
Dominant CT Patterns and Immune Responses during the Early Infection Phases of Different SARS-CoV-2 Variants
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
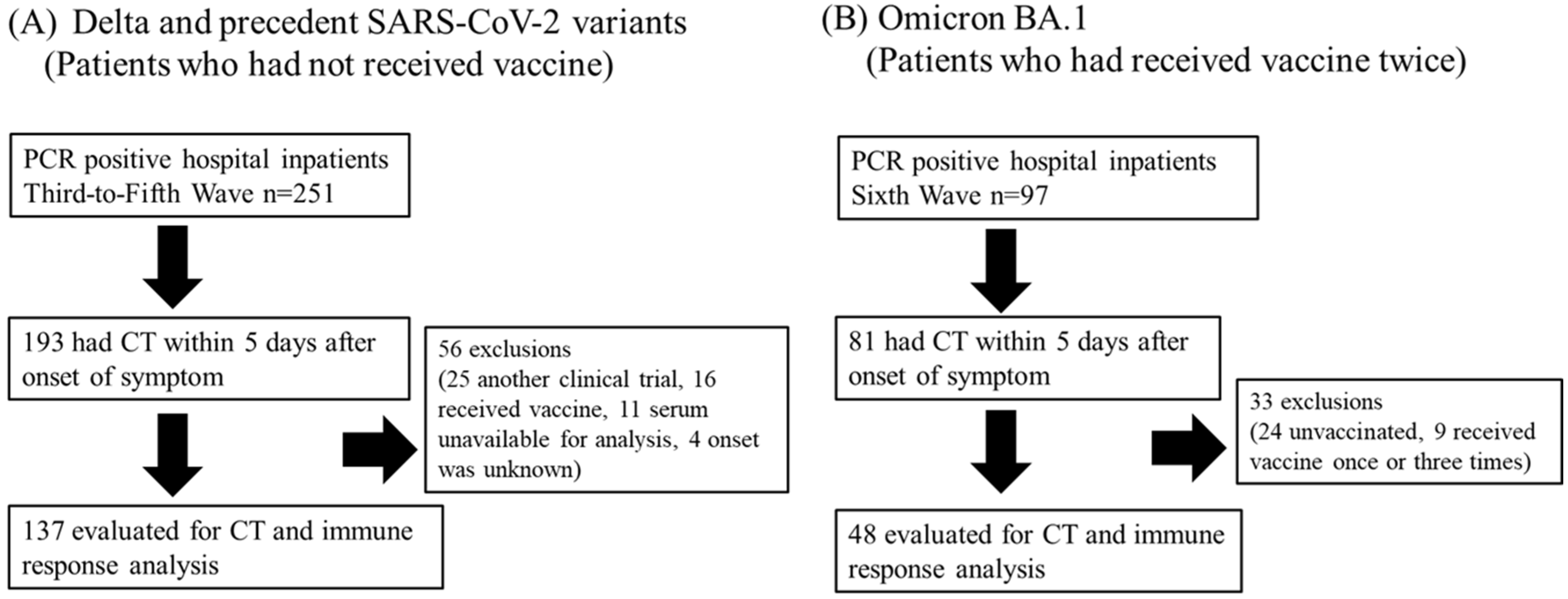
2.1. Study Design
2.2. Study Participants and Study Protocol
2.3. Image Analysis and Classification of CT Patterns
2.4. Chest CT Score
2.5. Cytokine Measurement
2.6. RT-qPCR
2.7. Pseudovirus Neutralization Assay
2.8. Statistical Analysis
3. Results
3.1. Clinical Features of Participants in This Study
3.2. Radiological Findings
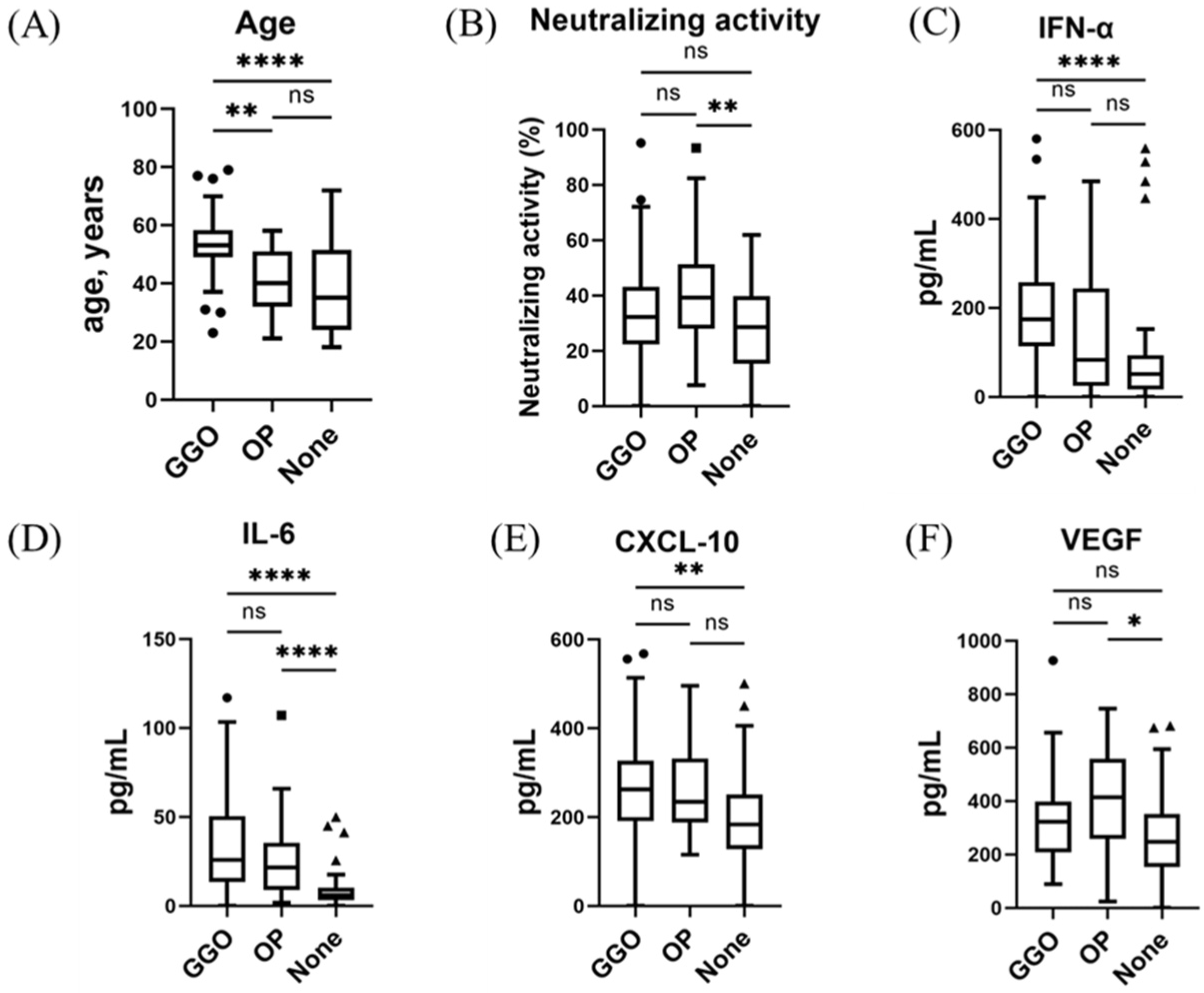
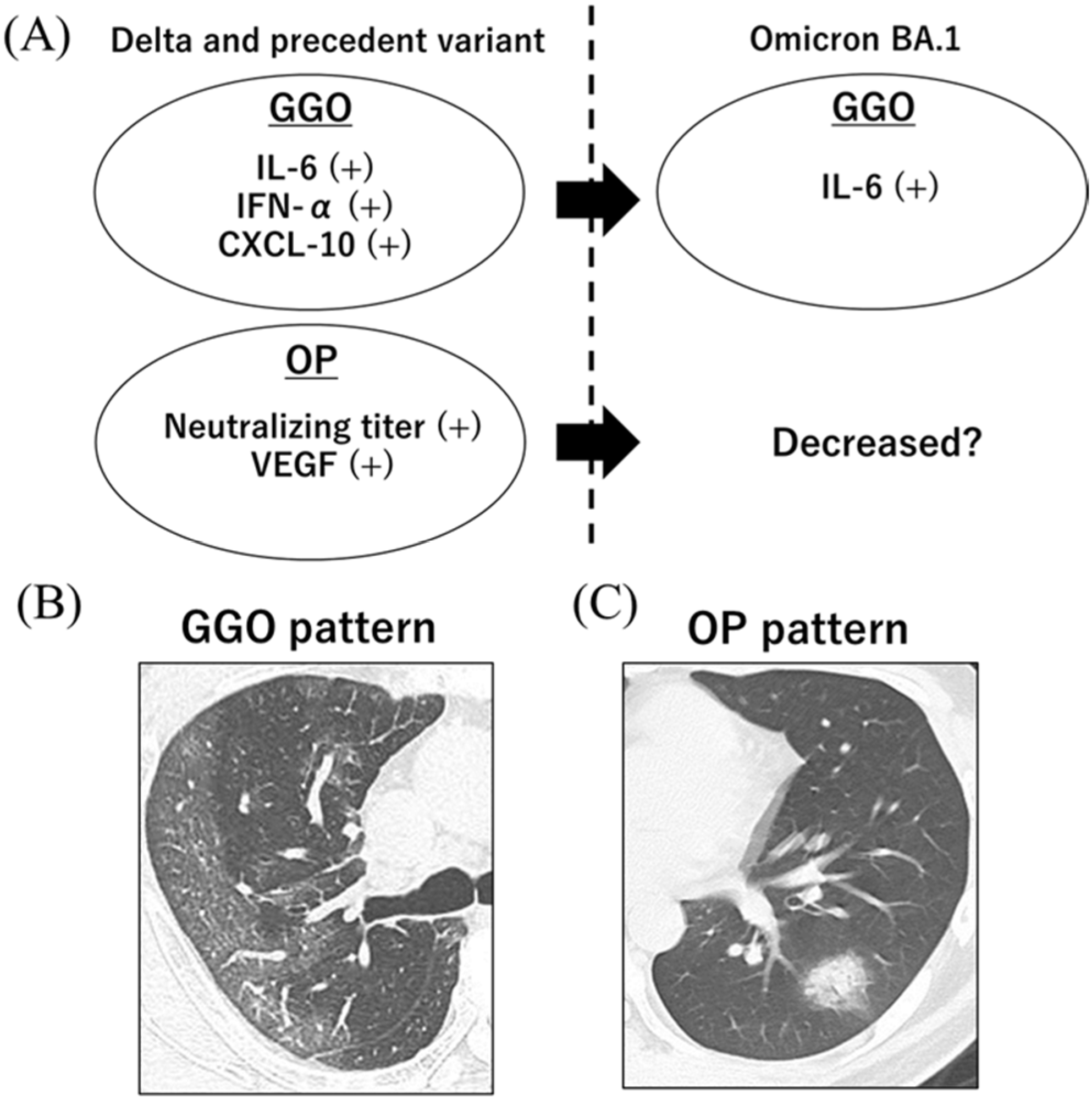
3.3. Serum Immune Indicators and Dominant CT Patterns at the Early Phase of SARS-CoV-2 Infection
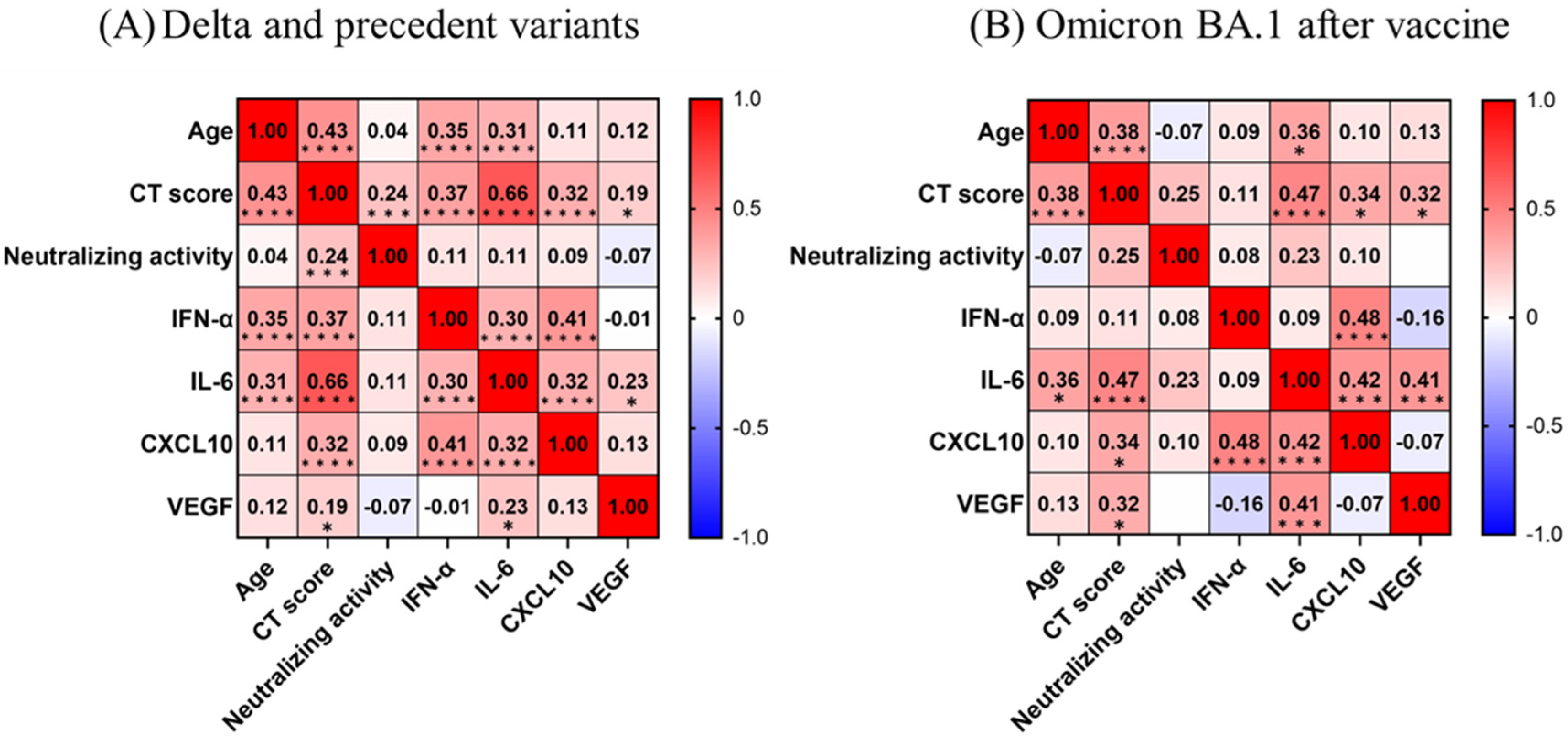
3.4. Correlations among CT Score and Immune Indicator Levels
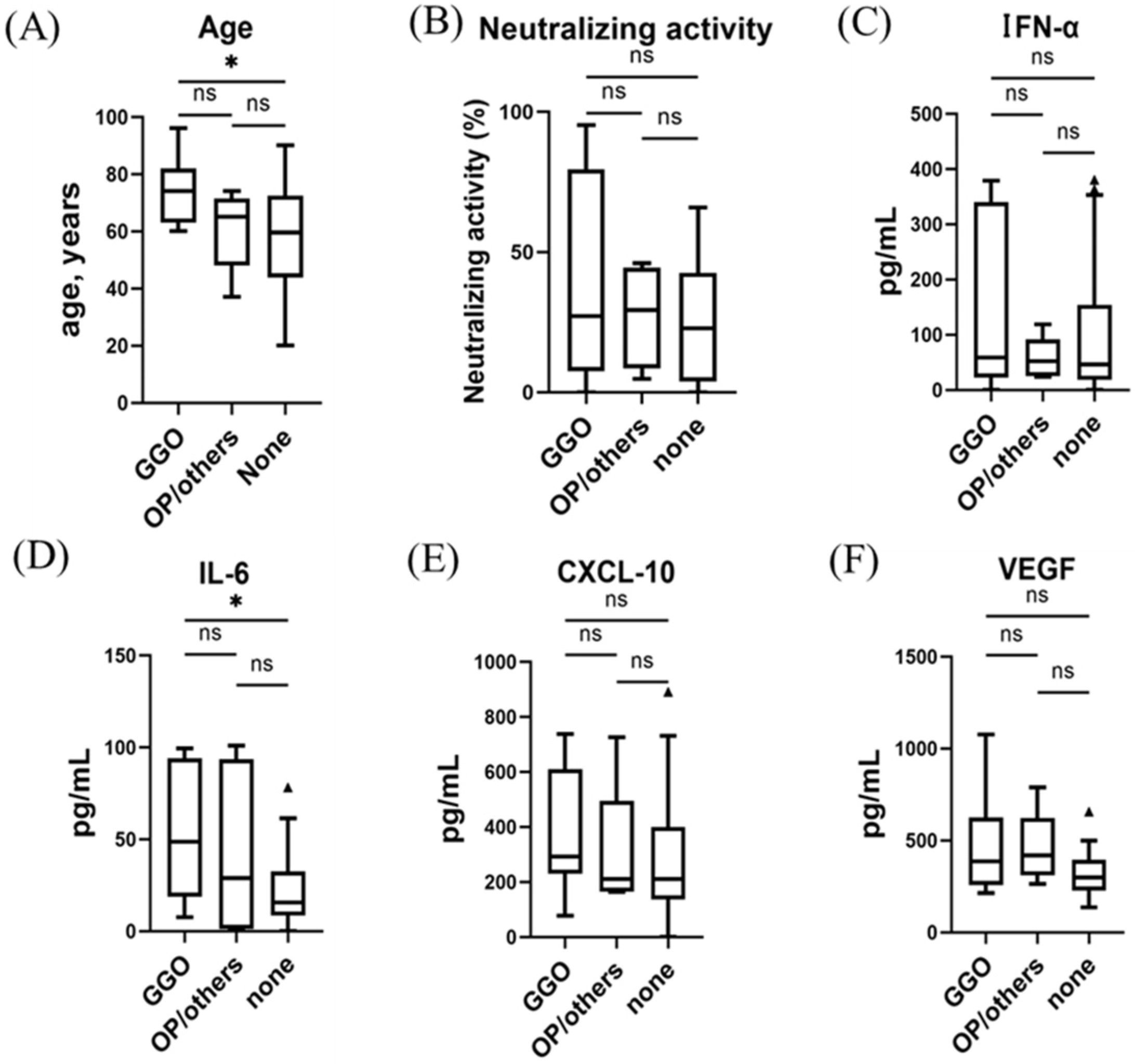
3.5. Serum Immune Indicator Levels and CT Findings in Unvaccinated Participants with the Omicron Variant
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Weekly Epidemiological Update on COVID-19- 19–25 May 2023; Edition 144. 2023. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---25-may-2023 (accessed on 29 May 2023).
- Ranney, M.L.; Valerie Griffeth, M.P.H.; Jha, A.K. Critical Supply Shortages—The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef] [PubMed]
- Mareiniss, D.P. The impending storm: COVID-19, pandemics and our overwhelmed emergency departments. Am. J. Emerg. Med. 2020, 38, 1293–1294. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Kmiec, D.; Koepke, L.; Zech, F.; Jacob, T.; Sparrer, K.-M.-J.; Kirchhoff, F. Omicron: What Makes the Latest SARS-CoV-2 Variant of Concern So Concerning? J. Virol. 2022, 96, e0207721. [Google Scholar] [CrossRef] [PubMed]
- Basso, P.; Negro, C.; Cegolon, L.; Filon, F.-L. Risk of Vaccine Breakthrough SARS-CoV-2 Infection and Associated Factors in Healthcare Workers of Trieste Teaching Hospitals (North-Eastern Italy). Viruses 2022, 14, 336. [Google Scholar] [CrossRef]
- Ulloa, A.-C.; Buchan, S.-A.; Daneman, N.; Brown, K.-A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.-G.; Everatt, J.; Bhiman, J.-N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Hui, K.-P.-Y.; Ho, J.-C.-W.; Cheung, M.-C.; Ng, K.-C.; Ching, R.-H.-H.; Lai, K.-L.; Kam, T.-T.; Gu, H.; Sit, K.-Y.; Hsin, M.-K.-Y.; et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef]
- Guo, K.; Barrett, B.-S.; Morrison, J.-H.; Mickens, K.-L.; Vladar, E.-K.; Hasenkrug, K.-J.; Hasenkrug, K.-J.; Poeschla, E.-M.; Santiago, M.-L. Interferon resistance of emerging SARS-CoV-2 variants. Proc. Natl. Acad. Sci. USA 2022, 119, e2203760119. [Google Scholar] [CrossRef]
- Alfi, O.; Hamdan, M.; Wald, O.; Yakirevitch, A.; Wandel, O.; Oiknine-Djian, E.; Gvili, B.; Knoller, H.; Rozendorn, N.; Golan Berman, H.; et al. SARS-CoV-2 Omicron Induces Enhanced Mucosal Interferon Response Compared to other Variants of Concern, Associated with Restricted Replication in Human Lung Tissues. Viruses 2022, 14, 1583. [Google Scholar] [CrossRef]
- Tsakok, M.-T.; Watson, R.-A.; Saujani, S.-J.; Kong, M.; Xie, C.; Peschl, H.; Wing, L.; MacLeod, F.-K.; Shine, B.; Talbot, N.-P.; et al. Reduction in Chest CT Severity and Improved Hospital Outcomes in SARS-CoV-2 Omicron Compared with Delta Variant Infection. Radiology 2023, 306, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Crombé, A.; Bensid, L.; Seux, M.; Fadli, D.; Arnaud, F.; Benhamed, A.; Banaste, N.; Gorincour, G. Impact of Vaccination and the Omicron Variant on COVID-19–related Chest CT Findings: A Multicenter Study. Radiology 2023, 307, 222730, Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Koh, J.; Jeon, Y.K.; Goo, J.M.; Yoon, S.H. An Integrated Radiologic-Pathologic Understanding of COVID-19 Pneumonia. Radiology 2023, 306, e222600. [Google Scholar] [CrossRef] [PubMed]
- Ojha, V.; Mani, A.; Pandey, N.N.; Sharma, S.; Kumar, S. CT in coronavirus disease 2019 (COVID-19): A systematic review of chest CT findings in 4410 adult patients. Eur. Radiol. 2020, 30, 6129–6138. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef]
- Tabatabaei, S.M.H.; Rahimi, H.; Moghaddas, F.; Rajebi, H. Predictive value of CT in the short-term mortality of Coronavirus Disease 2019 (COVID-19) pneumonia in nonelderly patients: A case-control study. Eur. J. Radiol. 2020, 132, 109298. [Google Scholar] [CrossRef]
- Coperchini, F.; Chiovato, L.; Rotondi, M. Interleukin-6, CXCL10 and Infiltrating Macrophages in COVID-19-Related Cytokine Storm: Not One for All but All for One! Front. Immunol. 2021, 12, 668507. [Google Scholar] [CrossRef]
- Fabris, M.; Del Ben, F.; Sozio, E.; Beltrami, A.P.; Cifù, A.; Bertolino, G.; Caponnetto, F.; Cotrufo, M.; Tascini, C.; Curcio, F. Cytokines from Bench to Bedside: A Retrospective Study Identifies a Definite Panel of Biomarkers to Early Assess the Risk of Negative Outcome in COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 4830. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Auto-antibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Guerra-López, J.A.; Amezcua-Castillo, L.M.; González-Pacheco, H.; Amezcua-Guerra, L.M. Levels of Vascular Endothelial Growth Factor and Its Association with Pulmonary Embolism in COVID-19. J. Interf. Cytokine Res. 2022, 42, 444–448. [Google Scholar] [CrossRef]
- Pradenas, E.; Ubals, M.; Urrea, V.; Suñer, C.; Trinité, B.; Riveira-Muñoz, E.; Marfil, S.; Ávila-Nieto, C.; Rodríguez de la Concepción, M.-L.; Tarrés-Freixas, F.; et al. Virological and Clinical Determinants of the Magnitude of Humoral Responses to SARS-CoV-2 in Mild-Symptomatic Individuals. Front. Immunol. 2022, 13, 860215. [Google Scholar] [CrossRef]
- Kawasuji, H.; Morinaga, Y.; Tani, H.; Saga, Y.; Yamada, H.; Yoshida, Y.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K.; et al. Neutralizing Antibody Response of the Wild-Type/Omicron BA.1 Bivalent Vaccine as the Second Booster Dose against Omicron BA.2 and BA.5. Microbiol. Spectr. 2023, 11, e0513122. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Lu, M.-C.; Yang, S.-F.; Bien, M.-Y.; Chen, Y.-F.; Li, Y.-T. Respiratory care for the critical patients with 2019 novel coronavirus. Respir. Med. 2021, 186, 106516. [Google Scholar] [CrossRef]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef]
- Prokop, M.; Van Everdingen, W.; van Rees Vellinga, T.; Quarles van Ufford, H.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS: A categorical CT assessment scheme for patients suspected of having COVID-19—definition and evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef]
- Machnicki, S.; Patel, D.; Singh, A.; Talwar, A.; Mina, B.; Oks, M.; Makkar, P.; Naidich, D.; Mehta, A.; Hill, N.-S.; et al. The usefulness of chest CT imaging in patients with suspected or diagnosed COVID-19: A review of literature. Chest 2021, 160, 652–670. [Google Scholar] [CrossRef]
- Kawasuji, H.; Morinaga, Y.; Tani, H.; Yoshida, Y.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K.; Ueno, A.; Miyajima, Y.; et al. SARS-CoV-2 RNAemia with higher nasopharyngeal viral load is strongly associated with severity and mortality in patients with COVID-19. J. Med. Virol. 2021, 10, 147–153. [Google Scholar] [CrossRef]
- Morinaga, Y.; Tani, H.; Terasaki, Y.; Nomura, S.; Kawasuji, H.; Shimada, T.; Igarashi, E.; Saga, Y.; Yoshida, Y.; Yasukochi, R.; et al. Correlation of the Commercial Anti-SARS-CoV-2 Receptor Binding Domain Antibody Test with the Chemiluminescent Reduction Neutralizing Test and Possible Detection of Antibodies to Emerging Variants. Microbiol. Spectr. 2021, 9, e0056021. [Google Scholar] [CrossRef]
- Nagaoka, K.; Kawasuji, H.; Takegoshi, Y.; Murai, Y.; Kaneda, M.; Ueno, A.; Miyajima, Y.; Wakasugi, M.; Noguchi, K.; Morimoto, S.; et al. Association of subpleural ground-glass opacities with respiratory failure and RNAemia in COVID-19. Eur. Radiol. 2023, 1–10, ahead of print. [Google Scholar] [CrossRef]
- Hariri, L.-P.; North, C.-M.; Shih, A.-R.; Israel, R.-A.; Maley, J.-H.; Villalba, J.-A.; Vinarsky, V.; Rubin, J.; Okin, D.-A.; Sclafani, A.; et al. Lung Histopathology in Coronavirus Disease 2019 as Compared With Severe Acute Respiratory Sydrome and H1N1 Influenza: A Systematic Review. Chest 2021, 159, 73–84. [Google Scholar] [CrossRef]
- Pogatchnik, B.P.; Swenson, K.E.; Sharifi, H.; Bedi, H.; Berry, G.J.; Guo, H.H. Radiology–Pathology Correlation Demonstrating Organizing Pneumonia in a Patient Who Recovered from COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 598–599. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jin, C.; Wu, C.C.; Zhao, H.; Liang, T.; Liu, Z.; Jian, Z.; Li, R.; Wang, Z.; Li, F.; et al. Organizing pneumonia of COVID-19: Time-dependent evolution and outcome in CT findings. PLoS ONE 2020, 15, e0240347. [Google Scholar] [CrossRef] [PubMed]
- Tajuelo, A.; Carretero, O.; García-Ríos, E.; López-Siles, M.; Cano, O.; Vázquez, M.; Más, V.; Rodríguez-Goncer, I.; Lalueza, A.; López-Medrano, F.; et al. Brief Research Report: Virus-Specific Humoral Immunity at Admission Predicts the Development of Respiratory Failure in Unvaccinated SARS-CoV-2 Patients. Front. Immunol. 2022, 13, 878812. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.-S.; Cromer, D.; Reynaldi, A.; Schlub, T.-E.; Wheatley, A.-K.; Juno, J.-A.; Subbarao, K.; Kent, S.-J.; Triccas, J.-A.; Davenport, M.-P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Cegolon, L.; Mastrangelo, G.; Bellizzi, S.; Filon, F.-L.; Salata, C. Supporting the Aspecific Physiological Defenses of Upper Airways against Emerging SARS-CoV-2 Variants. Pathogens 2023, 12, 211. [Google Scholar] [CrossRef]
- Pires, L.; Wilson, B.C.; Bremner, R.; Lang, A.; Larouche, J.; McDonald, R.; Pearson, J.D.; Trcka, D.; Wrana, J.; Wu, J.; et al. Translational feasibility and efficacy of nasal photodynamic disinfection of SARS-CoV-2. Sci. Rep. 2022, 12, 14438. [Google Scholar] [CrossRef]
- Nagaoka, K.; Kawasuji, H.; Murai, Y.; Kaneda, M.; Ueno, A.; Miyajima, Y.; Fukui, Y.; Morinaga, Y.; Yamamoto, Y. Circulating Type I Interferon Levels in the Early Phase of COVID-19 Are Associated With the Development of Respiratory Failure. Front. Immunol. 2022, 13, 844304. [Google Scholar] [CrossRef]
- Saleki, K.; Yaribash, S.; Banazadeh, M.; Hajihosseinlou, E.; Gouravani, M.; Saghazadeh, A.; Rezaei, N. Interferon therapy in patients with SARS, MERS, and COVID-19: A systematic review and meta-analysis of clinical studies. Eur. J. Pharmacol. 2021, 906, 174248. [Google Scholar] [CrossRef]
- Chen, L.-D.; Zhang, Z.-Y.; Wei, X.-J.; Cai, Y.-Q.; Yao, W.-Z.; Wang, M.-H.; Huang, Q.-F.; Zhang, X.-B. Association between cytokine profiles and lung injury in COVID-19 pneumonia. Respir. Res. 2020, 21, 201. [Google Scholar] [CrossRef]
- Rutkowska, E.; Kwiecień, I.; Żabicka, M.; Maliborski, A.; Raniszewska, A.; Kłos, K.; Urbańska, W.; Klajnowicz, I.; Rzepecki, P.; Chciałowski, A. Cytokines and Leukocytes Subpopulations Profile in SARS-CoV-2 Patients Depending on the CT Score Severity. Viruses 2021, 13, 880. [Google Scholar] [CrossRef]
- Cegolon, L.; Pol, R.; Simonetti, O.; Filon, F.L.; Luzzati, R. Molnupiravir, Nirmatrelvir/Ritonavir, or Sotrovimab for High-Risk COVID-19 Patients Infected by the Omicron Variant: Hospitalization, Mortality, and Time until Negative Swab Test in Real Life. Pharmaceuticals 2023, 16, 721. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Belati, A.; Tulone, O.; Diella, L.; Bavaro, D.F.; Bonica, R.; Genna, V.; Smith, L.; Trott, M.; Bruyere, O.; et al. Incidence of long COVID-19 in people with previous SARS-Cov2 infection: A systematic review and meta-analysis of 120,970 patients. Intern. Emerg. Med. 2022, 1–9, ahead of print. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Delta and Precedent Variants (n = 137) | Omicron BA.1 after Vaccine (n = 48) | p-Value | |
|---|---|---|---|
| Age, years | 49 (32–54) | 63 (51–74) | <0.001 |
| Sex; number of male/female | 79/58 | 31/17 | 0.401 |
| Underlying disease | |||
| None | 74 (54) | 14 (29) | 0.003 |
| Hypertension | 25 (18) | 20 (42) | 0.001 |
| Diabetes mellitus | 8 (6) | 8 (17) | 0.046 |
| Body mass index (kg/m2) | 22.5 (21–25] | 25.4 (23–28] | <0.001 |
| Initial nasopharyngeal viral load (log copies/μL) | 4.8 (3.8–5.6] | 4.4 (4.0–5.0] | 0.112 |
| RNAemia | 31 (23) | 5 (10) | 0.104 |
| Laboratory data | |||
| Neutrophil-to-lymphocyte ratio | 2.6 (1.6–4.0) | 2.9 (1.9–5.8] | 0.055 |
| LDH (IU/L) | 195 (173–217] | 180 (166–209] | 0.338 |
| CRP (mg/dL) | 0.6 (0.2–1.7] | 1.3 (0.8–3.3] | 0.046 |
| D-dimer (ng/mL) | 0.7 (0.6–0.9] | 0.8 (0.6–1.5] | 0.260 |
| Respiratory failure | 33 (24) | 8 (17) | 0.389 |
| Duration of oxygen therapy (days) | 7 (4–11] | 9.5 (3–30] | 0.153 |
| IPPV | 2 | 2 | 0.594 |
| Nasal high flow | 4 | 0 | 0.535 |
| Death within 30 days after onset | 0 (0%) | 0 (0%) | — |
| Delta and Precedent Variants (n = 137) | Omicron BA.1 after Vaccine (n = 48) | p-Value | |
|---|---|---|---|
| CT-evaluated day from clinical onset | 3 (2–4] | 2 (1–3] | 0.003 |
| Absence of abnormal pulmonary lesions | 61 (45) | 32 (67) | 0.008 |
| Semi-quantitative CT score | 1.5 (0–6] | 0 [0,1] | 0.041 |
| Dominant CT pattern | |||
| GGOs | 46 (34) | 11 (23) | 0.169 |
| OP | 27 (20) | 1 (2) | 0.007 |
| Others | 3 (2) | 4 (8) | 0.139 |
| Accompanied CT manifestation | |||
| Reversed halo shadow | 7 (5) | 2 (4) | 1.000 |
| Curvilinear shadow | 15 (11) | 5 (10) | 1.000 |
| Bronchovascular bundle thickening | 17 (12) | 6 (13) | 1.000 |
| Traction bronchial dilation | 3 (2) | 2 (4) | 0.834 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagaoka, K.; Kawasuji, H.; Takegoshi, Y.; Murai, Y.; Kaneda, M.; Kimoto, K.; Tani, H.; Niimi, H.; Morinaga, Y.; Noguchi, K.; et al. Dominant CT Patterns and Immune Responses during the Early Infection Phases of Different SARS-CoV-2 Variants. Viruses 2023, 15, 1304. https://doi.org/10.3390/v15061304
Nagaoka K, Kawasuji H, Takegoshi Y, Murai Y, Kaneda M, Kimoto K, Tani H, Niimi H, Morinaga Y, Noguchi K, et al. Dominant CT Patterns and Immune Responses during the Early Infection Phases of Different SARS-CoV-2 Variants. Viruses. 2023; 15(6):1304. https://doi.org/10.3390/v15061304
Chicago/Turabian StyleNagaoka, Kentaro, Hitoshi Kawasuji, Yusuke Takegoshi, Yushi Murai, Makito Kaneda, Kou Kimoto, Hideki Tani, Hideki Niimi, Yoshitomo Morinaga, Kyo Noguchi, and et al. 2023. "Dominant CT Patterns and Immune Responses during the Early Infection Phases of Different SARS-CoV-2 Variants" Viruses 15, no. 6: 1304. https://doi.org/10.3390/v15061304