
Post-Radiation Angiosarcoma (PRA) of the Small Bowel: Report of a Case and Review of the Literature
 , ,
, ,
Abstract
:1. Introduction
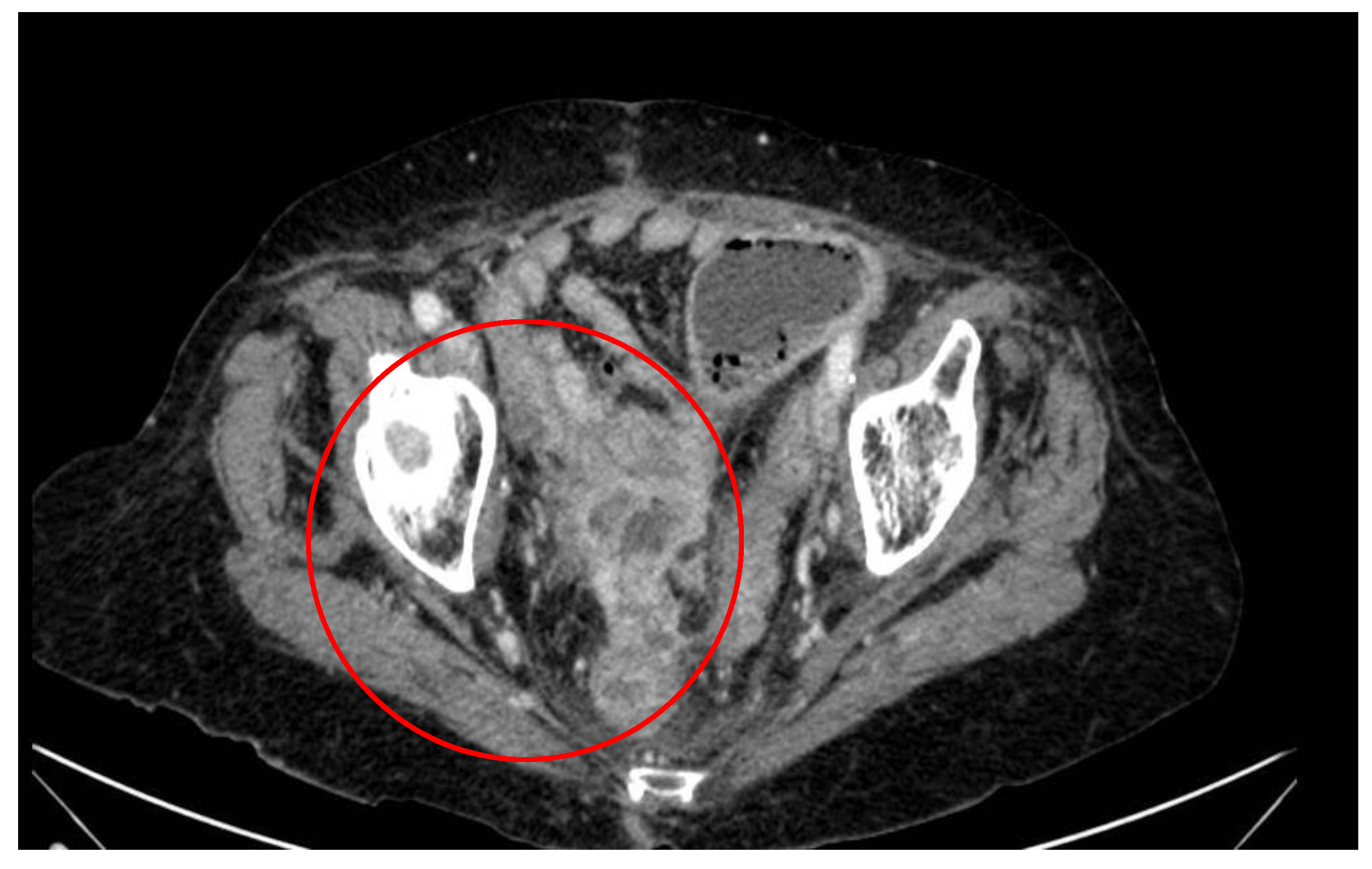
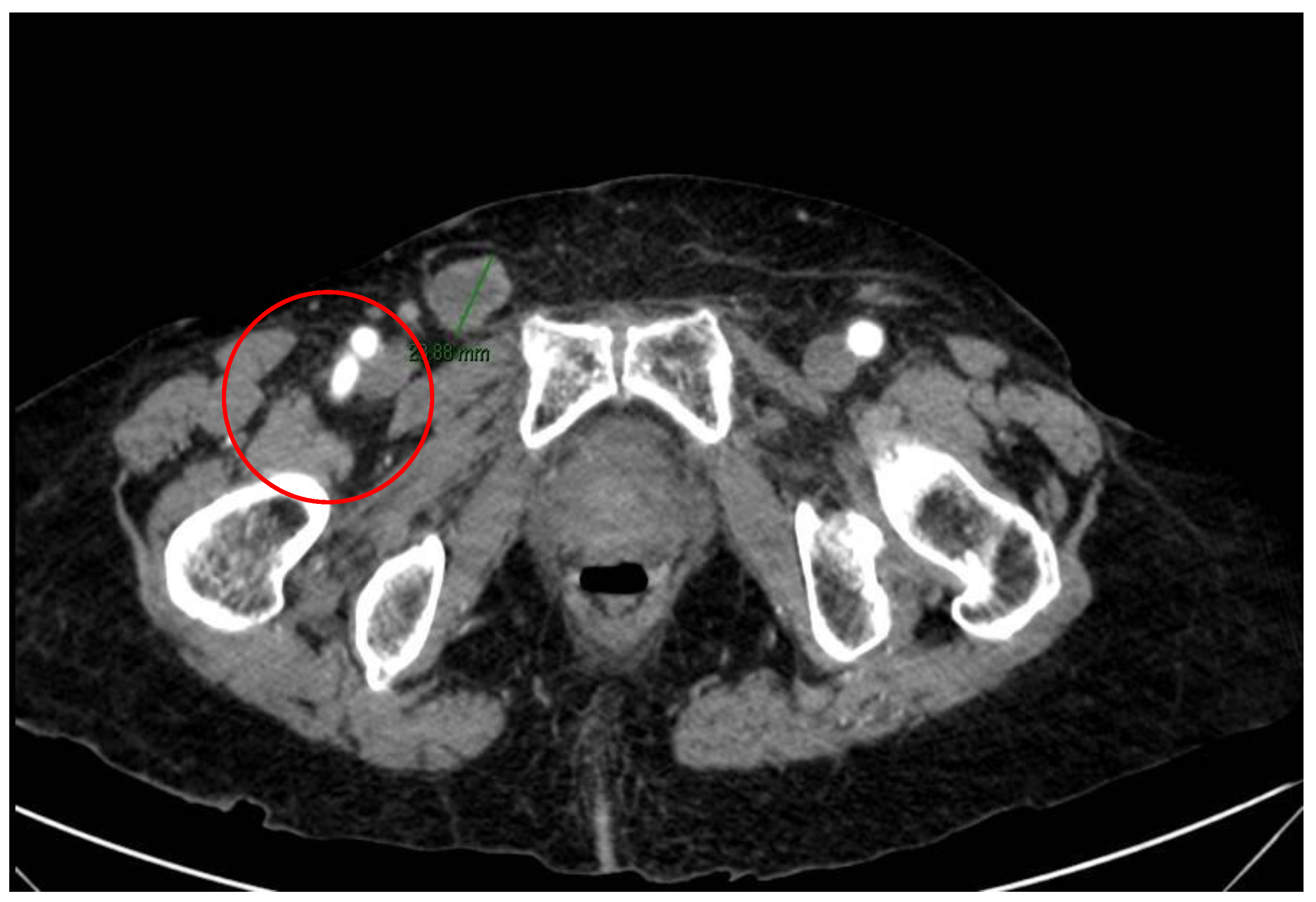
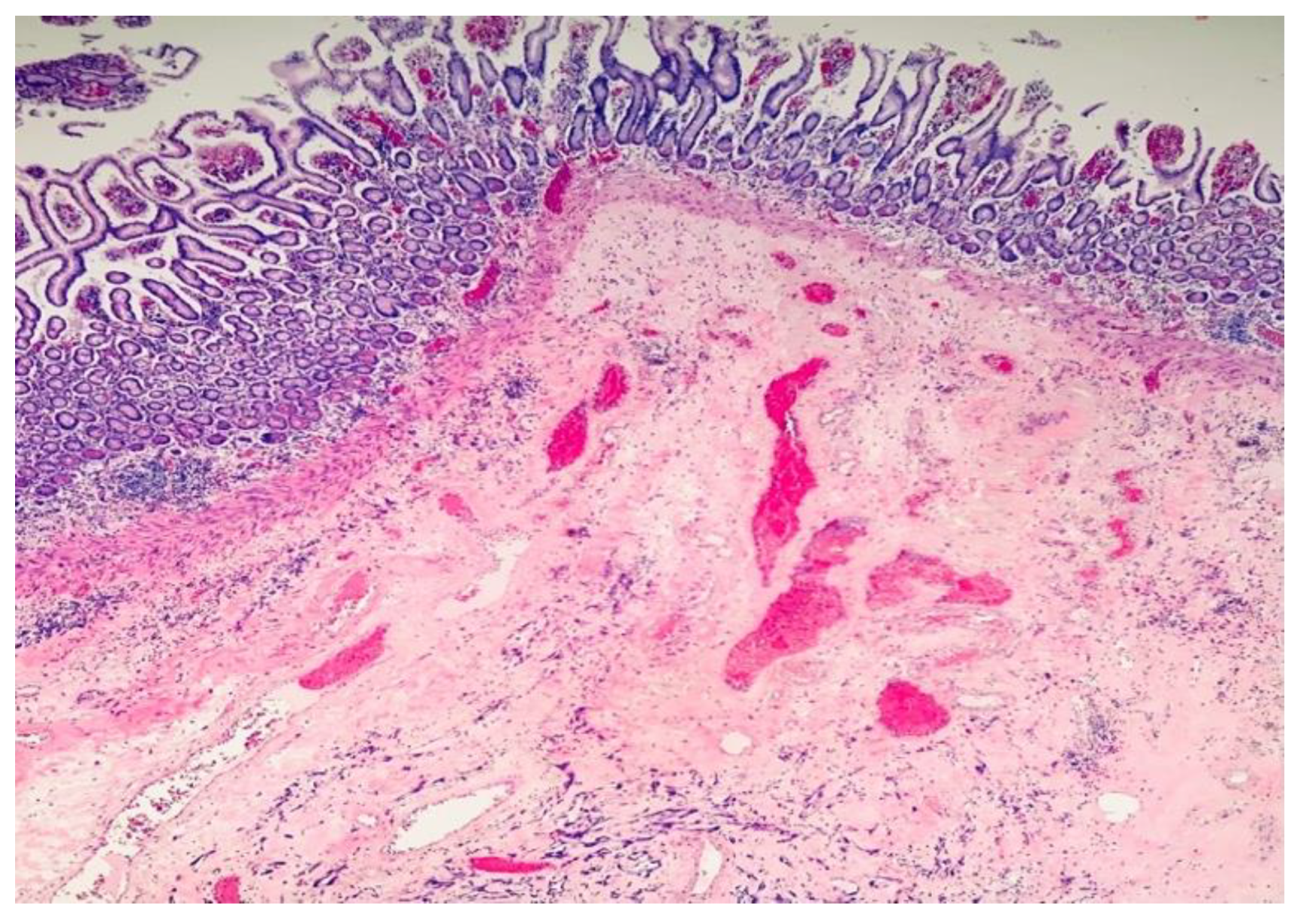
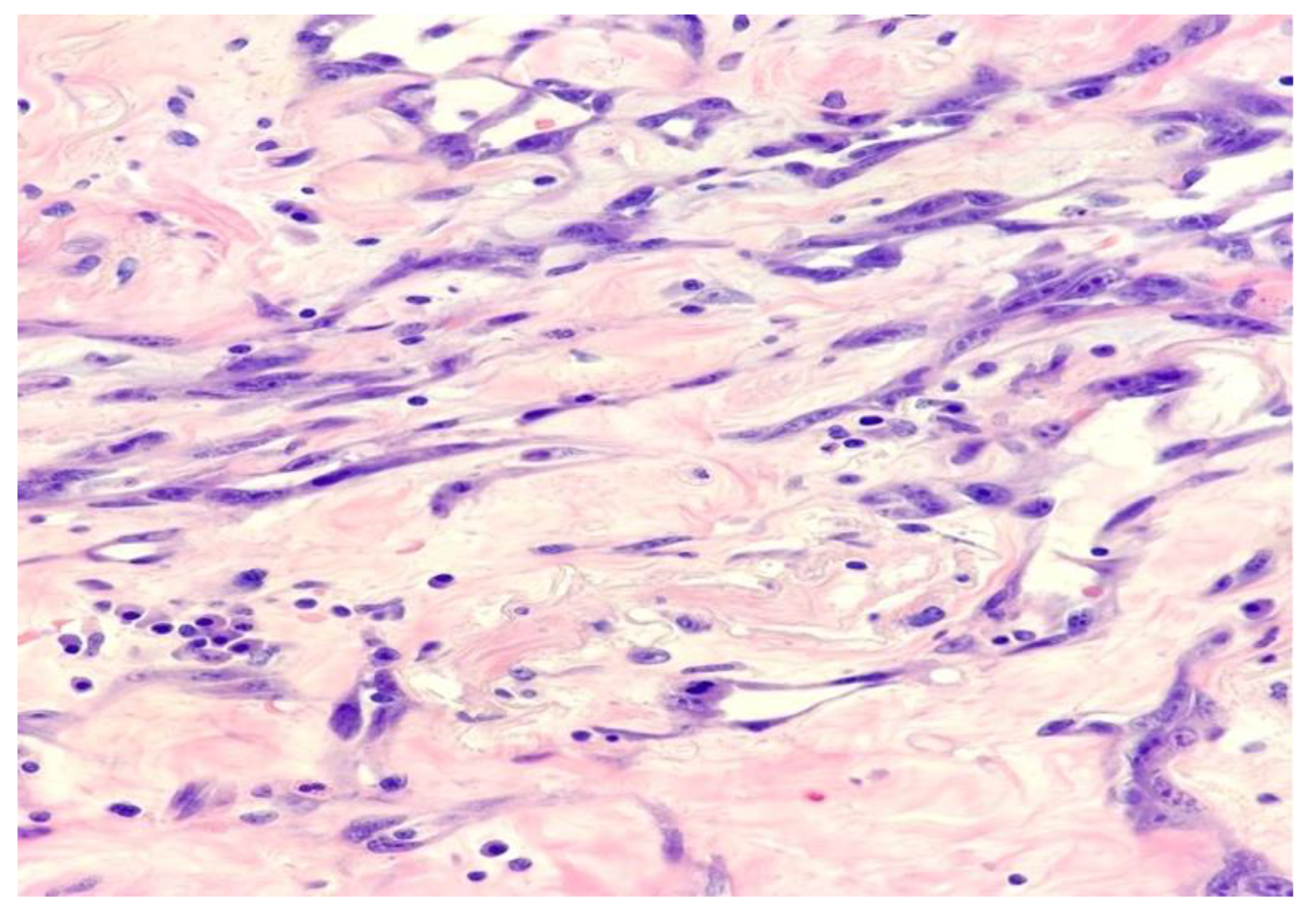
2. Case Report and Evolution
3. Review of the Literature

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Symptoms | Gender Prevalence | Markers for Angiosarcoma Diagnosis | |
|---|---|---|---|---|
| Primary [7] | Duodenum, jejunum, terminal ileum | Abdominal pain, vomiting, anemia, gastrointestinal bleeding, weakness | Male | CD31, vWF, CD34, ERG, vimentin |
| Secondary (Included PRA) [4] | Duodenum, jejunum, terminal ileum | Abdominal pain, gastrointestinal bleeding intestinal obstruction and perforation | Female | CD31, ERG, vWF, CD34, vimentin, MYC antibody |
| Authors | Sex/Age (Years) | Radiated for | Time after Radiation (Years) | Presentation | Treatment |
|---|---|---|---|---|---|
| Squillaci et al. [4] | F/72 | Uterine leiomyosarcoma | 24 | Abdominal pain | Resection |
| Hansen et al. [8] | F/76 | Endometrial adenocarcinoma | 7 | Watery diarrhea, vomiting, weight loss | Resection of ileal tract |
| Chen et al. [9] | F/66 | Endometrioid adenocarcinoma | 8 | Abdominal pain, vomiting | Ileo–colic resection |
| Aitola et al. [10] | F/50 | Endometrial adenocarcinoma | 14 | Intestinal obstruction | Resection followed by combination chemiotherapy with doxorubicin |
| Policarpio-Nicolas et al. [11] | F/51 | Adenocarcinoma of uterine cervix | 9 | Abdominal pain | Resection |
| Nanus et al. [12] | F/47 | Dysgerminoma/ovary | 16 | Perforated distal ileum | Resection |
| Hwang et al. [13] | F/60 | Carcinoma of uterin cervix | 8 | Abdominal pain | Resection |
| Suzuki et al. [14] | F/61 | Squamous cell carcinoma of uterus | 20 | Abdominal pain | Resection and intrabdominal cisplatin |
| Berry et al. [15] | M/51 | Hodgkin’s lymphoma | 3 | Peritonitis | Resection |
| Selk et al. [16] | M/57 | Chondrosarcoma | 8 | Abdominal distension | Resection |
| Wolov et al. [17] | F/80 | Squamous cell carcinoma of uterine cervix | 20 | Abdominal distension | Resection |
| Wolov et al. [17] | F/69 | Uterine adenocarcinoma | 7 | Abdominale distension, weight loss. | Resection |
| Our case | F/88 | Squamous cell carcinoma of uterine cervix | 20 | Abdominal pain, vomiting, intestinal obstruction | Resection |
| Authors | Gender/Age | Presentation | Site of Neoplasm | Treatment |
|---|---|---|---|---|
| Nai et al. [1] | M/73 | Chest pain, dyspnea, melena, weakness | Duodenum and jejunum, metastasis to peripancreatic and mesenteric lymph nodes | Pylorus preserving pancreaticoduodenectomy |
| Liu et al. [18] | F/43 | Intestinal perforation | Small bowel | Intestinal resection and entero-enterostomy |
| Takahashi et al. [19] | F/85 | Fever, abdominal distension | Small bowel | Laparotomy and resection of the mass |
| Xiao-Mei et al. [7] | M/70 | Abdominal pain and melena | Ileum | Intestinal resection |
| Zacarias et al. [20] | M/84 | Gastrointestinal bleeding | Jejunum | Resection of jejunum |
| Huntington et al. [21] | NA | Gastrointestinal bleeding | Small bowel | Resection |
| Chahbouni et al. [22] | F/25 | Unknown | Small bowel | Resection |
| Ryu et al. [23] | M/54 | Gastrointestinal bleeding | Small bowel | Resection |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | Angiosarcoma |
| PRA | Post-Radiation Angiosarcoma |
| ED | Emergency Department |
| GERD | Gastroesophageal reflux disease |
| GI | Gastrointestinal |
References
- Nai, Q.; Ansari, M.; Liu, J.; Razjouyan, H.; Pak, S.; Tian, Y.; Khan, R.; Broder, A.; Bagchi, A.; Iyer, V.; et al. Primary Small Intestinal Angiosarcoma: Epidemiology, Diagnosis and Treatment. J. Clin. Med. Res. 2018, 10, 294–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco Jimenez, J.; Aftab, G.; Ngo, D.Q. Metastatic Cutaneous Angiosarcoma: A Rare Entity. Cureus 2021, 13, e14577. [Google Scholar] [CrossRef] [PubMed]
- Cahan, W.G.; Woodard, H.Q.; Higinbotham, N.L.; Stewart, F.W.; Coley, B.L. Sarcoma arising in irradiated bone; report of 11 cases. Cancer 1948, 1, 3–29. [Google Scholar] [CrossRef] [PubMed]
- Squillaci, S.; Marasco, A.; Pizzi, G.; Chiarello, M.; Brisinda, G.; Tallarigo, F. Primary post-radiation angiosarcoma of the small bowel. Report of a case and review of the literature. Pathologica 2020, 112, 93–101. [Google Scholar] [CrossRef]
- Fleetwood, V.A.; Harris, J.C.; Luu, M.B. Cutaneous angiosarcoma metastatic to small bowel with nodal involvement. Gastroenterol. Hepatol. Bed Bench 2016, 9, 340–342. [Google Scholar]
- Rong, L.; Ze-ying, O.; Jun-bo, X.; Jian, H.; Yan-wu, Z.; Gui-ying, Z.; Qian, L.; Huan, G.; Ai-min, L.; Ting, L. Clinical Characteristics and Prognostic Factors of Small Intestine Angiosarcoma: A Retrospective Clinical Analysis of 66 Cases. Cell Physiol. Biochem. 2017, 44, 817–827. [Google Scholar]
- Ma, X.-M.; Yang, B.-S.; Yang, Y.; Wu, G.-Z.; Li, Y.-W.; Yu, X.; Ma, X.-L.; Wang, Y.-P.; Hou, X.-D.; Guo, Q.-H. Small intestinal angiosarcoma on clinical presentation, diagnosis, management and prognosis: A case report and review of the literature. Word J. Gastroenterol. 2023, 29, 561–578. [Google Scholar] [CrossRef]
- Hansen, S.H.; Holck, S.; Flyger, H.; Tange, U.B. Radiation-associated angiosarcoma of the small bowel. A case of multiploidy and a fulminant clinical course. APMIS 1996, 104, 891–894. [Google Scholar] [CrossRef]
- Chen, K.T.K.; Hoffman, K.D.; Hendricks, E.J. Angiosarcoma following therapeutic irradiation. Cancer 1979, 44, 2044–2048. [Google Scholar] [CrossRef]
- Aitola, P.; Poutiainen, A.; Nordback, I. Small-bowel angiosarcoma after pelvic irradiation: A report of two cases. Int. J. Color. Dis. 1999, 14, 308–310. [Google Scholar] [CrossRef]
- Policarpio-Nicolas, M.L.C.; Nicolas, M.M.; Keh, P.; Laskin, W.B. Post-radiation angiosarcoma of the small intestine: A case report and review of literature. Ann. Diagn. Pathol. 2006, 10, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Nanus, D.M.; Kelsen, D.; Clark, D.G.C. Radiation-induced angiosarcoma. Cancer 1987, 60, 777–779. [Google Scholar] [CrossRef]
- Hwang, T.L.; Sun, C.F.; Chen, M.F. Angiosarcoma of the small intestine after radiation therapy: Report of a case. J. Formos. Med. Assoc. 1993, 92, 658–661. [Google Scholar] [PubMed]
- Suzuki, F.; Saito, A.; Ishi, K.; Koyatsu, J.; Maruyama, T.; Suda, K. Intra-abdominal angiosarcomatosis after radiotherapy. J. Gastroenterol. Hepatol. 1999, 14, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Berry, G.J.; Anderson, C.J.; Pitts, W.C.; Neitzel, G.F.; Weiss, L.M. Cytology of angiosarcoma in effusions. Acta Cytol. 1991, 35, 538–542. [Google Scholar]
- Selk, A.; Wehrli, B.; Taylor, B.M. Chylous acites secondary to small-bowel angiosarcoma. Can. J. Surg. 2004, 47, 383–384. [Google Scholar]
- Wolov, R.B.; Sato, N.; Azumi, N.; Lack, E.E. Intra-abdominal “angiosarcomatosis”. Report of two cases after pelvic irradiation. Cancer 1991, 67, 2275–2279. [Google Scholar] [CrossRef]
- Liu, D.S.H.; Smith, H.; Lee, M.M.W.; Djeric, M. Small intestinal angiosarcoma masquerading as an appendiceal abscess. Ann. R. Coll. Surg. Engl. 2013, 95, e22–e24. [Google Scholar] [CrossRef]
- Takahashi, M.; Ohara, M.; Kimura, N.; Hiromitsu, D.; Takumi, Y.; Kazuteru, K.; Takahiro, T.; Satoshi, H.; Nozomu, I. Giant primary angiosarcoma of the small intestine showing severe sepsis. World J. Gastroenterol. 2014, 20, 16359–16363. [Google Scholar] [CrossRef]
- Zacarias Föhrding, L.; Macher, A.; Braunstein, S.; Knoefel, W.T.; Topp, S.A. Small intestine bleeding due to multifocal angiosarcoma. World J. Gastroenterol. 2012, 18, 6494–6500. [Google Scholar] [CrossRef]
- Huntington, J.T.; Jones, C.; Liebner, D.A.; James, L.C.; Raphael, E.P. Angiosarcoma: A rare malignancy with protean clinical presentations. J. Surg. Oncol. 2015, 111, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Chahbouni, S.; Barnoud, R.; Watkin, E.; Devouassoux-Shisheboran, M. High-grade small bowel angiosarcoma associated with angiosarcomatosis: A case report. Ann. Pathol. 2011, 31, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Ryu, D.Y.; Hwang, S.Y.; Lee, D.W.; Kim, T.O.; Park, D.Y.; Kim, G.A.; Heo, J.; Kang, D.H.; Song, G.A.; Cho, M. A case of primary angiosarcoma of small intestine presenting as recurrent gastrointestinal bleeding. Korean J. Gastroenterol. 2005, 46, 404–408. [Google Scholar] [PubMed]
- Udager, A.M.; Ishikawa, M.K.; Lucas, D.R.; McHugh, J.B.; Patel, R.M. MYC immunohistochemistry in angiosarcoma and atypical vascular lesions: Practical considerations based on a single institutional experience. Pathology 2016, 48, 697–704. [Google Scholar] [CrossRef]
- Motaparthi, K.; Lauer, S.C.; Patel, R.M.; Vidal, I.C.; Linos, K. MYC gene amplification by fluorescence in situ hybridization and MYC protein expression by immunohistochemistry in the diagnosis of cutaneous angiosarcoma: Systematic review and appropriate use criteria. J. Cutan. Pathol. 2021, 48, 578–586. [Google Scholar] [CrossRef]
- Guo, T.; Zhang, L.; Chang, N.-E.; Singer, S.; Maki, R.G.; Antonescu, C.R. Consistent MYC and FLT4 Gene Amplification in Radiation-Induced Angiosarcoma but not in other Radiation-Associated Atypical Vascular Lesions. Genes Chromosomes Cancer 2011, 50, 25–33. [Google Scholar] [CrossRef] [Green Version]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Gatta, M.; Zorzetti, N.; Baccaro, C.; Manuela, C.; Fornelli, A.; Cennamo, V.; Navarra, G.G. Post-Radiation Angiosarcoma (PRA) of the Small Bowel: Report of a Case and Review of the Literature. Surgeries 2023, 4, 381-390. https://doi.org/10.3390/surgeries4030038
La Gatta M, Zorzetti N, Baccaro C, Manuela C, Fornelli A, Cennamo V, Navarra GG. Post-Radiation Angiosarcoma (PRA) of the Small Bowel: Report of a Case and Review of the Literature. Surgeries. 2023; 4(3):381-390. https://doi.org/10.3390/surgeries4030038
Chicago/Turabian StyleLa Gatta, Marco, Noemi Zorzetti, Cinzia Baccaro, Cuoghi Manuela, Adele Fornelli, Vincenzo Cennamo, and Giuseppe Giovanni Navarra. 2023. "Post-Radiation Angiosarcoma (PRA) of the Small Bowel: Report of a Case and Review of the Literature" Surgeries 4, no. 3: 381-390. https://doi.org/10.3390/surgeries4030038