
Cost-Effectiveness Analysis of COVID-19 Vaccine Booster Dose in the Thai Setting during the Period of Omicron Variant Predominance

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
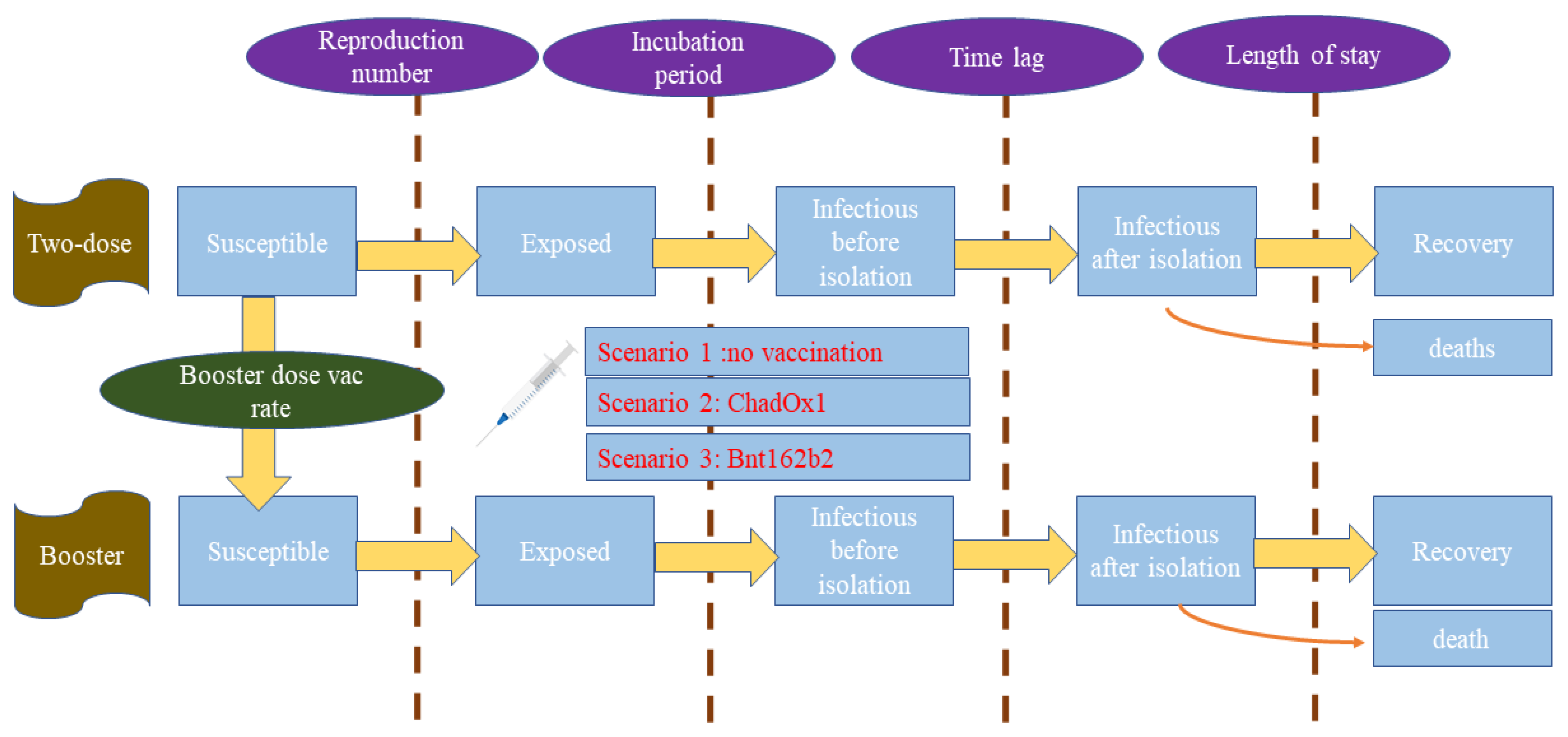
2.1. Study Design and Model Framework
2.2. Model Assumptions, Parameters, Formula, and Outcomes
2.3. Ethics Consideration
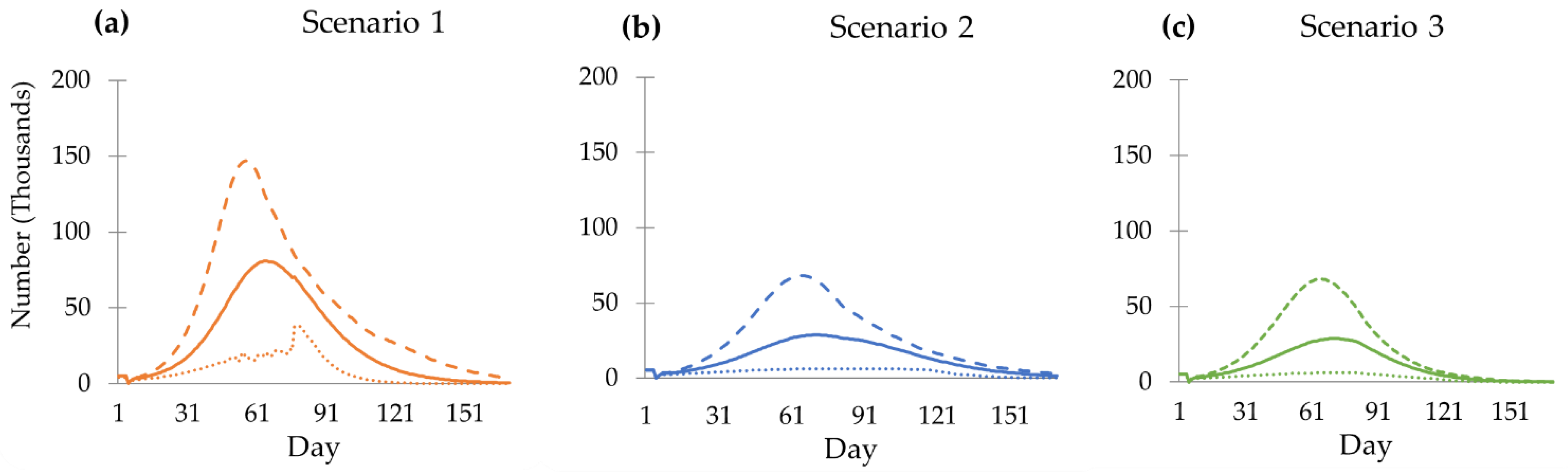
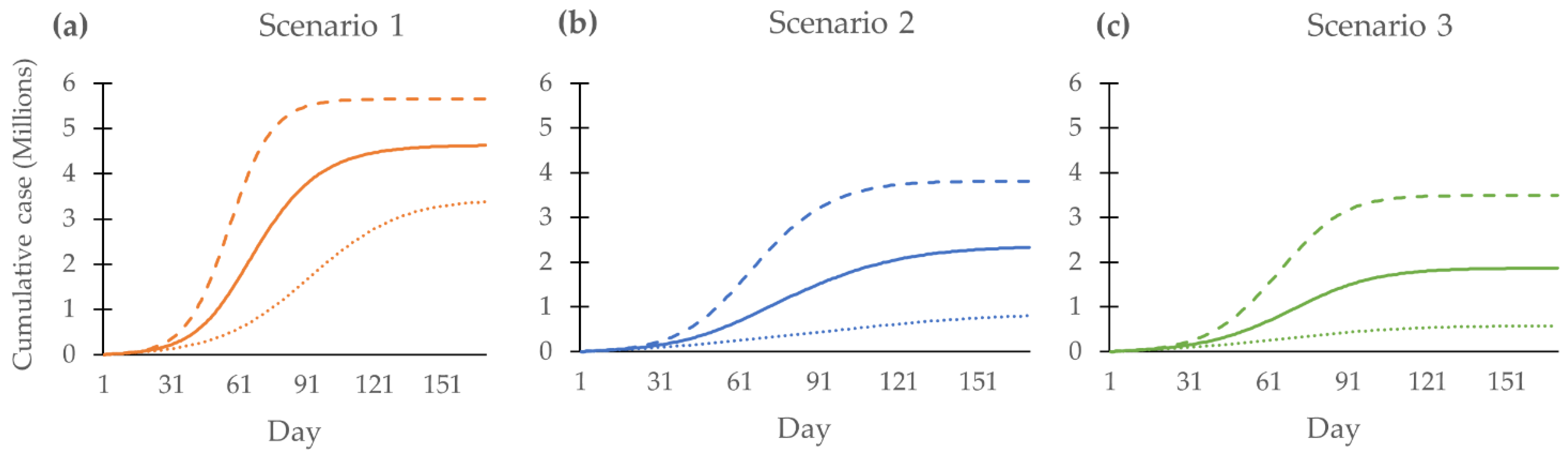
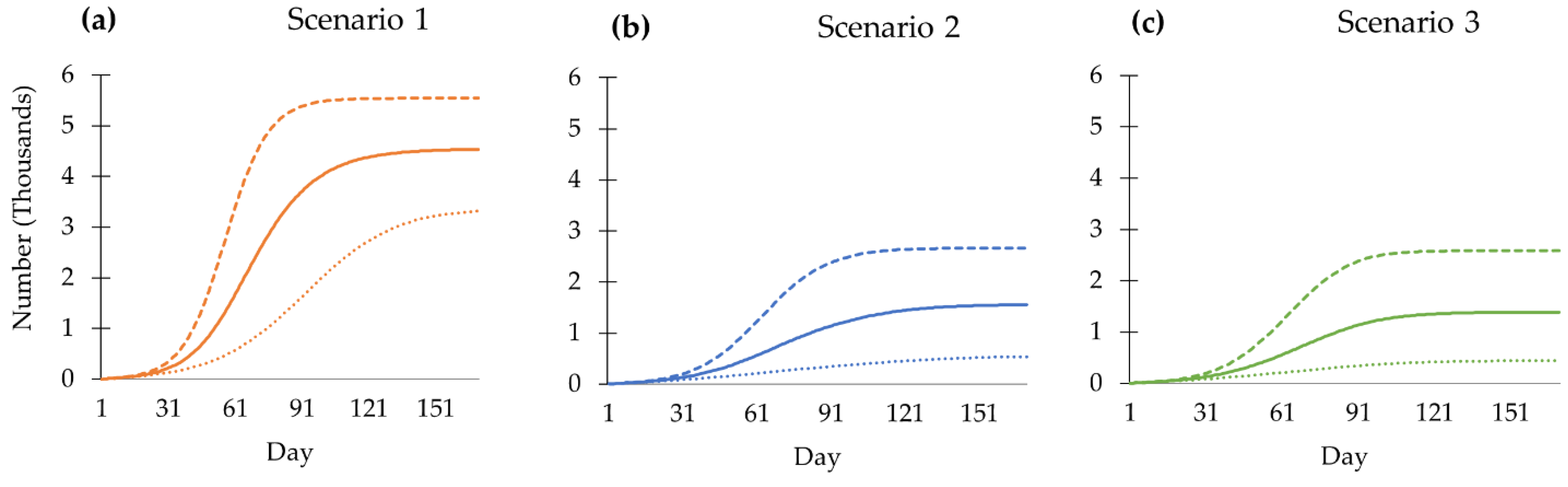
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19); StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Galloway, S.E.; Paul, P.; MacCannell, D.R.; Johansson, M.A.; Brooks, J.T.; MacNeil, A.; Slayton, R.B.; Tong, S.; Silk, B.J.; Armstrong, G.L.; et al. Emergence of SARS-CoV-2 B.1.1.7 Lineage—United States, December 29, 2020-January 12, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.J.; Guo, H.; Luo, G. Omicron variant (B.1.1.529) of SARS-CoV-2, a global urgent public health alert! J. Med. Virol. 2022, 94, 1255–1256. [Google Scholar] [CrossRef] [PubMed]
- Thailand, D.o.M.S.M.o.P.H. Thailand Corona Virus Disease (COVID-19): Thailand Situation; Department of Disease Control: Nonthaburi, Thailand, 2022. [Google Scholar]
- Thailand, F.a.D.A. Thai FDA Approved six COVID-19 Vaccines. Available online: https://oryor.com/media/newsUpdate/media_news/2087 (accessed on 22 July 2022).
- Bangkokpost. Covid Vaccination Priorities Announced. Available online: https://www.bangkokpost.com/thailand/general/2073071/covid-vaccination-priorities-announced (accessed on 20 May 2022).
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; Zubizarreta, J.R.; González, C.; Pizarro, A.; Acevedo, J.; Leo, K.; Paredes, F.; Bralic, T.; Vergara, V.; et al. Effectiveness of homologous and heterologous booster doses for an inactivated SARS-CoV-2 vaccine: A large-scale prospective cohort study. Lancet Glob. Health 2022, 10, e798–e806. [Google Scholar] [CrossRef]
- Suphanchaimat, R.; Nittayasoot, N.; Jiraphongsa, C.; Thammawijaya, P.; Bumrungwong, P.; Tulyathan, A.; Cheewaruangroj, N.; Pittayawonganon, C.; Tharmaphornpilas, P. Real-World Effectiveness of Mix-and-Match Vaccine Regimens against SARS-CoV-2 Delta Variant in Thailand: A Nationwide Test-Negative Matched Case-Control Study. Vaccines 2022, 10, 1080. [Google Scholar] [CrossRef]
- Whittaker, C.; Walker, P.G.T.; Alhaffar, M.; Hamlet, A.; Djaafara, B.A.; Ghani, A.; Ferguson, N.; Dahab, M.; Checchi, F.; Watson, O.J. Under-reporting of deaths limits our understanding of true burden of covid-19. BMJ Clin. Res. Ed. 2021, 375, n2239. [Google Scholar] [CrossRef]
- Lau, H.; Khosrawipour, T.; Kocbach, P.; Ichii, H.; Bania, J.; Khosrawipour, V. Evaluating the massive underreporting and undertesting of COVID-19 cases in multiple global epicenters. Pulmonology 2021, 27, 110–115. [Google Scholar] [CrossRef]
- BBC Thai. MOPH Admits Under-Reporting of COVID-19 Cases with Stable “Severity” of Situation in Bangkok. Available online: https://www.bbc.com/thai/thailand-58009764 (accessed on 12 January 2022).
- Nittayasoot, N.; Suphanchaimat, R.; Thammawijaya, P.; Jiraphongsa, C.; Siraprapasiri, T.; Ploddi, K.; Pittayawonganon, C.; Mahasirimongkol, S.; Tharmaphornpilas, P. Real-World Effectiveness of COVID-19 Vaccines against Severe Outcomes during the Period of Omicron Predominance in Thailand: A Test-Negative Nationwide Case-Control Study. Vaccines 2022, 10, 2123. [Google Scholar] [CrossRef]
- Choppradit, C.; Likittientong, T.; Sonthong, V. Adverse events following immunization (AEFIs) of COVID-19 vaccine in Samutsakhon Hospital. Hua Hin Med. J. 2023, 2, 52–70. [Google Scholar]
- 2021. Available online: http://statbbi.nso.go.th/staticreport/page/sector/th/01.aspx (accessed on 22 July 2022).
- Hart, W.S.; Miller, E.; Andrews, N.J.; Waight, P.; Maini, P.K.; Funk, S.; Thompson, R.N. Generation time of the alpha and delta SARS-CoV-2 variants: An epidemiological analysis. Lancet Infect. Dis. 2022, 22, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Helmsdal, G.; Hansen, O.K.; Møller, L.F.; Christiansen, D.H.; Petersen, M.S.; Kristiansen, M.F. Omicron outbreak at a private gathering in the Faroe Islands, infecting 21 of 33 triple-vaccinated healthcare workers. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Meeyai, A.; Praditsitthikorn, N.; Kotirum, S.; Kulpeng, W.; Putthasri, W.; Cooper, B.S.; Teerawattananon, Y. Seasonal influenza vaccination for children in Thailand: A cost-effectiveness analysis. PLoS Med. 2015, 12, e1001829. [Google Scholar] [CrossRef] [PubMed]
- Kirsebom, F.; Andrews, N.; Sachdeva, R.; Stowe, J.; Ramsay, M.; Bernal, J.L. Effectiveness of ChAdOx1-S COVID-19 Booster Vaccination against the Omicron and Delta variants in England. medRxiv 2022. preprint. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- El-Shabasy, R.M.; Nayel, M.A.; Taher, M.M.; Abdelmonem, R.; Shoueir, K.R.; Kenawy, E.R. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar] [CrossRef]
- Pheerapanyawaranun, C.; Wang, Y.; Kittibovorndit, N.; Pimsarn, N.; Sirison, K.; Teerawattananon, Y.; Isaranuwatchai, W. COVID-19 Vaccine Hesitancy Among Health Care Workers in Thailand: The Comparative Results of Two Cross-Sectional Online Surveys Before and After Vaccine Availability. Front. Public Health 2022, 10, 834545. [Google Scholar] [CrossRef]
- Thanapluetiwong, S.; Chansirikarnjana, S.; Sriwannopas, O.; Assavapokee, T.; Ittasakul, P. Factors associated with COVID-19 Vaccine Hesitancy in Thai Seniors. Patient Prefer. Adherence 2021, 15, 2389–2403. [Google Scholar] [CrossRef]
- Li, R.; Liu, H.; Fairley, C.K.; Zou, Z.; Xie, L.; Li, X.; Shen, M.; Li, Y.; Zhang, L. Cost-effectiveness analysis of BNT162b2 COVID-19 booster vaccination in the United States. Int. J. Infect.Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 119, 87–94. [Google Scholar] [CrossRef]
- Fu, Y.; Zhao, J.; Wei, X.; Han, P.; Yang, L.; Ren, T.; Zhan, S.; Li, L. Cost-Effectiveness of COVID-19 Sequential Vaccination Strategies in Inactivated Vaccinated Individuals in China. Vaccines 2022, 10, 1712. [Google Scholar] [CrossRef]
- Mungmunpuntipantip, R.; Wiwanitkit, V. Underreporting of COVID-19 deaths. J. Formos. Med. Assoc. 2021, 120, 1930. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparison | Incremental Cost (a) | Incremental Outcome (b) | Interpretation |
|---|---|---|---|
| Scenario 1 vs. scenario 2 | Grand cost 2 − grand cost 1 | Cumulative cases 1 − cumulative cases 2 | Incremental grand cost per case averted |
| Scenario 1 vs. scenario 2 | Grand cost 2 − grand cost 1 | Cumulative death 1 − cumulative death 2 | Incremental grand cost per death averted |
| Scenario 1 vs. scenario 2 | Vaccine cost 2 − vaccine cost 1 | Cumulative cases 1 − cumulative cases 2 | Incremental vaccination cost per case averted |
| Scenario 1 vs. scenario 2 | Vaccine cost 2 − vaccine cost 1 | Cumulative death 1 − cumulative death 2 | Incremental vaccination cost per death averted |
| Scenario 1 vs. scenario 3 | Grand cost 3 − grand cost 1 | Cumulative cases 1 − cumulative cases 3 | Incremental grand cost per case averted |
| Scenario 1 vs. scenario 3 | Grand cost 3 − grand cost 1 | Cumulative death 1 − cumulative death 3 | Incremental grand cost per death averted |
| Scenario 1 vs. scenario 3 | Vaccine cost 3 − vaccine cost 1 | Cumulative cases 1 − cumulative cases 3 | Incremental vaccination cost per case averted |
| Scenario 1 vs. scenario 3 | Vaccine cost 3 − vaccine cost 1 | Cumulative death 1 − cumulative death 3 | Incremental vaccination cost per death averted |
| Parameters | Unit | Value | Reference (Note) |
|---|---|---|---|
| Reproduction number | Unitless | 1.5 | Model calibration |
| Population | Persons | 50 × 106 | 70% of the total Thai population based on the National Statistical Office of Thailand [16] |
| Mean infectious duration | Days | 4.6 | Hart et al. (gamma distribution with scale parameter of 0.03 and shape parameter of 165.9) [17] |
| Mean incubation period | Days | 3.5 | Helmsdal et al. (gamma distribution with scale parameter of 0.01 and shape parameter of 302.7) [18] |
| Time lag from being infected to isolation | Days | 4 | Model calibration |
| Initial number of infectees | Persons | 125,000 | Assume 0.25% of the interested population with model calibration |
| Initial proportion of third dose vaccinees | Unitless | 20% | Division of Communicable Diseases, Department of Disease Control |
| Booster-dose vaccination rate | Persons/day | 171,300 | Division of Communicable Diseases, Department of Disease Control |
| Vaccine effectiveness against any infection of viral vector booster dose (two-dose vaccinees as reference) | Unitless | 34% | Vaccine Effectiveness Intelligence Unit, Division of Epidemiology, Department of Disease Control |
| Vaccine effectiveness against any infection of mRNA booster dose (two-dose vaccinees as reference) | Unitless | 55% | Vaccine Effectiveness Intelligence Unit, Division of Epidemiology, Department of Disease Control |
| Vaccine effectiveness against severe infection of viral vector booster dose (two-dose vaccinees as reference) | Unitless | 88% | Vaccine Effectiveness Intelligence Unit, Division of Epidemiology, Department of Disease Control |
| Vaccine effectiveness against severe infection of mRNA booster dose (two-dose vaccinees as reference) | Unitless | 78% | Vaccine Effectiveness Intelligence Unit, Division of Epidemiology, Department of Disease Control |
| Proportion of asymptomatic and mildly symptomatic infectees amongst all infectees | Unitless | 99.7% | Internal database of the Department of Disease Control and model calibration (accounted for underreporting factor) |
| Proportion of non-intubated pneumonic infectees amongst all infectees | Unitless | 0.25% | Internal database of the Department of Disease Control and model calibration (accounted for underreporting factor) |
| Proportion of intubated pneumonic infectees amongst all infectees | Unitless | 0.01% | Internal database of the Department of Disease Control and model calibration (accounted for underreporting factor) |
| Proportion of deaths amongst all infectees | Unitless | 0.02% | Internal database of the Department of Disease Control and model calibration (accounted for underreporting factor) |
| Recovery time for asymptomatic or mildly symptomatic patients | Days | 10 | Internal database of the Department of Disease Control and model calibration (assume same as clinical profile of the patients during the Delta wave) |
| Recovery time for pneumonic non-intubated cases | Days | 14 | Internal database of the Department of Disease Control and model calibration (assume same as clinical profile of the patients during the Delta wave) |
| Recovery time for asymptomatic or mildly symptomatic patients | Days | 21 | Internal database of the Department of Disease Control and model calibration (assume same as clinical profile of the patients during the Delta wave) |
| Recovery time for non-intubated pneumonic patients | Days | 21 | Internal database of the Department of Disease Control and model calibration (assume same as clinical profile of the patients during the Delta wave) |
| Administration cost of vaccination | Baht/ dose | 234 | Meeyai A et al. (3% discount rate adjusted per year) [19] |
| Viral vector vaccine | Baht/dose | 308 | Internal database, Division of Communicable Diseases, Department of Disease Control |
| mRNA vaccine | Baht/dose | 488 | Internal database, Division of Communicable Diseases, Department of Disease Control |
| Change of Status | Formula | Note |
|---|---|---|
| From susceptible to exposed | −β × (1−VE) × S × I1/P | β = reproduction number/infectious duration, VE = effectiveness of vaccine against any infection, S = susceptible population, I1 = non-isolated infectees, P = total population |
| From susceptible to non-isolated infectious | −αE | α = 1/incubation period, E = exposed population |
| From non-isolated infectious to isolated infectious | −δI1 | δ = 1/time lag from non-isolation to isolation, I1 = non-isolated infectious population |
| From isolated infectious to recovered | −ζI2 | ζ = 1/length of stay; I2 = isolated infectious population (Varying by severity profile) |
| ICER of Grand Cost (Thousands) per Case Averted (by Day 170) | ICER of Grand Cost (Millions) per Death Averted (by Day 170) | |
|---|---|---|
| Scenario 1 vs. scenario 2 | −17.0 (95% CI, −17.7 to −16.4) | −13.1 (95% CI, −16.3 to −10.6) |
| Scenario 1 vs. scenario 3 | −16.1 (95% CI, −16.8 to −15.3) | −14.2 (95% CI, −15.9 to −11.2) |
| ICER of Vaccine Cost (Thousands) per Case Averted (by Day 170) | ICER of Vaccine Cost (Millions) per Death Averted (by Day 170) | |
|---|---|---|
| Scenario 1 vs. scenario 2 | 7.5 (95% CI, 6.8 to 8.5) | 5.1 (95% CI, 4.7 to 5.6) |
| Scenario 1 vs. scenario 3 | 6.7 (95% CI, 5.9 to 7.4) | 6.5 (95% CI, 6.2 to 7.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirison, K.; Nittayasoot, N.; Techasuwanna, R.; Cetthakrikul, N.; Suphanchaimat, R. Cost-Effectiveness Analysis of COVID-19 Vaccine Booster Dose in the Thai Setting during the Period of Omicron Variant Predominance. Trop. Med. Infect. Dis. 2023, 8, 91. https://doi.org/10.3390/tropicalmed8020091
Sirison K, Nittayasoot N, Techasuwanna R, Cetthakrikul N, Suphanchaimat R. Cost-Effectiveness Analysis of COVID-19 Vaccine Booster Dose in the Thai Setting during the Period of Omicron Variant Predominance. Tropical Medicine and Infectious Disease. 2023; 8(2):91. https://doi.org/10.3390/tropicalmed8020091
Chicago/Turabian StyleSirison, Kanchanok, Natthaprang Nittayasoot, Ranida Techasuwanna, Nisachol Cetthakrikul, and Rapeepong Suphanchaimat. 2023. "Cost-Effectiveness Analysis of COVID-19 Vaccine Booster Dose in the Thai Setting during the Period of Omicron Variant Predominance" Tropical Medicine and Infectious Disease 8, no. 2: 91. https://doi.org/10.3390/tropicalmed8020091