
Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting: Zimbabwe and Harare
2.2.2. TB and HIV Services
2.2.3. Data Monitoring, Recording and Reporting for the Study in Health Facilities in Harare
2.3. Study Population
2.4. Data Variables, Sources of Data and Timing of Data Collection
2.5. Analysis and Statistics
3. Results
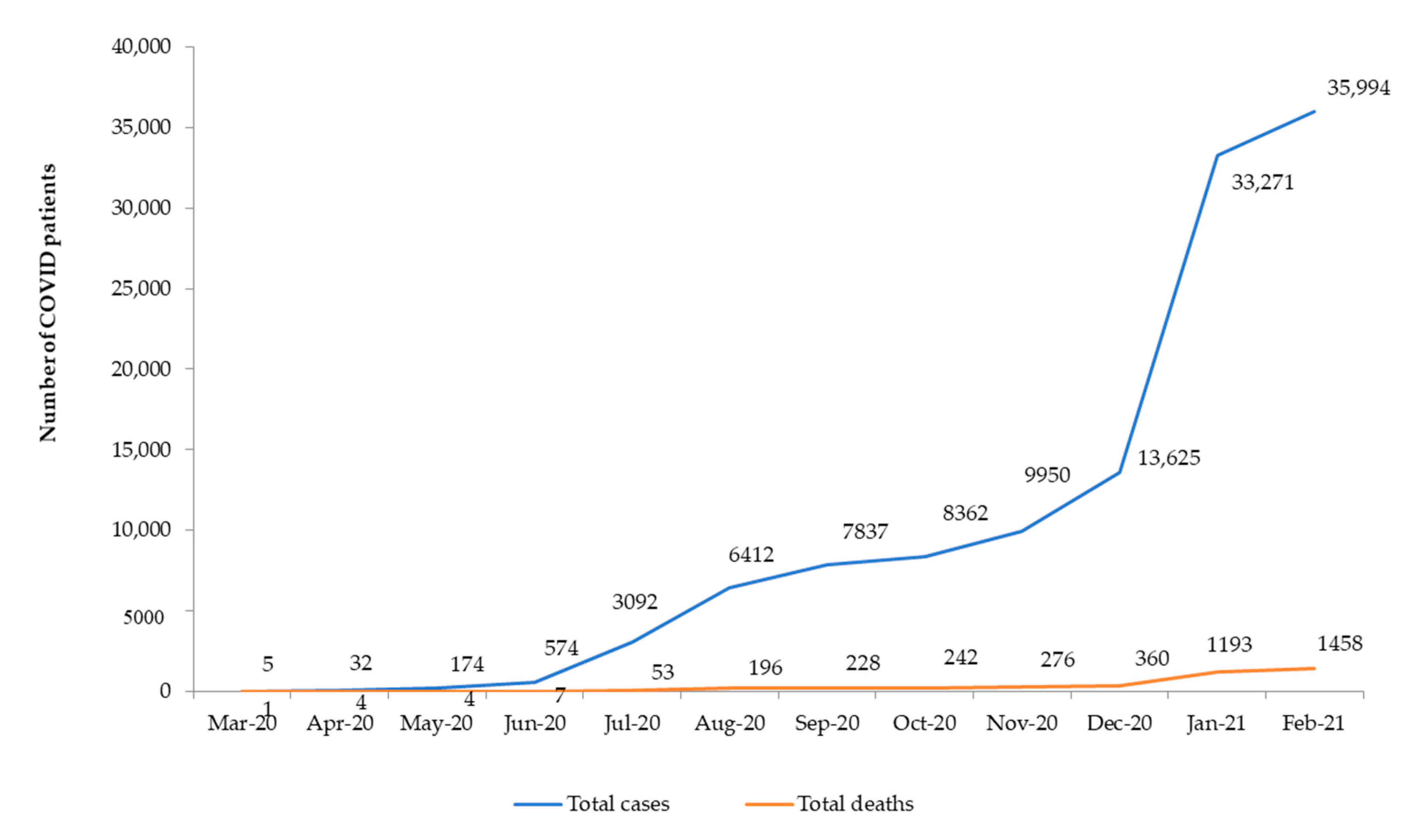
3.1. COVID-19 Cases and Deaths and General Effects on Health Services
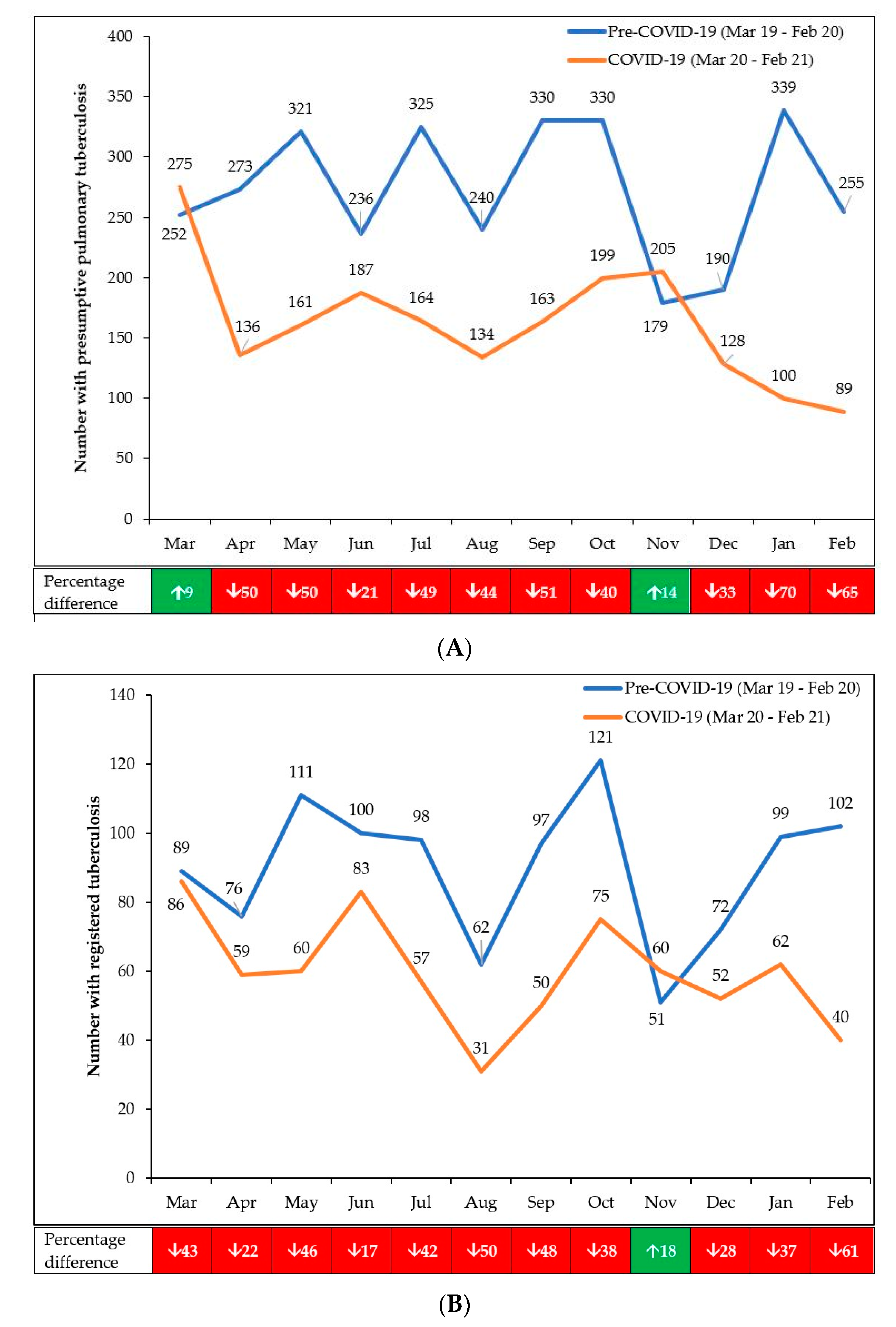
3.2. TB Case Finding, Diagnosis and Registration
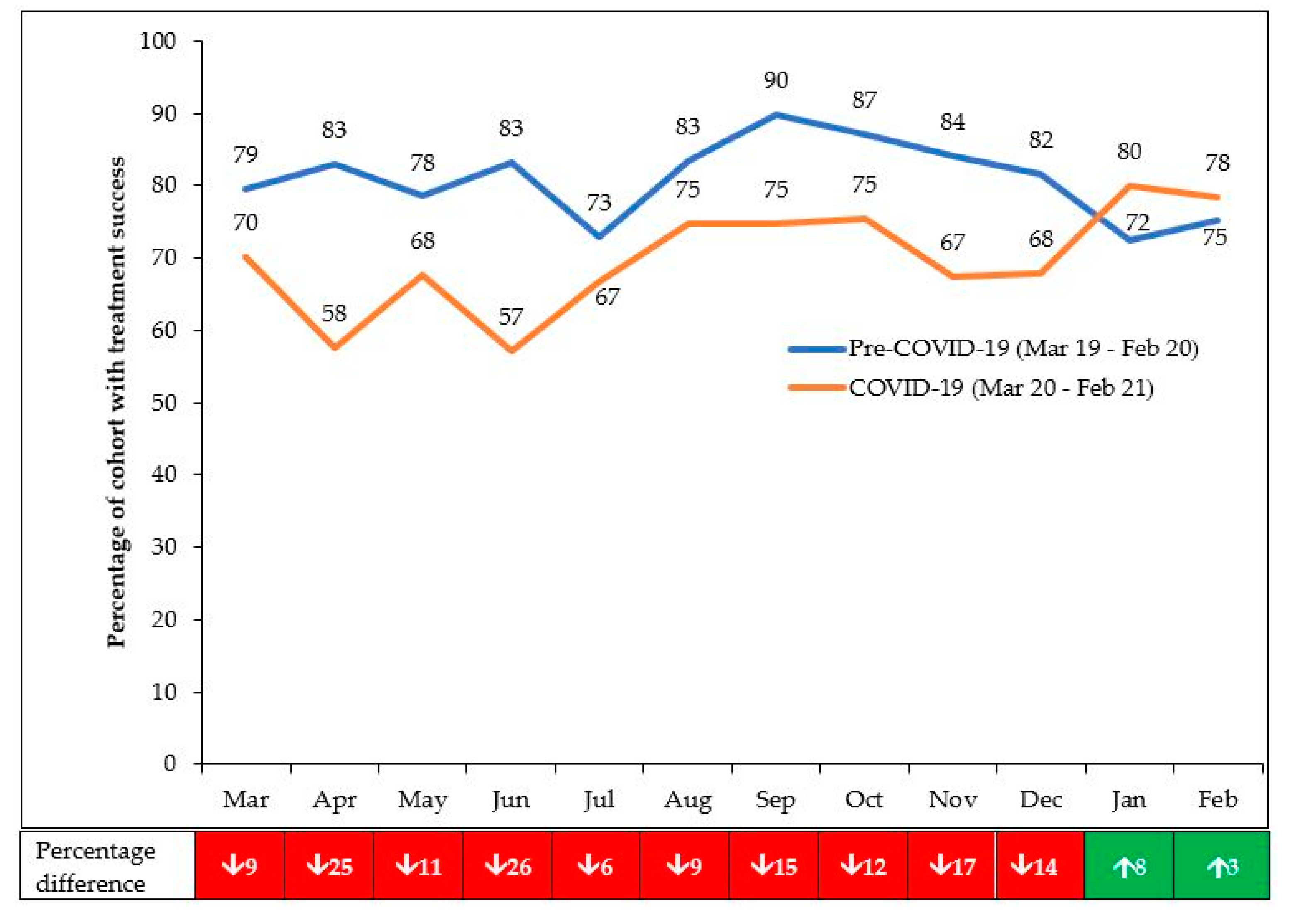
3.3. TB Treatment Outcomes
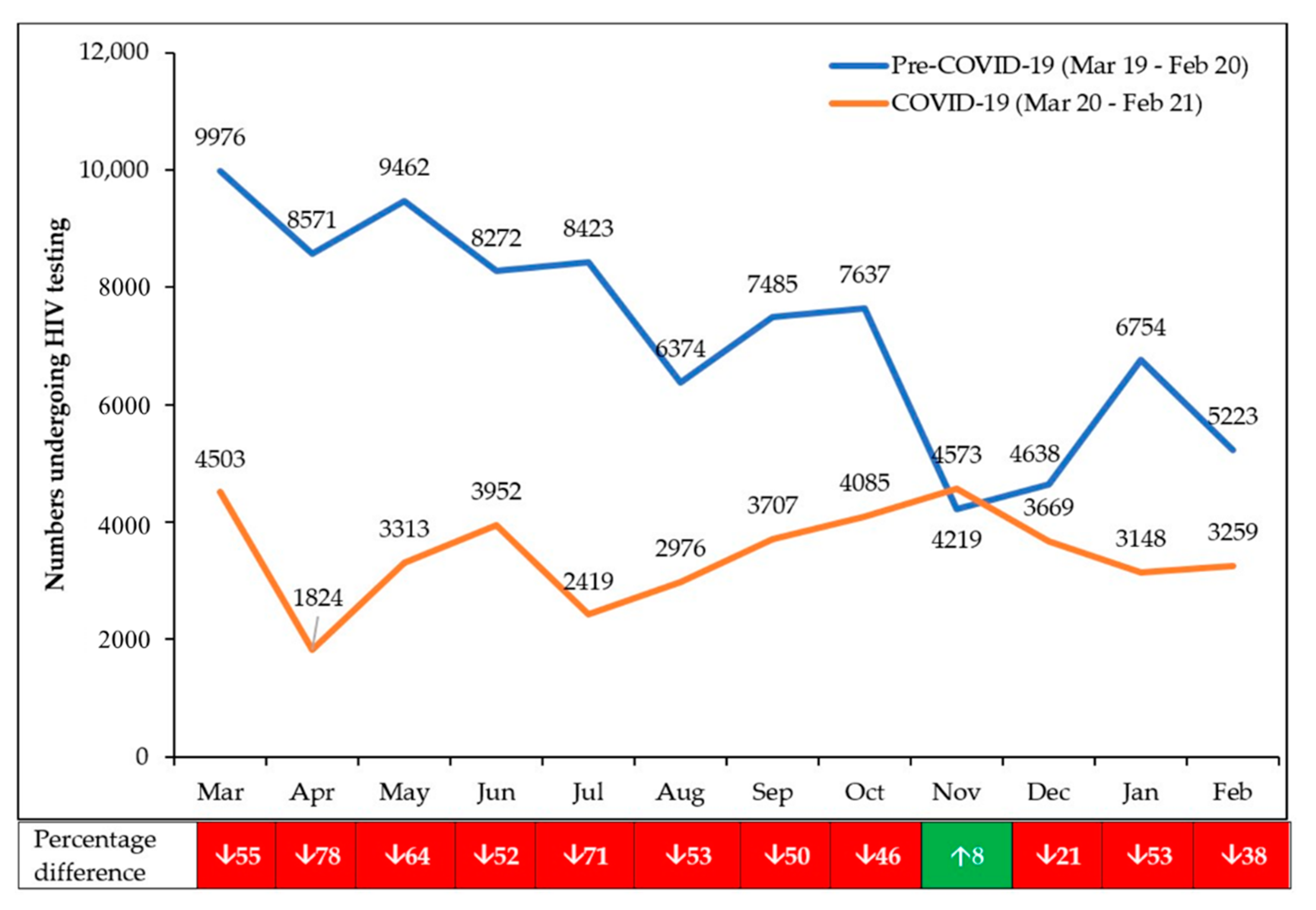
3.4. HIV Testing and Referral to ART
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update 29 December 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 30 March 2021).
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.Y.; D’Ortenzio, E.; Yazdanpanah, Y.; Eholie, S.P.; Altmann, M.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Nkengasong, J.N.; Mankoula, W. Looming threat of COVID-19 infection in Africa: Act collectively, and fast. Lancet 2020, 395, 841–842. [Google Scholar] [CrossRef] [Green Version]
- Pang, Y.; Liu, Y.; Du, J.; Gao, J.; Li, L. Impact of COVID-19 on tuberculosis control in China. Int. J. Tuberc. Lung Dis. 2020, 24, 545–547. [Google Scholar] [CrossRef]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, 1132–1141. [Google Scholar] [CrossRef]
- Bah, O.M.; Kamara, H.B.; Bhat, P.; Harries, A.D.; Owiti, P.; Katta, J.; Foray, L.; Kamara, M.I.; Kamara, B.O. The influence of the Ebola outbreak on presumptive and active tuberculosis in Bombali District, Sierra Leone. Public Health Action 2017, 7, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konwloh, P.K.; Cambell, C.L.; Ade, S.; Bhat, P.; Harries, A.D.; Wilkinson, E.; Cooper, C.T. Influence of Ebola on tuberculosis case finding and treatment outcomes in Liberia. Public Health Action 2017, 7, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Gamanga, A.H.; Owiti, P.; Bhat, P.; Harries, A.D.; Kargbo-Labour, I.; Koroma, M. The Ebola outbreak: Effects on HIV reporting, testing and care in Bonthe district, rural Sierra Leone. Public Health Action 2017, 7, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, G.P.; Bhat, P.; Owiti, P.; Edwards, J.K.; Tweya, H.; Najjemba, R. Did the 2014 Ebola outbreak in Liberia affect HIV testing, linkage to care and ART initiation? Public Health Action 2017, 7, 70–75. [Google Scholar] [CrossRef] [Green Version]
- Stop TB Partnership. TB and COVID-19. Available online: http://www.stoptb.org/covid19.asp?utm_source=The+Stop+TB+Pa (accessed on 30 March 2021).
- World Health Organization. World Health Organization (WHO) Information Note Tuberculosis and COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- UNAIDS. Covid-19 and HIV. Available online: https://www.unaids.org/en/covid19 (accessed on 30 March 2021).
- Chiang, C.Y.; Sony, A.E. Tackling the threat of COVID-19 in Africa: An urgent need for practical planning. Int. J. Tuberc. Lung Dis. 2020, 24, 541–542. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—86; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sandy, C.; Takarinda, K.C.; Timire, C.; Mutunzi, H.; Dube, M.; Dlodlo, R.A.; Harries, A.D. Preparing national tuberculosis control programmes for COVID-19. Int. J. Tuberc. Lung Dis. 2020, 24, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Ortuno-Gutierrez, N.; Zachariah, R.; Woldeyohannes, D.; Bangoura, A.; Chérif, G.-F.; Loua, F.; Hermans, V.; Tayler-Smith, K.; Sikhondze, W.; Camara, L.-M. Upholding Tuberculosis services during the 2014 Ebola storm: An encouraging experience from Conakry, Guinea. PLoS ONE 2016, 11, e0157296. [Google Scholar] [CrossRef]
- Zimbabwe National Statistics Agency. Zimbabwe Population Census, 2012; Zimbabwe National Statistics Agency: Harare, Zimbabwe, 2013. [Google Scholar]
- The World Bank. Zimbabwe. Available online: https://data.worldbank.org/country/ZW (accessed on 19 April 2021).
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Worldometer. Zimbabwe Population (2021). Available online: https://www.worldometers.info/world-population/zimbabwe-population/ (accessed on 19 April 2021).
- Ministry of Health and Child Care (MOHCC). Zimbabwe TB Guidelines; MOHCC: Harare, Zimbabwe, 2010. [Google Scholar]
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care (2017 Update); World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis; 2013 Revision, Updated December 2014 and January 2020. This document Revises Previous WHO, Standard Reporting Framework for TB. Available online: https://www.who.int/tb/publications/definitions/en/#:~:text=2013 (accessed on 30 March 2021).
- Ministry of Health and Child Care (MOHCC). Operational and Service Delivery Manual for the Prevention, Care and Treatment of HIV in Zimbabwe; MOHCC: Harare, Zimbabwe, 2017. [Google Scholar]
- World Health Organization. Consolidated Guidelines on HIV Testing Services. Available online: https://www.who.int/publications/i/item/978-92-4-155058-1 (accessed on 30 March 2021).
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach, 2nd ed.; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Makoni, M. COVID-19 worsens Zimbabwe’s health crisis. Lancet 2020, 396, 457. [Google Scholar] [CrossRef]
- Kargarpour Kamakoli, M.; Hadifar, S.; Khanipour, S.; Farmanfarmaei, G.; Fateh, A.; Mostafaei, S.; Siadat, S.D.; Vaziri, F. Tuberculosis under the Influence of COVID-19 Lockdowns: Lessons from Tehran, Iran. mSphere 2021, 6, e00076-21. [Google Scholar] [CrossRef] [PubMed]
- Adewole, O.O. Impact of COVID-19 on TB care: Experiences of a treatment centre in Nigeria. Int. J. Tuberc. Lung Dis. 2020, 24, 981–982. [Google Scholar] [CrossRef]
- Wu, Z.; Chen, J.; Xia, Z.; Pan, Q.; Yuan, Z.; Zhang, W.; Shen, X. Impact of the COVID-19 pandemic on the detection of TB in Shanghai, China. Int. J. Tuberc. Lung Dis. 2020, 24, 1122–1124. [Google Scholar] [CrossRef]
- De Souza, C.D.F.; Coutinho, H.S.; Costa, M.M.; Magalhães, M.A.F.M.; Carmo, R.F. Impact of COVID-19 on TB diagnosis in Northeastern Brazil. Int. J. Tuberc. Lung Dis. 2020, 24, 1220–1222. [Google Scholar] [CrossRef] [PubMed]
- Golandaj, J.A. Insight into the COVID-19 led slow-down in TB notifications in India. Indian J. Tuberc. 2021, 68, 142–145. [Google Scholar] [CrossRef]
- Cilloni, L.; Fu, H.; Vesga, J.F.; Dowdy, D.; Pretorius, C.; Ahmedov, S.; Nair, S.A.; Mosneaga, A.; Masini, E.; Sahu, S.; et al. The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis. EClinicalMedicine 2020, 28, 100603. [Google Scholar] [CrossRef] [PubMed]
- Simões, D.; Stengaard, A.R.; Combs, L.; Raben, D. Impact of the COVID-19 pandemic on testing services for HIV, viral hepatitis and sexually transmitted infections in the WHO european region, March to August 2020. Eurosurveillance 2020, 25, 2001943. [Google Scholar] [CrossRef]
- Hill, B.J.; Anderson, B.; Lock, L. COVID-19 pandemic, Pre-Exposure Prophylaxis (PrEP) Care, and HIV/STI testing among patients receiving care in three HIV epidemic priority states. AIDS Behav. 2021, 1, 1–5. [Google Scholar]
- Ponticiello, M.; Mwanga-Amumpaire, J.; Tushemereirwe, P.; Nuwagaba, G.; King, R.; Sundararajan, R. “Everything is a Mess”: How COVID-19 is impacting engagement with HIV testing services in rural southwestern uganda. AIDS Behav. 2020, 24, 3006–3009. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Mwamba, C.; Kerkhoff, A.D.; Kagujje, M.; Lungu, P.; Muyoyeta, M.; Sharma, A. Diagnosed with TB in the era of COVID-19: Patient perspectives in Zambia. Public Health Action 2021, 10, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, H.; Luo, G.; Meng, X.; Guo, W.; Fitzpatrick, T.; Ao, Y.; Feng, A.; Liang, B.; Zhan, Y.; et al. Antiretroviral treatment interruption among people living with HIV during COVID-19 outbreak in China: A nationwide cross-sectional study. J. Int. AIDS Soc. 2020, 23, e25637. [Google Scholar] [CrossRef] [PubMed]
- Jewell, B.L.; Smith, J.A.; Hallett, T.B. Understanding the impact of interruptions to HIV services during the COVID-19 pandemic: A modelling study. EClinicalMedicine 2020, 26, 100483. [Google Scholar] [CrossRef]
- Mwananyanda, L.; Gill, C.J.; MacLeod, W.; Kwenda, G.; Pieciak, R.; Mupila, Z.; Lapidot, R.; Mupeta, F.; Forman, L.; Ziko, L.; et al. Covid-19 deaths in Africa: Prospective systematic postmortem surveillance study. BMJ 2021, 372, n334. [Google Scholar] [CrossRef]
- Echeverría, G.; Espinoza, W.; de Waard, J.H. How TB and COVID-19 compare: An opportunity to integrate both control programmes. Int. J. Tuberc. Lung Dis. 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Meneguim, A.C.; Rebello, L.; Das, M.; Ravi, S.; Mathur, T.; Mankar, S.; Kharate, S.; Tipre, P.; Oswal, V.; Iyer, A.; et al. Adapting TB services during the COVID-19 pandemic in Mumbai, India. Int. J. Tuberc. Lung Dis. 2020, 24, 1119–1121. [Google Scholar] [CrossRef] [PubMed]
- Stop TB Partnership. One Year On, New Data Show Global Impact of COVID-19 on TB Epidemic is Worse than Expected. Available online: http://www.stoptb.org/covid19.asp (accessed on 30 March 2021).
- Chiang, C.Y.; Islam, T.; Xu, C.; Chinnayah, T.; Garfin, A.M.C.; Rahevar, K.; Raviglione, M. The impact of COVID-19 and the restoration of tuberculosis services in the Western Pacific Region. Eur. Respir. J. 2020, 56, 2003054. [Google Scholar] [CrossRef]
- Mhango, M.; Chitungo, I.; Dzinamarira, T. COVID-19 lockdowns: Impact on facility-based HIV testing and the case for the scaling up of home-based testing services in sub-saharan africa. AIDS Behav. 2020, 24, 3014–3016. [Google Scholar] [CrossRef]
- Odinga, M.M.; Kuria, S.; Muindi, O.; Mwakazi, P.; Njraini, M.; Melon, M.; Kombo, B.; Kaosa, S.; Kioko, J.; Musimbi, J.; et al. HIV testing amid COVID-19: Community efforts to reach men who have sex with men in three Kenyan counties. Gates Open Res. 2020, 4, 117. [Google Scholar] [CrossRef] [PubMed]
- Lagat, H.; Sharma, M.; Kariithi, E.; Otieno, G.; Katz, D.; Masyuko, S.; Mugambi, M.; Wamuti, B.; Weiner, B.; Farquhar, C. Impact of the COVID-19 pandemic on HIV testing and assisted partner notification services, western kenya. AIDS Behav. 2020, 24, 3010–3013. [Google Scholar] [CrossRef] [PubMed]
- Lurie, N.; Keusch, G.T.; Dzau, V.J. Urgent lessons from COVID 19: Why the world needs a standing, coordinated system and sustainable financing for global research and development. Lancet 2021, 397, 1229–1236. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Numbers of Patients | Pre-COVID-19 Mar 2019–Feb 2020 N | COVID-19 Mar 2020–Feb 2021 N | Difference between Pre-COVID-19 and COVID-19 % |
|---|---|---|---|
| Presumptive pulmonary TB: | 3270 | 1941 | ↓40.6 |
| Adults (≥15 years) | 3013 | 1849 | ↓38.6 |
| Children (<15 years) | 181 | 52 | ↓71.3 |
| Male | 1866 | 1150 | ↓38.4 |
| Female | 1221 | 782 | ↓36.0 |
| Bacteriologically positive | 442 | 309 | ↓30.1 |
| Positivity rate (%) | (13.5%) | (15.9%) | ↑2.4% * |
| Registered TB: | 1078 | 715 | ↓33.7 |
| Bacteriologically confirmed PTB | 528 | 346 | ↓34.5 |
| Clinically diagnosed PTB | 465 | 251 | ↓46.0 |
| Extrapulmonary TB | 136 | 97 | ↓28.7 |
| Eligible for being newly HIV tested | 586 | 423 | ↓27.8 |
| Newly tested for HIV (%) | (95.1%) | (90.3%) | ↓4.8% * |
| Treatment Outcomes in Patients Enrolled for TB Treatment | Pre-COVID-19 Mar 2019–Feb 2020 n | COVID-19 Mar 2020–Feb 2021 n | Difference between Pre-COVID-19 and COVID-19 % |
|---|---|---|---|
| Enrolled for treatment: | 1210 | 979 | |
| Treatment success (%) | (80.9) | (69.3) | ↓11.6 * |
| Lost to follow-up (%) | (2.0) | (2.3) | ↑0.3 * |
| Died (%) | (4.3) | (3.7) | ↓0.6 * |
| Failed (%) | (0.6) | (0.4) | ↓0.2 * |
| Not evaluated (%) | (12.2) | (24.3) | ↑12.1 * |
| Characteristics | Pre-COVID-19 Mar 2019–Feb 2020 n | COVID-19 Mar 2020–Feb 2021 N | Difference between Pre-COVID-19 and COVID-19 % |
|---|---|---|---|
| Underwent HIV testing at a health facility: | 51,078 | 18,987 | ↓62.8 |
| Adults (≥15 years) | 48,661 | 18,289 | ↓62.4 |
| Children (<15 years) | 2316 | 691 | ↓70.2 |
| Male | 18,278 | 3816 | ↓79.1 |
| Female | 32,706 | 15,171 | ↓53.6 |
| Positive for HIV | 3045 | 1547 | ↓36.7 |
| HIV positivity rate (%) | (6.0%) | (8.1%) | ↑2.1 * |
| Referred to ART (%) | (95.7%) | (91.7%) | ↓4.0 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thekkur, P.; Takarinda, K.C.; Timire, C.; Sandy, C.; Apollo, T.; Kumar, A.M.V.; Satyanarayana, S.; Shewade, H.D.; Khogali, M.; Zachariah, R.; et al. Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe. Trop. Med. Infect. Dis. 2021, 6, 94. https://doi.org/10.3390/tropicalmed6020094
Thekkur P, Takarinda KC, Timire C, Sandy C, Apollo T, Kumar AMV, Satyanarayana S, Shewade HD, Khogali M, Zachariah R, et al. Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe. Tropical Medicine and Infectious Disease. 2021; 6(2):94. https://doi.org/10.3390/tropicalmed6020094
Chicago/Turabian StyleThekkur, Pruthu, Kudakwashe C. Takarinda, Collins Timire, Charles Sandy, Tsitsi Apollo, Ajay M. V. Kumar, Srinath Satyanarayana, Hemant D. Shewade, Mohammed Khogali, Rony Zachariah, and et al. 2021. "Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe" Tropical Medicine and Infectious Disease 6, no. 2: 94. https://doi.org/10.3390/tropicalmed6020094