
Pandora’s Box: Disseminated Coccidioidomycosis Associated with Self-Medication with an Unregulated Potent Corticosteroid Acquired in Mexico


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case
3. Discussion
3.1. Dissemination in Coccidioidomycosis and in This Patient
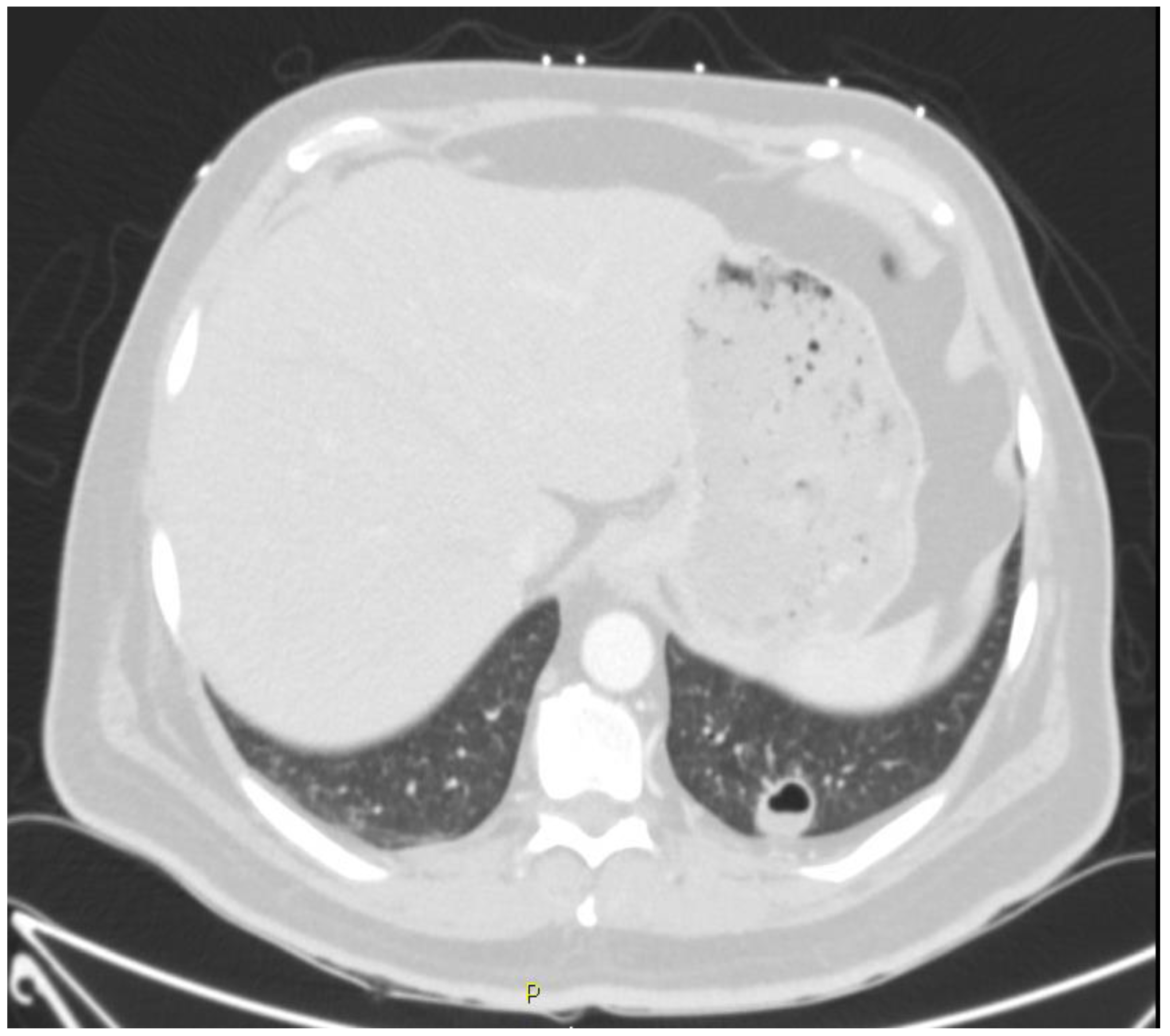
3.2. Pulmonary Manifestations of Coccidioidomycosis and in This Patient
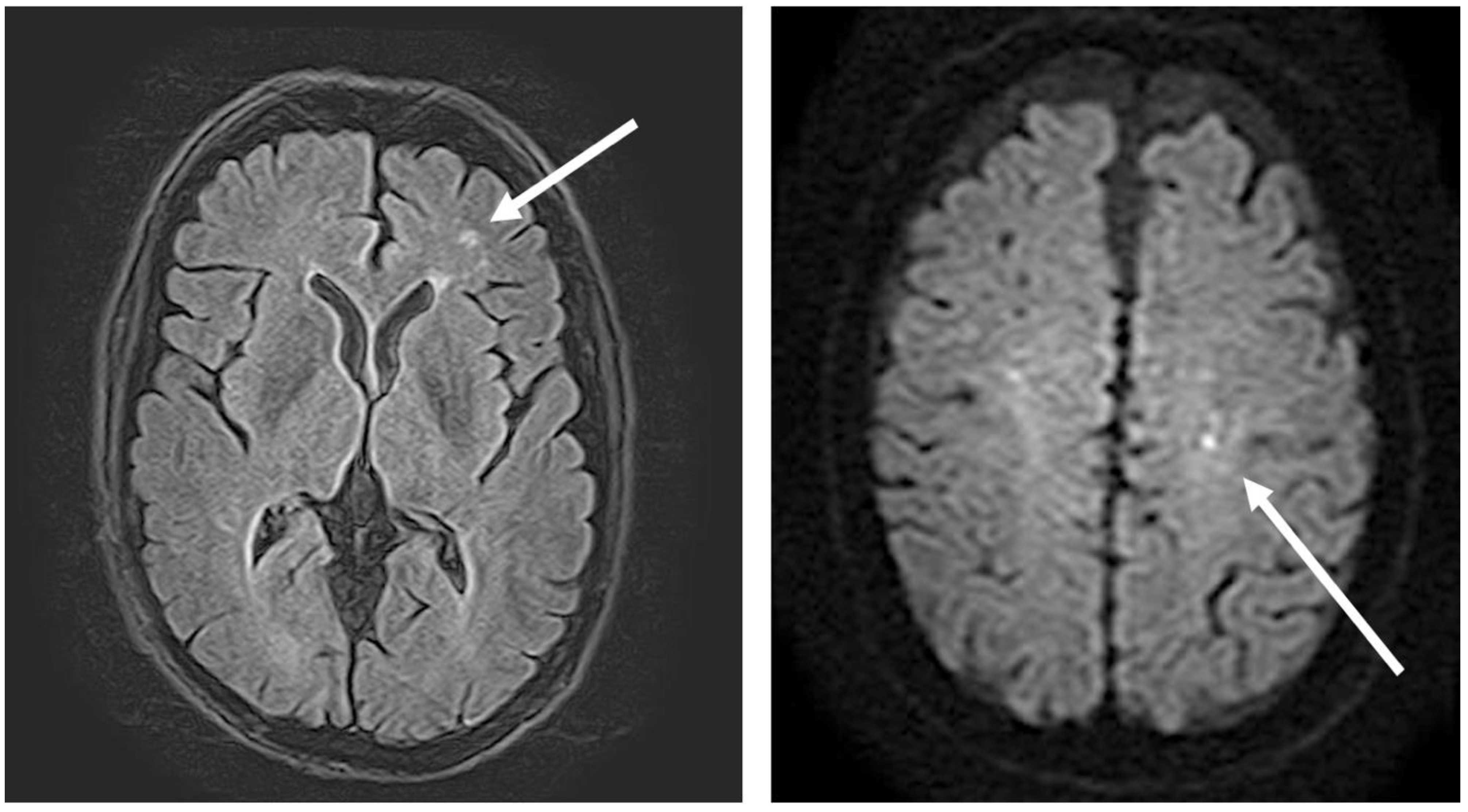
3.3. Central Nervous System Manifestations of Coccidioidomycosis and in This Patient
3.4. Osteoarticular Manifestations of Coccidioidomycosis and in This Patient
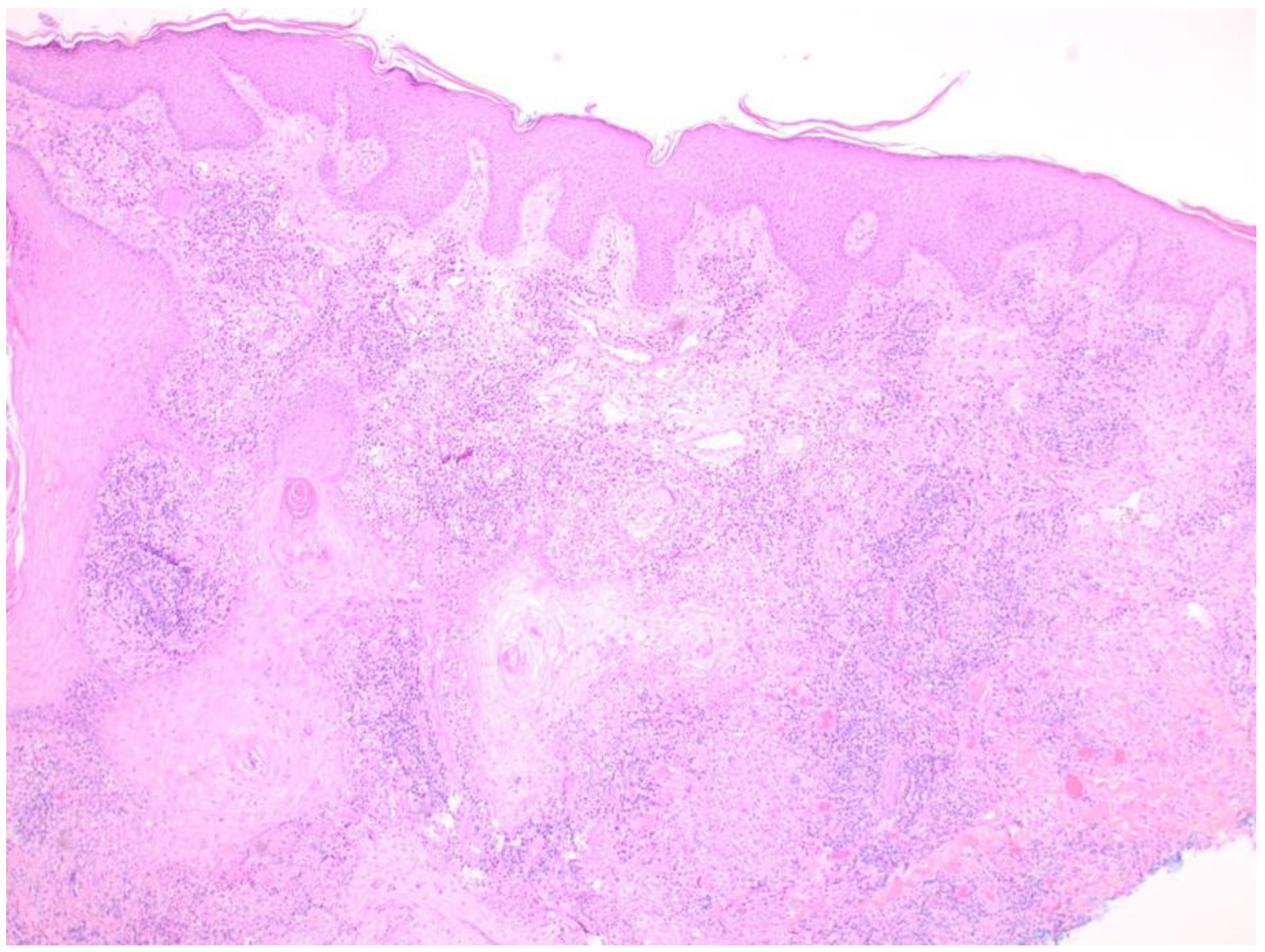
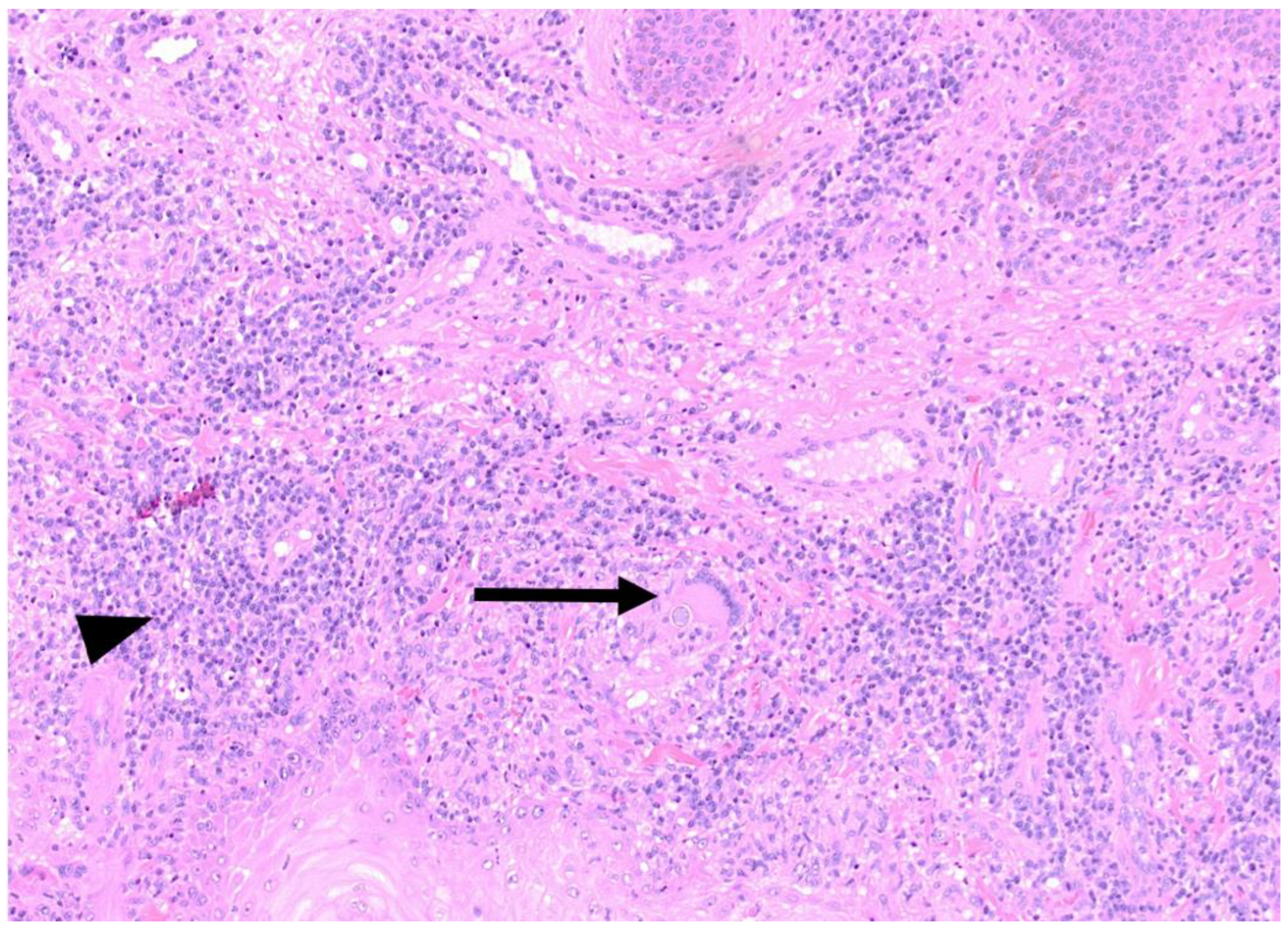
3.5. Skin Manifestations of Coccidioidomycosis and in This Patient
3.6. Ocular Manifestations of Coccidioidomycosis and in This Patient
3.7. The Dangers of Self-Medication
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Laniado-Laborín, R.; Arathoon, E.G.; Canteros, C.; Muñiz-Salazar, R.; Rendon, A. Coccidioidomycosis in Latin America. Med. Mycol. 2019, 57, S46–S55. [Google Scholar] [CrossRef] [PubMed]
- Odio, C.D.; Marciano, B.E.; Galgiani, J.N.; Holland, S.M. Risk factors for disseminated coccidioidomycosis, United States. Emerg. Infect. Dis. 2017, 23, 308–311. [Google Scholar] [CrossRef]
- Van Dyke, M.C.C.; Thompson, G.R.; Galgiani, J.N.; Barker, B.M. The rise of Coccidioides: Forces against the dust devil unleashed. Front. Immunol. 2019, 10, 2188. [Google Scholar] [CrossRef] [PubMed]
- Stockamp, N.W.; Thompson, G.R., 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2016, 30, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, E.C., III; Bone, W.D.; Martin, C.R.; Gray, G.C.; Olson, P.; Schillaci, R.F. Prediction of relapse after treatment of coccidioidomycosis. Clin. Infect. Dis. 1997, 25, 1205–1210. [Google Scholar] [CrossRef] [Green Version]
- Paliogianni, F.; Ahuja, S.S.; Balow, J.P.; Balow, J.E.; Boumpas, D.T. Novel mechanism for inhibition of human T cells by glucocorticoids. Glucocorticoids inhibit signal transduction through IL-2 receptor. J. Immunol. 1993, 151, 4081–4089. [Google Scholar]
- Cohen, J.J.; Duke, R.C. Glucocorticoid activation of a calcium-dependent endonuclease in thymocyte nuclei leads to cell death. J. Immunol. 1984, 132, 38–42. [Google Scholar]
- Liu, D.; Ahmet, A.; Ward, L.; Krishnamoorthy, P.; Mandelcorn, E.; Leigh, R.; Brown, J.P.; Cohen, A.; Kim, H. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin. Immunol. 2013, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Santelli, A.C.; Blair, J.E.; Roust, L.R. Coccidioidomycosis in patients with diabetes mellitus. Am. J. Med. 2006, 119, 964–969. [Google Scholar] [CrossRef]
- Anstead, G.M.; Graybill, J.R. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2006, 20, 621–643. [Google Scholar] [CrossRef]
- Panicker, R.R.; Bartels, H.C.; Gotway, M.B.; Ampel, N.M.; Buras, M.R.; Lim, E.S.; Blair, J.E. Cavitary coccidioidomycosis: Impact of azole antifungal therapy. Med. Mycol. 2021, 59, 834–841. [Google Scholar] [CrossRef]
- Chee, D.; Moritz, A.W.; Profit, A.P.; Agarwal, A.N.; Anstead, G.M. Fatal coccidioidomycosis involving the lungs, brain, tongue, and adrenals in a cirrhotic patient. An autopsy case. IDCases 2021, 23, e01049. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.H.; Einstein, H.E. Coccidioidal meningitis. Clin. Infect. Dis. 2006, 42, 103–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, R.; Ho, J.; Fowler, P.; Heidari, A. Coccidioidal meningitis: A review on diagnosis, treatment, and management of complications. Curr. Neurol. Neurosci. Rep. 2018, 18, 19. [Google Scholar] [CrossRef]
- Phelps, R.R.L.; Lu, A.Y.; Lee, A.T.; Yue, J.K.; Winkler, E.A.; Raygor, K.P.; Oh, T.; Barkovich, M.J.; Hollander, H. Cerebrovascular complications of coccidioidomycosis meningitis: Case report and systematic review. J. Clin. Neurosci. 2020, 80, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Arsura, E.L.; Johnson, R.; Penrose, J.; Stewart, K.; Kilgore, W.; Reddy, C.M.; Bobba, R.K. Neuroimaging as a guide to predict outcomes for patients with coccidioidal meningitis. Clin. Infect. Dis. 2006, 40, 624–627. [Google Scholar] [CrossRef]
- Thompson, G.R., 3rd; Blair, J.E.; Wang, S.; Bercovitch, R.; Bolaris, M.; Van Den Akker, D.; Lopez, R.; Heidari, A.; Catanzaro, A.; Cadena, J.; et al. Adjunctive corticosteroid therapy in the treatment of coccidioidal meningitis. Clin. Infect. Dis. 2017, 65, 338–341. [Google Scholar] [CrossRef] [Green Version]
- Ricciotti, R.W.; Shekhel, T.A.; Blair, J.E.; Colby, T.V.; Sobonya, R.E.; Larsen, B.T. Surgical pathology of skeletal coccidioidomycosis. A clinical and histopathologic analysis of 25 cases. Am. J. Surg. Pathol. 2014, 38, 1672–1680. [Google Scholar] [CrossRef]
- May, D.A.; Disler, D.G. Diagnosis please. Case 50: Primary coccidioidal synovitis of the knee. Radiology 2002, 224, 665–668. [Google Scholar] [CrossRef]
- Bayer, A.S.; Guze, L.B. Fungal arthritis. II. Coccidioidal synovitis: Clinical, diagnostic, therapeutic, and prognostic considerations. Semin. Arthritis Rheum. 1979, 8, 200–211. [Google Scholar] [CrossRef]
- Arsura, E.L.; Kilgore, W.B.; Caldwell, J.W.; Freeman, J.C.; Einstein, H.E.; Johnson, R.H. Association between facial cutaneous coccidioidomycosis and meningitis. West. J. Med. 1998, 169, 13–16. [Google Scholar] [PubMed]
- Mott, R.T.; Rosenberg, A.; Livingston, S.; Morgan, M.B. Melanoma associated with pseudoepitheliomatous hyperplasia: A case series and investigation into the role of epidermal growth factor receptor. J. Cutan. Pathol. 2002, 29, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.B.; Feldman, J.S.; Leyva, W.H.; DiCaudo, D.J. Clinical and pathologic characteristics of disseminated cutaneous coccidioidomycosis. J. Am. Acad. Dermatol. 2010, 62, 831–837. [Google Scholar] [CrossRef]
- Cunningham, E.T., Jr.; Seiff, S.R.; Berger, T.G.; Lizotte, P.E.; Howes, E.L., Jr.; Horton, J.C. Intraocular coccidioidomycosis diagnosed by skin biopsy. Arch. Ophthalmol. 1998, 116, 674–677. [Google Scholar] [CrossRef] [Green Version]
- Zayour, M.; Lazova, R. Pseudoepitheliomatous hyperplasia: A review. Amer. J. Dermatopathol. 2011, 33, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Rodenbiker, H.T.; Ganley, J.P. Ocular coccidioidomycosis. Surv. Ophthalmol. 1980, 24, 263–290. [Google Scholar] [CrossRef]
- Rodenbiker, H.T.; Ganley, J.P.; Galgiani, J.N.; Axline, S.G. Prevalence of chorioretinal scars associated with coccidioidomycosis. Arch. Ophthalmol. 1981, 99, 71–75. [Google Scholar] [CrossRef]
- Nordstrom, B.; Sherpa, N.; Marshall, M.; Chawla, A.; Heidari, A.; Johnson, R. Coccidioidomycosis chorioretinitis. J. Investig. Med. High Impact Case Rep. 2019, 7, 2324709619881561. [Google Scholar] [CrossRef] [Green Version]
- Toomey, C.B.; Gross, A.; Lee, J.; Spencer, D.B. A case of unilateral coccidioidal chorioretinitis in a patient with HIV-associated meningoencephalitis. Case Rep. Ophthalmol. Med. 2019, 2019, 1475628. [Google Scholar] [CrossRef]
- Quinlan, E.J.; Gill, V. Initial presentation of disseminated coccidioidomycosis with ocular lesions. Case Rep. Infect. Dis. 2020, 2020, 1305193. [Google Scholar] [CrossRef] [Green Version]
- Gabrielian, A.; Hariprasad, S.M. New onset of bilateral multifocal coccidioidomycosal choroiditis in a patient on oral fluconazole. Can. J. Ophthalmol. 2010, 45, 419–420. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos-Santos, D.V.; Lim, J.I.; Rao, N.A. Chronic coccidioidomycosis endophthalmitis without concomitant systemic involvement: A clinicopathological case report. Ophthalmology 2010, 117, 1839–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. 2016 Infectious Diseases Society of America (IDSA) clinical practice guideline for the treatment of coccidioidomycosis. Clin. Infect. Dis. 2016, 63, e112–e146. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.E. Risks of self-medication practices. Curr. Drug Saf. 2010, 5, 315–323. [Google Scholar] [CrossRef]
- Weber, T. Lethal drug trade: Unsafe medicines from Mexico. Los Angeles Times. 23 May 1999. Los Angeles, CA, USA. Available online: https://www.latimes.com/archives/la-xpm-1999-may-23-mn-40177-story.html (accessed on 3 July 2021).
- Chauhan, V.; Thakur, S. State of the globe: The frenzy of self-medication, cocktail regimens and everchanging guidelines on SARS-CoV-2. J. Glob. Infect. Dis. 2021, 13, 65–66. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coba, A.J.; Sallee, P.K.; Dixon, D.O.; Alkhateb, R.; Anstead, G.M. Pandora’s Box: Disseminated Coccidioidomycosis Associated with Self-Medication with an Unregulated Potent Corticosteroid Acquired in Mexico. Trop. Med. Infect. Dis. 2021, 6, 207. https://doi.org/10.3390/tropicalmed6040207
Coba AJ, Sallee PK, Dixon DO, Alkhateb R, Anstead GM. Pandora’s Box: Disseminated Coccidioidomycosis Associated with Self-Medication with an Unregulated Potent Corticosteroid Acquired in Mexico. Tropical Medicine and Infectious Disease. 2021; 6(4):207. https://doi.org/10.3390/tropicalmed6040207
Chicago/Turabian StyleCoba, Alejandro Jose, Patricia K. Sallee, Danielle O. Dixon, Rahaf Alkhateb, and Gregory M. Anstead. 2021. "Pandora’s Box: Disseminated Coccidioidomycosis Associated with Self-Medication with an Unregulated Potent Corticosteroid Acquired in Mexico" Tropical Medicine and Infectious Disease 6, no. 4: 207. https://doi.org/10.3390/tropicalmed6040207