
Factors Associated with Treatment Outcome in Patients with Nontuberculous Mycobacterial Pulmonary Disease: A Large Population-Based Retrospective Cohort Study in Shanghai


Abstract
:1. Introduction
2. Materials and Methods
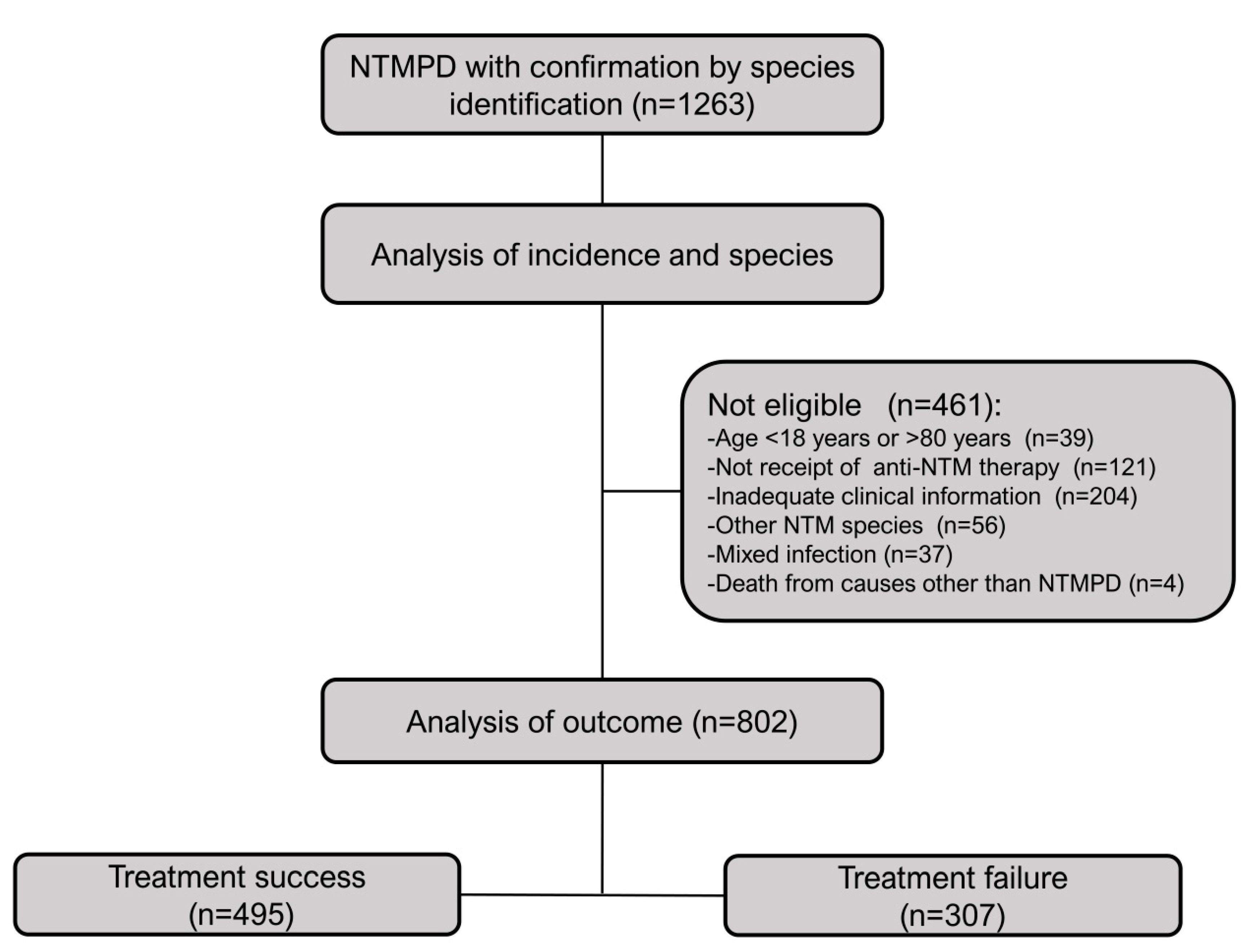
2.1. Patient Selection
2.2. Culture Methods, Species Identification, and Drug Susceptibility Testing
2.3. Study Design and Follow-Up
2.4. Treatment Outcome and Prognosis
2.5. Statistical Analysis
3. Results
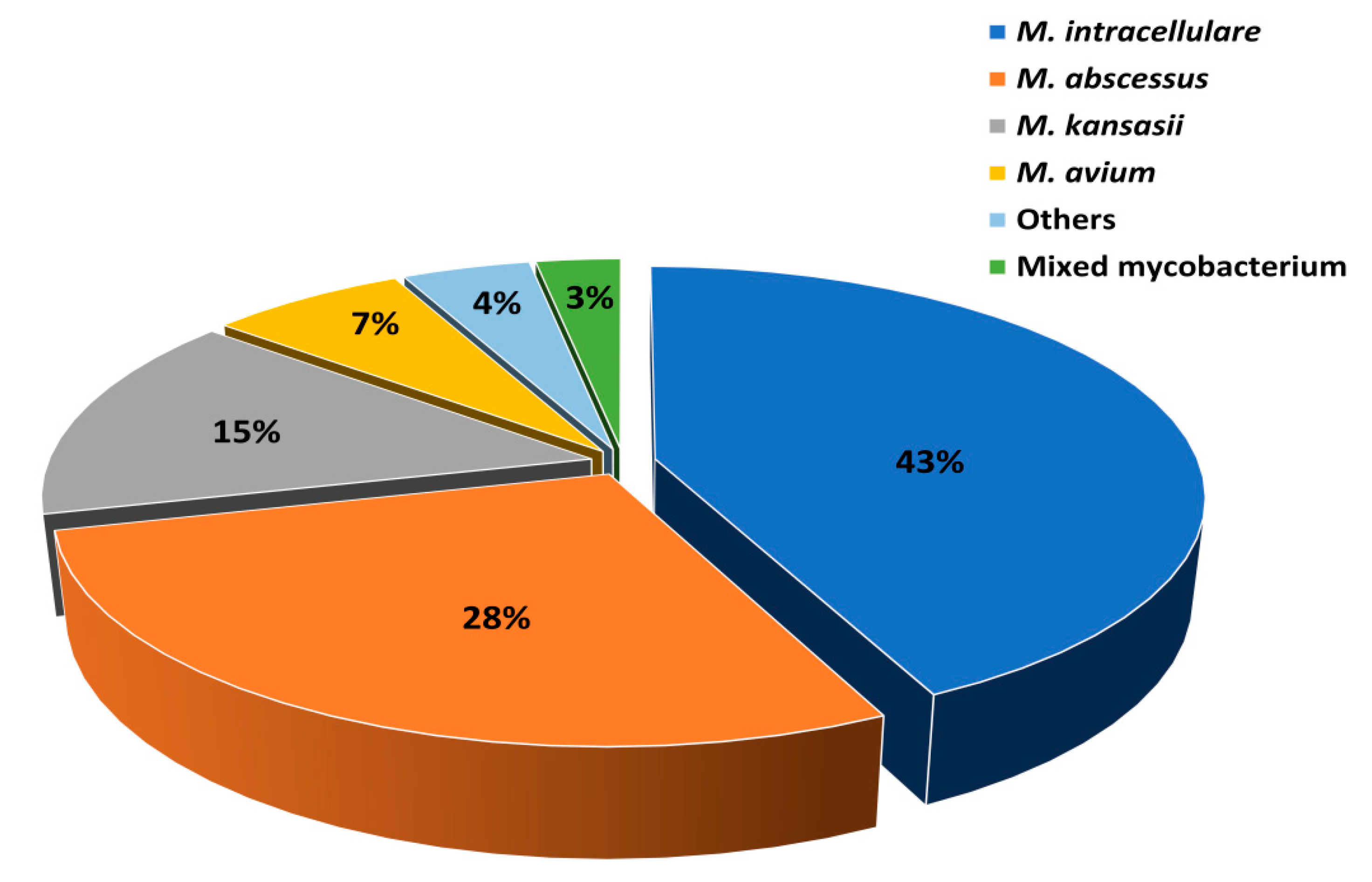
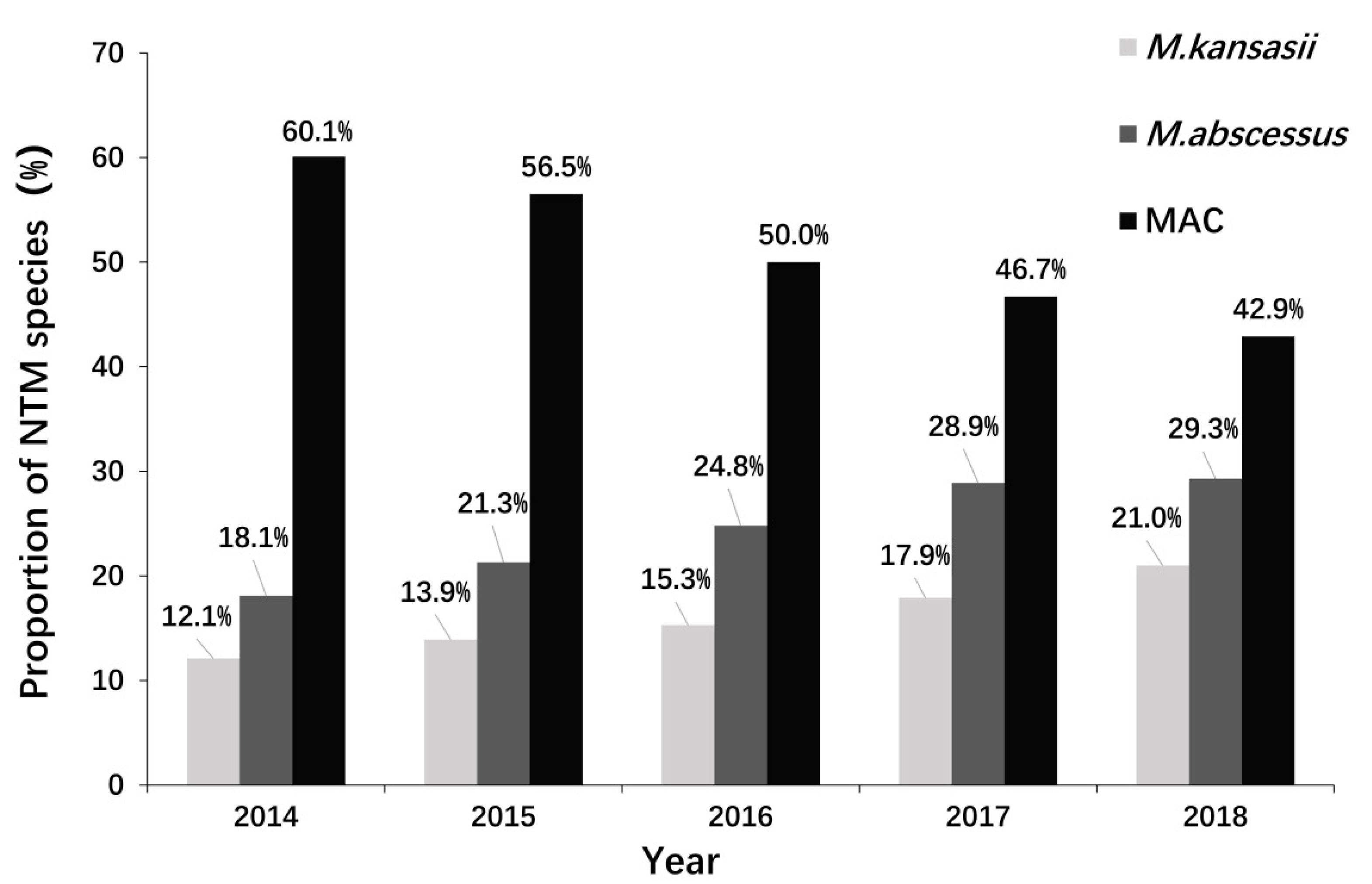
3.1. Abundances of Different NTM Species in Patients with NTMPD
3.2. Drug Susceptibility of the Three Major NTM Species
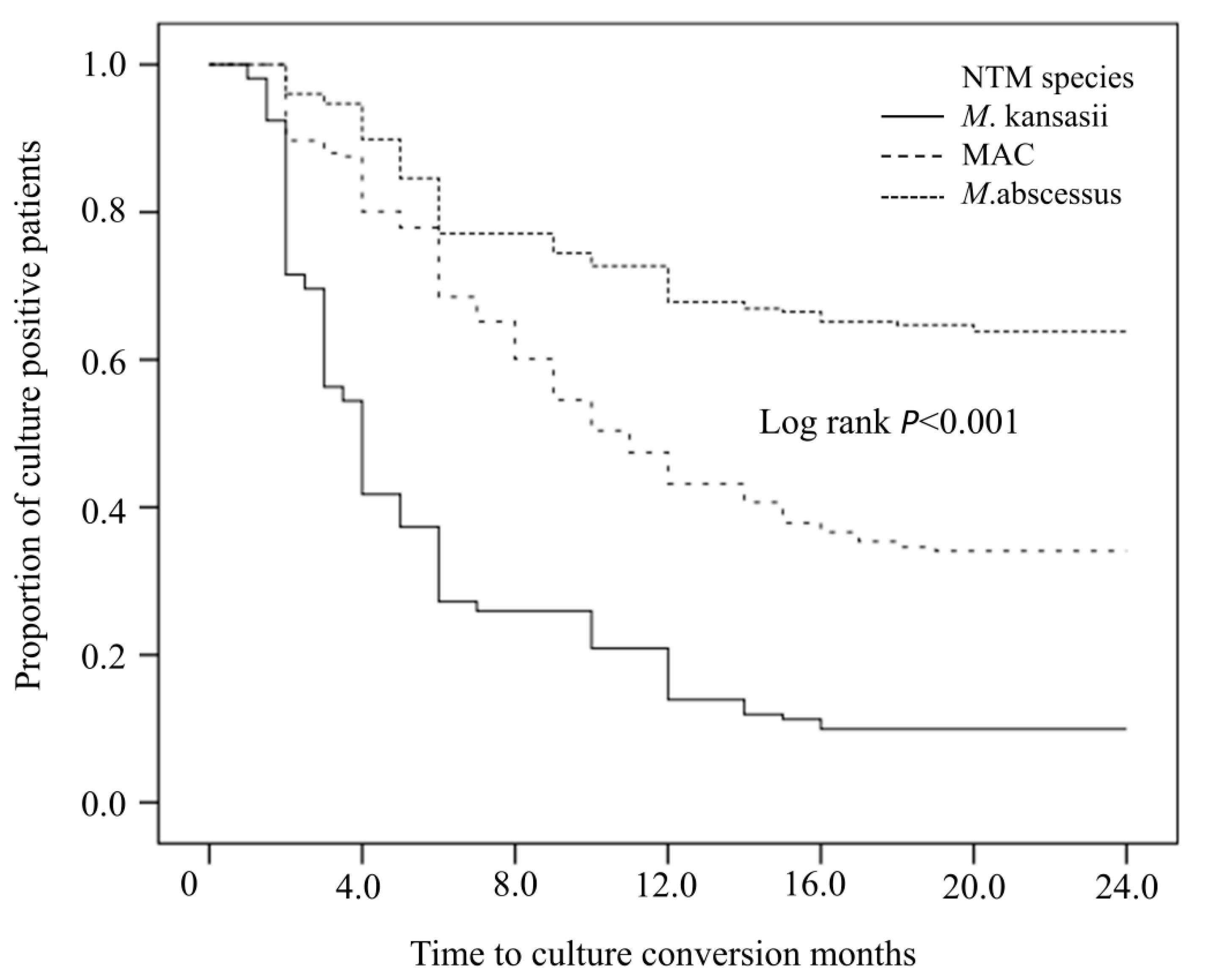
3.3. Outcomes and Sputum Culture Conversion Rates of Isolates from NTMPD Patients Infected with the Three Major Species
3.4. Univariate Analysis of Factors Associated with Treatment Failure in NTMPD Patients
3.5. Multivariate Analysis of Factors Associated with Treatment Failure in NTMPD Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haworth, C.S.; Banks, J.; Capstick, T.; Fisher, A.J.; Gorsuch, T.; Laurenson, I.F.; Leitch, A.; Loebinger, M.R.; Milburn, H.J.; Nightingale, M.; et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017, 72 (Suppl. 2), ii1–ii64. [Google Scholar] [CrossRef] [Green Version]
- Ratnatunga, C.N.; Lutzky, V.P.; Kupz, A.; Doolan, D.L.; Reid, D.W.; Field, M.; Bell, S.C.; Thomson, R.M.; Miles, J.J. The Rise of Non-Tuberculosis Mycobacterial Lung Disease. Front. Immunol. 2020, 11, 303. [Google Scholar] [CrossRef] [Green Version]
- Mirsaeidi, M.; Farshidpour, M.; Allen, M.B.; Ebrahimi, G.; Falkinham, J.O. Highlight on Advances in Nontuberculous Mycobacterial Disease in North America. BioMed Res. Int. 2014, 2014, 919474. [Google Scholar] [CrossRef]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J.; Andrejak, C.; Böttger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur. Respir. J. 2020, 56, 2000535. [Google Scholar] [CrossRef]
- Haworth, C.S.; Floto, R.A. Introducing the new BTS Guideline: Management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017, 72, 969–970. [Google Scholar] [CrossRef]
- Jankovic, M.; Sabol, I.; Zmak, L.; Jankovic, V.K.; Jakopovic, M.; Obrovac, M.; Ticac, B.; Bulat, L.K.; Grle, S.P.; Marekovic, I.; et al. Microbiological criteria in non-tuberculous mycobacteria pulmonary disease: A tool for diagnosis and epidemiology. Int. J. Tuberc. Lung Dis. 2016, 20, 934–940. [Google Scholar] [CrossRef] [Green Version]
- Prevots, D.R.; Marras, T.K. Epidemiology of human pulmonary infection with nontuberculous mycobacteria: A review. Clin. Chest Med. 2015, 36, 13–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philley, J.V.; Griffith, D.E. Treatment of slowly growing mycobacteria. Clin. Chest Med. 2015, 36, 79–90. [Google Scholar] [CrossRef]
- Kasperbauer, S.H.; De Groote, M.A. The treatment of rapidly growing mycobacterial infections. Clin. Chest Med. 2015, 36, 67–78. [Google Scholar] [CrossRef]
- Van Ingen, J.; Aksamit, T.; Andrejak, C.; Böttger, E.C.; Cambau, E.; Daley, C.L.; Griffith, D.E.; Guglielmetti, L.; Holland, S.M.; Huitt, G.A.; et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: An NTM-NET consensus statement. Eur. Respir. J. 2018, 51, 1800170. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Zhang, Y.; Li, J.; Lin, S.; Wang, L.; Jiang, Y.; Pan, Q.; Shen, X. Increase in Nontuberculous Mycobacteria Isolated in Shanghai, China: Results from a Population-Based Study. PLoS ONE 2014, 9, e109736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Luo, M.; Zhang, K.; Yang, X.; Hu, K.; Fu, Z.; Zhang, L.; Wu, P.; Wan, D.; Han, M.; et al. Species identification and antimicrobial susceptibility testing of non-tuberculous mycobacteria isolated in Chongqing, Southwest China. Epidemiol Infect. 2021, 149, e7. [Google Scholar] [CrossRef]
- Zweijpfenning, S.M.H.; Ingen, J.V.; Hoefsloot, W. Geographic Distribution of Nontuberculous Mycobacteria Isolated from Clinical Specimens: A Systematic Review. Semin. Respir. Crit. Care Med. 2018, 39, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, X.; Jin, J.; Wu, J.; Zhang, X.; Chen, J.; Zhang, W. In Vitro Susceptibility of Mycobacterium abscessus and Mycobacterium fortuitum Isolates to 30 Antibiotics. BioMed. Res Int. 2018, 2018, 4902941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.; Xu, D.; Liu, H.; Wan, K.; Wang, R.; Yang, Z. Trends in the Prevalence and Antibiotic Resistance of Non-tuberculous Mycobacteria in Mainland China, 2000–2019, Systematic Review and Meta-Analysis. Front. Public Health 2020, 8, 295. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Davies, D. Origins and evolution of antibiotic resistance. Microbiol. Mol. Biol. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Jarand, J.; Levin, A.; Zhang, L.; Huitt, G.; Mitchell, J.D.; Daley, C.L. Clinical and microbiologic outcomes in patients receiving treatment for Mycobacterium abscessus pulmonary disease. Clin. Infect. Dis. 2011, 52, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Hoefsloot, W.; van Ingen, J.; de Lange, W.C.; Dekhuijzen, P.N.; Boeree, M.J.; van Soolingen, D. Clinical relevance of Mycobacterium malmoense isolation in the Netherlands. Eur. Respir. J. 2009, 34, 926–931. [Google Scholar] [CrossRef] [Green Version]
- Litvinov, V.; Makarova, M.; Galkina, K.; Khachaturiants, E.; Krasnova, M.; Guntupova, L.; Safonova, S. Drug susceptibility testing of slowly growing non-tuberculous mycobacteria using slomyco test-system. PLoS ONE 2018, 13, e0203108. [Google Scholar] [CrossRef]
- Weng, Y.W.; Huang, C.K.; Sy, C.L.; Wu, K.S.; Tsai, H.C.; Lee, S.S. Treatment for Mycobacterium abscessus complex-lung disease. J. Formos. Med. Assoc. 2020, 119 (Suppl. 1), S58–S66. [Google Scholar] [CrossRef]
- Hatakeyama, S.; Ohama, Y.; Okazaki, M.; Nukui, Y.; Moriya, K. Antimicrobial susceptibility testing of rapidly growing mycobacteria isolated in Japan. BMC Infect. Dis. 2017, 17, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Q.; Wei, J.; Zou, W.; Li, Q.; Qian, X.; Zhu, Z. Antimicrobial susceptibility profiles of Mycobacterium abscessus complex isolates from respiratory specimens in Shanghai, China. J. Glob. Antimicrob Resist. 2021, 25, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Takayanagi, N.; Kanauchi, T.; Miyahara, Y.; Yanagisawa, T.; Sugita, Y. Prognostic factors of 634 HIV-negative patients with Mycobacterium avium complex lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Lipman, M.; Hoefsloot, W. High mortality in patients with Mycobacterium avium complex lung disease: A systematic review. BMC Infect. Dis. 2018, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Mirsaeidi, M.; Machado, R.F.; Garcia, J.G.; Schraufnagel, D.E. Nontuberculous mycobacterial disease mortality in the United States, 1999–2010, a population-based comparative study. PLoS ONE 2014, 9, e91879. [Google Scholar] [CrossRef]
- Andréjak, C.; Thomsen, V.Ø.; Johansen, I.S.; Riis, A.; Benfield, T.L.; Duhaut, P.; Sørensen, H.T.; Lescure, F.X.; Thomsen, R.W. Nontuberculous pulmonary mycobacteriosis in Denmark: Incidence and prognostic factors. Am. J. Respir. Crit. Care Med. 2010, 181, 514–521. [Google Scholar] [CrossRef]
- Fujiwara, K.; Furuuchi, K.; Aono, A.; Uesugi, F.; Shirai, T.; Nakamoto, K.; Shimada, T.; Mochizuki, F.; Tanaka, Y.; Iijima, H.; et al. Clinical risk factors related to treatment failure in Mycobacterium abscessus lung disease. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 247–254. [Google Scholar] [CrossRef]
- Gochi, M.; Takayanagi, N.; Kanauchi, T.; Ishiguro, T.; Yanagisawa, T.; Sugita, Y. Retrospective study of the predictors of mortality and radiographic deterioration in 782 patients with nodular/bronchiectatic Mycobacterium avium complex lung disease. BMJ Open 2015, 5, e008058. [Google Scholar] [CrossRef] [Green Version]
- Yamakawa, H.; Takayanagi, N.; Miyahara, Y.; Ishiguro, T.; Kanauchi, T.; Hoshi, T.; Yanagisawa, T.; Sugita, Y. Prognostic factors and radiographic outcomes of nontuberculous mycobacterial lung disease in rheumatoid arthritis. J. Rheumatol. 2013, 40, 1307–1315. [Google Scholar] [CrossRef]
- González-Pérez, M.; Mariño-Ramírez, L.; Parra-López, C.A.; Murcia, M.I.; Marquina, B.; Mata-Espinoza, D.; Rodriguez-Míguez, Y.; Baay-Guzman, G.J.; Huerta-Yepez, S.; Hernandez-Pando, R. Virulence and immune response induced by Mycobacterium avium complex strains in a model of progressive pulmonary tuberculosis and subcutaneous infection in BALB/c mice. Infect. Immun. 2013, 81, 4001–4012. [Google Scholar] [CrossRef] [Green Version]
- Mori, S.; Koga, Y.; Nakamura, K.; Hirooka, S.; Matsuoka, T.; Uramoto, H.; Sakamoto, O.; Ueki, Y. Mortality in rheumatoid arthritis patients with pulmonary nontuberculous mycobacterial disease: A retrospective cohort study. PLoS ONE 2020, 15, e0243110. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Ito, A.; Hashimoto, T.; Marumo, S.; Tokumasu, H.; Kotani, A.; Yamaki, H.; Shirata, M.; Furuuchi, K.; Fukui, M.; et al. Development and validation of a prognostic scoring model for Mycobacterium avium complex lung disease: An observational cohort study. BMC Infect. Dis. 2017, 17, 436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, C.; Huang, L.; Cai, M.; Wang, W.; Shi, X.; Chen, W. Characterization of non-tuberculous mycobacterial pulmonary disease in Nanjing district of China. BMC Infect. Dis. 2019, 19, 764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, I.; Yasin, A.; Fuks, L.; Stein, N.; Saliba, W.; Kramer, M.R.; Adir, Y.; Shteinberg, M. Radiologic Characteristics of Non-tuberculous Mycobacteria Infection in Patients with Bronchiectasis. Lung 2020, 198, 715–722. [Google Scholar] [CrossRef]
- Gopalaswamy, R.; Shanmugam, S.; Mondal, R.; Subbian, S. Of tuberculosis and non-tuberculous mycobacterial infections-a comparative analysis of epidemiology, diagnosis and treatment. J. Biomed. Sci. 2020, 27, 74. [Google Scholar] [CrossRef]
- Bai, X.; Bai, A.; Honda, J.R.; Eichstaedt, C.; Musheyev, A.; Feng, Z.; Huitt, G.; Harbeck, R.; Kosmider, B.; Sandhaus, R.A.; et al. Alpha-1-Antitrypsin Enhances Primary Human Macrophage Immunity Against Non-tuberculous Mycobacteria. Front. Immunol. 2019, 10, 1417. [Google Scholar] [CrossRef]
- López, C.M.; Gallego, C.L.; Calvo, J.C.; Vasallo, I.J.T.; Ramírez, M.T.R. Patients with non-tuberculous mycobacteria in respiratory samples: A 5-year epidemiological study. Rev. Esp. Quimioter. 2021, 34, 120–125. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | M. kansasii (n = 158) | MAC (n = 417) | M. abscessus (n = 227) |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Am | 4 (2.5) | 90 (21.6) | 57 (25.1) |
| INH | 40 (25.3) | 356 (85.4) | 227 (100) |
| RFP | 22 (13.9) | 165 (39.6) | 225 (99.1) |
| EMB | 30 (19.0) | 106 (27.8) | 223 (98.2) |
| Ofx | 20 (12.7) | 225 (54.0) | 225 (99.1) |
| Outcome | M. Kansasii (n = 158) | MAC (n = 417) | M. abscessus (n = 227) | χ2 | p a |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Success | 142(89.9) | 271(65.0) | 82(36.1) | 117.841 | <0.001 |
| Failure | 16(10.1) | 146(35.0) | 145(63.9) | 117.841 | <0.001 |
| Recurrence (within 1 year) | 1(0.6) | 9(2.1) | 11(4.8) | -- | 0.027 a |
| Factor | Success (n = 495) | Failure (n = 307) | OR | 95% CI | p Value |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age, years | |||||
| 18~44 | 145(29.3) | 46(15.0) | 1(ref) | ||
| 45~60 | 161(32.5) | 104(33.9) | 2.036 | 1.347, 3.078 | 0.001 |
| >60 | 189(38.2) | 157(51.1) | 2.618 | 1.767, 3.881 | <0.001 |
| Female | 244(49.3) | 186(60.6) | 1.581 | 1.185, 2.111 | 0.002 |
| Retreatment NTMPD | 131(26.5) | 155(50.5) | 2.881 | 2.121, 3.912 | <0.001 |
| Smoking history | 50(10.1) | 22(7.2) | 0.571 | 0.369, 1.732 | 0.800 |
| Rural residence | 215(43.4) | 141(45.9) | 1.112 | 0.831, 1.488 | 0.476 |
| History of pulmonary TB | 137(27.7) | 94(30.6) | 1.145 | 0.836, 1.568 | 0.399 |
| COPD | 27(5.4) | 32(10.4) | 2.167 | 1.279, 3.670 | 0.004 |
| Pneumoconiosis | 17(3.4) | 10(3.3) | 1.193 | 0.728, 2.095 | 0.893 |
| Long-term use of corticosteroid/immunosuppressant | 13(2.6) | 12(3.9) | 1.508 | 0.679, 3.349 | 0.313 |
| Diabetes Mellitus | 34(6.9) | 16(5.2) | 0.746 | 0.404, 1.375 | 0.347 |
| BMI (kg/m2) | |||||
| ≥18.5 | 322(65.1) | 180(58.6) | 1(ref) | ||
| <18.5 | 173(34.9) | 127(41.4) | 1.313 | 0.980, 1.760 | 0.068 |
| Pulmonary cavities | 249(50.3) | 180(58.6) | 1.404 | 1.056, 1.873 | 0.020 |
| Bronchiectasis | 306(61.8) | 218(71.0) | 1.513 | 1.114, 2.055 | 0.008 |
| Involvement of lung fields | |||||
| 1~2 | 146(29.5) | 51(16.6) | 1(ref) | ||
| 3~4 | 115(23.2) | 73(23.8) | 1.817 | 1.178, 2.802 | 0.007 |
| 5~6 | 234(47.3) | 183(59.6) | 2.239 | 1.542, 3.251 | <0.001 |
| ESR(mm/L) | |||||
| <15 | 168(33.9) | 73(23.8) | 1(ref) | ||
| 15~60 | 272(54.9) | 164(53.4) | 1.388 | 0.991, 1.942 | 0.056 |
| >60 | 55(11.2) | 70(22.8) | 2.929 | 1.872, 4.582 | <0.001 |
| Anemia | 417(84.2) | 256(83.4) | 0.927 | 0.630, 1.364 | 0.700 |
| Albumin (g/L) | |||||
| >34 | 430(86.9) | 247(80.5) | 1(ref) | ||
| 25~34 | 53(10.7) | 51(16.6) | 1.304 | 0.784, 2.171 | 0.306 |
| <25 | 12(2.4) | 9(2.9) | 2.036 | 1.169, 3.522 | 0.813 |
| Flow Cytometry | |||||
| CD4+ (<0.34) | 307(62.0) | 172(56.0) | 1.276 | 0.845, 1.926 | 0.247 |
| CD8+ (<0.25) | 147(29.7) | 94(30.6) | 0.959 | 0.617, 1.490 | 0.853 |
| CD4+/CD8+ (<0.68) | 482(97.4) | 296(96.4) | 1.437 | 0.431, 4.793 | 0.555 |
| Bacterial species | |||||
| M. kansasii | 142(28.7) | 16(5.2) | 1(ref) | ||
| MAC | 271(54.7) | 146(47.6) | 4.781 | 2.746, 8.326 | <0.001 |
| M. abscessus | 82(16.6) | 145(47.2) | 15.694 | 8.756, 28.128 | <0.001 |
| Treatment regimen changes | 143(28.9) | 108(21.8) | 1.336 | 0.985, 1.811 | 0.062 |
| Adverse drug reactions | |||||
| Hepatotoxicity | 43(8.7) | 24(4.8) | 0.891 | 0.529, 1.501 | 0.666 |
| Cytopenia | 43(8.7) | 21(6.8) | 0.618 | 0.255, 1.498 | 0.287 |
| Hypersensitivity | 17(3.4) | 14(4.6) | 1.344 | 0.653, 2.766 | 0.423 |
| Gastrointestinal | 21(4.2) | 26(8.5) | 2.088 | 1.153, 3.781 | 0.015 |
| Factor | aOR | 95% CI | p Value |
|---|---|---|---|
| Retreatment NTMPD | 2.074 | 1.470, 2.926 | <0.001 |
| Age, years | |||
| 18~44 | 1(ref) | ||
| 45~60 | 1.661 | 1.038, 2.659 | 0.034 |
| >60 | 1.739 | 1.088, 2.778 | 0.021 |
| ESR(mm/h) | |||
| <15 | 1(ref) | ||
| 15~60 | 1.185 | 0.800,1.755 | 0.398 |
| >60 | 2.658 | 1.560, 4.529 | <0.001 |
| Bacterial species | |||
| M. kansasii | 1(ref) | ||
| MAC | 2.970 | 1.620, 5.443 | <0.001 |
| M. abscessus | 9.355 | 4.977, 17.584 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, L.-P.; Chen, S.-H.; Lou, H.; Gui, X.-W.; Shen, X.-N.; Cao, J.; Sha, W.; Sun, Q. Factors Associated with Treatment Outcome in Patients with Nontuberculous Mycobacterial Pulmonary Disease: A Large Population-Based Retrospective Cohort Study in Shanghai. Trop. Med. Infect. Dis. 2022, 7, 27. https://doi.org/10.3390/tropicalmed7020027
Cheng L-P, Chen S-H, Lou H, Gui X-W, Shen X-N, Cao J, Sha W, Sun Q. Factors Associated with Treatment Outcome in Patients with Nontuberculous Mycobacterial Pulmonary Disease: A Large Population-Based Retrospective Cohort Study in Shanghai. Tropical Medicine and Infectious Disease. 2022; 7(2):27. https://doi.org/10.3390/tropicalmed7020027
Chicago/Turabian StyleCheng, Li-Ping, Shan-Hao Chen, Hai Lou, Xu-Wei Gui, Xiao-Na Shen, Jie Cao, Wei Sha, and Qin Sun. 2022. "Factors Associated with Treatment Outcome in Patients with Nontuberculous Mycobacterial Pulmonary Disease: A Large Population-Based Retrospective Cohort Study in Shanghai" Tropical Medicine and Infectious Disease 7, no. 2: 27. https://doi.org/10.3390/tropicalmed7020027