Contribution of Single-Fiber Evaluation on Monitoring Outcomes Following Injection of Botulinum Toxin-A: A Narrative Review of the Literature


Abstract
:1. Introduction
2. Results
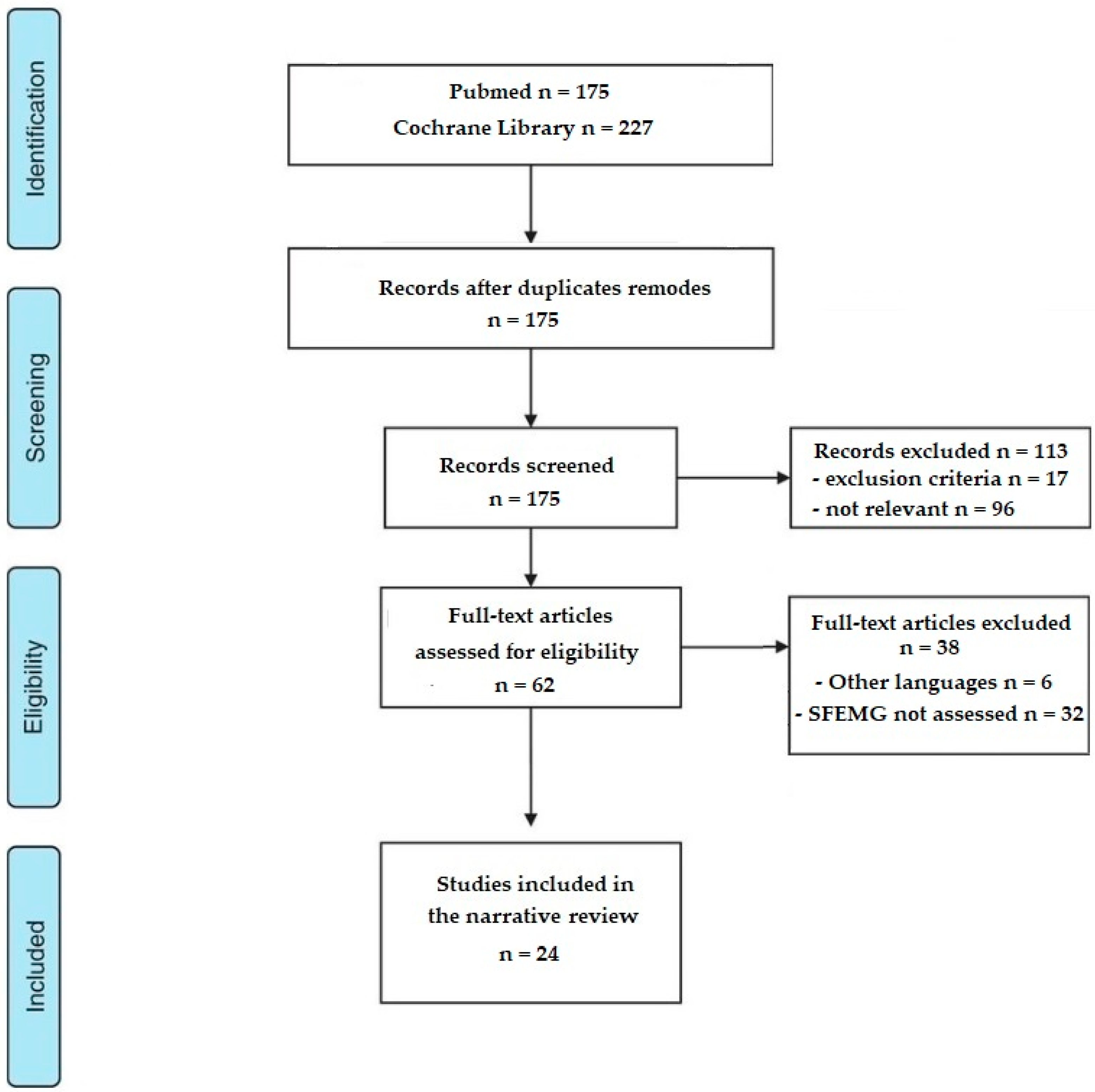
2.1. Selection of the Studies
2.2. Literature Analysis
2.2.1. Local Effects of BoNT-A
2.2.2. Distant Effects of BoNT-A
2.2.3. Clinical Correlation and Jitter
2.2.4. Dose-Effect Relationship
2.2.5. Outliers
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Identification of Studies
5.2. Study Selection
5.3. Eligibility Criteria
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duarte, G.S.; Rodrigues, F.B.; Marques, R.E.; Castelão, M.; Ferreira, J.; Sampaio, C.; Moore, A.P.; Costa, J. Botulinum toxin type A therapy for blepharospasm. Cochrane Database Syst. Rev. 2020, 11, CD004900. [Google Scholar]
- Jankovic, J.; Schwartz, K.; Donovan, D.T. Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, other focal dystonias and hemifacial spasm. J. Neurol. Neurosurg. Psychiatry 1990, 53, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, F.B.; Duarte, G.S.; Marques, R.E.; Castelão, M.; Ferreira, J.; Sampaio, C.; Moore, A.P.; Costa, J. Botulinum toxin type A therapy for cervical dystonia. Cochrane Database Syst. Rev. 2020, 11, CD003633. [Google Scholar] [PubMed]
- Elovic, E.P.; Brashear, A.; Kaelin, D.; Liu, J.; Millis, S.R.; Barron, R.; Turkel, C. Repeated treatments with botulinum toxin type a produce sustained decreases in the limitations associated with focal upper-limb poststroke spasticity for caregivers and patients. Arch. Phys. Med. Rehabil. 2008, 89, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A.; Novak, I.; Sheean, G.; Singer, B.J.; Ward, A.B. International consensus statement for the use of botulinum toxin treatment in adults and children with neurological impairments--introduction. Eur. J. Neurol. 2010, 17 (Suppl. 2), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D.M.; Hallett, M.; Ashman, E.J.; Comella, C.L.; Green, M.W.; Gronseth, G.S.; Armstrong, M.J.; Gloss, D.; Potrebic, S.; Jankovic, J.; et al. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016, 86, 1818–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrich, R.J.; Janis, J.E.; Fagien, S.; Stuzin, J.M. The cosmetic use of botulinum toxin. Plast. Reconstr. Surg. 2003, 112, 177S–88S. [Google Scholar] [CrossRef] [PubMed]
- Ross, B.G.; Fradet, G.; Nedzelski, J.M. Development of a sensitive clinical facial grading system. Otolaryngol. Head Neck Surg. 1996, 114, 380–386. [Google Scholar] [CrossRef]
- Jh, S.; Mn, Y.F.T.; Xl, Z.; Yg, P.; Y, H.; Lb, X.; Lz, P.; Lx, L.; Lj, J. Synkinesis in primary and postparalytic hemifacial spasm: Clinical features and therapeutic outcomes of botulinum toxin A treatment. Toxicon. Off. J. Int. Soc. Toxinology 2020, 184, 122–126. [Google Scholar]
- Guarin, D.L.; Dusseldorp, J.; Hadlock, T.A.; Jowett, N. A Machine Learning Approach for Automated Facial Measurements in Facial Palsy. JAMA Facial Plast. Surg. 2018, 20, 335–337. [Google Scholar] [CrossRef]
- Lindeboom, R.; De Haan, R.; Aramideh, M.; Speelman, J.D. The blepharospasm disability scale: An instrument for the assessment of functional health in blepharospasm. Mov. Disord. 1995, 10, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Casse, G.; Adenis, J.-P.; Sauvage, J.-P.; Robert, P.-Y. Videonystagmography to assess eyelid dynamic disorders. Orbit 2009, 28, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Physiology 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Abolhasani, H.; Ansari, N.N.; Naghdi, S.; Mansouri, K.; Ghotbi, N.; Hasson, S. Comparing the validity of the Modified Modified Ashworth Scale (MMAS) and the Modified Tardieu Scale (MTS) in the assessment of wrist flexor spasticity in patients with stroke: Protocol for a neurophysiological study. BMJ Open 2012, 2, e001394. [Google Scholar] [CrossRef] [Green Version]
- Ansari, N.N.; Naghdi, S.; Moammeri, H.; Jalaie, S. Ashworth Scales are unreliable for the assessment of muscle spasticity. Physiother. Theory Pr. 2006, 22, 119–125. [Google Scholar] [CrossRef]
- Tardieu, G.; Shentoub, S.; Delarue, R. [Research on a technic for measurement of spasticity]. Rev. Neurol. 1954, 91, 143–144. [Google Scholar]
- Morris, S. Ashworth and Tardieu Scales: Their Clinical Relevance For Measuring Spasticity In Adult And Paediatric Neurological Populations. Phys. Rev. 2002, 7, 53–62. [Google Scholar] [CrossRef]
- Patrick, E.; Ada, L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin. Rehabil. 2006, 20, 173–182. [Google Scholar] [CrossRef]
- Alhusaini, A.A.A.; Dean, C.M.; Crosbie, J.; Shepherd, R.B.; Lewis, J. Evaluation of spasticity in children with cerebral palsy using Ashworth and Tardieu Scales compared with laboratory measures. J. Child. Neurol. 2010, 25, 1242–1247. [Google Scholar] [CrossRef]
- Aloraini, S.M.; Gäverth, J.; Yeung, E.; MacKay-Lyons, M. Assessment of spasticity after stroke using clinical measures: A systematic review. Disabil. Rehabil. 2015, 37, 2313–2323. [Google Scholar] [CrossRef]
- Pandyan, A.D.; Johnson, G.R.; Price, C.I.; Curless, R.H.; Barnes, M.P.; Rodgers, H. A review of the properties and limitations of the Ashworth and modified Ashworth Scales as measures of spasticity. Clin. Rehabil. 1999, 13, 373–383. [Google Scholar] [CrossRef]
- Haugh, A.B.; Pandyan, A.D.; Johnson, G.R. A systematic review of the Tardieu Scale for the measurement of spasticity. Disabil. Rehabil. 2006, 28, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Meseguer-Henarejos, A.-B.; Sánchez-Meca, J.; López-Pina, J.-A.; Carles-Hernández, R. Inter- and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2017, 54, 576–590. [Google Scholar] [CrossRef] [PubMed]
- Brashear, A.; Zafonte, R.; Corcoran, M.; Galvez-Jimenez, N.; Gracies, J.-M.; Gordon, M.F.; McAfee, A.; Ruffing, K.; Thompson, B.; Williams, M.; et al. Inter- and intrarater reliability of the Ashworth Scale and the Disabil.ity Assessment Scale in patients with upper-limb poststroke spasticity. Arch. Phys. Med. Rehabil. 2002, 83, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Ansari, N.N.; Naghdi, S.; Arab, T.K.; Jalaie, S. The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: Limb and muscle group effect. NeuroRehabilitation 2008, 23, 231–237. [Google Scholar] [CrossRef]
- Platz, T.; Eickhof, C.; Nuyens, G.; Vuadens, P. Clinical scales for the assessment of spasticity, associated phenomena, and function: A systematic review of the literature. Disabil. Rehabil. 2005, 27, 7–18. [Google Scholar] [CrossRef]
- Sunnerhagen, K.S. Stop using the Ashworth scale for the assessment of spasticity. J. Neurol. Neurosurg. Psychiatry 2010, 81, 2. [Google Scholar] [CrossRef]
- Ghotbi, N.; Nakhostin Ansari, N.; Naghdi, S.; Hasson, S. Measurement of lower-limb muscle spasticity: Intrarater reliability of Modified Modified Ashworth Scale. J. Rehabil. Res. Dev. 2011, 48, 83–88. [Google Scholar] [CrossRef]
- Burridge, J.H.; Wood, D.E.; Hermens, H.J.; Voerman, G.E.; Johnson, G.R.; van Wijck, F.; Platz, T.; Gregoric, M.; Hitchcock, R.; Pandyan, A.D. Theoretical and methodological considerations in the measurement of spasticity. Disabil. Rehabil. 2005, 27, 69–80. [Google Scholar] [CrossRef]
- Lee, H.-M.; Chen, J.-J.J.; Ju, M.-S.; Lin, C.-C.K.; Poon, P.P.W. Validation of portable muscle tone measurement device for quantifying velocity-dependent properties in elbow spasticity. J. Electromyogr. Kinesiol. Off. J. Int. Soc. Electrophysiol. Kinesiol. 2004, 14, 577–589. [Google Scholar] [CrossRef]
- Calota, A.; Feldman, A.G.; Levin, M.F. Spasticity measurement based on tonic stretch reflex threshold in stroke using a portable device. Clin. Neurophysiol. 2008, 119, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, P.G.; Gäverth, J.; Islam, M.; Fagergren, A.; Borg, J.; Forssberg, H. Validation of a new biomechanical model to measure muscle tone in spastic muscles. Neurorehabil. Neural. Repair 2011, 25, 617–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, S.; Gregson, J.; Leathley, M.; Smith, T.; Sharma, A.; Watkins, C. Development and Inter-rater Reliability of an Assessment Tool for Measuring Muscle Tone in People with Hemiplegia after a Stroke. Physiotherapy 1999, 85, 405–409. [Google Scholar] [CrossRef]
- Pomeroy, V.M.; Dean, D.; Sykes, L.; Faragher, E.B.; Yates, M.; Tyrrell, P.J.; Moss, S.; Tallis, R.C. The unreliability of clinical measures of muscle tone: Implications for stroke therapy. Age Ageing 2000, 29, 229–233. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, N.; Kuwabara, T.; Usuda, S. Development and evaluation of a new measure for muscle tone of ankle plantar flexors: The ankle plantar flexors tone scale. Arch. Phys. Med. Rehabil. 2009, 90, 2054–2061. [Google Scholar] [CrossRef]
- Picelli, A.; Tamburin, S.; Cavazza, S.; Scampoli, C.; Manca, M.; Cosma, M.; Berto, G.; Vallies, G.; Roncari, L.; Melotti, C.; et al. Relationship Between Ultrasonographic, Electromyographic, and Clinical Parameters in Adult Stroke Patients With Spastic Equinus: An Observational Study. Arch. Phys. Med. Rehabil. 2014, 95, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Lee, H.J.; Lee, W.H. Intra- and inter-rater reliabilities of measurement of ultrasound imaging for muscle thickness and pennation angle of tibialis anterior muscle in stroke patients. Top. Stroke Rehabil. 2017, 24, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, A.S.; Ertl-Wagner, B.; Britsch, S.; Schröder, J.M.; Nikolin, S.; Weis, J.; Müller-Felber, W.; Koerte, I.; Stehr, M.; Berweck, S.; et al. Muscle biopsy substantiates long-term MRI alterations one year after a single dose of botulinum toxin injected into the lateral gastrocnemius muscle of healthy volunteers. Mov. Disord. 2009, 24, 1494–1503. [Google Scholar] [CrossRef]
- Kesikburun, S.; Yaşar, E.; Adıgüzel, E.; Güzelküçük, Ü.; Alaca, R.; Tan, A.K. Assessment of Spasticity with Sonoelastography Following Stroke: A Feasibility Study. PMR 2015, 7, 1254–1260. [Google Scholar] [CrossRef]
- Eby, S.F.; Zhao, H.; Song, P.; Vareberg, B.J.; Kinnick, R.R.; Greenleaf, J.F.; An, K.-N.; Brown, A.W.; Chen, S. Quantifying spasticity in individual muscles using shear wave elastography. Radiol. Case Rep. 2017, 12, 348–352. [Google Scholar] [CrossRef]
- Wu, C.-H.; Ho, Y.-C.; Hsiao, M.-Y.; Chen, W.-S.; Wang, T.-G. Evaluation of Post-Stroke Spastic Muscle Stiffness Using Shear Wave Ultrasound Elastography. Ultrasound Med. Biol. 2017, 43, 1105–1111. [Google Scholar] [CrossRef]
- Yaşar, E.; Adigüzel, E.; Kesikburun, S.; Yenihayat, I.; Yilmaz, B.; Alaca, R.; Tan, A.K. Assessment of forearm muscle spasticity with sonoelastography in patients with stroke. Br. J. Radiol. 2016, 89, 20160603. [Google Scholar] [CrossRef]
- Voerman, G.E.; Gregoric, M.; Hermens, H.J. Neurophysiological methods for the assessment of spasticity: The Hoffmann reflex, the tendon reflex, and the stretch reflex. Disabil. Rehabil. 2005, 27, 33–68. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Ugawa, Y. [Clinical signs, neurophysiological evaluation, and medication of spasticity--review]. Brain Nerve 2008, 60, 1409–1414. [Google Scholar] [PubMed]
- Phadke, C.P.; Ismail, F.; Boulias, C. Assessing the neurophysiological effects of botulinum toxin treatment for adults with focal limb spasticity: A systematic review. Disabil. Rehabil. 2012, 34, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Girlanda, P.; Quartarone, A.; Sinicropi, S.; Nicolosi, C.; Roberto, M.L.; Picciolo, G.; Macaione, V.; Battaglia, F.; Ruggeri, M.; Messina, C. Botulinum toxin in upper limb spasticity: Study of reciprocal inhibition between forearm muscles. Neuroreport 1997, 8, 3039–3044. [Google Scholar] [CrossRef]
- Panizza, M.; Castagna, M.; di Summa, A.; Saibene, L.; Grioni, G.; Nilsson, J. Functional and clinical changes in upper limb spastic patients treated with botulinum toxin (BTX). Funct. Neurol. 2000, 15, 147–155. [Google Scholar] [PubMed]
- Pauri, F.; Boffa, L.; Cassetta, E.; Pasqualetti, P.; Rossini, P.M. Botulinum toxin type-A treatment in spastic paraparesis: A neurophysiological study. J. Neurol. Sci. 2000, 181, 89–97. [Google Scholar] [CrossRef]
- Frasson, E.; Priori, A.; Ruzzante, B.; Didonè, G.; Bertolasi, L. Nerve stimulation boosts botulinum toxin action in spasticity. Mov. Disord. 2005, 20, 624–629. [Google Scholar] [CrossRef]
- Manca, M.; Merlo, A.; Ferraresi, G.; Cavazza, S.; Marchi, P. Botulinum toxin type A versus phenol. A clinical and neurophysiological study in the treatment of ankle clonus. Eur. J. Phys. Rehabil. Med. 2010, 46, 11–18. [Google Scholar]
- Sanders, D.B.; Stålberg, E.V. AAEM minimonograph #25: Single-fiber electromyography. Muscle Nerve 1996, 19, 1069–1083. [Google Scholar] [PubMed]
- Tanhehco, J.L. Single-fiber electromyography. Phys. Med. Rehabil. Clin. N Am. 2003, 14, 207–229. [Google Scholar] [CrossRef]
- AAEM Quality Assurance Committee; American Association of Electrodiagnostic Medicine. Literature review of the usefulness of repetitive nerve stimulation and single fiber EMG in the electrodiagnostic evaluation of patients with suspected myasthenia gravis or Lambert-Eaton myasthenic syndrome. Muscle Nerve 2001, 24, 1239–1247. [Google Scholar] [CrossRef]
- Padua, L.; Stalberg, E.; LoMonaco, M.; Evoli, A.; Batocchi, A.; Tonali, P. SFEMG in ocular myasthenia gravis diagnosis. Clin. Neurophysiol. 2000, 111, 1203–1207. [Google Scholar] [CrossRef]
- Chiou-Tan, F.Y.; Gilchrist, J.M. Repetitive nerve stimulation and single-fiber electromyography in the evaluation of patients with suspected myasthenia gravis or Lambert-Eaton myasthenic syndrome: Review of recent literature. Muscle Nerve 2015, 52, 455–462. [Google Scholar] [CrossRef]
- Chauplannaz, G.; Vial, C. [Electrodiagnostic assessment of neuromuscular junction disorders]. Rev. Med. Liege 2004, 59 (Suppl. 1), 184–189. [Google Scholar]
- Lin, T.S.; Cheng, K.S. Characterization of the relationship between motor end-plate jitter and the safety factor. Muscle Nerve 1998, 21, 628–636. [Google Scholar] [CrossRef]
- Trontelj, J.V.; Mihelin, M.; Fernandez, J.M.; Stålberg, E. Axonal stimulation for end-plate jitter studies. J. Neurol. Neurosurg. Psychiatry 1986, 49, 677–685. [Google Scholar] [CrossRef] [Green Version]
- Ad Hoc Committee of the AAEM Special Interest Group on Single Fiber EMG; Gilchrist, J.M. Single fiber EMG reference values: A collaborative effort. Muscle Nerve 1992, 15, 151–161. [Google Scholar]
- Lange, D.J. Single fiber electromyography in normal subjects: Reproducibility, variability, and technical considerations. Electromyogr. Clin. Neurophysiol. 1992, 32, 397–402. [Google Scholar]
- Bromberg, M.B.; Scott, D.M.; AD HOC Committee of the AAEM Single Fiber Special Interest Group. Single fiber EMG reference values: Reformatted in tabular form. Muscle Nerve 1994, 17, 820–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balci, K.; Turgut, N.; Nurlu, G. Normal values for single fiber EMG parameters of frontalis muscle in healthy subjects older than 70 years. Clin. Neurophysiol. 2005, 116, 1555–1557. [Google Scholar] [CrossRef] [PubMed]
- Kouyoumdjian, J.A.; Stålberg, E.V. Reference jitter values for concentric needle electrodes in voluntarily activated extensor digitorum communis and orbicularis oculi muscles. Muscle Nerve 2008, 37, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Stålberg, E.V.; Sanders, D.B. Jitter recordings with concentric needle electrodes. Muscle Nerve 2009, 40, 331–339. [Google Scholar] [CrossRef]
- Stålberg, E.; Sanders, D.B.; Ali, S.; Cooray, G.; Leonardis, L.; Löseth, S.; Machado, F.; Maldonado, A.; Martinez-Aparicio, C.; Sandberg, A.; et al. Reference values for jitter recorded by concentric needle electrodes in healthy controls: A multicenter study. Muscle Nerve 2016, 53, 351–362. [Google Scholar] [CrossRef]
- Sanders, D.B.; Arimura, K.; Cui, L.; Ertaş, M.; Farrugia, M.E.; Gilchrist, J.; Kouyoumdjian, J.A.; Padua, L.; Pitt, M.; Stålberg, E. Guidelines for single fiber EMG. Clin. Neurophysiol. 2019, 130, 1417–1439. [Google Scholar] [CrossRef] [PubMed]
- Tamburin, S.; Zanette, G. A case of oligosymptomatic botulism. The role of single-fiber EMG in early diagnosis. J. Peripher. Nerv. Syst. 2004, 9, 130–131. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Garner, C.G.; Witt, T.N. Complete bilateral internal ophthalmoplegia as sole clinical sign of botulism: Confirmation of diagnosis by single fibre electromyography. J. Neurol. 1989, 236, 243–245. [Google Scholar] [CrossRef]
- Schiller, H.H.; Stålberg, E. Human botulism studied with single-fiber electromyography. Arch. Neurol. 1978, 35, 346–349. [Google Scholar] [CrossRef]
- Padua, L.; Aprile, I.; Monaco, M.L.; Fenicia, L.; Anniballi, F.; Pauri, F.; Tonali, P. Neurophysiological assessment in the diagnosis of botulism: Usefulness of single-fiber EMG. Muscle Nerve 1999, 22, 1388–1392. [Google Scholar] [CrossRef]
- Girlanda, P.; Dattola, R.; Messina, C. Single fibre EMG in 6 cases of botulism. Acta Neurol. Scand 1983, 67, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Monaco, S.; Freddi, N.; Francavilla, E.; Meneghetti, F.; Fenicia, L.; Franciosa, G.; Cadrobbi, P. Transient tonic pupils in botulism type B. J. Neurol. Sci. 1998, 156, 96–98. [Google Scholar] [CrossRef]
- Chaudhry, V.; Crawford, T.O. Stimulation single-fiber EMG in infant botulism. Muscle Nerve 1999, 22, 1698–1703. [Google Scholar] [CrossRef]
- Mandler, R.N.; Maselli, R.A. Stimulated single-fiber electromyography in wound botulism. Muscle Nerve 1996, 19, 1171–1173. [Google Scholar] [CrossRef]
- Cherington, M. Clinical spectrum of botulism. Muscle Nerve 1998, 21, 701–710. [Google Scholar] [CrossRef]
- Keesey, J.C. AAEE Minimonograph #33: Electrodiagnostic approach to defects of neuromuscular transmission. Muscle Nerve 1989, 12, 613–626. [Google Scholar]
- Sanders, D.B. Clinical impact of single-fiber electromyography. Muscle Nerve Suppl. 2002, 11, S15–S20. [Google Scholar] [CrossRef]
- Comella, C.L.; Pullman, S.L. Botulinum toxins in neurological disease. Muscle Nerve 2004, 29, 628–644. [Google Scholar] [CrossRef]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef]
- Lundh, H.; Schiller, H.H.; Elmqvist, D. Correlation between single fibre EMG jitter and endplate potentials studied in mild experimental botulinum poisoning. Acta Neurol. Scand. 1977, 56, 141–152. [Google Scholar] [CrossRef]
- Rosales, R.L.; Arimura, K.; Takenaga, S.; Osame, M. Extrafusal and intrafusal muscle effects in experimental botulinum toxin-A injection. Muscle Nerve 1996, 19, 488–496. [Google Scholar] [CrossRef]
- Rosales, R.L.; Bigalke, H.; Dressler, D. Pharmacology of botulinum toxin: Differences between type A preparations. Eur. J. Neurol. 2006, 13 (Suppl. 1), 2–10. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Xiang, Y.; Hu, X. Acrylamide inhibits nerve sprouting induced by botulinum toxin type A. Neural Regen. Res. 2014, 9, 1525–1531. [Google Scholar] [PubMed]
- Nakamura, Y.; Sawada, M.; Ikeguchi, K.; Nakano, I. Food-borne botulism. Brain Nerve 2011, 63, 979–985. [Google Scholar] [PubMed]
- Funakawa, I.; Yasuda, T.; Katoh, H.; Hara, K.; Terao, A. A case of bilateral blepharospasm responsive to edrophonium. Rinsho Shinkeigaku 1992, 32, 527–531. [Google Scholar]
- Wan, X.; Tang, X.; Cui, L. Remote effects of local injection of botulinum toxin type A. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 1999, 21, 362–367. [Google Scholar]
- Mikhaĭlov, V.V. Mechanism of disorders in neurotrophic regulation of the level of striated skeletal muscle polarization by botulinum toxin. Bull. Eksp Biol. Med. 1980, 89, 276–278. [Google Scholar]
- Caruso, G.; Brienza, A.; Labianca, O.; Ferrannini, E.; Perniola, T. Muscular electrophysiological and histochemical findings in a case of botulinic poisoning. Acta Neurol. 1971, 26, 23–35. [Google Scholar]
- Westhues, M. Studies Using Non Myelinated Nerve Fibers on The Site of The Effect of Botulinum and Tetanus Toxin. Naunyn Schmiedebergs Arch. Exp. Pathol. Pharmakol. 1964, 246, 308–315. [Google Scholar] [PubMed]
- Leonardi, L.; Haggiag, S.; Petrucci, A.; Lispi, L. Electrophysiological abnormalities in iatrogenic botulism: Two case reports and review of the literature. J. Clin. Neurosci. 2019, 60, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Tugnoli, V.; Eleopra, R.; Quatrale, R.; Capone, J.G.; Sensi, M.; Gastaldo, E. Botulism-like syndrome after botulinum toxin type A injections for focal hyperhidrosis. Br. J. Derm. 2002, 147, 808–809. [Google Scholar] [CrossRef] [PubMed]
- Emmerson, J. Botulinum toxin for spasmodic torticollis in a patient with myasthenia gravis. Mov. Disord. 1994, 9, 367. [Google Scholar] [CrossRef]
- Coban, A.; Matur, Z.; Hanagasi, H.A.; Parman, Y. Iatrogenic botulism after botulinum toxin type A injections. Clin. Neuropharmacol. 2010, 33, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.B.; Massey, E.W.; Buckley, E.G. Botulinum toxin for blepharospasm: Single-fiber EMG studies. Neurology 1986, 36, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Lange, D.J.; Brin, M.F.; Warner, C.L.; Fahn, S.; Lovelace, R.E. Distant effects of local injection of botulinum toxin. Muscle Nerve 1987, 10, 552–555. [Google Scholar] [CrossRef]
- Olney, R.K.; Aminoff, M.J.; Gelb, D.J.; Lowenstein, D.H. Neuromuscular effects distant from the site of botulinum neurotoxin injection. Neurology 1988, 38, 1780–1783. [Google Scholar]
- Lange, D.J.; Rubin, M.; Greene, P.E.; Kang, U.J.; Moskowitz, C.B.; Brin, M.F.; Lovelace, R.E.; Fahn, S. Distant effects of locally injected botulinum toxin: A double-blind study of single fiber EMG changes. Muscle Nerve 1991, 14, 672–675. [Google Scholar] [CrossRef]
- Girlanda, P.; Vita, G.; Nicolosi, C.; Milone, S.; Messina, C. Botulinum toxin therapy: Distant effects on neuromuscular transmission and autonomic nervous system. J. Neurol. Neurosurg. Psychiatry 1992, 55, 844–845. [Google Scholar] [CrossRef] [Green Version]
- Garner, C.G.; Straube, A.; Witt, T.N.; Gasser, T.; Oertel, W.H. Time course of distant effects of local injections of botulinum toxin. Mov. Disord. 1993, 8, 33–37. [Google Scholar] [CrossRef]
- Girlanda, P.; Quartarone, A.; Sinicropi, S.; Nicolosi, C.; Messina, C. Unilateral injection of botulinum toxin in blepharospasm: Single fiber electromyography and blink reflex study. Mov. Disord. Off. J. Mov. Disord. Soc. 1996, 11, 27–31. [Google Scholar] [CrossRef]
- Bogucki, A. Serial SFEMG studies of orbicularis oculi muscle after the first administration of botulinum toxin. Eur. J. Neurol. 1999, 6, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Bakheit, A.M.; Ward, C.D.; McLellan, D.L. Generalised botulism-like syndrome after intramuscular injections of botulinum toxin type A: A report of two cases. J. Neurol. Neurosurg. Psychiatry 1997, 62, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, K.P.; Münchau, A.; Thompson, P.D.; Houser, M.; Chauhan, V.S.; Hutchinson, M.; Shapira, A.H.; Marsden, C.D. Generalised muscular weakness after botulinum toxin injections for dystonia: A report of three cases. J. Neurol. Neurosurg. Psychiatry 1999, 67, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, V.; Woodson, G.E.; Bertorini, T.E. Single-fiber electromyography of the laryngeal muscles. Muscle Nerve 1999, 22, 111–114. [Google Scholar] [CrossRef]
- Tang, X.; Wan, X. Comparison of Botox with a Chinese type A botulinum toxin. Chin. Med. J. 2000, 113, 794–798. [Google Scholar]
- Roche, N.; Schnitzler, A.; Genêt, F.; Durand, M.C.; Bensmail, D. Undesirable distant effects following botulinum toxin type A injection. Clin. Neuropharmacol. 2008, 31, 272–280. [Google Scholar] [CrossRef]
- Osio, M.; Mailland, E.; Muscia, F.; Nascimbene, C.; Vanotti, A.; Bana, C.; Corsi, F.; Foschi, D.; Mariani, C. Botulinum neurotoxin-A does not spread to distant muscles after intragastric injection: A double-blind single-fiber electromyography study. Muscle Nerve 2010, 42, 165–169. [Google Scholar] [CrossRef]
- Schnitzler, A.; Genet, F.; Durand, M.-C.; Roche, N.; Bensmail, D.; Chartier-Kastler, E.; Denys, P. Pilot study evaluating the safety of intradetrusor injections of botulinum toxin type A: Investigation of generalized spread using single-fiber EMG. Neurourol. Urodyn 2011, 30, 1533–1537. [Google Scholar] [CrossRef]
- Alimohammadi, M.; Andersson, M.; Punga, A.R. Correlation of botulinum toxin dose with neurophysiological parameters of efficacy and safety in the glabellar muscles: A double-blind, placebo-controlled, randomized study. Acta Derm. Venereol. 2014, 94, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Punga, A.R.; Eriksson, A.; Alimohammadi, M. Regional diffusion of botulinum toxin in facial muscles: A randomised double-blind study and a consideration for clinical studies with split-face design. Acta Derm. Venereol. 2015, 95, 948–951. [Google Scholar] [CrossRef]
- Ruet, A.; Durand, M.C.; Denys, P.; Lofaso, F.; Genet, F.; Schnitzler, A. Single-fiber electromyography analysis of botulinum toxin diffusion in patients with fatigue and pseudobotulism. Arch. Phys. Med. Rehabil. 2015, 96, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Szuch, E.; Caress, J.B.; Paudyal, B.; Brashear, A.; Cartwright, M.S.; Strowd, R.E. Head drop after botox: Electrodiagnostic evaluation of iatrogenic botulinum toxicity. Clin. Neurol. Neurosurg. 2017, 156, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lispi, L.; Leonardi, L.; Petrucci, A. Longitudinal neurophysiological assessment of intramuscular type-A botulin toxin in healthy humans. Neurol. Sci. 2018, 39, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, G.; Depierreux, F.; Wang, F.; Hansen, I.; Maquet, P. Cosmetic Injection of Botulinum Toxin Unmasking Subclinical Myasthenia Gravis: A Case Report and Literature Review. Case Rep. Neurol. 2019, 11, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Punga, A.R.; Liik, M. Botulinum toxin injections associated with suspected myasthenia gravis: An underappreciated cause of MG-like clinical presentation. Clin. Neurophysiol. Pr. 2020, 5, 46–49. [Google Scholar] [CrossRef]
- Eleopra, R.; Rinaldo, S.; Montecucco, C.; Rossetto, O.; Devigili, G. Clinical duration of action of different botulinum toxin types in humans. Toxicon 2020, 179, 84–94. [Google Scholar] [CrossRef]
- Dutton, J.J. Botulinum-A toxin in the treatment of craniocervical muscle spasms: Short- and long-term, local and systemic effects. Surv. Ophthalmol. 1996, 41, 51–65. [Google Scholar] [CrossRef]
- Kessler, K.R.; Skutta, M.; Benecke, R. Long-term treatment of cervical dystonia with botulinum toxin A: Efficacy, safety, and antibody frequency. J. Neurol. 1999, 246, 265–274. [Google Scholar] [CrossRef]
- Ertaş, M.; Baslo, M.B.; Yildiz, N.; Yazici, J.; Oge, A.E. Concentric needle electrode for neuromuscular jitter analysis. Muscle Nerve 2000, 23, 715–719. [Google Scholar] [CrossRef]
- Sarrigiannis, P.G.; Kennett, R.P.; Read, S.; Farrugia, M.E. Single-fiber EMG with a concentric needle electrode: Validation in myasthenia gravis. Muscle Nerve 2006, 33, 61–65. [Google Scholar] [CrossRef]
- Marchand-Pauvert, V.; Aymard, C.; Giboin, L.-S.; Dominici, F.; Rossi, A.; Mazzocchio, R. Beyond muscular effects: Depression of spinal recurrent inhibition after botulinum neurotoxin A. J. Physiol. 2013, 591, 1017–1029. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.S.J.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Derm. 2004, 140, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Currà, A.; Berardelli, A. Do the unintended actions of botulinum toxin at distant sites have clinical implications? Neurology 2009, 72, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Currà, A.; Trompetto, C.; Abbruzzese, G.; Berardelli, A. Central effects of botulinum toxin type A: Evidence and supposition. Mov. Disord. 2004, 19 (Suppl. 8), S60–S64. [Google Scholar] [CrossRef] [PubMed]
- Abbruzzese, G.; Berardelli, A. Neurophysiological effects of botulinum toxin type A. Neurotox. Res. 2006, 9, 109–114. [Google Scholar] [CrossRef]
- Wiegand, H.; Erdmann, G.; Wellhöner, H.H. 125I-labelled botulinum A neurotoxin: Pharmacokinetics in cats after intramuscular injection. Naunyn Schmiedebergs Arch. Pharm. 1976, 292, 161–165. [Google Scholar] [CrossRef]
- Antonucci, F.; Rossi, C.; Gianfranceschi, L.; Rossetto, O.; Caleo, M. Long-Distance Retrograde Effects of Botulinum Neurotoxin, A. J. Neurosci. 2008, 28, 3689–3696. [Google Scholar] [CrossRef]
- Matak, I.; Riederer, P.; Lacković, Z. Botulinum toxin’s axonal transport from periphery to the spinal cord. Neurochem. Int. 2012, 61, 236–239. [Google Scholar] [CrossRef] [Green Version]
- Restani, L.; Giribaldi, F.; Manich, M.; Bercsenyi, K.; Menendez, G.; Rossetto, O.; Caleo, M.; Schiavo, G. Botulinum neurotoxins A and E undergo retrograde axonal transport in primary motor neurons. PLoS Pathog. 2012, 8, e1003087. [Google Scholar] [CrossRef] [Green Version]
- Holds, J.B.; Alderson, K.; Fogg, S.G.; Anderson, R.L. Motor nerve sprouting in human orbicularis muscle after botulinum A injection. Invest. Ophthalmol. Vis. Sci. 1990, 31, 964–967. [Google Scholar]
- Alderson, K.; Holds, J.B.; Anderson, R.L. Botulinum-induced alteration of nerve-muscle interactions in the human orbicularis oculi following treatment for blepharospasm. Neurology 1991, 41, 1800–1805. [Google Scholar] [CrossRef]
- Juzans, P.; Comella, J.X.; Molgo, J.; Faille, L.; Angaut-Petit, D. Nerve terminal sprouting in botulinum type-A treated mouse levator auris longus muscle. Neuromuscul. Disord. Nmd 1996, 6, 177–185. [Google Scholar] [CrossRef]
- de Paiva, A.; Meunier, F.A.; Molgó, J.; Aoki, K.R.; Dolly, J.O. Functional repair of motor endplates after botulinum neurotoxin type A poisoning: Biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc. Natl. Acad. Sci. USA 1999, 96, 3200–3205. [Google Scholar] [CrossRef] [Green Version]
- Harris, C.P.; Alderson, K.; Nebeker, J.; Holds, J.B.; Anderson, R.L. Histologic features of human orbicularis oculi treated with botulinum A toxin. Arch. Ophthalmol. 1991, 109, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Borodic, G.E.; Ferrante, R. Effects of repeated botulinum toxin injections on orbicularis oculi muscle. J. Clin. Neuroophthalmol. 1992, 12, 121–127. [Google Scholar]
- Van Putten, M.J.M.; Padberg, M.; Tavy, D.L.J. In vivo analysis of end-plate noise of human extensor digitorum brevis muscle after intramuscularly injected botulinum toxin type A. Muscle Nerve 2002, 26, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Duchen, L.W.; Strich, S.J. The effects of botulinum toxin on the pattern of innervation of skeletal muscle in the mouse. Q. J. Exp. Physiol. Cogn. Med. Sci. 1968, 53, 84–89. [Google Scholar] [CrossRef] [Green Version]
- Angaut-Petit, D.; Molgó, J.; Comella, J.X.; Faille, L.; Tabti, N. Terminal sprouting in mouse neuromuscular junctions poisoned with botulinum type A toxin: Morphological and electrophysiological features. Neuroscience 1990, 37, 799–808. [Google Scholar] [CrossRef]
- Thompson, W.; Jansen, J.K. The extent of sprouting of remaining motor units in partly denervated immature and adult rat soleus muscle. Neuroscience 1977, 2, 523–535. [Google Scholar] [CrossRef]
- Jankovic, J.; Kenney, C.; Grafe, S.; Goertelmeyer, R.; Comes, G. Relationship between various clinical outcome assessments in patients with blepharospasm. Mov. Disord. 2009, 24, 407–413. [Google Scholar] [CrossRef]
- Wabbels, B.; Jost, W.H.; Roggenkämper, P. Difficulties with differentiating botulinum toxin treatment effects in essential blepharospasm. J. Neural. Transm. 2011, 118, 925–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefaucheur, J.P. Electrophysiological assessment of reflex pathways involved in spasticity. Neurochirurgie 2003, 49, 205–214. [Google Scholar]
- Pandyan, A.D.; Vuadens, P.; van Wijck, F.M.J.; Stark, S.; Johnson, G.R.; Barnes, M.P. Are we underestimating the clinical efficacy of botulinum toxin (type A)? Quantifying changes in spasticity, strength and upper limb function after injections of Botox to the elbow flexors in a unilateral stroke population. Clin. Rehabil. 2002, 16, 654–660. [Google Scholar] [CrossRef]
- Albani, G.; Cimolin, V.; Galli, M.; Vimercati, S.; Bar, D.; Campanelli, L.; Gandolfi, R.; Lombardi, R.; Mauro, A. Use of surface EMG for evaluation of upper limb spasticity during botulinum toxin therapy in stroke patients. Funct. Neurol. 2010, 25, 103–107. [Google Scholar]
- Kawakami, Y.; Abe, T.; Fukunaga, T. Muscle-fiber pennation angles are greater in hypertrophied than in normal muscles. J. Appl. Physiol. 1993, 74, 2740–2744. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Tong, K.Y.; Hu, X. The Effect of Poststroke Impairments on Brachialis Muscle Architecture as Measured by Ultrasound. Arch. Phys. Med. Rehabil. 2007, 88, 243–250. [Google Scholar] [CrossRef]
- Mohagheghi, A.A.; Khan, T.; Meadows, T.H.; Giannikas, K.; Baltzopoulos, V.; Maganaris, C.N. Differences in gastrocnemius muscle architecture between the paretic and non-paretic legs in children with hemiplegic cerebral palsy. Clin. Biomech. Bristol. Avon. 2007, 22, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Girardi, P.; Manca, M.; Gimigliano, R.; Smania, N. Is spastic muscle echo intensity related to the response to botulinum toxin type A in patients with stroke? A cohort study. Arch. Phys. Med. Rehabil. 2012, 93, 1253–1258. [Google Scholar] [CrossRef]
- Park, G.-Y.; Kwon, D.R. Sonoelastographic evaluation of medial gastrocnemius muscles intrinsic stiffness after rehabilitation therapy with botulinum toxin A injection in spastic cerebral palsy. Arch. Phys. Med. Rehabil. 2012, 93, 2085–2089. [Google Scholar] [CrossRef]
- Ceyhan Bilgici, M.; Bekci, T.; Ulus, Y.; Bilgici, A.; Tomak, L.; Selcuk, M.B. Quantitative assessment of muscle stiffness with acoustic radiation force impulse elastography after botulinum toxin A injection in children with cerebral palsy. J. Med. Ultrason. 2018, 45, 137–141. [Google Scholar] [CrossRef]
- Aşkın, A.; Kalaycı, Ö.T.; Bayram, K.B.; Tosun, A.; Demirdal, Ü.S.; Atar, E.; İnci, M.F. Strain sonoelastographic evaluation of biceps muscle intrinsic stiffness after botulinum toxin-A injection. Top. Stroke Rehabil. 2017, 24, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Elsaidi, G.A.; Smith, T.L.; Walker, F.O.; Tan, K.H.; Martin, E.; Koman, L.A.; Smith, B.P. Time course of recovery of juvenile skeletal muscle after botulinum toxin A injection: An animal model study. Am. J. Phys. Med. Rehabil. 2004, 83, 774–780, quiz 781–783. [Google Scholar] [CrossRef] [PubMed]
- Spaans, F.; Wilts, G. Denervation due to lesions of the central nervous system. An EMG study in cases of cerebral contusion and cerebrovascular accidents. J. Neurol. Sci. 1982, 57, 291–305. [Google Scholar] [CrossRef]
- Chang, C.W. Evident trans-synaptic degeneration of motor neurons after stroke: A study of neuromuscular jitter by axonal microstimulation. Electroencephalogr. Clin. Neurophysiol. 1998, 109, 199–202. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Kokubun, N.; Sonoo, M.; Imai, T.; Arimura, Y.; Kuwabara, S.; Komori, T.; Kobayashi, M.; Nagashima, T.; Hatanaka, Y.; Tsuda, E.; et al. Reference values for voluntary and stimulated single-fibre EMG using concentric needle electrodes: A multicentre prospective study. Clin. Neurophysiol. 2012, 123, 613–620. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Population Number, Age (Years), Disease | Injected Muscle(s) | Jitter (MCD in µs) Mean Pre-Injection Value/Maximum Post Injection Value |
|---|---|---|---|
| Sanders et al. 1986 [94] | n = 4, age and sex US, BSP- HSF | OO bilaterally | OO: 30/>300; Frontal: 24/>300; EDC: 30/50 BB: US/66 |
| Lange et al. 1987 [95] | n = 5, 42‒62 Torticollis, Dystonia | SCM, Trapezius Temporalis | EDC: 28/65.2 |
| Olney et al. 1988 [96] | n = 6, 31‒64, Torticollis | Cervical | BB: 26/46 |
| Lange et al. 1991 [97] | n = 42, 25‒75, Torticollis | Cervical | EDC: 21/43.6; BB: 21.7/US; TA: 28.8/US; Pb: 25.7/26.5 |
| Girlanda et al. 1992 [98] | n = 5, 25‒64, BSP, HSF, Torticollis | US | EDC: US/40 |
| Garner et al. 1993 [99] | n = 8, 31‒66, HSF, MGS, Perioral Dystonia | Right upper lip Cervical, Left eye, Periorbital | EDC: US/156 TA: US/129 |
| Girlanda et al. 1996 [100] | n = 6, 56‒70, BSP | Around one eye BoNT-A Around the other eye Pb | BoNT-A side: <30/250 Placebo side: 20/48 |
| Bogucki et al. 1999 [101] | n = 16, 41‒84, BSP, HSF, MGS | OO | OO: 22.7 ± 2.5/150 |
| Bakheit et al. 1997 [102] | n = 2, 34‒67, MS, MSA with torticollis | Hamstring, SCM, Splenius, Trapezius | EDC: US/408 |
| Bhatia et al. 1999 [103] | n = 3, 32‒57, Cervical dystonia, Hemidystonia | SCM, Splenius, BB, Brachioradialis, Flexor carpi ulnaris, Adductor pollicis, Flexor hallucis brevis, Flexor digitorum | EDC: US/93.6 BB: US/US |
| Schweizer et al. 1999 [104] | n = 1, 73, US | Thyroarytenoid | Thyroarytenoid: US/40.70 |
| Tang et al. 2000 [105] | n = 785, 5‒82, BSP, Cervical dystonia, HSF, MGS | EDC | EDC Botox®: 29.9/43.8 CBTX-A®: 28.5/46.2 |
| Roche et al. 2008 [106] | n = 4, 25‒59, Hemiplegic, Paraplegia, MS | FDL, FDP, FDS, FRC, FHL, TS | EDC: US/54.2 OO: US/31.31 |
| Osio et al. 2010 [107] | n = 24, BoNT-A group 40.6 ± 3.5, Pb group 45.2 ± 3.7, Obesity | Intragastric | EDC: BoNT-A group: 29.12 ± 4.38/33.1; Pb group: 29.44 ± 3.64/33.1 EDC: US/24.9 |
| Schnitzler et al. 2011 [108] | n = 21, 22‒65, Medullary lesion with neurogenic overactive bladder | Intradetrusor injection | OO: US/25.9 BoNT-A group: 27.6/38.9 Pb group: 28.7/31.7 |
| Alimohammadi et al. 2014 [109] | n = 16, 31‒64, healthy | Glabellar muscle | Contralateral Frontalis: 28/39 |
| Punga et al. 2015 [110] | n = 5, 33‒52, Glabellar frown lines | Corrugator muscle | EDC: US/110.9 |
| Ruet et al. 2015 [111] | n = 5, 30‒77, Detrusor hyperactivity, Hypertonia | Detrusor muscle, Striated muscle responsible for dystonia | OO: US/31.6 |
| Szuch et al. 2017 [112] | n = 1, 72, Parkinson’s disease | EHL, FDL, Gastrocnemius, Peroneus longus, Soleus | EDC: US/66.2 for voluntary SFEMG; 52.7 for stimulated SFEMG |
| Lispi et al. 2018 [113] | n = 10, 42‒64, Healthy | EDB | EDB: 28 ± 7.5/148.3 |
| Leonardi et al. 2019 [90] | n = 2, 32‒48, CP, MS | Quadriceps, Adductors | Deltoid: US/111.4 EDC: US/75.6 |
| Timmermans et al. 2019 [114] | n = 1, 43, Healthy | Glabellar, Forehead, Lateral canthal rhytids | OO: US/112 |
| Punga et al. 2020 [115] | n = 2, 46‒55, Wrinkles, Migraine | Around OO, Glabellar, Head, Neck | Deltoid: US/25; Frontalis: US/US; OO: US/125 |
| Eleopra et al. 2020 [116] | n = 12, 34‒51, Healthy | ADM | ADM: 25.3/133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moron, H.; Gagnard-Landra, C.; Guiraud, D.; Dupeyron, A. Contribution of Single-Fiber Evaluation on Monitoring Outcomes Following Injection of Botulinum Toxin-A: A Narrative Review of the Literature. Toxins 2021, 13, 356. https://doi.org/10.3390/toxins13050356
Moron H, Gagnard-Landra C, Guiraud D, Dupeyron A. Contribution of Single-Fiber Evaluation on Monitoring Outcomes Following Injection of Botulinum Toxin-A: A Narrative Review of the Literature. Toxins. 2021; 13(5):356. https://doi.org/10.3390/toxins13050356
Chicago/Turabian StyleMoron, Hélène, Corine Gagnard-Landra, David Guiraud, and Arnaud Dupeyron. 2021. "Contribution of Single-Fiber Evaluation on Monitoring Outcomes Following Injection of Botulinum Toxin-A: A Narrative Review of the Literature" Toxins 13, no. 5: 356. https://doi.org/10.3390/toxins13050356