
Seroprevalence and Clinical Features of Scrub Typhus among Febrile Patients Attending a Referral Hospital in Kathmandu, Nepal

 ,
, 
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Sample Size
2.2. Sample and Clinical Data Collection
2.3. Sample Processing
2.4. Biochemical Test
2.5. Hematological Test
2.6. Preparation of Thin Smear
2.7. Serological Test
2.8. Data Analysis
2.9. Ethical Statement
3. Results
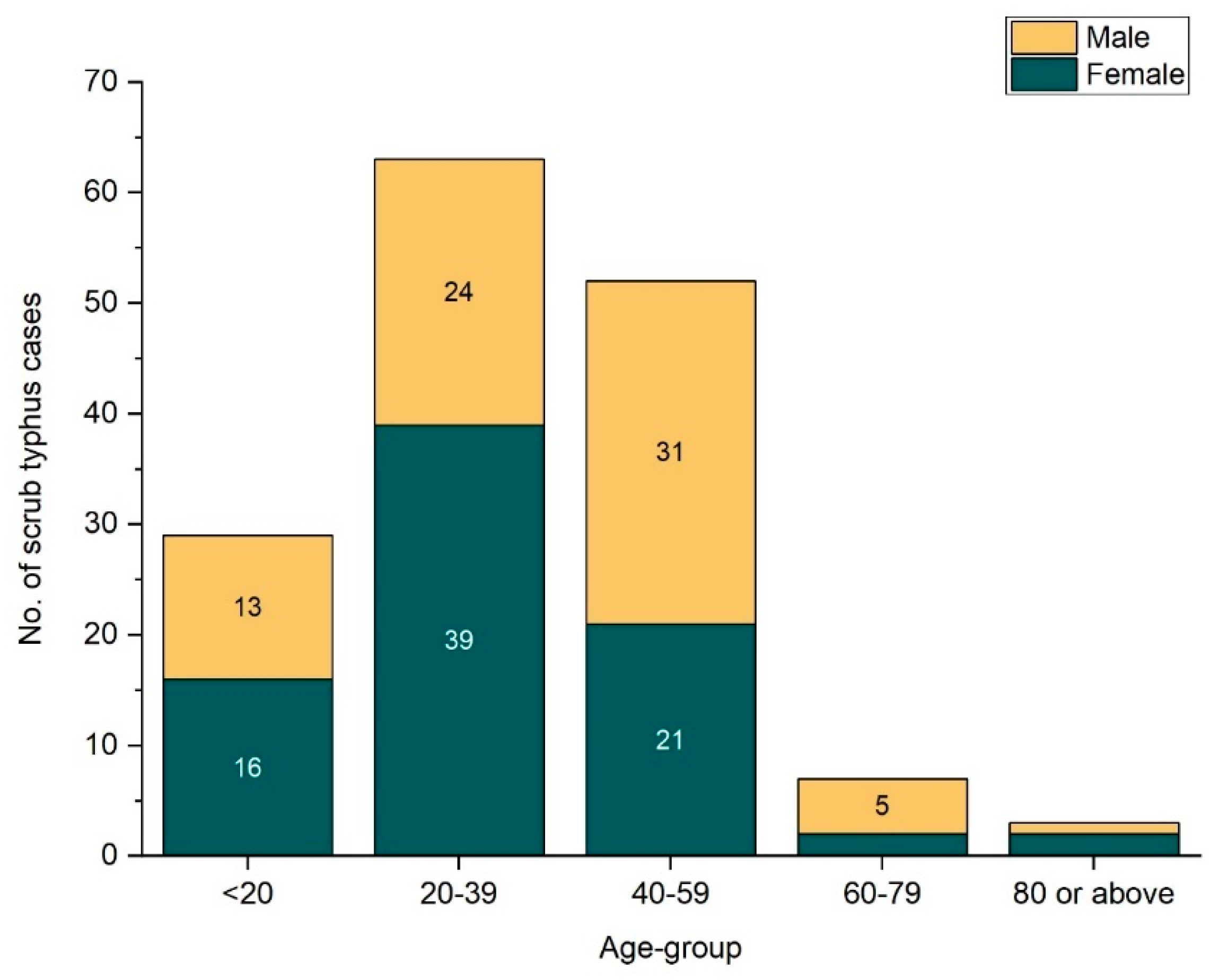
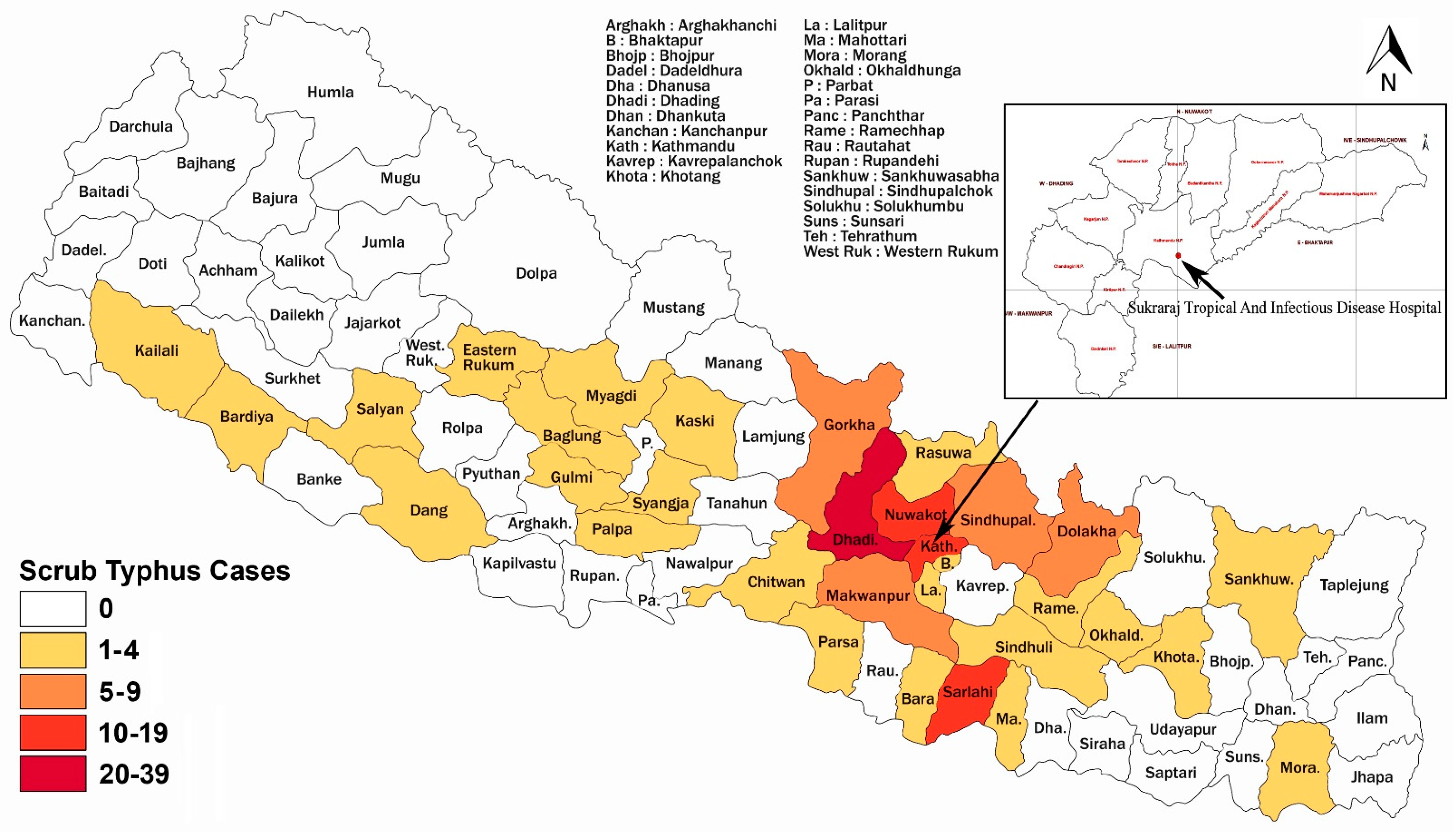
3.1. Demographic and Geographic Distribution of Patients
3.2. Biochemical and Hematological Investigations
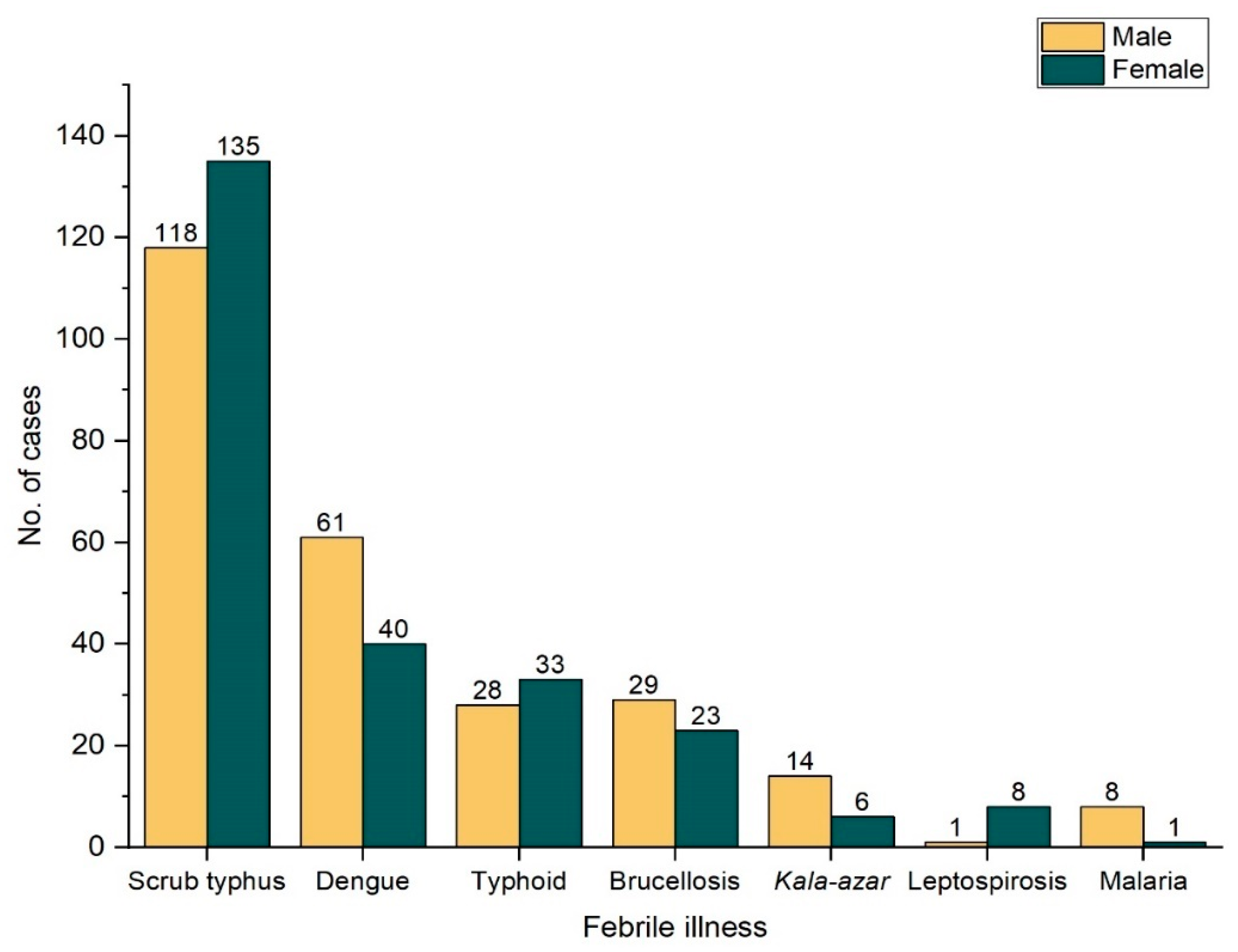
3.3. Different Febrile Illnesses and Mixed Seropositivity
3.4. Clinical Features of ST Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALP | Alkaline phosphatase |
| BD | Direct bilirubin |
| BT | Total bilirubin |
| LMIC | Low-and middle-income country |
| PCR | Polymerase chain reaction |
| RDT | Rapid diagnostic test |
| SGOT | Serum glutamic oxaloacetic transaminase |
| SGPT | Serum glutamic pyruvic transaminase |
| TLC | Total leukocyte count |
| UFI | Undifferentiated febrile illness |
| WBC | White blood corpuscle |
References
- Jang, W.-J.; Huh, M.-S.; Park, K.-H.; Choi, M.-S.; Kim, I.-S. Evaluation of an immunoglobulin M capture enzyme-linked immuno-sorbent assay for diagnosis of Orientia tsutsugamushi infection. Clin. Diagn. Lab. Immunol. 2003, 10, 394–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeon, J.J.; Kim, S.; Yeh, D.W.; Jun, W.L.; Kim KIl Sun, H.L. Scrub typhus: Clinical, pathologic, and imaging findings. Radiographics 2007, 27, 161–172. [Google Scholar]
- Manickam, K.; Sunderkumar, S.; Chinnaraj, S.; Sivathanu, S. Massive consolidation: A rare manifestation of paediatric Scrub typhus. BMJ Case Rep. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Paris, D.H.; Dumler, J.S. State of the art of diagnosis of rickettsial diseases: The use of blood specimens for diagnosis of scrub typhus, spotted fever group rickettsiosis, and murine typhus. Curr. Opin. Infect. Dis. 2016, 29, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Prakash, J.A.J.; Abraham, O.C.; Mathai, E. Evaluation of tests for serological diagnosis of scrub typhus. Trop. Dr. 2006, 36, 212–213. [Google Scholar] [CrossRef]
- Xu, G.; Walker, D.H.; Jupiter, D.; Melby, P.C.; Arcari, C.M. A review of the global epidemiology of scrub typhus. PLOS Neglected Trop. Dis. 2017, 11, e0006062. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.; Mutkule, D.; Rao, M.; Venkategowda, P.; Taggu, A. Scrub typhus: Clinical spectrum and outcome. Indian J. Crit. Care Med. 2015, 19, 208. Available online: http://www.ijccm.org/text.asp?2015/19/4/208/154553 (accessed on 11 September 2020).
- Basnyat, B. Typhoid versus typhus fever in post-earthquake Nepal. Lancet Glob. Health 2016, 4, e516–e517. [Google Scholar] [CrossRef] [Green Version]
- Singhsilarak, T.; Leowattana, W.; Looareesuwan, S.; Wongchotigul, V.; Jiang, J.; Richards, A.L.; Watt, G. Short report: Detection of Orientia tsutsugamushi in clinical samples by quantitative real-time polymerase chain reaction. Am. J. Trop. Med. Hyg. 2005, 72, 640–641. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Basnyat, B.; Keenan, A.J.; Dull, P.M.; Archibald, L.K.; Woods, C.W.; Scott, R.M.; Belbase, R.H.; Reller, L.B.; Zimmerman, M.D. The etiology of febrile illness in adults presenting to patan hospital in Kathmandu, Nepal. Am. J. Trop. Med. Hyg. 2004, 70, 670–675. [Google Scholar] [CrossRef]
- Sharma, N.P.; Peacock, S.J.; Phumratanaprapin, W.; Day, N.; White, N.; Pukrittayakamee, S. A hospital-based study of bloodstream infections in febrile patients in Dhulikhel Hospital Kathmandu University Teaching Hospital, Nepal. S. Asian J. Trop. Med. Public Health 2006, 37, 351–356. [Google Scholar]
- Sedhain, A.; Bhattarai, G.R. Renal manifestation in scrub typhus during a major outbreak in central Nepal. Indian J. Nephrol. 2017, 27, 440. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Shirai, A.; Gan, E.; Bernthall, P. Antibodies to typhus in Eastern Nepal. Trans. R. Soc. Trop. Med. Hyg. 1981, 75, 586–587. [Google Scholar] [CrossRef] [PubMed]
- Karki, K.B.; Acharya, B.P.; Dhimal, M.; Aryal, K.K.; Sharma, G.N.; Khanal, P.; Ranabhat, K.; Dumre, S.P.; Jha, A.K. Descriptive Epidemiology of Scrub Typhus in Nepal; Nepal Health Research Council: Kathmandu, Nepal, 2017.
- Zimmerman, M.D.; Murdoch, D.R.; Rozmajzl, P.J.; Basnyat, B.; Woods, C.W.; Richards, A.L.; Belbase, R.H.; Hammer, D.A.; Anderson, T.P.; Reller, L.B. Murine Typhus and Febrile Illness, Nepal. Emerg. Infect. Dis. 2008, 14, 1656–1659. [Google Scholar] [CrossRef]
- Gupta, N.; Chaudhry, R.; Mirdha, B.; Das, B.; Dar, L.; Kabra, S.; Lodha, R.; Dey, A.; Sood, R.; Sreenivas, N.W.A.V. Scrub Typhus and Leptospirosis: The fallacy of Diagnosing with IgM Enzyme Linked Immunosorbant Assay. J. Microb. Biochem. Technol. 2016, 8, 71–75. [Google Scholar] [CrossRef]
- Bhattacharyya, P.; Rapsang, A.G. Scrub typhus. Indian J. Anaesth. 2013, 57, 127–134. [Google Scholar] [CrossRef]
- Cheesbrough, M. District Laboratory Practices in Tropical Countries, 2nd ed.; Cambridge University Press: New Delhi, India, 2006; pp. 320–321. [Google Scholar]
- ImmuneMed. Available online: http://www.immunemed.co.kr/eng/product/product.asp (accessed on 21 September 2020).
- Tulip Diagnostic. Tulip Diagnostic, India. Slide and Tube Test for Detection of Antibodies to Brucella Abortus/Melitensis. Available online: www.tulipgroup.com (accessed on 21 September 2020).
- InBios International, Inc. Kalazar DetectTM Rapid Test for Visceral Leishmaniasis. Available online: https://inbios.com/kalazar-detecttm-rapid-test-for-visceral-leishmaniasis-intl/ (accessed on 21 September 2020).
- Tulip Diagnostics, India. Widal Antigen Set/Antigen for Salide and Tube Tests. Available online: www.tulipgroup.com (accessed on 21 September 2020).
- Rijal, K.R.; Adhikari, B.; Ghimire, P.; Banjara, M.R.; Hanboonkunupakarn, B.; Imwong, M.; Chotivanich, K.; Ceintury, K.P.; Lal, B.K.; Das Thakur, G.; et al. Epidemiology of Plasmodium vivax Malaria Infection in Nepal. Am. J. Trop. Med. Hyg. 2018, 99, 680–687. [Google Scholar] [CrossRef]
- Rijal, K.R.; Adhikari, B.; Ghimire, B.; Dhungel, B.; Pyakurel, U.R.; Shah, P.; Bastola, A.; Lekhak, B.; Banjara, M.R.; Pandey, B.D.; et al. Epidemiology of dengue virus infections in Nepal, 2006–2019. Infect. Dis. Poverty 2021, 10, 1–10. [Google Scholar] [CrossRef]
- Walker, D.H. After malaria is controlled, what’s next? Am. J. Trop. Med. Hyg. 2014, 91, 7–10. [Google Scholar]
- Mayxay, M.; Castonguay-Vanier, J.; Chansamouth, V.; Dubot-Pérès, A.; Paris, D.H.; Phetsouvanh, R.; Tangkhabuanbutra, J.; Douangdala, P.; Inthalath, S.; Souvannasing, P.; et al. Causes of non-malarial fever in Laos: A prospective study. Lancet Glob Health 2013, 1, 46–54. [Google Scholar]
- Gautam, R.; Parajuli, K.; Sherchand, J.B. Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Ne-pal. Trop. Med. Infect. Dis. 2019, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blacksell, S.D.; Sharma, N.P.; Phumratanaprapin, W.; Jenjaroen, K.; Peacock, S.J.; White, N.J.; Pukrittayakamee, S.; Day, N.P. Serological and blood culture investigations of Nepalese fever patients. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 686–690. [Google Scholar] [CrossRef]
- Upadhyaya, B.P.; Shakya, G.; Adhikari, S.; Rijal, N.; Acharya, J.; Maharjan, L.; Marasini, B.R. Scrub Typhus: An Emerging Neglected Tropical Disease in Nepal. J. Nepal Health Res. Counc. 2016, 14, 122–127. [Google Scholar]
- Maude, R.R.; Maude, R.J.; Ghose, A.; Amin, M.R.; Islam, M.B.; Ali, M.; Bari, M.S.; Majumder, M.I.; Tanganuchitcharnchai, A.; Dondorp, A.M.; et al. Serosurveillance of Orientia tsutsugamushi and Rickettsia typhi in Bangladesh. Am. J. Trop. Med. Hyg. 2014, 91, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Chrispal, A.; Boorugu, H.; Chandy, S.; Prakash, J.A.J.; Abraham, O.C.; Thomas, K.; Gopinath, K.G.; Thomas, E.M.; Abraham, A.M. Acute undifferentiated febrile illness in adult hospitalized patients: The disease spectrum and diagnostic predictors—An experience from a tertiary care hospital in South India. Trop. Dr. 2010, 40, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.T.; Mohamed Zan, H.A.; Lim, Y.A.L.; Ngui, R. Antibody Prevalence and Factors Associated with Exposure to Orientia tsutsugamushi in Different Aboriginal Subgroups in West Malaysia. PLoS Negl. Trop. Dis. 2013, 7, e2341. [Google Scholar] [CrossRef] [Green Version]
- Tay, S.T.; Kamalanathan, M.; Rohani, M.Y. Antibody prevalence of Orientia tsutsugamushi, Rickettsia typhi and TT118 spotted fever group rickettsiae among Malaysian blood donors and febrile patients in the urban areas. S. Asian J. Trop. Med. Public Heal. 2003, 34, 165–170. [Google Scholar]
- Neupanae, B.; Rijal, K.R.; Aryal, G.B.; Shah, Y.; Banjara, M.R.; Sherchand, J.B.; Morita, K.; Pandey, B.D. Clinical and laboratory features of dengue fever in southern lowlands of Nepal. Dengue Bulletin 2013, 37, 1–10. [Google Scholar]
- Shrestha, K.L.; Pant, N.D.; Bhandari, R.; Khatri, S.; Shrestha, B.; Lekhak, B. Re-emergence of the susceptibility of the Salmonella spp. isolated from blood samples to conventional first line antibiotics. Antimicrob. Resist. Infect. Control 2016, 5, 22. [Google Scholar] [CrossRef] [Green Version]
- Bhetwal, A.; Maharjan, A.; Khanal, P.R.; Parajuli, N.P. Enteric Fever Caused by Salmonella enterica Serovars with Reduced Susceptibility of Fluoroquinolones at a Community Based Teaching Hospital of Nepal. Int. J. Microbiol. 2017, 2017, 2869458. [Google Scholar] [CrossRef] [Green Version]
- Myat, T.O.; Oo, K.M.; Mone, H.K.; Htike, W.W.; Biswas, A.; Hannaway, R.F.; Murdoch, D.R.; Ussher, J.E.; Crump, J.A. A prospective study of bloodstream infections among febrile adolescents and adults attending Yangon General Hospital, Yangon, Myanmar. PLoS Negl. Trop. Dis. 2020, 14, e0008268. [Google Scholar] [CrossRef] [PubMed]
- Andualem, G.; Abebe, T.; Kebede, N.; Gebre-Selassie, S.; Mihret, A.; Alemayehu, H. A comparative study of Widal test with blood culture in the diagnosis of typhoid fever in febrile patients. BMC Res. Notes 2014, 7, 653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tjernberg, I.; Krüger, G.; Eliasson, I. C6 peptide ELISA test in the serodiagnosis of Lyme borreliosis in Sweden. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 26, 37–42. Available online: https://pubmed.ncbi.nlm.nih.gov/17180348/ (accessed on 22 October 2020). [CrossRef]
- Philipp, M.T.; Bowers, L.C.; Fawcett, P.T.; Jacobs, M.B.; Liang, F.T.; Marques, A.R.; Mitchell, P.D.; Purcell, J.E.; Ratterree, M.S.; Straubinger, R.K. Antibody Response to IR6, a Conserved Immunodominant Region of the VlsE Lipoprotein, Wanes Rapidly after Antibiotic Treatment of Borrelia burgdorferi Infection in Experimental Animals and in Humans. J. Infect. Dis. 2001, 184, 870–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regmi, L.; Pandey, K.; Malla, M.; Khanal, S.; Pandey, B.D. Sero-epidemiology study of leptospirosis in febrile patients from Terai region of Nepal. BMC Infect. Dis. 2017, 17, 628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nepal, H.P.; Gautam, R.; Ansari, S.; Shrestha, S.; Neopane, P. Seroprevalence of brucellosis in clinically suspect-ed patients at a tertiary care center of central Nepal. Eur. J. Biomed Pharm. Sci. 2016, 3, 6. [Google Scholar]
- Goswami, R.P.; Bairagi, B.; Kundu, P.K. K39 strip test--easy, reliable and cost-effective field diagnosis for visceral leishmaniasis in India. J. Assoc. Physicians India 2003, 51, 759–761. [Google Scholar]
- Raina, S.; Raina, R.K.; Agarwala, N.; Raina, S.K.; Sharma, R. Coinfections as an aetiology of acute undifferentiated febrile illness among adult patients in the sub-Himalayan region of north India. J. Vector Borne Dis. 2018, 55, 130–136. Available online: https://pubmed.ncbi.nlm.nih.gov/30280711/ (accessed on 1 September 2020). [CrossRef]
- Kweon, S.-S.; Choi, J.-S.; Lim, H.-S.; Kim, J.-R.; Kim, K.-Y.; Ryu, S.-Y.; Yoo, H.-S.; Park, O. Rapid increase of scrub typhus, South Korea, 2001–2006. Emerg. Infect Dis. 2009, 15, 1127. [Google Scholar] [CrossRef]
- Park, J.-H.; Kim, S.-J.; Youn, S.-K.; Park, K.; Gwack, J. Epidemiology of Scrub Typhus and the Eschars Patterns in South Korea from 2008 to 2012. Jpn. J. Infect. Dis. 2014, 67, 458–463. Available online: https://pubmed.ncbi.nlm.nih.gov/25410561/ (accessed on 31 August 2020). [CrossRef]
- Pokharel, S.; Basnyat, B.; Arjyal, A.; Mahat, S.P.; Kc, R.K.; Bhuju, A.; Poudyal, B.; Kestelyn, E.; Shrestha, R.; Phuong, D.N.T.; et al. Co-trimoxazole versus azithromycin for the treatment of undifferentiated febrile illness in Nepal: Study protocol for a randomized controlled trial. Trials 2017, 18, 450. Available online: http://trialsjournal.biomedcentral.com/articles/10.1186/s13063-017-2199-6 (accessed on 1 September 2020). [CrossRef] [PubMed] [Green Version]
- Kaljee, L.M.; Pach, A.; Garrett, D.; Bajracharya, D.; Karki, K.; Khan, I. Social and Economic Burden Associated With Typhoid Fever in Kathmandu and Surrounding Areas: A Qualitative Study. J. Infect. Dis. 2017, 218, S243–S249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajapakse, S.; Weeratunga, P.; Sivayoganathan, S.; Fernando, S.D. Clinical manifestations of scrub typhus. Trans. R. Soc. Trop. Med. Hyg. 2017, 111, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Epidemiology and Disease Control Division (EDCD). EDCD Interim Guideline on Prevention and Control of Scrub Typhus September 2015. Updated in August 2016. 2016. Available online: https://www.edcd.gov.np/resources/download/scrub-typhus-guideline-on-prevention-and-control (accessed on 11 October 2020).
- Tsay, R.W.; Chang, F.Y. Serious complications in scrub typhus. J. Microbiol. Immunol. Infect. 1998, 31, 240–244. [Google Scholar]
- Pradeepan, J.A.; Ketheesan, N.; Murugananthan, K. Emerging scrub typhus infection in the northern region of Sri Lanka. BMC Res. Notes 2014, 7, 719. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Biswal, M.; Kumar, A.; Zaman, K.; Jain, S.; Bhalla, A. Scrub Typhus in a Tertiary Care Hospital in North India. Am. J. Trop. Med. Hyg. 2016, 95, 447–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anitharaj, V.; Stephen, S.; Pradeep, J.; Park, S.; Kim, S.-H.; Kim, Y.J.; Kim, E.-Y.; Kim, Y.-W. Serological Diagnosis of Acute Scrub Typhus in Southern India: Evaluation of InBios Scrub Typhus Detect IgM Rapid Test and Comparison with other Serological Tests. J. Clin. Diagn. Res. 2016, 10, DC07–DC10. [Google Scholar] [CrossRef]
- Sirisanthana, V.; Puthanakit, T.; Sirisanthana, T. Epidemiologic, clinical and laboratory features of scrub typhus in thirty Thai children. Pediatr. Infect. Dis. J. 2003, 22, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-X.; Feng, D.; Suo, J.-J.; Xing, Y.-B.; Liu, G.; Liu, L.-H.; Xiao, H.-J.; Jia, N.; Gao, Y.; Yang, H.; et al. Clinical characteristics of the autumn-winter type scrub typhus cases in south of Shandong province, northern China. BMC Infect. Dis. 2009, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, M.; Kaiho, I.; Ito, T.; Nemoto, H.; Hagiwara, T.; Kishimoto, T.; Shiga, S.; Yamamoto, N.; Yoshida, Y.; Masukawa, K.; et al. Scrub typhus in Japan: Epidemiology and clinical features of cases reported in 1998. Am. J. Trop. Med. Hyg. 2002, 67, 162–165. [Google Scholar] [CrossRef] [Green Version]
- Mathai, E.; Rolain, J.M.; Verghese, G.M.; Abraham, O.C.; Mathai, D.; Mathai, M.; Raoult, D. Outbreak of Scrub Typhus in Southern India during the Cooler Months. Ann. N. Y. Acad. Sci. 2003, 990, 359–364. [Google Scholar] [CrossRef]
- Sharma, A.; Mahajan, S.; Gupta, M.L.; Kanga, A.; Sharma, V. Investigation of an outbreak of scrub typhus in the himalayan region of India. Jpn. J. Infect. Dis. 2005, 58, 208–210. [Google Scholar] [PubMed]
- Hu, M.-L.; Liu, J.-W.; Wu, K.-L.; Lu, S.-N.; Chiou, S.-S.; Kuo, C.-H.; Chuah, S.-K.; Wang, J.-H.; Hu, T.-H.; Chiu, K.-W.; et al. Short report: Abnormal liver function in scrub typhus. Am. J. Trop. Med. Hyg. 2005, 73, 667–668. [Google Scholar] [CrossRef] [PubMed]
- Silpapojakul, K.; Varachit, B.; Silpapojakul, K. Paediatric scrub typhus in Thailand: A study of 73 confirmed cases. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 354–359. [Google Scholar] [CrossRef]
- Varghese, G.M.; Janardhanan, J.; Trowbridge, P.; Peter, J.V.; Prakash, J.A.; Sathyendra, S.; Thomas, K.; David, T.S.; Kavitha, M.; Abraham, O.C.; et al. Scrub typhus in South India: Clinical and laboratory manifestations, genetic variability, and outcome. Int. J. Infect. Dis. 2013, 17, e981–e987. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, S.; Sarma, N. Scrub Typhus: An Emerging Threat. Indian J. Dermatol. 2017, 62, 478–485. Available online: /pmc/articles/PMC5618834/?report=abstract (accessed on 22 December 2020). [PubMed]
- Mahajan, S.K.; Rolain, J.-M.; Kashyap, R.; Bakshi, D.; Sharma, V.; Prasher, B.S.; Pal, L.S.; Raoult, D. Scrub Typhus in Himalayas. Emerg. Infect. Dis. 2006, 12, 1590–1592. [Google Scholar] [CrossRef]
- Silpapojakul, K. Scrub typhus in the Western Pacific region. Ann. Acad. Med. Singap. 1997, 26, 794–800. [Google Scholar]
- Kang, J.-I.; Kim, D.-M.; Lee, J. Acute sensorineural hearing loss and severe otalgia due to scrub typhus. BMC Infect. Dis. 2009, 9, 173. [Google Scholar] [CrossRef] [Green Version]
- Stephen, S.; Kim, S.-H.; Pradeep, J.; Kim, Y.J.; Kim, E.-Y.; Park, S.; Kim, M.-W.; Kim, Y.-W. Evaluation of ImmuneMed scrub typhus rapid test kit, for diagnosis of scrub typhus. J. Vector Borne Dis. 2016, 53, 283–287. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Test Kit Used (S1%, S2%) | Manufacturer |
|---|---|---|
| Scrub typhus | ImmuneMed Scrub typhus Rapid (97.3%, 99.5%) | ImmuneMed Inc., Songpa-gu, Korea [19]) |
| Dengue | ImmuneMed Dengue combo (NS1: 97.7%, 99.5%; IgM & IgG: 98.5%, 92.3%) | ImmuneMed Inc., Songpa-gu, Korea [19] |
| Leptospirosis | ImmuneMed leptospira Rapid (96.4%, 98.4%) | ImmuneMed Inc., Songpa-gu, Korea [19] |
| Brucellosis | Brucel® antigen solution ‘A’ and solution ‘B’ (70%, 70%) | Tulip Diagnostics, Goa, India [20] |
| Kala-azar | Kalazar DetectTM (>90%, >90%) | InBios International Inc., Songpa-gu, USA [21] |
| Enteric fever | TYDAL® (Widal test) (70%, 70%) | Tulip Diagnostics, Goa, India [22] |
| A: Distribution of Total Febrile Patients Based on Age-Group (n = 2070) | |||
| Age Category | Frequency | Total | |
| Male N (%) | Female N (%) | ||
| <20 | 196 (16.5) | 138 (15.7) | 334 (16.14) |
| 20–39 | 493 (41.4) | 359 (40.8) | 852 (41.15) |
| 40–59 | 347 (29.1) | 266 (30.3) | 613 (29.61) |
| 60–79 | 136 (11.4) | 108 (12.3) | 244 (11.79) |
| 80 or above | 19 (1.6) | 8 (0.9) | 27 (1.31) |
| Total | 1191 (57.5) | 879 (42.5) | 2070 (100) |
| B: Distribution of ST Patients Using Antibiotics before the Hospital Visit (n = 95) | |||
| Age group | Frequencies, n (%) | ||
| Less than 20 | 15 (15.8) | ||
| 20–39 | 42 (44.2) | ||
| 40–59 | 30 (31.6) | ||
| 60–79 | 6 (6.3) | ||
| 80 and above | 2 (2.1) | ||
| Total | 95 (100) | ||
| C: Biochemical and Hematological Findings of ST Patients (n = 139) | |||
| Parameters * | Frequencies, n (%) | ||
| WBC count | |||
| Low | 11 (7.9) | ||
| High | 3 (2.2) | ||
| Thrombocytopenia | 77 (55.4) | ||
| Raised ALP | 44 (31.7) | ||
| Raised SGPT | 53 (38.1) | ||
| Raised SGOT | 85 (61.2) | ||
| Raised BT | 9 (6.5) | ||
| Raised BD | 13 (9.4) | ||
| Raised serum creatinine | 14 (10.1) | ||
| Febrile Illness(es) | Frequency (% of Total Febrile Patients) |
|---|---|
| ST + | 221 (10.7) |
| DEN + | 81 (3.9) |
| LEP + | 3 (0.1) |
| BRU + | 39 (1.9) |
| MAL + | 7 (0.3) |
| KAL + | 18 (0.9) |
| TYP + | 52 (2.5) |
| ST + DEN + | 12 (0.6) |
| ST + LEP + | 2 (0.1) |
| ST + BRU + | 9 (0.4) |
| ST + MAL + | 1 (0.0*) |
| ST + KAL + | 1 (0.0*) |
| ST + TYP + | 5 (0.2) |
| DEN + LEP + | 2 (0.1) |
| DEN + BRU + | 1 (0.0*) |
| DEN + MAL + | 1 (0.0*) |
| DEN + TYP + | 2 (0.1) |
| BRU + KAL + | 1 (0.0*) |
| BRU + TYP + | 2 (0.1) |
| ST + DEN + LEP + | 2 (0.1) |
| Total | 462 (22.3) |
| Presented Signs and Symptoms | Value | p-Value (χ2) |
|---|---|---|
| Fever, n (%) | 154 (100) | |
| Duration of fever before hospital visit (days), mean ± SD (Range) | 9.34 ± 4.84 days (1–30) | |
| Headache, n (%) | 122 (79.2) | <0.01 |
| Sweating, n (%) | 108 (70.1) | <0.01 |
| Difficulty in breathing, n (%) | 79 (51.3) | <0.01 |
| Redness of eyes, n (%) | 67 (43.5) | <0.01 |
| Rashes, n (%) | 15 (9.7) | |
| Eschar, n (%) | 14 (9.1) | |
| Diarrhea, n (%) | 5 (3.2) | |
| Tinnitus, n (%) | 3 (1.9) | |
| Lymphadenopathy, n (%) | 3 (1.9) | |
| Splenomegaly, n (%) | 1 (0.6) | |
| Hepatomegaly, n (%) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pokhrel, A.; Rayamajhee, B.; Khadka, S.; Thapa, S.; Kapali, S.; Pun, S.B.; Banjara, M.R.; Joshi, P.; Lekhak, B.; Rijal, K.R. Seroprevalence and Clinical Features of Scrub Typhus among Febrile Patients Attending a Referral Hospital in Kathmandu, Nepal. Trop. Med. Infect. Dis. 2021, 6, 78. https://doi.org/10.3390/tropicalmed6020078
Pokhrel A, Rayamajhee B, Khadka S, Thapa S, Kapali S, Pun SB, Banjara MR, Joshi P, Lekhak B, Rijal KR. Seroprevalence and Clinical Features of Scrub Typhus among Febrile Patients Attending a Referral Hospital in Kathmandu, Nepal. Tropical Medicine and Infectious Disease. 2021; 6(2):78. https://doi.org/10.3390/tropicalmed6020078
Chicago/Turabian StylePokhrel, Anil, Binod Rayamajhee, Saroj Khadka, Sandeep Thapa, Samjhana Kapali, Sher Bahadur Pun, Megha Raj Banjara, Prakash Joshi, Binod Lekhak, and Komal Raj Rijal. 2021. "Seroprevalence and Clinical Features of Scrub Typhus among Febrile Patients Attending a Referral Hospital in Kathmandu, Nepal" Tropical Medicine and Infectious Disease 6, no. 2: 78. https://doi.org/10.3390/tropicalmed6020078