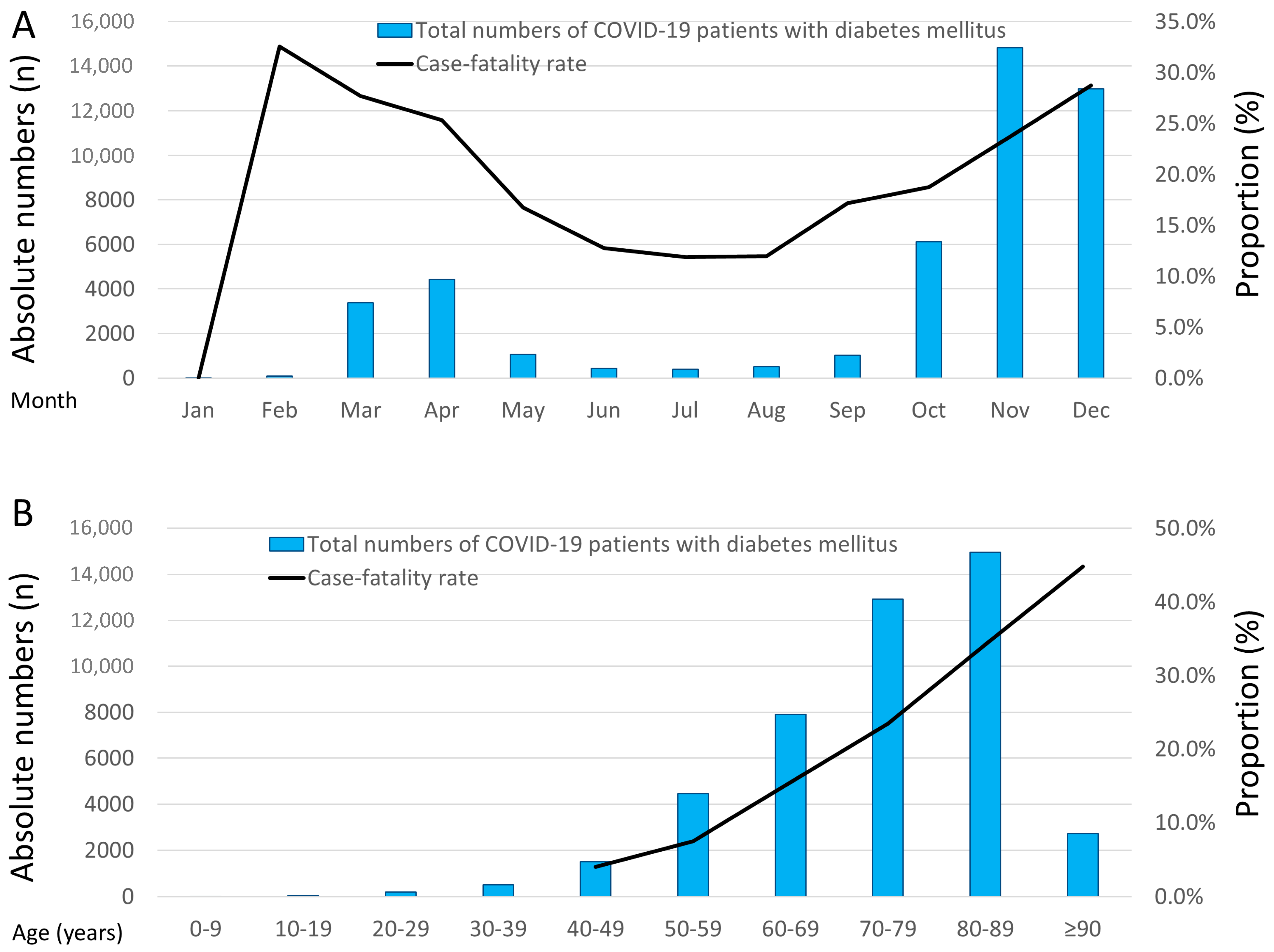
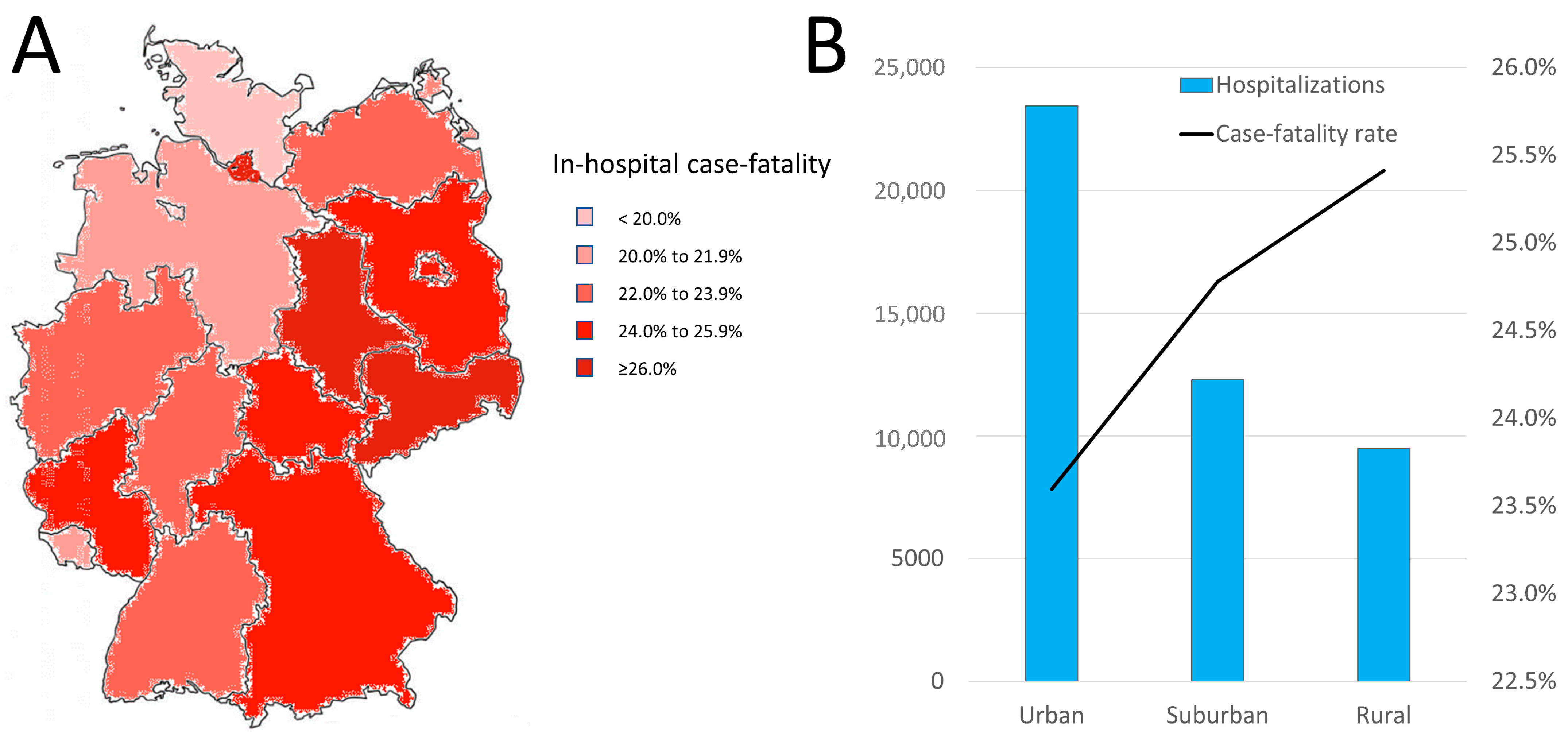
3.6. Temporal and Regional Trends
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Böhmer, M.M.; Buchholz, U.; Corman, V.M.; Hoch, M.; Katz, K.; Marosevic, D.V.; Böhm, S.; Woudenberg, T.; Ackermann, N.; Konrad, R.; et al. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: A case series. Lancet Infect. Dis. 2020, 20, 920–928. [Google Scholar] [CrossRef]
- Hobohm, L.; Sagoschen, I.; Barco, S.; Schmidtmann, I.; Espinola-Klein, C.; Konstantinides, S.; Münzel, T.; Keller, K. Trends and Risk Factors of In-Hospital Mortality of Patients with COVID-19 in Germany: Results of a Large Nationwide Inpatient Sample. Viruses 2022, 14, 275. [Google Scholar] [CrossRef]
- Keller, K.; Sagoschen, I.; Schmitt, V.H.; Sivanathan, V.; Espinola-Klein, C.; Lavie, C.J.; Münzel, T.; Hobohm, L. Obesity and Its Impact on Adverse In-Hospital Outcomes in Hospitalized Patients With COVID-19. Front. Endocrinol. 2022, 13, 876028. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ullrich, A.; Schranz, M.; Rexroth, U.; Hamouda, O.; Schaade, L.; Diercke, M.; Boender, T.S. Impact of the COVID-19 pandemic and associated non-pharmaceutical interventions on other notifiable infectious diseases in Germany: An analysis of national surveillance data during week 1–2016–week 32–2020. Lancet Reg. Health Eur. 2021, 6, 100103. [Google Scholar] [CrossRef]
- Keller, K.; Friedrich, O.; Treiber, J.; Quermann, A.; Friedmann-Bette, B. Former SARS-CoV-2 Infection Was Related to Decreased VO2 Peak and Exercise Hypertension in Athletes. Diagnostics 2023, 13, 1792. [Google Scholar] [CrossRef]
- Voci, D.; Fedeli, U.; Farmakis, I.T.; Hobohm, L.; Keller, K.; Valerio, L.; Schievano, E.; Amidei, C.B.; Konstantinides, S.V.; Kucher, N.; et al. Deaths related to pulmonary embolism and cardiovascular events before and during the 2020 COVID-19 pandemic: An epidemiological analysis of data from an Italian high-risk area. Thromb. Res. 2022, 212, 44–50. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: A registry study. Lancet Public Health 2020, 5, e536–e542. [Google Scholar] [CrossRef]
- Toscano, O.; Cosentino, N.; Campodonico, J.; Bartorelli, A.L.; Marenzi, G. Acute Myocardial Infarction During the COVID-19 Pandemic: An Update on Clinical Characteristics and Outcomes. Front. Cardiovasc. Med. 2021, 8, 648290. [Google Scholar] [CrossRef] [PubMed]
- Reichardt, P.; Bollmann, A.; Hohenstein, S.; Glass, B.; Untch, M.; Reichardt, A.; Amrein, D.; Kuhlen, R. Decreased Incidence of Oncology Admissions in 75 Helios Hospitals in Germany during the COVID-19 Pandemic. Oncol. Res. Treat. 2020, 44, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Gurney, J.K.; Millar, E.; Dunn, A.; Pirie, R.; Mako, M.; Manderson, J.; Hardie, C.; Jackson, C.G.; North, R.; Ruka, M.; et al. The impact of the COVID-19 pandemic on cancer diagnosis and service access in New Zealand–a country pursuing COVID-19 elimination. Lancet Reg. Health West. Pac. 2021, 10, 100127. [Google Scholar] [CrossRef]
- Kapsner, L.A.; Kampf, M.O.; Seuchter, S.A.; Gruendner, J.; Gulden, C.; Mate, S.; Mang, J.M.; Schüttler, C.; Deppenwiese, N.; Krause, L.; et al. Reduced Rate of Inpatient Hospital Admissions in 18 German University Hospitals During the COVID-19 Lockdown. Front. Public Health 2021, 8, 594117. [Google Scholar] [CrossRef]
- Sena, G.; Gallelli, G. An increased severity of peripheral arterial disease in the COVID-19 era. J. Vasc. Surg. 2020, 72, 758. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Valabhji, J.; Misra, S. Diabetes and the COVID-19 pandemic. Diabetologia 2023, 66, 255–266. [Google Scholar] [CrossRef]
- Keller, K.; Hobohm, L.; Ebner, M.; Kresoja, K.-P.; Münzel, T.; Konstantinides, S.V.; Lankeit, M. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur. Heart J. 2020, 41, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Khunti, K. COVID-19 and Diabetes. Annu. Rev. Med. 2022, 73, 129–147. [Google Scholar] [CrossRef]
- Singh, A.K.; Gupta, R.; Ghosh, A.; Misra, A. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab. Syndr. 2020, 14, 303–310. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team; Chow, N.; Fleming-Dutra, K.; Gierke, R.; Hall, A.; Hughes, M.; Pilishvili, T.; Ritchey, M.; Roguski, K. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019—United States, February 12–March 28, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 382–386. [Google Scholar]
- Prieto-Alhambra, D.; Balló, E.; Coma, E.; Mora, N.; Aragón, M.; Prats-Uribe, A.; Fina, F.; Benítez, M.; Guiriguet, C.; Fàbregas, M.; et al. Filling the gaps in the characterization of the clinical management of COVID-19: 30-day hospital admission and fatality rates in a cohort of 118 150 cases diagnosed in outpatient settings in Spain. Leuk. Res. 2020, 49, 1930–1939. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Bello-Chavolla, O.Y.; Bahena-López, J.P.; Antonio-Villa, N.E.; Vargas-Vázquez, A.; González-Díaz, A.; Márquez-Salinas, A.; Fermín-Martínez, C.A.; Naveja, J.J.; Aguilar-Salinas, C.A. Predicting Mortality Due to SARS-CoV-2: A Mechanistic Score Relating Obesity and Diabetes to COVID-19 Outcomes in Mexico. J. Clin. Endocrinol. Metab. 2020, 105, 2752–2761. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Jevalikar, G.; Sharma, R.; Singh, A.; Farooqui, K.J.; Mahendru, S.; Krishnamurthy, A.; Dewan, A.; Budhiraja, S. High prevalence of diabetes and other comorbidities in hospitalized patients with COVID-19 in Delhi, India, and their association with outcomes. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 15, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gillies, C.L.; Singh, R.; Singh, A.; Chudasama, Y.; Coles, B.; Seidu, S.; Zaccardi, F.; Davies, M.J.; Khunti, K. Prevalence of co-morbidities and their association with mortality in patients with COVID-19: A systematic review and meta-analysis. Diabetes Obes. Metab. 2020, 22, 1915–1924. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Shen, M.; Yang, Q.; Fairley, C.K.; Chai, Z.; McIntyre, R.; Ong, J.J.; Liu, H.; Lu, P.; Hu, W.; et al. Global Diabetes Prevalence in COVID-19 Patients and Contribution to COVID-19– Related Severity and Mortality: A Systematic Review and Meta-analysis. Diabetes Care 2023, 46, 890–897. [Google Scholar] [CrossRef]
- Hartmann-Boyce, J.; Morris, E.; Goyder, C. Diabetes and Risks from COVID-19. Cent. Evid. Based Med. Diabetes Care 2020, 43, 1695–1703. [Google Scholar]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, J.; Sun, X.; Wang, L.; Xu, Y.; Zhang, Y.; Liu, X.; Dong, C. Influence of diabetes mellitus on the severity and fatality of SARS-CoV-2 (COVID-19) infection. Diabetes Obes. Metab. 2020, 22, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and risk factors for COVID-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2020, 9, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Kania, M.; Mazur, K.; Terlecki, M.; Matejko, B.; Hohendorff, J.; Chaykivska, Z.; Fiema, M.; Kopka, M.; Kostrzycka, M.; Wilk, M.; et al. Characteristics, Mortality, and Clinical Outcomes of Hospitalized Patients with COVID-19 and Diabetes: A Reference Single-Center Cohort Study from Poland. Int. J. Endocrinol. 2023, 2023, 8700302. [Google Scholar] [CrossRef]
- Sindi, A.A.; Tashkandi, W.A.; Jastaniah, M.W.; Bashanfar, M.A.; Fakhri, A.F.; Alsallum, F.S.; Alguydi, H.B.; Elhazmi, A.; Al-Khatib, T.A.; Alawi, M.M.; et al. Impact of diabetes mellitus and co-morbidities on mortality in patients with COVID-19: A single-center retrospective study. Saudi Med. J. 2023, 44, 67–73. [Google Scholar] [CrossRef]
- Mayerhöfer, T.; Klein, S.; Wernly, B.; Flaatten, H.; Guidet, B.; De Lange, D.W.; Fjølner, J.; Leaver, S.; Beil, M.; Sviri, S.; et al. Diabetes mellitus is associated with 90-day mortality in old critically ill COVID-19 patients: A multicenter prospective observational cohort study. Infection 2023, 1–9. [Google Scholar] [CrossRef]
- Roy, B.; Runa, S.A. SARS-CoV-2 infection and diabetes: Pathophysiological mechanism of multi-system organ failure. World J. Virol. 2022, 11, 252–274. [Google Scholar] [CrossRef] [PubMed]
- Wieczfinska, J.; Kleniewska, P.; Pawliczak, R. Oxidative Stress-Related Mechanisms in SARS-CoV-2 Infections. Oxidative Med. Cell. Longev. 2022, 2022, 5589089. [Google Scholar] [CrossRef]
- Grossmann, V.; Schmitt, V.H.; Zeller, T.; Panova-Noeva, M.; Schulz, A.; Laubert-Reh, D.; Juenger, C.; Schnabel, R.B.; Abt, T.G.; Laskowski, R.; et al. Profile of the Immune and Inflammatory Response in Individuals With Prediabetes and Type 2 Diabetes. Diabetes Care 2015, 38, 1356–1364. [Google Scholar] [CrossRef] [Green Version]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Hamer, M.; Gale, C.R.; Batty, G.D. Diabetes, glycaemic control, and risk of COVID-19 hospitalisation: Population-based, prospective cohort study. Metab. Clin. Exp. 2020, 112, 154344. [Google Scholar] [CrossRef]
- Sathish, T.; Kapoor, N.; Cao, Y.; Tapp, R.J.; Zimmet, P. Proportion of newly diagnosed diabetes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Obes. Metab. 2020, 23, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Ingraham, N.E.; Murray, T.A.; Marmor, S.; Hovertsen, S.; Gronski, J.; McNeil, C.; Feng, R.; Guzman, G.; Abdelwahab, N.; et al. Metformin and risk of mortality in patients hospitalised with COVID-19: A retrospective cohort analysis. Lancet Heal. Longev. 2020, 2, e34–e41. [Google Scholar] [CrossRef]
- Sardu, C.; D’Onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 2020, 43, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.K.; Rangari, G.; Madhavrao, C.; Sharma, S. Current management of diabetes patients with COVID-19. Expert Rev. Endocrinol. Metab. 2023, 18, 199–207. [Google Scholar] [CrossRef]
- Javid, F.A.; Waheed, F.A.; Zainab, N.; Khan, H.; Amin, I.; Bham, A.; Ghoghawala, M.; Sheraz, A.; Haloub, R. COVID-19 and diabetes in 2020: A systematic review. J. Pharm. Policy Pract. 2023, 16, 42. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Thimmareddygari, D.; Ramahi, A.; Atallah, L.; Baranetsky, N.G.; Slim, J. Clinical characteristics and outcome in patients with combined diabetic ketoacidosis and hyperosmolar hyperglycemic state associated with COVID-19: A retrospective, hospital-based observational case series. Diabetes Res. Clin. Pract. 2020, 166, 108279. [Google Scholar] [CrossRef]
- Boddu, S.K.; Aurangabadkar, G.; Kuchay, M.S. New onset diabetes, type 1 diabetes and COVID-19. Diabetes Metab. Syndr. 2020, 14, 2211–2217. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Al-Aly, Z. Risks and burdens of incident diabetes in long COVID: A cohort study. Lancet Diabetes Endocrinol. 2022, 10, 311–321. [Google Scholar] [CrossRef]
- Skurk, T. COVID-19 kann auch noch im Nachgang Typ-2-Diabetes begünstigen. Info Diabetol. 2022, 16, 10–11. [Google Scholar] [CrossRef]
- Rathmann, W.; Kuss, O.; Kostev, K. Incidence of newly diagnosed diabetes after Covid-19. Diabetologia 2022, 65, 949–954. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | COVID-19 with Diabetes Mellitus (n = 45,232; 25.7%) | COVID-19 without Diabetes Mellitus (n = 130,905; 74.3%) | p-Value |
|---|---|---|---|
| Age | 76.0 (66.0–83.0) | 69.0 (52.0–81.0) | <0.001 |
| Age ≥70 years | 30,610 (67.7%) | 63,719 (48.7%) | <0.001 |
| Female sex | 19,907 (44.0%) | 64,042 (48.9%) | <0.001 |
| In-hospital stay (days) | 10.0 (5.0–17.0) | 7.0 (3.0–13.0) | <0.001 |
| Cardiovascular risk factors | |||
| Obesity | 4293 (9.5%) | 5090 (3.9%) | <0.001 |
| Essential arterial hypertension | 28,752 (63.6%) | 53,728 (41.0%) | <0.001 |
| Hyperlipidaemia | 12,012 (26.6%) | 15,561 (11.9%) | <0.001 |
| Comorbidities | |||
| Coronary artery disease | 11,264 (24.9%) | 14,310 (10.9%) | <0.001 |
| Heart failure | 11,002 (24.3%) | 16,117 (12.3%) | <0.001 |
| Peripheral artery disease | 3135 (6.9%) | 2505 (1.9%) | <0.001 |
| Atrial fibrillation/flutter | 12,336 (27.3%) | 21,824 (16.7%) | <0.001 |
| Chronic obstructive pulmonary disease | 4384 (9.7%) | 7770 (5.9%) | <0.001 |
| Chronic renal insufficiency (glomerular filtration rate <60 mL/min/1.73 m2) | 12,395 (27.4%) | 14,977 (11.4%) | <0.001 |
| Cancer | 2262 (5.0%) | 6739 (5.1%) | 0.221 |
| Mild liver disease | 655 (1.4%) | 990 (0.8%) | <0.001 |
| Severe liver disease | 1525 (3.4%) | 2614 (2.0%) | <0.001 |
| Charlson comorbidity index | 6.0 (4.0–8.0) | 3.0 (1.0–5.0) | <0.001 |
| Respiratory manifestations of COVID-19 and post-COVID-19 status | |||
| Pneumonia | 31,266 (69.1%) | 75,647 (57.8%) | <0.001 |
| Acute respiratory distress syndrome | 4190 (9.3%) | 7404 (5.7%) | <0.001 |
| Multisystemic inflammatory syndrome COVID-19 infection | 172 (0.4%) | 325 (0.2%) | <0.001 |
| Post-COVID-19 status | 152 (0.3%) | 405 (0.3%) | 0.384 |
| Treatment | |||
| Intensive care unit | 9651 (21.3%) | 17,402 (13.3%) | <0.001 |
| Mechanical ventilation | 4437 (9.8%) | 7705 (5.9%) | <0.001 |
| Extracorporeal membrane oxygenation (ECMO) | 449 (1.0%) | 1005 (0.8%) | <0.001 |
| Dialysis | 2448 (5.4%) | 3127 (2.4%) | <0.001 |
| Adverse events during hospitalization | |||
| In-hospital death | 10,991 (24.3%) | 20,616 (15.7%) | <0.001 |
| Major adverse cardiac and cerebrovascular events (MACCE) | 12,210 (27.0%) | 22,814 (17.4%) | <0.001 |
| Cardiopulmonary resuscitation | 1150 (2.5%) | 1709 (1.3%) | <0.001 |
| Venous thromboembolism | 1334 (2.9%) | 3653 (2.8%) | 0.079 |
| Acute kidney failure | 8815 (19.5%) | 13,260 (10.1%) | <0.001 |
| Myocarditis | 54 (0.1%) | 172 (0.1%) | 0.539 |
| Myocardial infarction | 1097 (2.4%) | 1656 (1.3%) | <0.001 |
| Stroke (ischaemic or haemorrhagic) | 1085 (2.4%) | 2111 (1.6%) | <0.001 |
| Intracerebral bleeding | 170 (0.4%) | 406 (0.3%) | 0.035 |
| Gastrointestinal bleeding | 904 (2.0%) | 2044 (1.6%) | <0.001 |
| Transfusion of blood constituents | 4752 (10.5%) | 9122 (7.0%) | <0.001 |
| Univariate Regression Model | Multivariate Regression Model * | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| In-hospital death | 1.717 (1.673–1.763) | <0.001 | 1.258 (1.222–1.296) | <0.001 |
| MACCE | 1.752 (1.708–1.797) | <0.001 | 1.236 (1.201–1.271) | <0.001 |
| Pneumonia | 1.635 (1.599–1.673) | <0.001 | 1.380 (1.346–1.414) | <0.001 |
| ARDS | 1.703 (1.637–1.772) | <0.001 | 1.530 (1.466–1.597) | <0.001 |
| Venous thromboembolism | 1.059 (0.993–1.128) | 0.079 | 1.021 (0.954–1.092) | 0.554 |
| Acute renal failure | 2.148 (2.085–2.212) | <0.001 | 1.486 (1.439–1.534) | <0.001 |
| Myocardial infarction | 1.940 (1.796–2.095) | <0.001 | 1.059 (0.975–1.150) | 0.176 |
| Cardiopulmonary resuscitation | 1.972 (1.829–2.127) | <0.001 | 1.476 (1.361–1.601) | <0.001 |
| Stroke (ischemic or hemorrhagic) | 1.499 (1.392–1.615) | <0.001 | 1.170 (1.082–1.264) | <0.001 |
| Intracerebral bleeding | 1.213 (1.013–1.451) | 0.035 | 1.096 (0.908–1.322) | 0.339 |
| Gastrointestinal bleeding | 1.286 (1.188–1.391) | <0.001 | 0.980 (0.902–1.065) | 0.639 |
| Transfusion of blood constituents | 1.567 (1.511–1.626) | <0.001 | 1.157 (1.112–1.204) | <0.001 |
| Mechanical ventilation | 1.739 (1.673–1.808) | <0.001 | 1.494 (1.433–1.558) | <0.001 |
| ECMO | 1.296 (1.159–1.449) | <0.001 | 1.436 (1.270–1.623) | <0.001 |
| Dialysis | 2.338 (2.215–2.468) | <0.001 | 1.559 (1.468–1.655) | <0.001 |
| Post-COVID status | 1.086 (0.901–1.310) | 0.384 | 1.029 (0.844–1.256) | 0.775 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmitt, V.H.; Hobohm, L.; Sagoschen, I.; Sivanathan, V.; Hahad, O.; Espinola-Klein, C.; Münzel, T.; Keller, K. Diabetes Mellitus and Its Association with Adverse In-Hospital Outcomes in Patients with COVID-19—A Nationwide Study. Viruses 2023, 15, 1627. https://doi.org/10.3390/v15081627
Schmitt VH, Hobohm L, Sagoschen I, Sivanathan V, Hahad O, Espinola-Klein C, Münzel T, Keller K. Diabetes Mellitus and Its Association with Adverse In-Hospital Outcomes in Patients with COVID-19—A Nationwide Study. Viruses. 2023; 15(8):1627. https://doi.org/10.3390/v15081627
Chicago/Turabian StyleSchmitt, Volker H., Lukas Hobohm, Ingo Sagoschen, Visvakanth Sivanathan, Omar Hahad, Christine Espinola-Klein, Thomas Münzel, and Karsten Keller. 2023. "Diabetes Mellitus and Its Association with Adverse In-Hospital Outcomes in Patients with COVID-19—A Nationwide Study" Viruses 15, no. 8: 1627. https://doi.org/10.3390/v15081627