
Bacteriophage Therapy for Difficult-to-Treat Infections: The Implementation of a Multidisciplinary Phage Task Force (The PHAGEFORCE Study Protocol)

 , , , , , , , ,
, , , , , , , ,  ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Objectives
- -
- Implementing phage therapy in three medical disciplines and creating a prospective patient registry;
- -
- Gaining insight in the kinetics of phage therapy using three different routes of administration;
- -
- Characterizing the interaction between phage and bacteria and optimizing future phage cocktails by applying a genome-based approach.
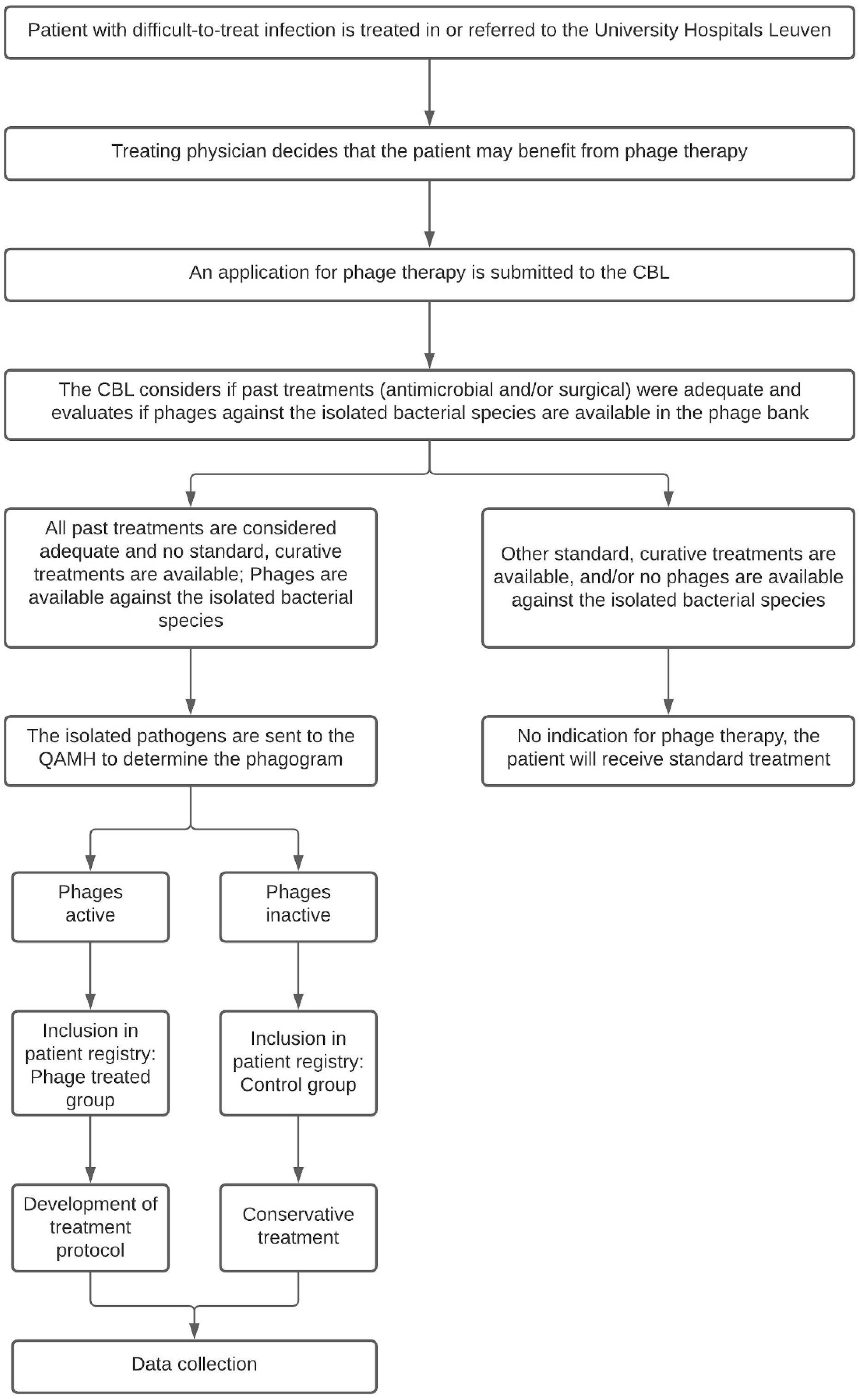
2.2. Study Design
2.3. Study Population
2.3.1. Sample Size Calculation
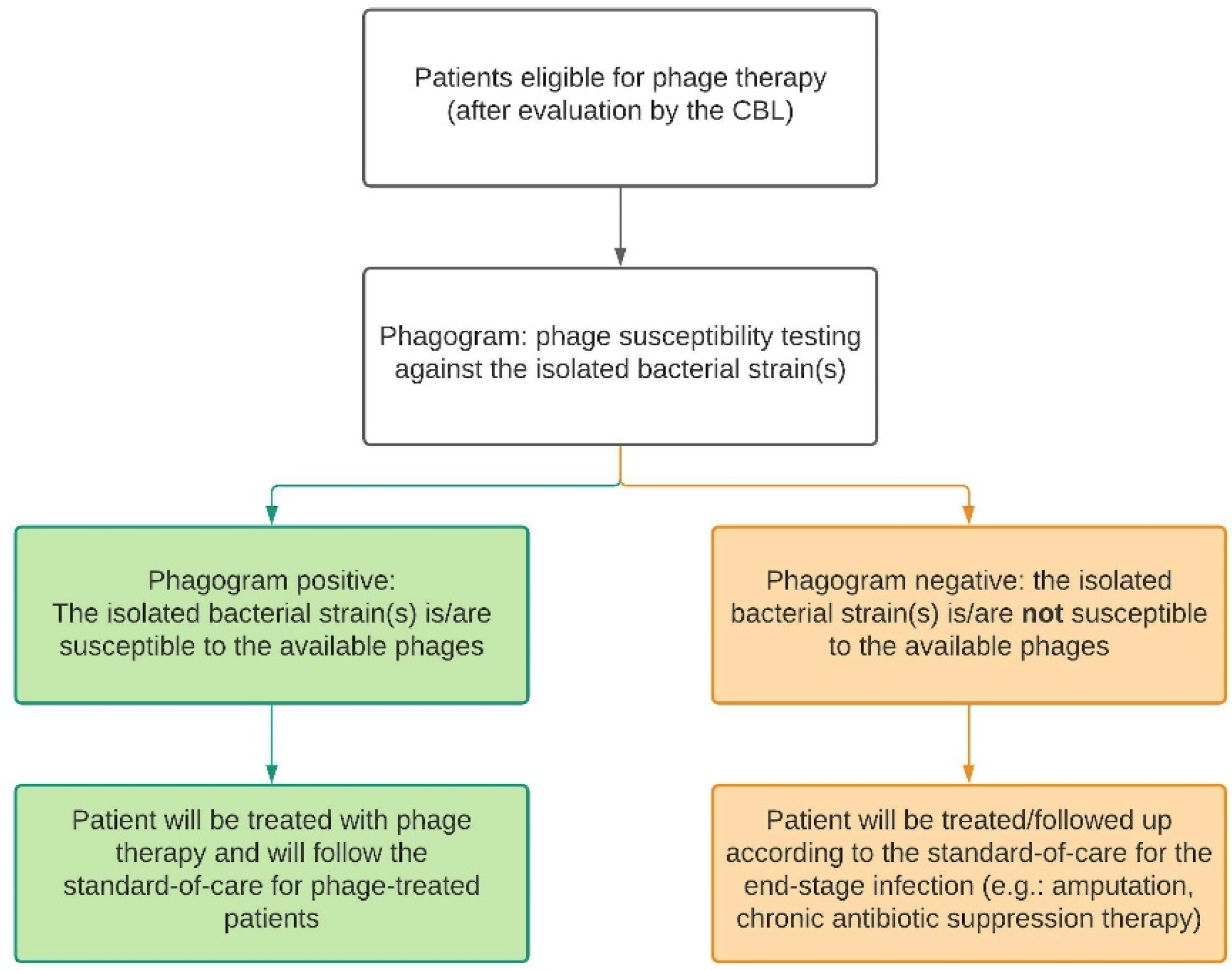
2.3.2. Eligibility
2.3.3. Inclusion Criteria
- -
- Diagnosed with a difficult-to-treat MSI, CRS or sepsis, and;
- -
- For whom all previous treatments (surgical and antibiotic) have failed or for whom no other curative treatment options are available (i.e., ‘last resort cases’, based on the CBL assessment), for example in case of bacterial resistance, and;
- -
- For whom phages targeting the isolated bacterial species are available in the phage bank, and;
- -
- Who have given informed consent to have their data collected in a patient registry.
2.3.4. Exclusion Criteria
- -
- With an infectious disease other than MSI, CRS or sepsis, and/or;
- -
- For whom standard curative treatment alternatives are still available, and/or;
- -
- For whom phages targeting the isolated bacterial species are not available in the phage bank, and/or;
- -
- Who refuse to give their informed consent.
2.4. Study Procedures
2.4.1. Baseline Parameters
2.4.2. Treatment-Specific Parameters: Phage Treatment Group
Phage Dynamics
- Assessment of Safety
- -
- Complete blood count (CBC);
- -
- Basic metabolic panel;
- -
- Inflammatory parameters;
- -
- Lactic acid, Creatine kinase;
- -
- Liver function tests;
- -
- Antiphage antibodies (serum);
- -
- Phage titration and isolation from draining fluid (MSI), nasal swabs (CRS) or serum (sepsis).
- Assessment of Efficacy
Phage Kinetics
2.4.3. Follow-Up Parameters: Phage Treatment Group
2.4.4. Treatment-Specific and Follow-Up Parameters: Control/Standard Treatment Group
2.5. Translational Research
2.5.1. Microbiological Analysis of Patient Bacterial Isolates and Identification of Novel or Long-Circulating Phage Mutants
2.5.2. Characterization of the Phage Library and Using Machine Learning to Predict Host Range Phenotype from the Genotype
2.6. Statistical Analysis
2.7. Ethics and Regulatory Approvals
2.8. Data Handling and Management
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- O’Neill, J. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. In Review on Antimicrobial Resistance; Wellcome Trust: London, UK, 2014. [Google Scholar]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Onsea, J.; Wagemans, J.; Pirnay, J.P.; Di Luca, M.; Gonzalez-Moreno, M.; Lavigne, R.; Trampuz, A.; Moriarty, T.F.; Metsemakers, W.J. Bacteriophage therapy as a treatment strategy for orthopaedic device-related infections: Where do we stand? Eur. Cells Mater. 2020, 39, 193–210. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Flemming, H.C.; Wingender, J.; Szewzyk, U.; Steinberg, P.; Rice, S.A.; Kjelleberg, S. Biofilms: An emergent form of bacterial life. Nat. Rev. Microbiol. 2016, 14, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Bowler, P.; Murphy, C.; Wolcott, R. Biofilm exacerbates antibiotic resistance: Is this a current oversight in antimicrobial stewardship? Antimicrob. Resist. Infect. Control. 2020, 9, 162. [Google Scholar] [CrossRef] [PubMed]
- Pirnay, J.P.; Verbeken, G.; Ceyssens, P.J.; Huys, I.; de Vos, D.; Ameloot, C.; Fauconnier, A. The Magistral Phage. Viruses 2018, 10, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onsea, J.; Soentjens, P.; Djebara, S.; Merabishvili, M.; Depypere, M.; Spriet, I.; de Munter, P.; Debaveye, Y.; Nijs, S.; Vanderschot, P.; et al. Bacteriophage Application for Difficult-to-treat Musculoskeletal Infections: Development of a Standardized Multidisciplinary Treatment Protocol. Viruses 2019, 11, 891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabrowska, K.; Abedon, S.T. Pharmacologically Aware Phage Therapy: Pharmacodynamic and Pharmacokinetic Obstacles to Phage Antibacterial Action in Animal and Human Bodies. Microbiol. Mol. Biol. Rev. MMBR 2019, 83, e00012–e00019. [Google Scholar] [CrossRef] [PubMed]
- Dufour, N.; Delattre, R.; Debarbieux, L. In Vivo Bacteriophage Biodistribution. In Bacteriophage Therapy; Azeredo, J., Sillankorva, S., Eds.; Humana Press: New York, NY, USA, 2018; Volume 1693, pp. 123–137. [Google Scholar]
- Dąbrowska, K. Phage therapy: What factors shape phage pharmacokinetics and bioavailability? Systematic and critical review. Med. Res. Rev. 2019, 39, 2000–2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cisek, A.A.; Dabrowska, I.; Gregorczyk, K.P.; Wyzewski, Z. Phage Therapy in Bacterial Infections Treatment: One Hundred Years After the Discovery of Bacteriophages. Curr. Microbiol. 2017, 74, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, D.J.; Sokolov, I.J.; Vinner, G.K.; Mancuso, F.; Cinquerrui, S.; Vladisavljevic, G.T.; Clokie, M.R.J.; Garton, N.J.; Stapley, A.G.F.; Kirpichnikova, A. Formulation, stabilisation and encapsulation of bacteriophage for phage therapy. Adv. Colloid Interface Sci. 2017, 249, 100–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmerer, M.; Molineux, I.J.; Bull, J.J. Synergy as a rationale for phage therapy using phage cocktails. PeerJ 2014, 2, e590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boon, M.; Holtappels, D.; Lood, C.; van Noort, V.; Lavigne, R. Host range expansion of Pseudomonas virus LUZ7 is driven by a conserved tail fiber mutation. PHAGE Ther. Appl. Res. 2020, 1, 87–90. [Google Scholar] [CrossRef]
- Burrowes, B.H.; Molineux, I.J.; Fralick, J.A. Directed in Vitro Evolution of Therapeutic Bacteriophages: The Appelmans Protocol. Viruses 2019, 11, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segall, A.M.; Roach, D.R.; Strathdee, S.A. Stronger together? Perspectives on phage-antibiotic synergy in clinical applications of phage therapy. Curr. Opin. Microbiol. 2019, 51, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Lood, C.; Peeters, C.; Lamy-Besnier, Q.; Wagemans, J.; de Vos, D.; Proesmans, M.; Pirnay, J.P.; Echahidi, F.; Piérard, D.; Thimmesch, M.; et al. Genomics of an endemic cystic fibrosis Burkholderia multivorans strain reveals low within-patient evolution but high between-patient diversity. PLoS Pathog. 2021, 17, e1009418. [Google Scholar] [CrossRef]
- De Smet, J.; Hendrix, H.; Blasdel, B.G.; Danis-Wlodarczyk, K.; Lavigne, R. Pseudomonas predators: Understanding and exploiting phage-host interactions. Nat. Rev. Microbiol. 2017, 15, 517–530. [Google Scholar] [CrossRef]
- Uyttebroek, S.; Chen, B.; Onsea, J.; Ruythooren, F.; Debaveye, Y.; Devolder, D.; Spriet, I.; Depypere, M.; Wagemans, J.; Lavigne, R.; et al. Safety and efficacy of phage therapy in difficult-to-treat infections: A systematic review. Lancet Infect. Dis. 2021, under review. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onsea, J.; Uyttebroek, S.; Chen, B.; Wagemans, J.; Lood, C.; Van Gerven, L.; Spriet, I.; Devolder, D.; Debaveye, Y.; Depypere, M.; et al. Bacteriophage Therapy for Difficult-to-Treat Infections: The Implementation of a Multidisciplinary Phage Task Force (The PHAGEFORCE Study Protocol). Viruses 2021, 13, 1543. https://doi.org/10.3390/v13081543
Onsea J, Uyttebroek S, Chen B, Wagemans J, Lood C, Van Gerven L, Spriet I, Devolder D, Debaveye Y, Depypere M, et al. Bacteriophage Therapy for Difficult-to-Treat Infections: The Implementation of a Multidisciplinary Phage Task Force (The PHAGEFORCE Study Protocol). Viruses. 2021; 13(8):1543. https://doi.org/10.3390/v13081543
Chicago/Turabian StyleOnsea, Jolien, Saartje Uyttebroek, Baixing Chen, Jeroen Wagemans, Cédric Lood, Laura Van Gerven, Isabel Spriet, David Devolder, Yves Debaveye, Melissa Depypere, and et al. 2021. "Bacteriophage Therapy for Difficult-to-Treat Infections: The Implementation of a Multidisciplinary Phage Task Force (The PHAGEFORCE Study Protocol)" Viruses 13, no. 8: 1543. https://doi.org/10.3390/v13081543