Involvement of Workers in Closed and Semiclosed Institutions in Outbreaks of Acute Gastroenteritis Due to Norovirus

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
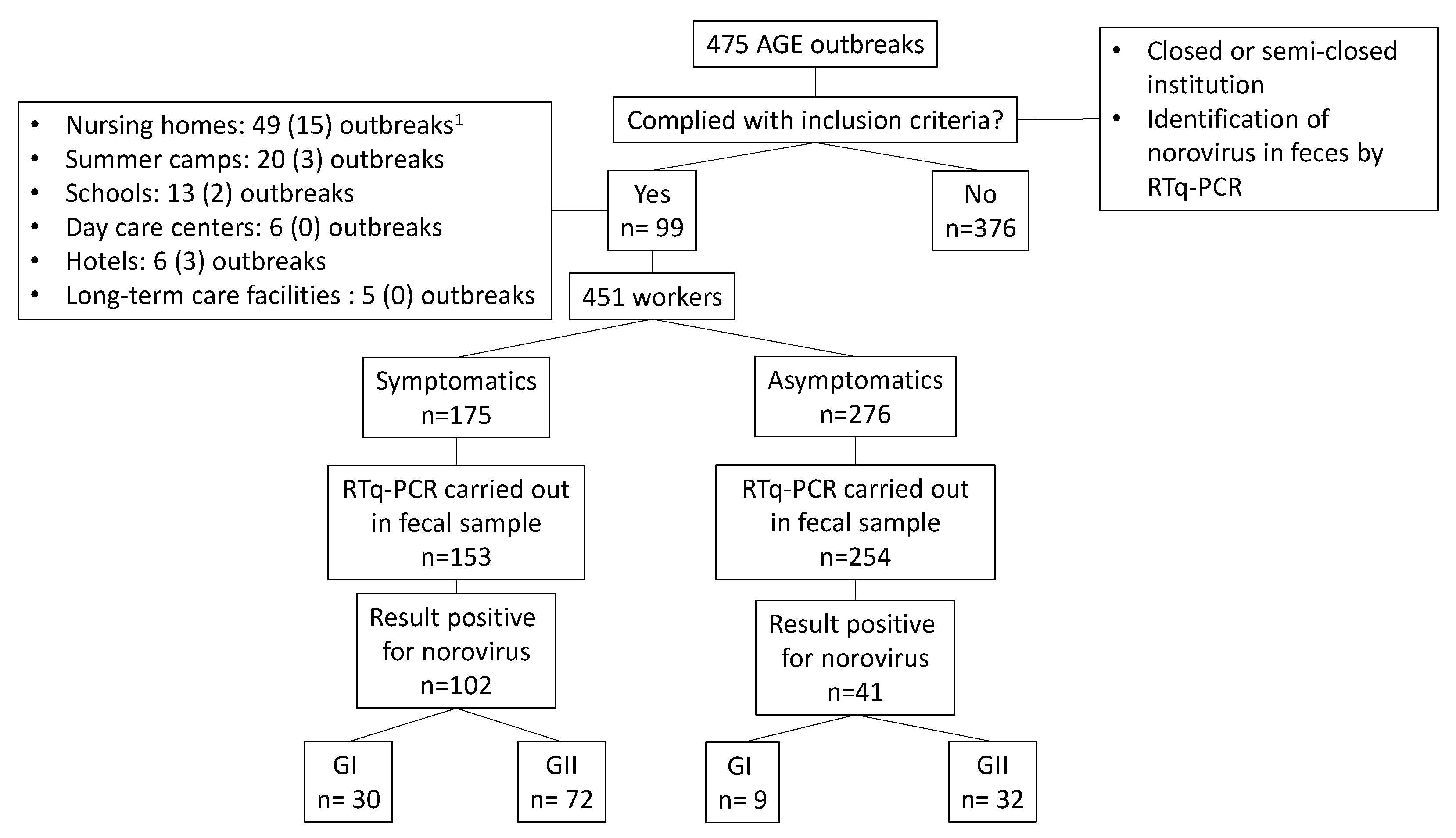
2.1. Type of Study, Study Period and Study Population
2.2. Outbreaks Included in the Study
2.3. Data Collection
2.4. Data Analysis and Management
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mead, P.S.; Slutsker, L.; Dietz, V.; McCaig, L.F.; Bresee, J.S.; Shapiro, C.; Griffin, P.M.; Tauxe, R.V. Food-related illness and death in the United States. Emerg. Infect. Dis. 1999, 5, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Bereciartu, A.; Bok, K.; Gómez, J. Identification of viral agents causing gastroenteritis among children in Buenos Aires, Argentina. J. Clin. Virol. 2002, 25, 197–203. [Google Scholar] [CrossRef]
- Marie-Cardine, A.; Gourlain, K.; Mouterde, O.; Castignolles, N.; Hellot, M.F.; Mallet, E.; Buffet-Janvresse, C. Epidemiology of acute viral gastroenteritis in children hospitalized in Rouen, France. Clin. Infect. Dis. 2002, 34, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Ramani, S.; Estes, M.K. Human noroviruses: Recent advances in a 50-year history. Curr. Opin. Infect. Dis. 2018, 31, 422–432. [Google Scholar] [CrossRef] [PubMed]
- International Committee on Taxonomy of Viruses. ICTV 9th Report. 2011. Available online: https://talk.ictvonline.org/ictv-reports/ictv_9th_report/positive-sense-rna-viruses-2011/w/posrna_viruses/253/caliciviridae (accessed on 24 November 2020).
- Godoy, P.; Alsedà, M.; Bartolomé, R.; Clavería, D.; Módol, I.; Bach, P.; Mirada, G.; Domínguez, À. Norovirus gastroenteritis outbreak transmitted by food and vomit in a high school. Epidemiol. Infect. 2016, 144, 1951–1958. [Google Scholar] [CrossRef] [Green Version]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E. Child Health Epidemiology Reference Group of the World Health Organization and UNICEF. Global causes of diarrheal disease mortality in children <5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar] [CrossRef] [Green Version]
- Keswick, B.H.; Satterwhite, T.K.; Johnson, P.C.; DuPont, H.L.; Secor, S.L.; Bitsura, J.A.; Gary, G.W.; Hoff, J.C. Inactivation of Norwalk virus in drinking water by chlorine. Appl. Environ. Microbiol. 1985, 50, 261–264. [Google Scholar] [CrossRef] [Green Version]
- Butot, S.; Putallaz, T.; Sánchez, G. Effects of sanitation, freezing and frozen storage on enteric viruses in berries and herbs. Int. J. Food Microbiol. 2008, 126, 30–35. [Google Scholar] [CrossRef]
- Cook, N.; Knight, A.; Richards, G.P. Persistence and elimination of human norovirus in food and on food contact surfaces: A critical review. J. Food Prot. 2016, 79, 1273–1294. [Google Scholar] [CrossRef]
- Wobus, E.; Green, K.Y. Caliciviridae: The viruses and their replication. In Fields Virology, Emerging Viruses, 7th ed.; Howley, P.M., Knipe, D.M., Whelan, S., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2020; Volume 1, pp. 129–169. [Google Scholar]
- Wu, H.M.; Fornek, M.; Schwab, K.J.; Chapin, A.R.; Gibson, K.; Schwab, E.; Spencer, C.; Henning, K. A norovirus outbreak at a long-term-care facility: The role of environmental surface contamination. Infect. Control Hosp. Epidemiol. 2005, 26, 802–810. [Google Scholar] [CrossRef]
- Ramani, S.; Estes, M.K.; Atmar, R.L. Correlates of protection against norovirus infection and disease—Where are we now, where do we go? PLoS Pathog. 2016, 12, e1005334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teunis, P.F.; Moe, C.L.; Liu, P.; Miller, S.E.; Lindesmith, L.; Baric, R.S.; Le Pendu, J.; Calderon, R.L. Norwalk virus: How infectious is it? J. Med. Virol. 2008, 80, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.E.; Teunis, P.F.; Moe, C.L. Two human challenge studies confirm high infectivity of Norwalk virus. J. Infect. Dis. 2015, 211, 166–167. [Google Scholar] [CrossRef] [Green Version]
- Guix, S.; Fuentes, C.; Pintó, R.M.; Blanco, A.; Sabrià, A.; Anfruns-Estrada, E.; Garrido, V.R.; Alonso, M.; Bartolomé, R.; Cornejo, T.; et al. Infectivity of norovirus GI and GII from bottled mineral water during a waterborne outbreak, Spain. Emerg. Infect. Dis. 2020, 26, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Opekun, A.R.; Gilger, M.A.; Estes, M.K.; Crawford, S.E.; Neill, F.H.; Ramani, S.; Hill, H.; Ferreira, J.; Graham, D.Y. Determination of the 50% human infectious dose for Norwalk virus. J. Infect. Dis. 2014, 209, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Miura, F.; Matsuyama, R.; Nishiura, H. Estimating the asymptomatic ratio of norovirus infection during foodborne outbreaks with laboratory testing in Japan. J. Epidemiol. 2018, 28, 382–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez, A.; Torner, N.; Broner, S.; Bartolomé, R.; Guix, S.; De Simón, M.; Godoy, P.; Moreno, A.; Company, M.; Balanyà, P.J.; et al. Norovirus: A growing cause of gastroenteritis in Catalonia (Spain)? J. Food Prot. 2013, 76, 1810–1816. [Google Scholar] [CrossRef]
- Barberà, E.; Bartolomé, R.; Bosch, A.; Cardeñosa, N.; Cabedo, L.; Domínguez, A.; Ferrer, M.D.; Godoy, P.; Martínez, A.; Masó, M.; et al. Guia per a la Prevenció i Control de les Toxiinfeccions Alimentàries, 2nd ed.; Generalitat de Catalunya: Barcelona, Spain, 2006; pp. 175–176. Available online: https://scientiasalut.gencat.cat/bitstream/handle/11351/1930/guia_prevencio_control_toxiinfeccions_alimentaries_2006.pdf?sequence=1&isAllowed=y (accessed on 26 November 2020).
- Wu, Q.-S.; Xuan, Z.-L.; Liu, J.-Y.; Zhao, X.-T.; Chen, Y.-F.; Wang, C.-X.; Shen, X.-T.; Wang, Y.-X.; Wang, L.; Hu, Y. Norovirus shedding among symptomatic and asymptomatic employees in outbreak settings in Shanghai, China. BMC Infect. Dis. 2019, 19, 592. [Google Scholar] [CrossRef]
- Sabrià, A.; Pintó, R.M.; Bosch, A.; Bartolomé, R.; Cornejo, T.; Torner, N.; Martínez, A.; De Simón, M.; Domínguez, À.; Guix, S. Norovirus shedding among food and healthcare workers exposed to the virus in outbreak settings. J. Clin. Virol. 2016, 82, 119–125. [Google Scholar] [CrossRef]
- Generalitat de Catalunya. Decret 203/2015 de 15 de setembre, pel qual es crea la Xarxa de Vigilància Epidemiològica i es regulen els sistemes de notificació de malalties de declaració obligatòria i brots epidèmics. Diari Oficial de la Generalitat de Catalunya, Núm 6958, 1–19. Available online: https://portaldogc.gencat.cat/utilsEADOP/PDF/6958/1444533.pdf (accessed on 26 November 2020).
- Institut Estadistic de Catalunya. Population on 1 January. By Sex. Available online: https://www.idescat.cat/indicadors/?id=anuals&n=10328&col=1&lang=en (accessed on 18 October 2020).
- Kageyama, T.; Kojima, S.; Shinohara, M.; Uchida, K.; Fukushi, S.; Hoshino, F.B.; Takeda, N.; Katayama, K. Broadly reactive and highly sensitive assay for Norwalk-like viruses based on real-time quantitative reverse transcription-PCR. J. Clin. Microbiol. 2003, 41, 1548–1557. [Google Scholar] [CrossRef] [Green Version]
- Farkas, T.; Singh, A.; Le Guyader, F.S.; La Rosa, G.; Saif, L.; McNeal, M. Multiplex real-time RT-PCR for the simultaneous detection and quantification of GI, GII and GIV noroviruses. J. Virol. Methods 2015, 223, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Phillips, G.; Lopman, B.; Tam, C.C.; Iturriza-Gomara, M.; Brown, D.; Gray, J. Diagnosing norovirus-associated infectious intestinal disease using viral load. BMC Infect. Dis. 2009, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Qi, R.; Huang, Y.T.; Liu, J.W.; Sun, Y.; Sun, X.F.; Han, H.J.; Qin, X.R.; Zhao, M.; Wang, L.J.; Li, W.; et al. Global prevalence of asymptomatic norovirus infection: A meta-analysis. EClinicalMedicine 2018, 2, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.H.; Kim, N.Y.; Lee, E.J.; Jeon, I.S. Norovirus infections in asymptomatic food handlers in elementary schools without norovirus outbreaks in some regions of Incheon, Korea. J. Korean Med. Sci. 2011, 26, 734–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okabayashi, T.; Yokota, S.; Ohkoshi, Y.; Ohuchi, H.; Yoshida, Y.; Kikuchi, M.; Yano, K.; Fujii, N. Occurrence of norovirus infections unrelated to norovirus outbreaks in an asymptomatic food handler population. J. Clin. Microbiol. 2008, 46, 1985–1988. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Huang, Q.; Qin, L.; Zhong, X.; Li, H.; Chen, R.; Wan, Z.; Lin, H.; Liang, J.; Li, J.; et al. Epidemiological characteristics of asymptomatic Norovirus infection in a population from oyster (Ostrea rivularis Gould) farms in southern China. Epidemiol. Infect. 2018, 146, 1955–1964. [Google Scholar] [CrossRef] [Green Version]
- Luo, L.; Gu, Y.; Wang, X.; Zhang, Y.; Zhan, L.; Liu, J.; Yan, H.; Liu, Y.; Zhen, S.; Chen, X.; et al. Epidemiological and clinical differences between sexes and pathogens in a three-year surveillance of acute infectious gastroenteritis in Shanghai. Sci. Rep. 2019, 9, 9993. [Google Scholar] [CrossRef] [Green Version]
- Koo, H.L.; Ajami, N.; Atmar, R.L.; DuPont, H.L. Noroviruses: The principal cause of foodborne disease worldwide. Discov. Med. 2010, 10, 61–70. [Google Scholar]
- Wikswo, M.E.; Hall, A.J. Outbreaks of acute gastroenteritis transmitted by person-to-person contact—United States, 2009–2010. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2012, 61, 1–12. [Google Scholar]
- Godoy, P.; Artigues, A.; Bartolomé, R.; Domínguez, A.; Plasència, A. Norovirus gastroenteritis outbreak by person-to-person transmission in a nursing home. Med. Clin. 2006, 127, 538–541. [Google Scholar] [CrossRef]
- Park, G.W.; Williamson, K.J.; DeBess, E.; Cieslak, P.R.; Gregoricus, N.; De Nardo, E.; Fricker, C.; Costantini, V.; Vinjé, J. High hand contamination rates during norovirus outbreaks in long-term care facilities. Infect. Control Hosp. Epidemiol. 2018, 39, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Qi, R.; Ye, C.; Chen, C.; Yao, P.; Hu, F.; Lin, Q. Norovirus prevention and the prevalence of asymptomatic norovirus infection in kindergartens and primary schools in Changzhou, China: Status of the knowledge, attitudes, behaviors, and requirements. Am. J. Infect. Control 2015, 43, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Marsh, Z.; Shah, M.P.; Wikswo, M.E.; Barclay, L.; Kisselburgh, H.; Kambhampati, A.; Cannon, J.L.; Parashar, U.D.; Vinjé, J.; Hall, A.J. Epidemiology of foodborne norovirus outbreaks—United States, 2009–2015. Food Saf. 2018, 6, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teunis, P.F.M.; Sukhrie, F.H.A.; Vennema, H.; Bogerman, J.; Beersma, M.F.C.; Koopmans, M.P.G. Shedding of norovirus in symptomatic and asymptomatic infections. Epidemiol. Infect. 2015, 143, 1710–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabue, J.P.; Meader, E.; Hunter, P.R.; Potgieter, N. Norovirus prevalence and estimated viral load in symptomatic and asymptomatic children from rural communities of Vhembe district, South Africa. J. Clin. Virol. 2016, 84, 12–18. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Males | Females | ||||||
|---|---|---|---|---|---|---|---|
| Age (Years) | Symptomatic | Exposed | Attack Rate | Symptomatic | Exposed | Attack Rate | p-Value |
| 17–25 | 10 | 17 | 58.82% | 29 | 45 | 64.44% | 0.69 |
| 26–35 | 11 | 38 | 28.95% | 28 | 58 | 48.28% | 0.06 |
| 36–45 | 10 | 27 | 37.04% | 20 | 55 | 36.36% | 0.95 |
| 46–55 | 5 | 24 | 20.83% | 31 | 83 | 37.35% | 0.13 |
| 56–65 | 4 | 14 | 28.57% | 14 | 37 | 37.84% | 0.54 |
| NA | 1 | 8 | 12.50% | 12 | 45 | 26.67% | 0.35 |
| Total | 41 | 128 | 32.03% | 134 | 323 | 41.49% | 0.06 |
| Type of Institution (Total Affected) 1 | Symptomatic | Exposed | Attack Rate | RR (95% CI) |
|---|---|---|---|---|
| Summer camp | ||||
| Person-to-person (74) | 1 | 11 | 9.09% | 0.17 (0.02 to 1.30) |
| Common vehicle (105) | 12 | 32 | 37.5% | 1 |
| Mixed transmission (4) | 0 | 8 | 0% | NC |
| Total (183) | 13 | 51 | 25.49% | |
| School | ||||
| Person-to-person (144) | 15 | 56 | 26.79% | 1.93 (1.07 to 3.49) |
| Common vehicle (24) | 11 | 69 | 15.94% | 1 |
| Total (168) | 26 | 125 | 20.80% | |
| Daycare center | ||||
| Person-to-person (69) | 6 | 14 | 42.86% | NC |
| Common vehicle (0) | 0 | 0 | 0% | |
| Total (69) | 6 | 14 | 42.86% | |
| Hotel | ||||
| Person-to-person (14) | 9 | 40 | 22.5% | 0.93 (0.44 to 1.95) |
| Common vehicle (48) | 5 | 21 | 23.81% | 1 |
| Total (62) | 14 | 61 | 22.95% | |
| Nursing home | ||||
| Person-to-person (400) | 77 | 133 | 57.89% | 1.03 (0.78 to 1.38) |
| Common vehicle (93) | 28 | 50 | 56.00% | 1 |
| Total (493) | 105 | 183 | 57.37% | |
| Long-term care facility | ||||
| Person-to-person (55) | 11 | 17 | 64.70% | NC |
| Common vehicle (0) | 0 | 0 | 0% | |
| Total (55) | 11 | 17 | 64.70% | |
| Total | ||||
| Person-to-person (756) | 119 | 271 | 43.91% | 1.35 (1.05 to 1.74) |
| Common vehicle (270) | 56 | 172 | 32.56% | 1 |
| Mixed transmission (4) | 0 | 8 | 0% | NC |
| Total (1030) | 175 | 451 | 38.80% |
| Type of Institution | Symptomatic | Exposed | Attack Rate | RR (95% CI) |
|---|---|---|---|---|
| Summer camp | 0.30 (0. 19 to 0. 48) 1 | |||
| Workers | 13 | 51 | 25.49 | |
| Users | 170 | 201 | 84.58 | |
| Total | 183 | 252 | 72.62 | |
| Schools | 0.25 (0.17 to 0.35) 1 | |||
| Workers | 26 | 125 | 20.80 | |
| Users | 141 | 167 | 84.43 | |
| Total | 167 | 292 | 57.19 | |
| Daycare center | 0.53 (0.28 to 0.97) 1 | |||
| Workers | 6 | 14 | 42.86 | |
| Users | 62 | 76 | 81.58 | |
| Total | 68 | 90 | 75.56 | |
| Hotel | 0.26 (0.16 to 0.42) 1 | |||
| Workers | 14 | 61 | 22.95 | |
| Users | 48 | 55 | 87.27 | |
| Total | 62 | 116 | 34.83 | |
| Nursing home | 0.69 (0.61 to 0.79) 1 | |||
| Workers | 105 | 183 | 57.38 | |
| Users | 388 | 468 | 82.91 | |
| Total | 493 | 651 | 75. 73 | |
| Long-term care facility | 0.69 (0.48 to 0.99) 1 | |||
| Workers | 11 | 17 | 64.71 | |
| Users | 45 | 48 | 93.75 | |
| Total | 56 | 65 | 86.15 | |
| Total | 0.46 (0.41 to 0.52) 1 | |||
| Workers | 175 | 451 | 38.80 | |
| Users | 854 | 1015 | 84.14 | |
| Total | 1029 | 1466 | 70.19 |
| Type of Occupation | Attack Rate | RR 1 (95% CI) |
|---|---|---|
| Cook | 9.8% | 0.26 (0.12.0.56) |
| Kitchen assistant | 15.0% | 0.36 (0.23.0.59) |
| Waiter | 37.5% | 1.13 (0.45. 2.79) |
| Dining monitor | 27.8% | 0.79 (0.54. 1.14) |
| Caregiver or healthcare worker | 71.6% | 3.18 (2.32. 4.35) |
| Global attack rate | 38.8% |
| Genogroup | Symptomatic | N | Mean Cq | SD | p-Value |
|---|---|---|---|---|---|
| GI | Yes | 30 | 30.01 | 5.51 | 0.002 |
| No | 9 | 36.97 | 5.13 | ||
| GII | Yes | 72 | 27.01 | 5.84 | 0.07 |
| No | 32 | 29.19 | 5.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrón, I.; Barrabeig, I.; Alseda, M.; Cornejo-Sánchez, T.; Guix, S.; Jané, M.; Izquierdo, C.; Rius, C.; Domínguez, À.; the Working Group for the Study of Acute Gastroenteritis Outbreaks in Catalonia. Involvement of Workers in Closed and Semiclosed Institutions in Outbreaks of Acute Gastroenteritis Due to Norovirus. Viruses 2020, 12, 1392. https://doi.org/10.3390/v12121392
Parrón I, Barrabeig I, Alseda M, Cornejo-Sánchez T, Guix S, Jané M, Izquierdo C, Rius C, Domínguez À, the Working Group for the Study of Acute Gastroenteritis Outbreaks in Catalonia. Involvement of Workers in Closed and Semiclosed Institutions in Outbreaks of Acute Gastroenteritis Due to Norovirus. Viruses. 2020; 12(12):1392. https://doi.org/10.3390/v12121392
Chicago/Turabian StyleParrón, Ignacio, Irene Barrabeig, Miquel Alseda, Thais Cornejo-Sánchez, Susana Guix, Mireia Jané, Conchita Izquierdo, Cristina Rius, Àngela Domínguez, and the Working Group for the Study of Acute Gastroenteritis Outbreaks in Catalonia. 2020. "Involvement of Workers in Closed and Semiclosed Institutions in Outbreaks of Acute Gastroenteritis Due to Norovirus" Viruses 12, no. 12: 1392. https://doi.org/10.3390/v12121392