
Suprasellar Ganglioglioma Arising from the Third Ventricle Floor: A Case Report and Review of the Literature
Abstract
:1. Introduction
2. Patient Information
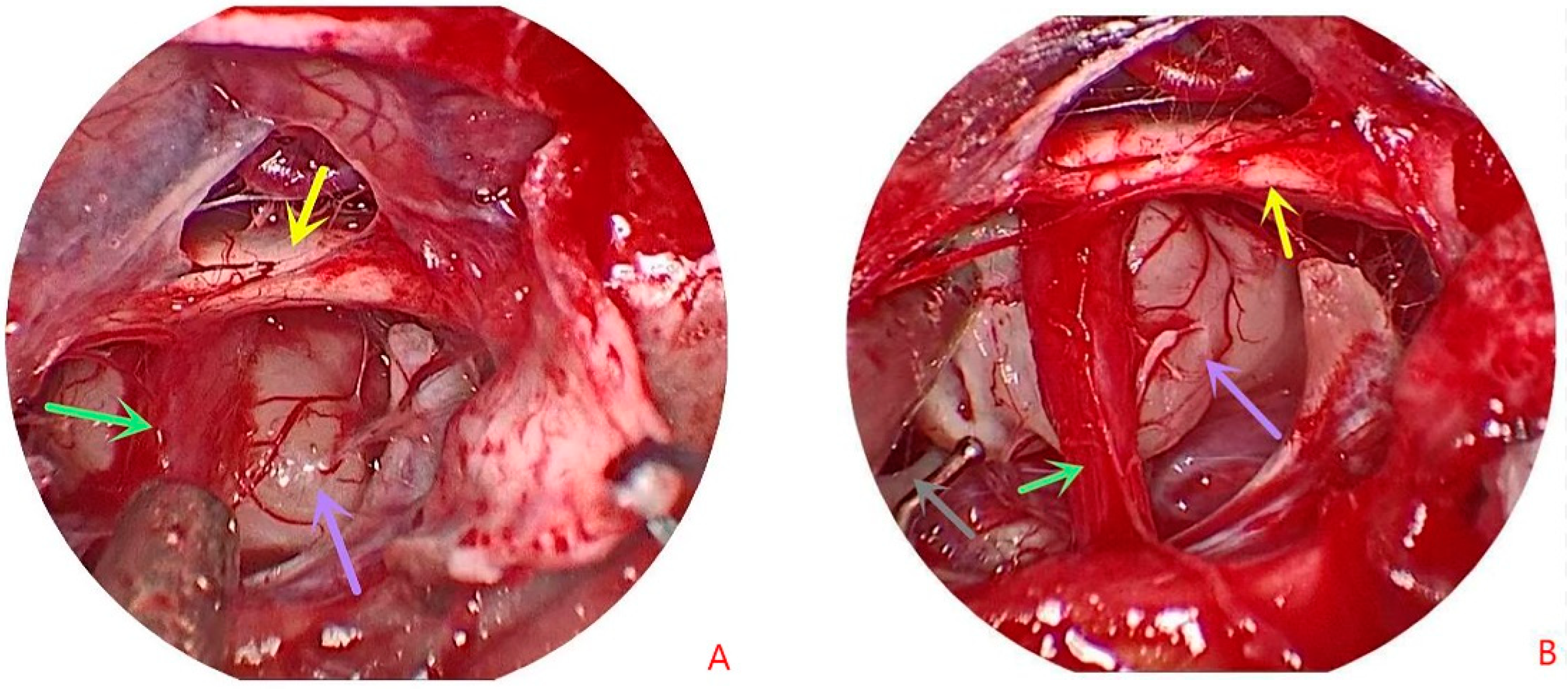
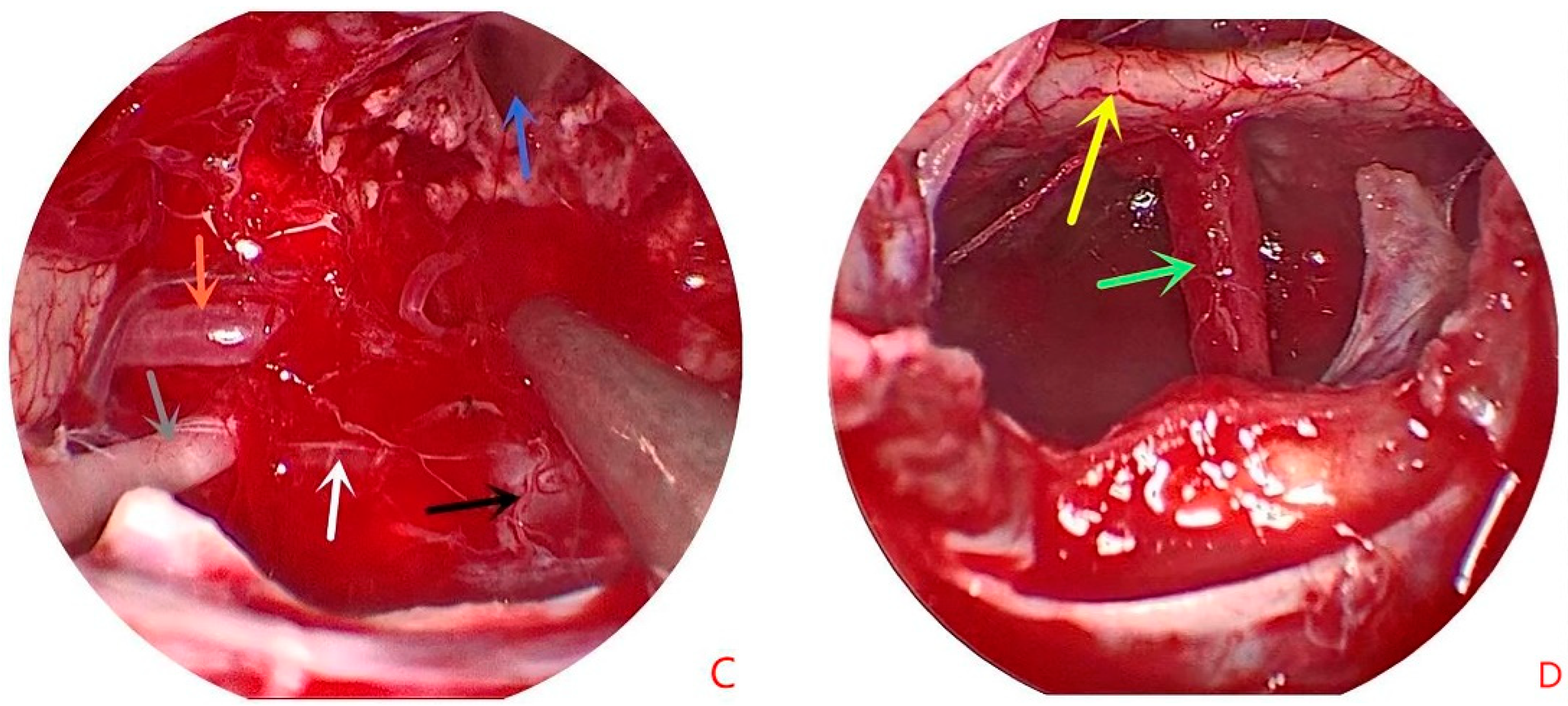
3. Operative Note
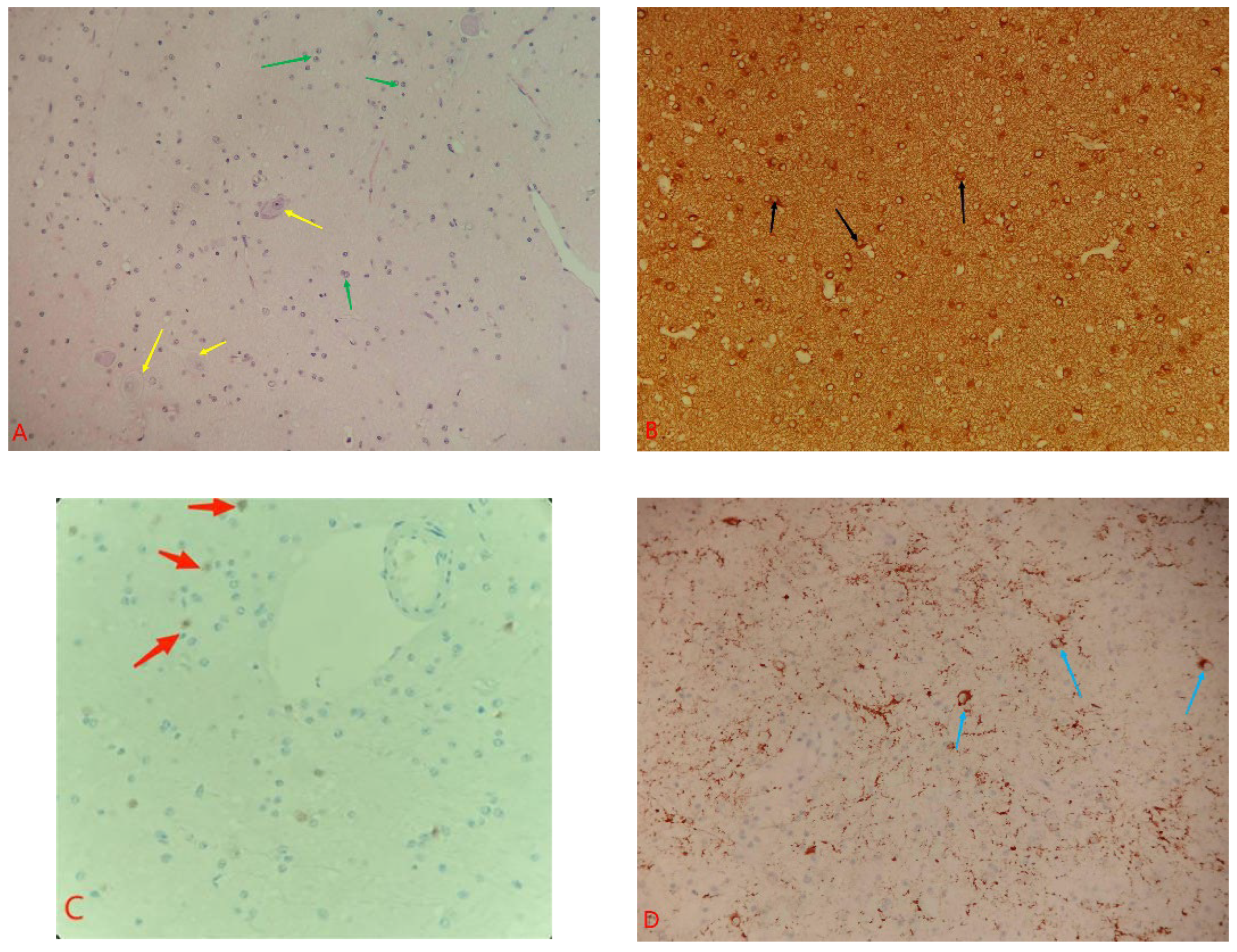
4. Histopathology
5. Postoperative Course
6. Review of Ganglioglioma Cases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Publications | Age, Gender | Signs and Symptoms | Symptom Duration | Location | MRI Signs | Treatment Solutions | Preoperative Diagnosis |
|---|---|---|---|---|---|---|---|
| Khoi D. Nguyen et al. [8] | 25, M | Headache, agitation, mental status decline, obstructive hydrocephalus | Acute onset | Sellar/suprasellar region | Heterogeneously enhanced 3.6 cm × 4.2 cm cystic and solid mass | STR | Craniopharyngioma |
| Shanop Shuangshoti et al. [7] | 21, F | Hyperprolactinemia, decreased vision | 2 Y 6 Mon | Suprasellar and optic chiasm | Heterogeneously enhanced 3.0 cm × 2.8 cm cystic and solid mass | NTR | Pilocytic astrocytoma |
| Laura Pastor et al. [5] | 9, M | Headache and epistaxis, lefthemiparesis and gait impairment (middle cerebral arteryinfarction) | 2 Mon | Suprasellar | Heterogeneously enhanced 2.2 cm × 2.5 cm cystic and solid mass | Biopsy | Germ-cell neoplasm, hypothalamic glioma |
| Ruchika Gupta et al. [6] | 7, M | Abnormal weight gain, diabetes insipidus, decreased vision, obstructive hydrocephalus | 18 Mon | Suprasellar | 4.2 cm × 4.5 cm cystic and solid mass | Biopsy + R | Germinoma |
| Rakesh Jalali et al. [18] | 7, F | Decreased vision | 6 Mon | Suprasellar and left parasellar regions | Enhanced cystic and solid mass | Biopsy + R | Optic pathway glioma, germ-cell neoplasm |
| Ishita Pant et al. [19] | 8, F | Decreased vision, headaches | 5 Y | Suprasellar, third ventricle | 7 × 6.5 cm cystic and solid mass | NTR | Chiasmatic glioma |
| John D. Rolston et al. [20] | 49, M | Developed headaches, decreased vision | Several months | Suprasellar | Enhanced 2 × 1.2 cm cystic and solid mass | Biopsy | NR |
| Ramazan Albayrak et al. [21] | 52, F | Decreased vision, headaches | Several months | Right optic tract | Diffuse contrast enhancement in right optic tract mass | Partial resection | Optic tract glioma |
| Jonathan Chilton et al. [9] | 33, M | Decreased vision | NR | Optic chiasm, optic nerve | Solid mass | Biopsy | Optic pathway glioma |
| Donald J. Bergin et al. [10] | 13, M | Proptosis, decreased vision, optic atrophy | NR | Optic nerve | 3.0 × 1.8 cm left retrobulbar optic nerve | NR | Optic pathway glioma |
| Kazuhiko Sugiyama et al. [4] | 12, F | Decreased vision, gradual hemiplegia of left limb | 4 Y | Optic nerve | Cystic and solid mass | Biopsy | Optic pathway glioma |
| Yoshito Sugita et al. [11] | 26, M | Decreased vision, headache, obstructive hydrocephalus | 1 Mon | Optic chiasm, suprasellar | Cystic and solid mass | Partially resection + V-P shunt + R | NR |
| Burak Karaaslan et al. [12] | 12, F | Decreased vision | 6 Mon | Suprasellar, optic nerve | Heterogeneously enhanced 3.0 cm × 3.0 cm cystic and solid mass | Biopsy | NR |
| G. V. Vajramani et al. [13] | 18, M | Decreased vision | 1 Y | Optic nerve, optic tract, geniculate | Heterogeneously enhanced cystic and solid mass | Biopsy + C | NR |
| G. T. Liu et al. [14] | 6, M | Headache, vomiting, decreased vision | NR | NR | NR | Biopsy + R | NR |
| William Y. Lu et al. [15] | 38, M | Decreased vision | 6 Mon | Optic nerve | Enhanced 4.8 × 0.9 cm mass | Surgery | NR |
| Pietro Spennato et al. [16] | 6, M | Decreased vision | NR | Sellar, suprasellar, third ventricle | Cystic and solid mass | Surgery + V-P shunt + R + C | NR |
| Bashar Abuzayed et al. [17] | 16, F | Decreased vision | 15 Y | Hypothalamus, optic chiasm | Uniformly enhanced solid mass | Surgery | NR |
| ShaoGuang Li et al. | 40, F | Dizziness, visual field defect | NR | Suprasellar | Enhanced 1.7 × 1.1 cm cystic mass | GTR + R | Craniopharyngioma |
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blümcke, I.; Wiestler, O.D. Gangliogliomas: An intriguing tumor entity associated with focal epilepsies. J. Neuropathol. Exp. Neurol. 2002, 61, 575–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Brem, H.; Brem, S.; Butowski, N.; Campian, J.L.; Clark, S.W.; Fabiano, A.J.; et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1537–1570. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for the diagnosis and treatment of gliomas (2018 edition). Chin. J. Neurosurg. 2019, 03, 217–239.
- Sugiyama, K.; Goishi, J.; Sogabe, T.; Uozumi, T.; Hotta, T.; Kiya, K. Ganglioglioma of the optic pathway. A case report. Surg. Neurol. 1992, 37, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Pastor, L.; Iglesias, S.; Ros, B.; Weil, B.; Martínez-León, M.I.; Arráez, M.Á. Suprasellar ganglioglioma presenting as a middle cerebral artery infarction. Childs Nerv. Syst. 2019, 35, 1625–1628. [Google Scholar] [CrossRef]
- Gupta, R.; Suri, V.; Arora, R.; Sharma, M.C.; Mishra, S.; Singh, M.; Sarkar, C. Suprasellar ganglioglioma presenting with diabetes insipidus in a young boy: A rare clinical presentation. Childs Nerv. Syst. 2010, 26, 255–258. [Google Scholar] [CrossRef]
- Shuangshoti, S.; Kirsch, E.; Bannan, P.; Fabian, V.A. Ganglioglioma of the optic chiasm: Case report and review of the literature. AJNR Am. J. Neuroradiol. 2000, 21, 1486–1489. [Google Scholar]
- Nguyen, K.D.; Waitt, T.; Alleyne, C.H., Jr. Sellar/Suprasellar Ganglioglioma: Clinical Image. World Neurosurg. 2019, 132, 1–3. [Google Scholar] [CrossRef]
- Chilton, J.; Caughron, M.R.; Kepes, J.J. Ganglioglioma of the optic chiasm: Case report and review of the literature. Neurosurgery 1990, 26, 1042–1045. [Google Scholar] [CrossRef]
- Bergin, D.J.; Johnson, T.E.; Spencer, W.H.; McCord, C.D. Ganglioglioma of the optic nerve. Am. J. Ophthalmol. 1988, 105, 146–149. [Google Scholar] [CrossRef]
- Sugita, Y.; Sawada, M.; Munemitsu, T.; Higashi, T.; Hojo, M. Discrepancy between radiological and histological findings in ganglioglioma of the optic chasm: Case report. Surg. Neurol. Int. 2017, 8, 146. [Google Scholar] [PubMed] [Green Version]
- Karaaslan, B.; Uçar, M.; Kulduk, G.; Börcek, A.Ö.; Baykaner, M.K. Bilateral Optic Pathway Ganglioglioma: The Fifth Case in the Literature. Pediatr. Neurosurg. 2016, 51, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Vajramani, G.V.; Dambatta, S.; Walker, M.; Grundy, P.L. Multiple gangliogliomas of the optic pathway. Br. J. Neurosurg. 2006, 20, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.T.; Galetta, S.L.; Rorke, L.B.; Bilaniuk, L.T.; Vojta, D.D.; Molloy, P.T.; Phillips, P.C.; Needle, M.; Duhaime, A.C.; Sutton, L.N.; et al. Gangliogliomas involving the optic chiasm. Neurology 1996, 46, 1669–1673. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.Y.; Goldman, M.; Young, B.; Davis, D.G. Optic nerve ganglioglioma. Case report. J. Neurosurg. 1993, 78, 979–982. [Google Scholar] [CrossRef] [PubMed]
- Spennato, P.; Giordano, M.; Ruggiero, C.; Aliberti, F.; Buonocore, M.C.; Nastro, A.; D’Onofrio, V.; Bifani, D.; Cinalli, G. Optic pathway ganglioglioma with intraventricular cyst. J. Neurooncol. 2011, 102, 499–508. [Google Scholar] [CrossRef]
- Abuzayed, B.; Alawneh, K.; Al-Qawasmeh, M.; Al-Khatib, S.; Barukba, M.; Raffee, L. Ganglioglioma of optic chiasma: A case report and review of literature. Surg. Neurol. Int. 2020, 11, 392. [Google Scholar] [CrossRef]
- Jalali, R.; Deopujari, C.E.; Bhutani, R.; Suhas, U.; Rajasekharan, P.; Kane, S.V.; Gupta, T. Suprasellar ganglioglioma with unusual diffuse involvement of the entire optico-chiasmal hypothalamic pathway. J. Cancer Res. Ther. 2008, 4, 140–143. [Google Scholar] [CrossRef]
- Pant, I.; Suri, V.; Chaturvedi, S.; Dua, R.; Kanodia, A.K. Ganglioglioma of optic chiasma: Case report and review of literature. Childs Nerv. Syst. 2006, 22, 717–720. [Google Scholar] [CrossRef]
- Rolston, J.D.; Han, S.J.; Cotter, J.A.; El-Sayed, I.H.; Aghi, M.K. Gangliogliomas of the optic pathway. J. Clin. Neurosci. 2014, 21, 2244–2249. [Google Scholar] [CrossRef]
- Albayrak, R.; Albayram, S.; Port, J.; Değirmenci, B.; Acar, M.; Yücel, A. Ganglioglioma of the right optic tract: Case report and review of the literature. Magn. Reson. Imaging 2004, 22, 1047–1051. [Google Scholar] [CrossRef]
- Fehn, M.; Lohmann, F.; Lüdecke, D.K.; Rudorff, K.H.; Saeger, W. Ganglioglioma of the neurohypophysis with secretion of vasopressin. Exp. Clin. Endocrinol. Diabetes 1998, 106, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Fang, Y.; Wu, Q.; Zhang, J.; Wang, Y. Ganglioglioma of the adenohypophysis mimicking pituitary adenoma: A case report and review of the literature. Medicine (Baltimore) 2018, 97, e11583. [Google Scholar] [CrossRef]
- Scheithauer, B.W.; Silva, A.I.; Parisi, J.E.; Kovacs, K.; Horvath, E. Ganglioglioma of the neurohypophysis. Endocr. Pathol. 2008, 19, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Omofoye, O.A.; Lechpammer, M.; Steele, T.O.; Harsh, G.R., 4th. Pituitary stalk gangliogliomas: Case report and literature review. Clin. Neurol. Neurosurg. 2021, 201, 106405. [Google Scholar] [CrossRef] [PubMed]
- Hauck, E.F.; Vu, L.; Campbell, G.A.; Nauta, H.J. Intraventricular ganglioglioma. J. Clin. Neurosci. 2008, 15, 1291–1293. [Google Scholar] [CrossRef]
- Shono, T.; Tosaka, M.; Matsumoto, K.; Onaka, S.; Yamaguchi, S.; Mizoguchi, M.; Iwaki, T.; Nakazato, Y.; Sasaki, T. Ganglioglioma in the third ventricle: Report on two cases. Neurosurg. Rev. 2007, 30, 253–258, discussion 258. [Google Scholar] [CrossRef]
- Campos, A.R.; Biscoito, L.; Gasparinho, M.G. Intraventricular Ganglioglioma Presenting with Spontaneous Hemorrhage. Acta Med. Port. 2018, 31, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Jaeger, M.; Hussein, S.; Schuhmann, M.U.; Brandis, A.; Samii, M.; Blömer, U. Intraventricular trigonal ganglioglioma arising from the choroid plexus. Acta Neurochir. (Wien) 2001, 143, 953–955. [Google Scholar] [CrossRef]
- Majós, C.; Aguilera, C.; Ferrer, I.; López, L.; Pons, L.C. Intraventricular ganglioglioma: Case report. Neuroradiology 1998, 40, 377–379. [Google Scholar] [CrossRef]
- Harrison, W.; Elsamadicy, A.A.; McMahon, J.T.; Chagoya, G.; Sobel, R.A.; McLendon, R.E.; Adamson, C. Glioneuronal Tumor With Features of Ganglioglioma and Neurocytoma Arising in the Fourth Ventricle: A Report of 2 Unusual Cases and a Review of Infratentorial Gangliogliomas. J. Neuropathol. Exp. Neurol. 2019, 78, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Bhat, D.I.; Mahadevan, A.; Manish, R.; Sampath, S.; Chandramouli, B.A.; Shankar, S.K. Intraventricular ganglioglioma with bleed: A rare case report. Neurol India. 2010, 58, 477–480. [Google Scholar] [CrossRef] [PubMed]
- d’Andrea, G.; Sessa, G.; Ferrante, L. Ganglioglioma of the right lateral ventricle approached with neuronavigation and intraoperative DTI. Case report and literature review. Cent. Eur. Neurosurg. 2011, 72, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Yin Foo Lee, G.; Scott, G.; Blumbergs, P.C.; Patrick Brophy, B.; Lionel Crompton, J. Ganglioglioma of the lateral ventricle presenting with blepharospasm—Case report and review of the literature. J. Clin. Neurosci. 2001, 8, 279–282. [Google Scholar] [CrossRef]
- Higa, N.; Yonezawa, H.; Oyoshi, T.; Hiraki, T.; Hirano, H.; Arita, K. Ganglioglioma in the Third Ventricle: A Case Report and Literature Review. NMC Case Rep. J. 2016, 3, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Li, H.; Chen, M.; Si, Y.; Lei, D. Factors associated with preoperative and postoperative epileptic seizure in patients with cerebral ganglioglioma. Pak. J. Med. Sci. 2014, 30, 245–249. [Google Scholar] [CrossRef]
- Rana, R.; Perrillo, T.; Santoro, N.; Ortolani, F.; Messina, R.; Resta, M.; Perrucci, I.; Ingravallo, G.; Cazzato, G.; Grass, M.; et al. A Rare Case of Posterior Fossa Tumor and Central Precocious Puberty: Case Presentation and Review of the Literature. Neurol. Int. 2021, 13, 535–540. [Google Scholar] [CrossRef]
- Dash, R.C.; Provenzale, J.M.; McComb, R.D.; Perry, D.A.; Longee, D.C.; McLendon, R.E. Malignant supratentorial ganglioglioma (ganglion cell-giant cell glioblastoma): A case report and review of the literature. Arch. Pathol. Lab. Med. 1999, 123, 342–345. [Google Scholar] [CrossRef]
- Wolf, H.K.; Müller, M.B.; Spänle, M.; Zentner, J.; Schramm, J.; Wiestler, O.D. Ganglioglioma: A detailed histopathological and immunohistochemical analysis of 61 cases. Acta Neuropathol. 1994, 88, 166–173. [Google Scholar] [CrossRef]
- Fukushima, T.; Katayama, Y.; Watanabe, T.; Yoshino, A.; Komine, C.; Yokoyama, T. Aberrant TP53 protein accumulation in the neuronal component of ganglioglioma. J. Neurooncol. 2005, 72, 103–106. [Google Scholar] [CrossRef]
- Zentner, J.; Wolf, H.K.; Ostertun, B.; Hufnagel, A.; Campos, M.G.; Solymosi, L.; Schramm, J. Gangliogliomas: Clinical, radiological, and histopathological findings in 51 patients. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1497–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbach, H. MRI of long-term epilepsy-associated tumors. Semin Ultrasound CT MR 2008, 29, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Henning, T.D.; Zou, L.G.; Hu, L.B.; Wen, L.; Feng, X.Y.; Dai, S.H.; Wang, W.X.; Sun, Q.R.; Zhang, Z.G. Intracranial ganglioglioma: Clinicopathological and MRI findings in 16 patients. Clin. Radiol. 2008, 63, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Tamiya, T.; Ono, Y.; Furuta, T.; Asari, S.; Ohmoto, T. Cerebral gangliogliomas: Clinical characteristics, CT and MRI. Acta Neurochir. (Wien) 1999, 141, 135–141. [Google Scholar] [CrossRef]
- Jeswani, S.; Nuño, M.; Wu, A.; Bonert, V.; Carmichael, J.D.; Black, K.L.; Chu, R.; King, W.; Mamelak, A.N. Comparative analysis of outcomes following craniotomy and expanded endoscopic endonasal transsphenoidal resection of craniopharyngioma and related tumors: A single-institution study. J. Neurosurg. 2016, 124, 627–638. [Google Scholar] [CrossRef] [Green Version]
- Höhne, J.; Acerbi, F.; Falco, J.; Akçakaya, M.O.; Schmidt, N.O.; Kiris, T.; de Laurentis, C.; Ferroli, P.; Broggi, M.; Schebesch, K.-M. Lighting Up the Tumor-Fluorescein-Guided Resection of Gangliogliomas. J. Clin. Med. 2020, 9, 2405. [Google Scholar] [CrossRef]
- Compton, J.J.; Laack, N.N.; Eckel, L.J.; Schomas, D.A.; Giannini, C.; Meyer, F.B. Long-term outcomes for low-grade intracranial ganglioglioma: 30-year experience from the Mayo Clinic. J. Neurosurg. 2012, 117, 825–830. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Xiong, Y.; Hu, G.; Lv, S.; Song, P.; Guo, H.; Wu, L. Suprasellar Ganglioglioma Arising from the Third Ventricle Floor: A Case Report and Review of the Literature. Tomography 2022, 8, 2844-2853. https://doi.org/10.3390/tomography8060238
Li S, Xiong Y, Hu G, Lv S, Song P, Guo H, Wu L. Suprasellar Ganglioglioma Arising from the Third Ventricle Floor: A Case Report and Review of the Literature. Tomography. 2022; 8(6):2844-2853. https://doi.org/10.3390/tomography8060238
Chicago/Turabian StyleLi, Shaoguang, Yuanyuan Xiong, Guowen Hu, Shigang Lv, Pingan Song, Hua Guo, and Lei Wu. 2022. "Suprasellar Ganglioglioma Arising from the Third Ventricle Floor: A Case Report and Review of the Literature" Tomography 8, no. 6: 2844-2853. https://doi.org/10.3390/tomography8060238