
The Elevated De Ritis Ratio on Admission Is Independently Associated with Mortality in COVID-19 Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Laboratory Findings
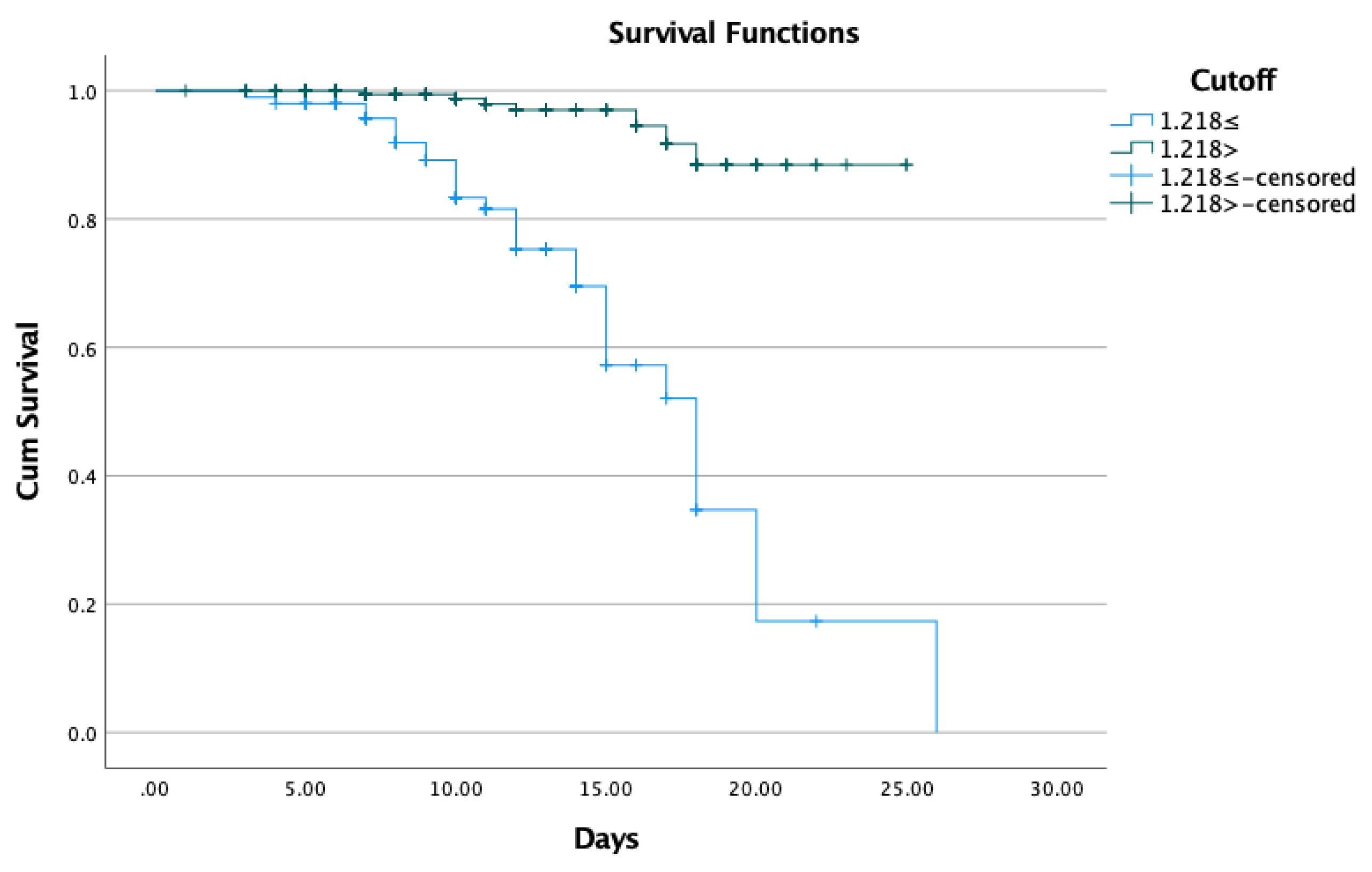
3.3. De Ritis Ratio as an Independent Predictor for In-Hospital Mortality in COVID-19 Patients
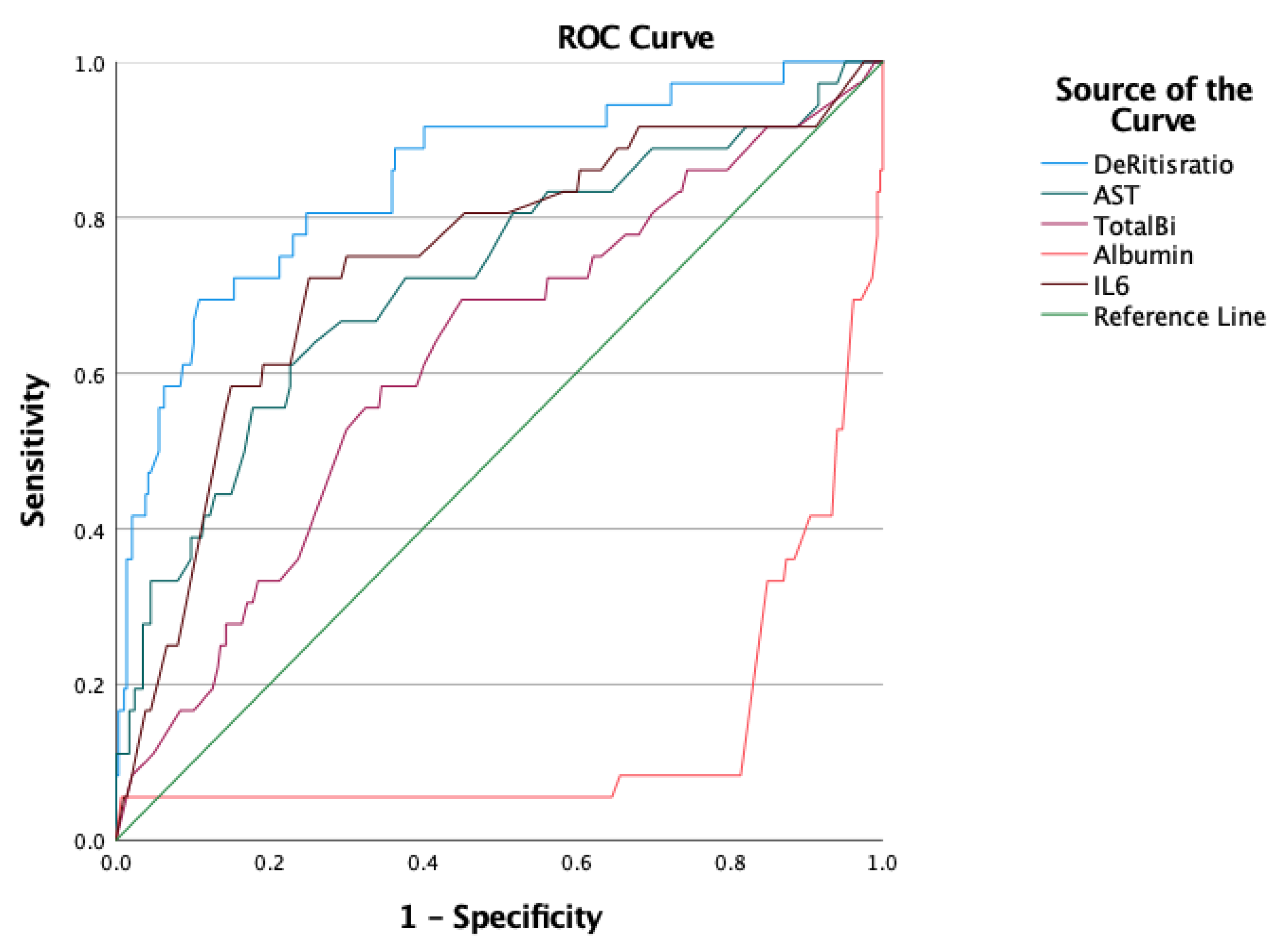
3.4. Predictive Value of the De Ritis Ratio for In-Hospital Mortality
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| OR | odds ratio |
| IQR | interquartile range |
| ROC | Receiver Operating Characteristic |
| MOF | multiple organ failure |
| CAID | cirrhosis-associated immune dysfunction |
| ACLF | acute-on-chronic liver failure |
| HRCT | high-resolution computer tomography |
| RT-PCR | reverse transcription-polimerase chain reaction |
| WHO | World Health Organization |
| ARDS | Acute respiratory distress syndrome |
| CRP | C-reactive protein |
| DILI | Drug-induced liver injury |
References
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 1 February 2022).
- WHO. Hungary Situtation—WHO COVID-19 Dashboard. Available online: https://covid19.who.int/region/euro/country/hu (accessed on 1 February 2022).
- Cha, M.H.; Regueiro, M.; Sandhu, D.S. Gastrointestinal and hepatic manifestations of COVID-19: A comprehensive review. World J. Gastroenterol. 2020, 26, 2323–2332. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhao, N.; Shu, Y.; Han, S.; Chen, B.; Shu, X. Effect of Gastrointestinal Symptoms in Patients With COVID-19. Gastroenterology 2020, 158, 2294–2297. [Google Scholar] [CrossRef] [PubMed]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and the liver. J. Hepatol. 2020, 73, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.A.; Schattenberg, J.M. Liver injury in COVID-19: The current evidence. United Eur. Gastroenterol. J. 2020, 8, 509–519. [Google Scholar] [CrossRef]
- Nardo, A.D.; Schneeweiss-Gleixner, M.; Bakail, M.; Dixon, E.D.; Lax, S.F.; Trauner, M. Pathophysiological mechanisms of liver injury in COVID-19. Liver Int. 2021, 41, 20–32. [Google Scholar] [CrossRef]
- Wu, J.; Song, S.; Cao, H.C.; Li, L.J. Liver diseases in COVID-19: Etiology, treatment and prognosis. World J. Gastroenterol. 2020, 26, 2286–2293. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.t.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef]
- Noor, M.T.; Manoria, P. Immune Dysfunction in Cirrhosis. J. Clin. Transl. Hepatol. 2017, 5, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano, S.; Brocca, A.; Mareso, S.; Angeli, P. Infections complicating cirrhosis. Liver Int. 2018, 38 (Suppl. S1), 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pose, E.; Coll, M.; Martínez-Sánchez, C.; Zeng, Z.; Surewaard, B.G.J.; Català, C.; Velasco-de Andrés, M.; Lozano, J.J.; Ariño, S.; Fuster, D.; et al. Programmed Death Ligand 1 Is Overexpressed in Liver Macrophages in Chronic Liver Diseases, and Its Blockade Improves the Antibacterial Activity Against Infections. Hepatology 2021, 74, 296–311. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.U.; Mushtaq, K.; Alkaabi, S.R. Acute-on-Chronic Liver Failure: Possibly the Main Culprit of Increased Mortality in COVID-19 Patients with Liver Disease. Gastroenterology 2021, 160, 1894–1895. [Google Scholar] [CrossRef] [PubMed]
- WHO. Laboratory Testing for Coronavirus Disease (COVID-19) in Suspected Human Cases; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Xu, Y.; Chen, Y.; Tang, X. Guidelines for the diagnosis and treatment of coronavirus disease 2019 (COVID-19) in China. Glob. Health Med. 2020, 2, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Gong, J.; Ou, J.; Qiu, X.; Jie, Y.; Chen, Y.; Yuan, L.; Cao, J.; Tan, M.; Xu, W.; Zheng, F.; et al. A Tool for Early Prediction of Severe Coronavirus Disease 2019 (COVID-19): A Multicenter Study Using the Risk Nomogram in Wuhan and Guangdong, China. Clin. Infect. Dis. 2020, 71, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhou, H.; Zhou, Y.; Wu, X.; Zhao, Y.; Lu, Y.; Tan, W.; Yuan, M.; Ding, X.; Zou, J.; et al. Risk factors associated with disease severity and length of hospital stay in COVID-19 patients. J. Infect. 2020, 81, e95–e97. [Google Scholar] [CrossRef]
- Ragab, D.; Salah Eldin, H.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 Cytokine Storm; What We Know So Far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Chinn, J.; Nahmias, J.; Yuen, S.; Kirby, K.A.; Hohmann, S.; Amin, A. Outcomes and Mortality Among Adults Hospitalized with COVID-19 at US Medical Centers. JAMA Netw. Open 2021, 4, e210417. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Hao, S.R.; Jia, H.Y.; Cai, H.; Zhang, X.L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical Characteristics of COVID-19 Patients with Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 among Patients with Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771.e3. [Google Scholar] [CrossRef]
- Mantovani, A.; Beatrice, G.; Dalbeni, A. Coronavirus disease 2019 and prevalence of chronic liver disease: A meta-analysis. Liver Int. 2020, 40, 1316–1320. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Shi, L.; Wang, F.S. Liver injury in COVID-19: Management and challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, L.; Liu, L.; Zhao, M.; Xiao, J.; Zhao, Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020, 40, 2095–2103. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Du, Q.; Yan, S.; Guo, X.G.; He, Y.; Zhu, G.; Zhao, K.; Ouyang, S. Liver injury in COVID-19: Clinical features and treatment management. Virol. J. 2021, 18, 121. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Higuera-de la Tijera, F.; Servín-Caamaño, A.; Reyes-Herrera, D.; Flores-López, A.; Robiou-Vivero, E.J.A.; Martínez-Rivera, F.; Galindo-Hernández, V.; Chapa-Azuela, O.; Chávez-Morales, A.; Rosales-Salyano, V.H. Impact of liver enzymes on SARS-CoV-2 infection and the severity of clinical course of COVID-19. Liver Res. 2021, 5, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Huang, I.; Lim, M.A.; Yonas, E.; Vania, R.; Lukito, A.A.; Nasution, S.A.; Siswanto, B.B.; Kuswardhani, R.A.T. Elevated De Ritis Ratio Is Associated With Poor Prognosis in COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 676581. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Arru, F.; De Vito, A.; Sassu, A.; Valdes, G.; Scano, V.; Zinellu, E.; Perra, R.; Madeddu, G.; Carru, C.; et al. The De Ritis ratio as prognostic biomarker of in-hospital mortality in COVID-19 patients. Eur. J. Clin. Investig. 2021, 51, e13427. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wei, Y.; Lyu, X.; Zhao, B.; Feng, Y.; Li, T.; Cao, H.; Yang, X.; Zhou, X.; Wang, W.; et al. High aspartate aminotransferase to alanine aminotransferase ratio on admission as risk factor for poor prognosis in COVID-19 patients. Sci. Rep. 2020, 10, 16496. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Vale, C.L.; Godolphin, P.J.; Fisher, D.; Higgins, J.P.T.; Spiga, F.; Savovic, J.; Tierney, J.; Baron, G.; Benbenishty, J.S.; et al. Association between Administration of IL-6 Antagonists and Mortality among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar]
- Sayah, W.; Berkane, I.; Guermache, I.; Sabri, M.; Lakhal, F.Z.; Yasmine Rahali, S.; Djidjeli, A.; Lamara Mahammed, L.; Merah, F.; Belaid, B.; et al. Interleukin-6, procalcitonin and neutrophil-to-lymphocyte ratio: Potential immune-inflammatory parameters to identify severe and fatal forms of COVID-19. Cytokine 2021, 141, 155428. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidemiological, Clinical Characteristics | Patients (n = 322) |
|---|---|
| * Age (years) | 66 (54–77) |
| Gender (male/female), n * Admission time (days) | 178/144 4 (3–6) |
| Hospital stay (days) | 11 (8–14) |
| GI symptoms n (%) | 57 (17.7) |
| Diarrhea, n (%) Vomit, n (%) Melaena, n (%) Ascites, n (%) | 31 (9.6) 5 (1.6) 5 (1.6) 7 (2.2) |
| Hipertension, n (%) | 171 (53) |
| Diabetes, n (%) | 100 (31) |
| Cancer, n (%) Anaemia, n (%) | 21 (6.5) 9 (2.8) |
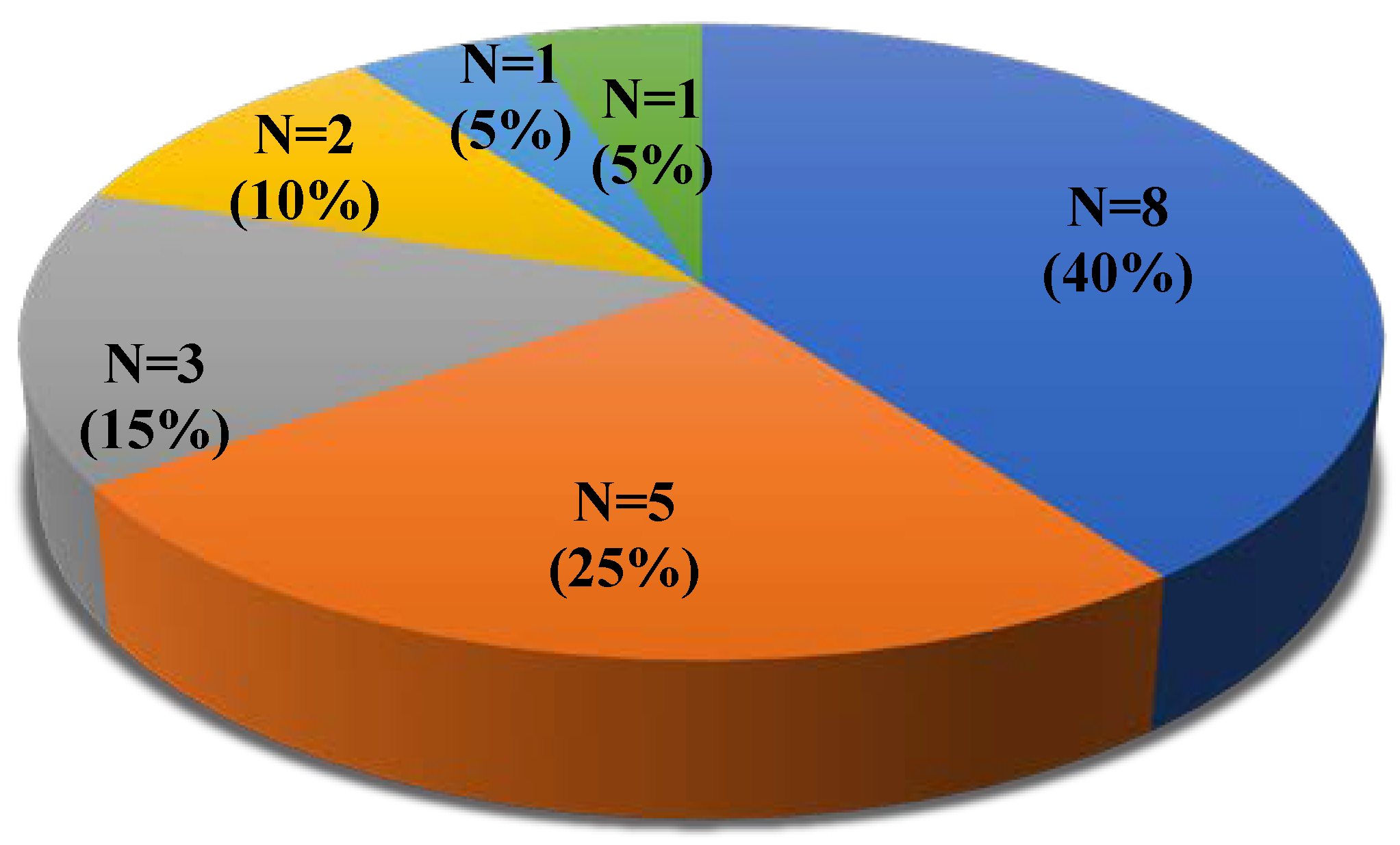
| Liver disease, n (%) cirrhosis, n Child–Pugh A, n Child–Pugh B, n Child–Pugh C, n without cirrhosis, n | 30 (9.3) 20 9 7 4 10 |
| Severity grade Mild, n (%) Moderate, n (%) Severe, n (%) Critical, n (%) In-hospital mortality rate, n (%) | 50 (15.5) 181 (56.2) 52 (16.1) 39 (12.1) 36(11.2) |
| Parameter | COVID-19 Recovered Patients n = 286 | COVID-19 Patients Who Died n = 36 | p |
|---|---|---|---|
| AST, mean (SD) | 33.1 (26) | 74.2 (78) | <0.001 |
| ALT, mean (SD) | 37.4 (29.6) | 48.4 (75.3) | 0.745 |
| De Ritis ratio, mean (SD) | 1.0 (.39) | 1.8 (.85) | <0.001 |
| GGT, mean (SD) | 91 (123) | 125 (169) | 0.437 |
| ALP, mean (SD) | 136.9 (126) | 189.7 (172) | 0.061 |
| Total bilirubin, mean (SD) | 33.1 (84.6) | 70.8 (154.4) | 0.019 |
| Albumin, mean (SD) | 35.7 (7) | 27.9 (13.7) | <0.001 |
| CRP, mean (SD) | 148.4 (230.9) | 260.3 (397.9) | 0.008 |
| PCT, mean (SD) | 6.67 (46.9) | 23.1 (92.5) | <0.001 |
| IL-6, mean (SD) | 39.6 (43.3) | 86.4 (60.7) | <0.001 |
| Age, mean (SD) | 63 (16) | 79 (10) | <0.001 |
| Admission time, mean (SD) Hospital days, mean (SD) | 5 (2.5) 11 (5) | 4 (2) 13 (5) | 0.495 0.077 |
| Diarrhea, n (%) | 30 (10.4) | 1 (2.7) | 0.139 |
| Ascites, n (%) | 5 (1.7) | 2 (5.5) | 0.140 |
| Hipertension, n (%) | 154 (53.8) | 17 (47.2) | 0.453 |
| Diabetes, n (%) | 91 (31.8) | 9 (25) | 0.405 |
| Liver disease, n (%) | 26 (9) | 4 (11.1) | 0.694 |
| Cirrhosis, n (%) | 17 (5.9) | 3 | 0.576 |
| Variable | β | SE | p | OR | CI 95% |
|---|---|---|---|---|---|
| AST | 0.034 | 0.010 | <0.001 | 1.034 | 1.015–1.054 |
| De Ritis ratio | 3.400 | 0.887 | <0.001 | 29.967 | 5.266–170.514 |
| Total bilirubin | 0.008 | 0.003 | 0.003 | 1.008 | 1.003–1.013 |
| CRP | −0.001 | 0.002 | 0.336 | 0.999 | 0.996–1.002 |
| PCT | 0.002 | 0.005 | 0.613 | 1.002 | 0.993–1.012 |
| IL-6 | 0.027 | 0.008 | <0.001 | 1.027 | 1.012–1.042 |
| Albumin | −0.293 | 0.058 | <0.001 | 0.746 | 0.666–0.836 |
| Age | 0.129 | 0.032 | <0.001 | 1.138 | 1.069–1.211 |
| Prognostic Marker | AUC (95% CI) | Cut-Off | Sensitivity | Specificity | p |
|---|---|---|---|---|---|
| AST | 0.723 (0.624–0.821) | 29.5 | 0.722 | 0.622 | <0.05 |
| De Ritis ratio | 0.850 (0.777–0.923) | 1.218 | 0.806 | 0.752 | <0.05 |
| Total bilirubin | 0.619 (0.519–0.719) | 10.1 | 0.722 | 0.437 | <0.05 |
| IL-6 | 0.743 (0.649–0.837) | 51.915 | 0.722 | 0.748 | <0.05 |
| Albumin | 0.133 (0.057–0.208) | 29.4 | 0.361 | 0.126 | <0.05 |
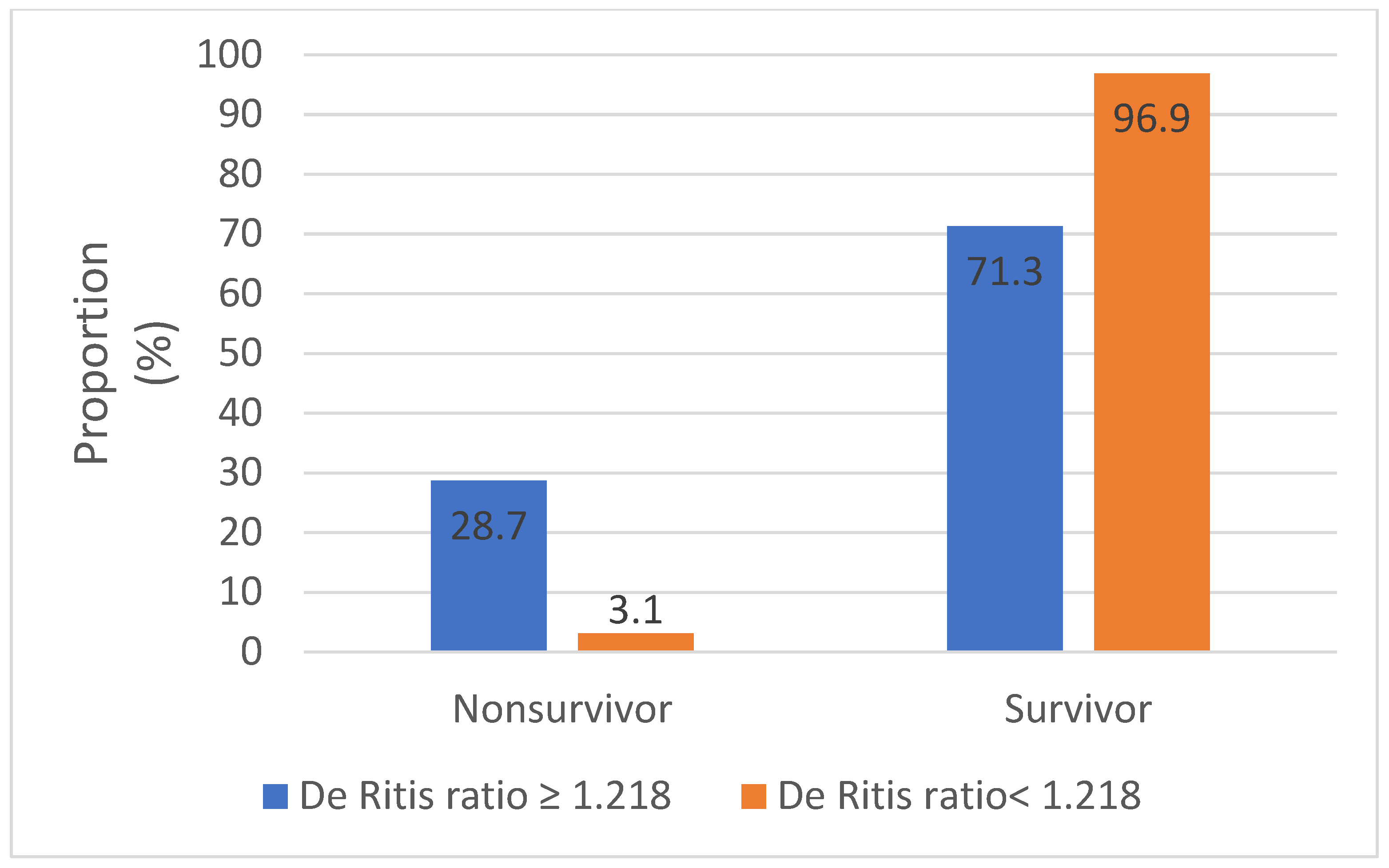
| Variable | De Ritis Ratio ≥ 1.218 n = 101 | De Ritis Ratio < 1.218 n = 221 | p |
|---|---|---|---|
| Mortality rate, n (%) | 29 (28.7) | 7 (3.1) | <0.001 |
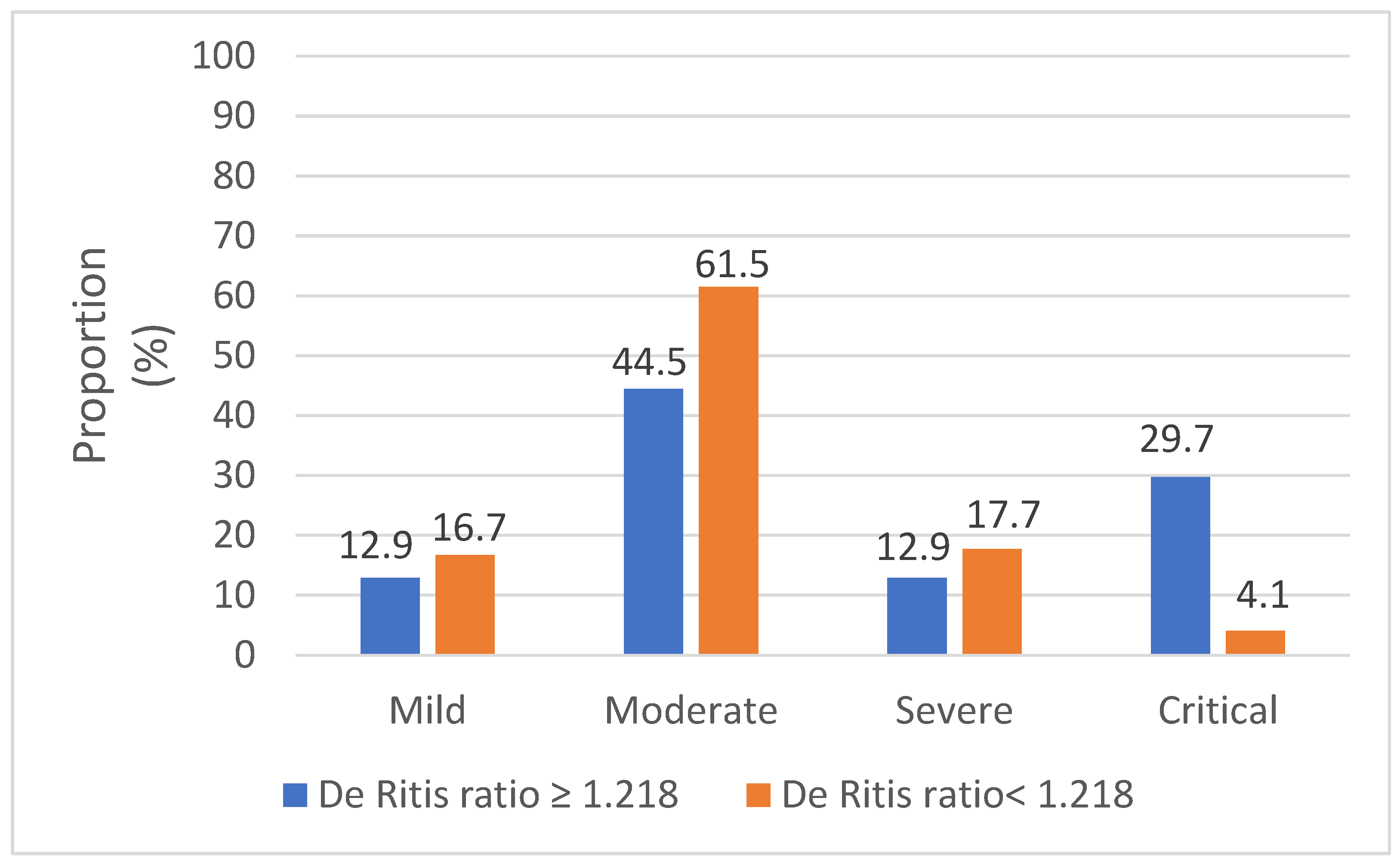
| Severity grade Mild, n (%) Moderate, n (%) Severe, n (%) Critical, n (%) | 13 (12.9) 45 (44.5) 13 (12.9) 30 (29.7) | 37 (16.7) 136 (61.5) 39 (17.7) 9 (4.1) | <0.001 |
| Gender (male/female), n | 50/51 | 128/93 | 0.159 |
| GI symptoms n (%) Diarrhea, n (%) Ascites, n (%) | 19 (18.8) 7 (6.9) 5 (5) | 38 (17.2) 24 (10.9) 2 (0.9) | 0.724 0.267 0.021 |
| Hypertension, n (%) | 51 (50.5) | 120 (54.3) | 0.526 |
| Diabetes, n (%) | 30 (29.7) | 70 (31.7) | 0.723 |
| Liver disease, n (%) cirrhosis, n | 9 (8.9) 6 (5.9) | 21 (9.5) 14 (6.3) | 0.865 |
| AST, mean (SD) | 45.9 (39) | 34 (36.8) | <0.001 |
| ALT, mean (SD) | 27.9 (19.8) | 43.5 (42.4) | <0.001 |
| Total bilirubin, mean (SD) | 41 (98.3) | 35.6 (94.1) | 0.133 |
| Albumin, mean (SD) | 34 (9.6) | 35.2 (7.7) | 0.088 |
| CRP, mean (SD) | 158.5 (256) | 162 (257.4) | 0.539 |
| PCT, mean (SD) | 13.2 (68) | 6.3 (46.2) | 0.449 |
| IL-6, mean (SD) | 56.9 (55.7) | 39.4 (42.8) | 0.006 |
| Age, mean (SD) | 70 (16) | 63 (16) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drácz, B.; Czompa, D.; Müllner, K.; Hagymási, K.; Miheller, P.; Székely, H.; Papp, V.; Horváth, M.; Hritz, I.; Szijártó, A.; et al. The Elevated De Ritis Ratio on Admission Is Independently Associated with Mortality in COVID-19 Patients. Viruses 2022, 14, 2360. https://doi.org/10.3390/v14112360
Drácz B, Czompa D, Müllner K, Hagymási K, Miheller P, Székely H, Papp V, Horváth M, Hritz I, Szijártó A, et al. The Elevated De Ritis Ratio on Admission Is Independently Associated with Mortality in COVID-19 Patients. Viruses. 2022; 14(11):2360. https://doi.org/10.3390/v14112360
Chicago/Turabian StyleDrácz, Bálint, Diána Czompa, Katalin Müllner, Krisztina Hagymási, Pál Miheller, Hajnal Székely, Veronika Papp, Miklós Horváth, István Hritz, Attila Szijártó, and et al. 2022. "The Elevated De Ritis Ratio on Admission Is Independently Associated with Mortality in COVID-19 Patients" Viruses 14, no. 11: 2360. https://doi.org/10.3390/v14112360