
A Brief Overview of the Effects of Exercise and Red Beets on the Immune System in Patients with Prostate Cancer

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
1.1. Prevalence and Mortality
1.2. Factors Involved in PCa

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors Involved in PCa | Mechanisms Related to Factors Leading to PCa |
|---|---|
| Age | Older men are at higher risk of PCa than others. The prevalence of this cancer increases with age compared to other cancers [13]. PCa is less common in men under the age of 40 compared to men in their 50s [14]. Its prevalence increases after the age of 50, and 75% of PCa prevalence is observed in people over 65 years of age [15]. Pervasive data suggest that the number of men dying from PCa is increasing [16]. |
| Racial origin | Another known risk factor for PCa. According to epidemiological data, the prevalence of PCa varies between countries and ethnic differences [17]. Black people are more prone to PCa than white people, as well as Americans than Asians. In the same situation as living in the US, Ashkenazi and Icelandic Jews have a 31% higher incidence of early and more aggressive PCa, with mutations in genes such as BRCA2 [18]. |
| Genetics | Genetics is another important risk factor for PCa. Family history increases the risk of cancer, with approximately 9% of people with a family history having two or more relatives with PCa. Men with first-degree relatives with PCa are twice as likely to develop the disease [18]. |
| Androgens | Androgens are necessary for the growth, development, maintenance, and normal function of the prostate [19]. Androgen biosynthesis occurs in the testes and adrenal glands along with peripheral tissues such as the skin or prostate [20]. The two most important androgens in adult men are testosterone and its dependent metabolite, dihydrotestosterone [20]. Testosterone is the major circulating androgen that is essential for muscle mass growth, bone and cardiovascular health, sperm production regulation, and sexual function [21]. Dihydrotestosterone, on the other hand, is a functional androgen in prostate tissue and a major regulator of androgenic processes within the prostate, such as proliferation and cell differentiation [21]. In the prostate, dihydrotestosterone is made from testosterone by type 5 alpha-reductase activity [20]. Evidence supports the claim that androgens play an important role in PCa, and that high concentrations of circulating androgens are a risk factor for PCa [20]. |
| Insulin and insulin-like growth factors | In addition to androgens, other growth factors involved in regulating the growth of PCa cells are insulin and insulin-like growth factor-1 (IGF-1). IGF-1 is a peptide hormone involved in DNA synthesis, cell cycle stimulation, and the inhibition of cellular apoptosis [22]. In addition, it is a strong mitogen for normal and cancerous cells. Large amounts of IGF-1 are synthesized in the liver and released into the bloodstream, but some of them are produced locally within IGF-1-responsive tissues such as the prostate [23]. Thus, IGF-1 is regulated by the autocrine and paracrine mechanisms, and both mechanisms influence the action and production of IGF-1 [24]. Insulin can act as a growth factor and regulate cell differentiation, proliferation, and apoptosis [25]. The signaling pathway of insulin is similar to that of IGF-1 and its receptors; thus, these two mitogens can act similarly [26]. In the liver, insulin can stimulate IGF-1 synthesis and suppress insulin-like growth factor-binding proteins 1 and 2 (IGF-BP1 2), thus affecting the bioavailability of IGF-1 [27]. Insulin suppresses sex hormone-binding globulin (SHBG) production, which ultimately increases free testosterone levels, thus preparing the ground for PCa [28]. |
| Obesity | Obesity is associated with the onset and progression of several cancers, such as colon, pancreas, breast, and PCa [26,29,30]. In the US, obesity is estimated to account for 14% of all fatal cancers in men and 20% in women [31]. Figure 1 depicts the factors involved in PCa. |
2. Approach to Prevention, Control, and Treatment of PCa
2.1. Exercise Training
2.1.1. Recommended Exercise for the Treatment or Reduction of Cancer Complications
2.1.2. Mechanism of the Effect of Aerobic Exercise on PCa
2.2. Bioactive Compounds
Beetroot
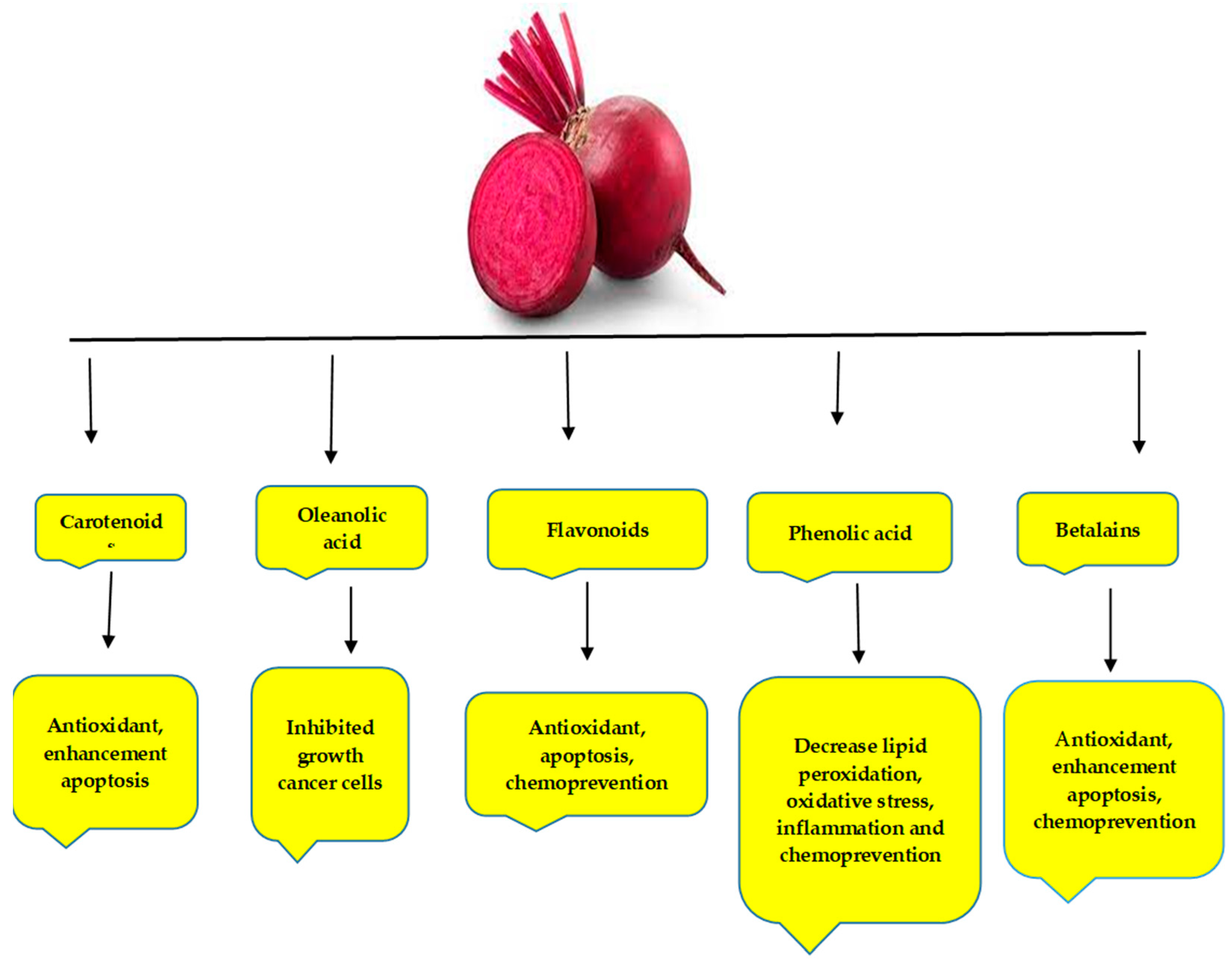
- Composition of Beetroot
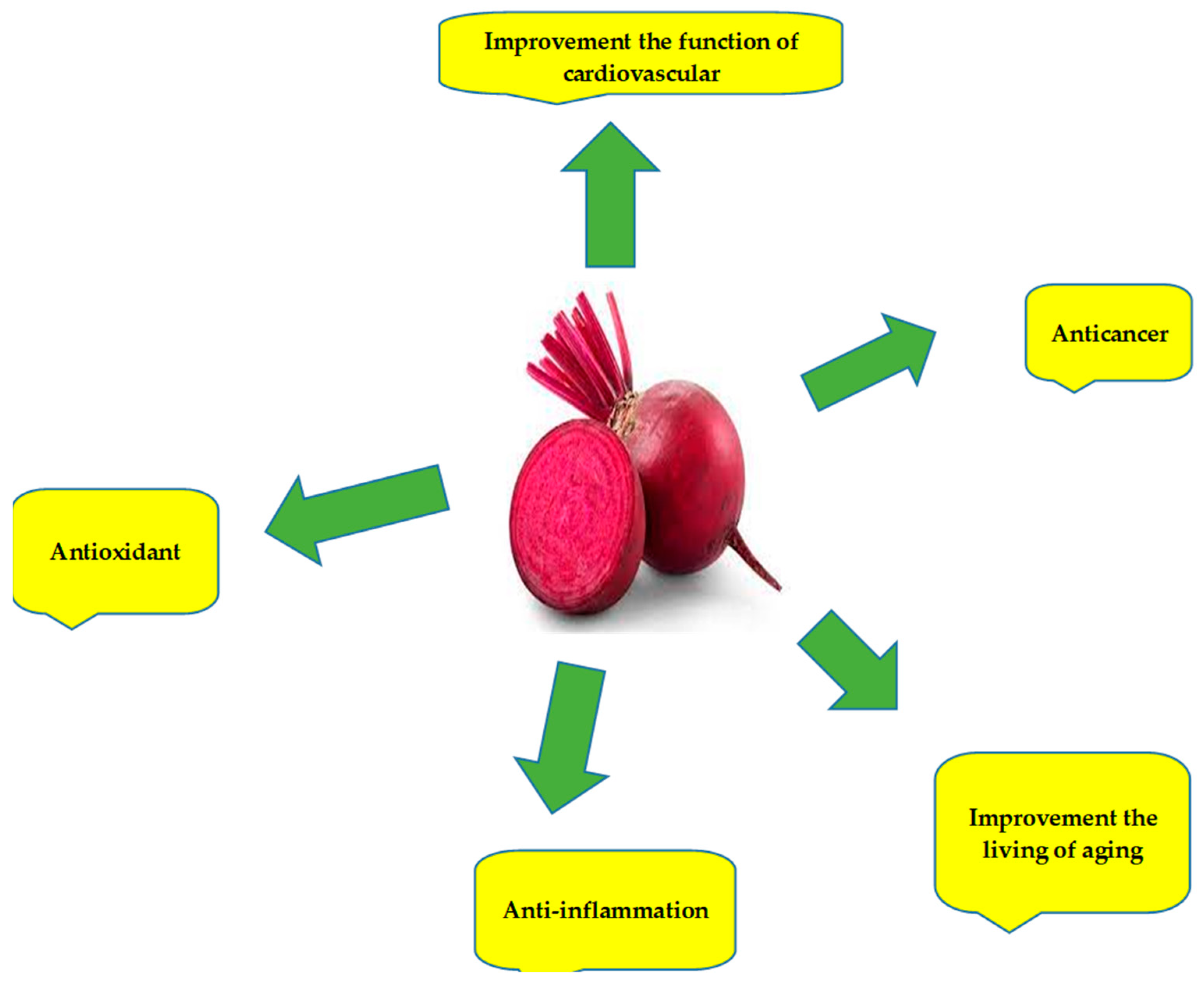
- Properties of Beetroot That Have Potentially Preventive Effects on Cancer
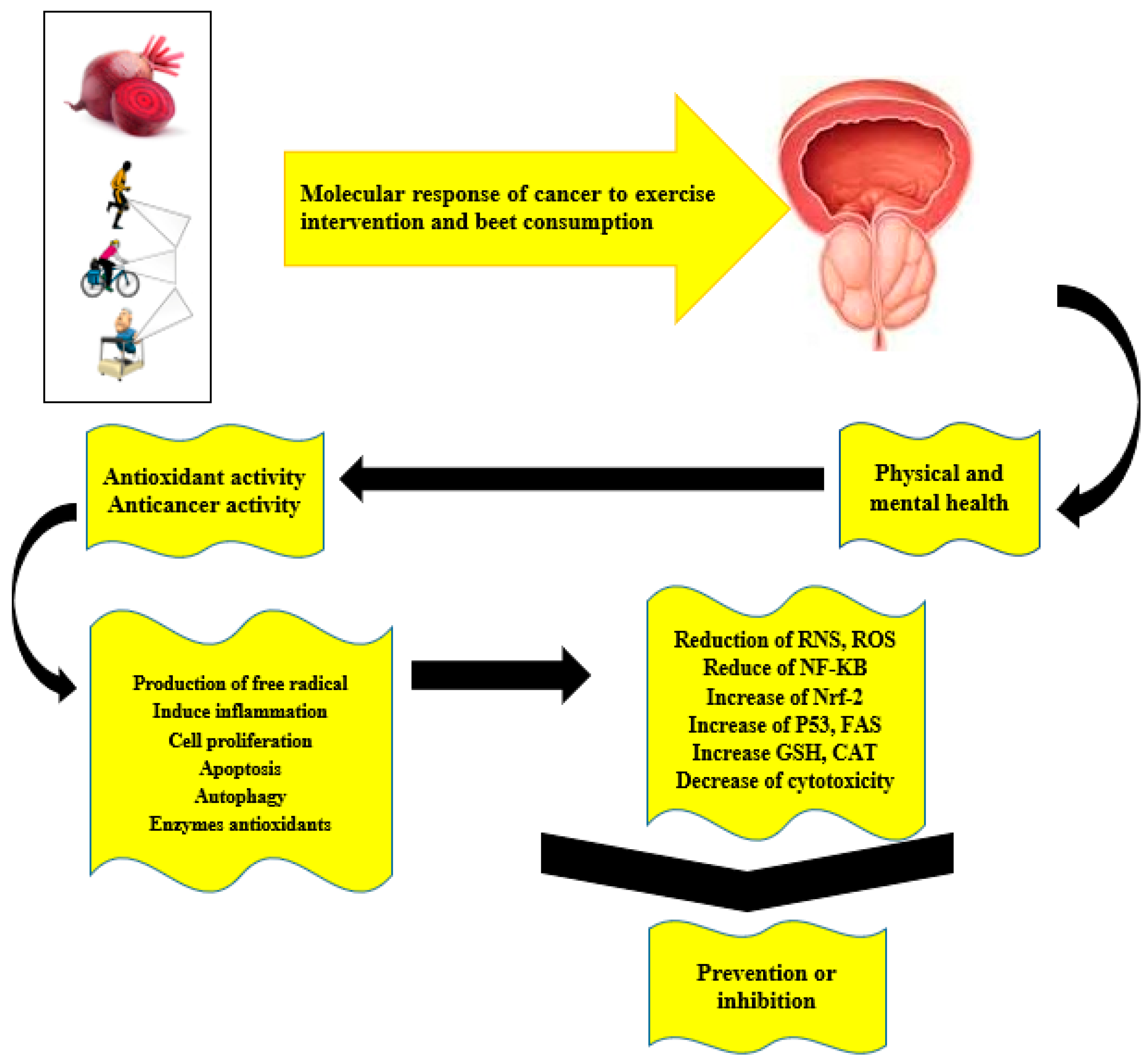
3. Use of Two the Beets Exercise Interventions in Individuals with Various Diseases, including Cancer
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P. Epidemiology of prostate cancer. World J. Oncol. 2019, 10, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christie, D.R.; Sharpley, C.F. How accurately can prostate gland imaging measure the prostate gland volume? Results of a systematic review. Prostate Cancer 2019, 2019, 6932572. [Google Scholar] [CrossRef] [PubMed]
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. The epidemiology of prostate cancer. Cold Spring Harb. Perspect. Med. 2018, 8, a030361. [Google Scholar] [CrossRef]
- Frank, S.J.; Grimm, P.D.; Sylvester, J.E.; Merrick, G.S.; Davis, B.J.; Zietman, A.; Moran, B.J.; Beyer, D.C.; Roach, M., III; Clarke, D.H. Interstitial implant alone or in combination with external beam radiation therapy for intermediate-risk prostate cancer: A survey of practice patterns in the United States. Brachytherapy 2007, 6, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Saedmocheshi, S.; Saghebjoo, M.; Vahabzadeh, Z.; Sheikholeslami-Vatani, D. Aerobic Training and Green Tea Extract Protect against NMU-induced Prostate Cancer. Med. Sci. Sports Exerc. 2019, 51, 2210–2216. [Google Scholar] [CrossRef]
- Vahabzadeh, Z.; Molodi, M.; Nikkho, B.; Saghebjoo, M.; Saedmocheshi, S.; Zamani, F.; Roshani, Y.; Babanzadeh, S. Aerobic training and hydroalcoholic extracts of green tea improve pro-oxidant-antioxidant balance and histopathological score in the N-methyl-N-nitrosourea-induced prostate cancer model of rat. EXCLI J. 2020, 19, 762. [Google Scholar]
- Hébert, J.R.; Hurley, T.G.; Harmon, B.E.; Heiney, S.; Hebert, C.J.; Steck, S.E. A diet, physical activity, and stress reduction intervention in men with rising prostate-specific antigen after treatment for prostate cancer. Cancer Epidemiol. 2012, 36, e128–e136. [Google Scholar] [CrossRef] [Green Version]
- Nobari, H.; Fashi, M.; Eskandari, A.; Pérez-Gómez, J.; Suzuki, K. Potential Improvement in Rehabilitation Quality of 2019 Novel Coronavirus by Isometric Training System; Is There "Muscle-Lung Cross-Talk"? Int. J. Environ. Res. Public Health 2021, 18, 6304. [Google Scholar] [CrossRef]
- Shams, A.; Nobari, H.; Afonso, J.; Abbasi, H.; Mainer-Pardos, E.; Pérez-Gómez, J.; Bayati, M.; Bahrami, A.; Carneiro, L. Effect of Aerobic-Based Exercise on Psychological Well-Being and Quality of Life Among Older People: A Middle East Study. Front. Public Health 2021, 9, 764044. [Google Scholar] [CrossRef]
- Nobari, H.; Rezaei, S.; Sheikh, M.; Fuentes-García, J.P.; Pérez-Gómez, J. Effect of Virtual Reality Exercises on the Cognitive Status and Dual Motor Task Performance of the Aging Population. Int. J. Environ. Res. Public Health 2021, 18, 8005. [Google Scholar] [CrossRef]
- Perdana, N.R.; Mochtar, C.A.; Umbas, R.; Hamid, A.R.A. The risk factors of prostate cancer and its prevention: A literature review. Acta Med. Indones. 2017, 48, 228–238. [Google Scholar]
- Nobari, H.; Nejad, H.A.; Kargarfard, M.; Mohseni, S.; Suzuki, K.; Carmelo Adsuar, J.; Pérez-Gómez, J. The Effect of Acute Intense Exercise on Activity of Antioxidant Enzymes in Smokers and Non-Smokers. Biomolecules 2021, 11, 171. [Google Scholar] [CrossRef] [PubMed]
- Nelen, V. Epidemiology of prostate cancer. In Prostate Cancer; Springer: Berlin/Heidelberg, Germany, 2007; pp. 1–8. [Google Scholar]
- Grönberg, H. Prostate cancer epidemiology. Lancet 2003, 361, 859–864. [Google Scholar] [CrossRef]
- Spickett, I.; Robertson, J. Prostate cancer: The ongoing challenge. Prim. Health Care 2010, 20, 16. [Google Scholar] [CrossRef]
- Dunn, M.W.; Kazer, M.W. Prostate cancer overview. In Proceedings of Seminars in Oncology Nursing; Elsevier: Amsterdam, The Netherlands; pp. 241–250.
- Paller, C.J.; Wang, L.; Brawley, O.W. Racial inequality in prostate cancer outcomes—socioeconomics, not biology. JAMA Oncol. 2019, 5, 983–984. [Google Scholar] [CrossRef]
- Harris, E.L. Genetic Inheritance of Cancer Risk: Applications to Cancer Screening. In Cancer Screening: Theory and Practice; CRC Press: Boca Raton, FL, USA, 2021; pp. 595–610. [Google Scholar] [CrossRef]
- Jadvar, H.; Desai, B.; Ji, L.; Conti, P.S.; Dorff, T.B.; Groshen, S.G.; Gross, M.E.; Pinski, J.K.; Quinn, D.I. Prospective evaluation of 18F-NaF and 18F-FDG PET/CT in detection of occult metastatic disease in biochemical recurrence of prostate cancer. Clin. Nucl. Med. 2012, 37, 637. [Google Scholar] [CrossRef] [Green Version]
- Hsing, A.W.; Wang, R.-T.; Gu, F.-L.; Lee, M.; Wang, T.; Leng, T.J.; Spitz, M.; Blot, W.J. Vasectomy and prostate cancer risk in China. Cancer Epidemiol. Prev. Biomark. 1994, 3, 285–288. [Google Scholar]
- Vis, A.N.; Schröder, F.H. Key targets of hormonal treatment of prostate cancer. Part 1: The androgen receptor and steroidogenic pathways. BJU Int. 2009, 104, 438–448. [Google Scholar] [CrossRef]
- Lima, G.A.B.; Corrêa, L.L.; Gabrich, R.; de Miranda, L.C.D.; Gadelha, M.R. IGF-I, insulin and prostate cancer. Arq. Bras. Endocrinol. Metabol. 2009, 53, 969–975. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, M.; Paolisso, G.; Kimura, M.; Gardner, J.P.; Boccardi, V.; Papa, M.; Hjelmborg, J.V.; Christensen, K.; Brimacombe, M.; Nawrot, T.S. Higher circulating levels of IGF-1 are associated with longer leukocyte telomere length in healthy subjects. Mech. Ageing Dev. 2009, 130, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Berkel, H.; Yu, H. Insulin-like growth factor-I and prostate cancer: A meta-analysis. Br. J. Cancer 2001, 85, 991. [Google Scholar] [CrossRef] [PubMed]
- Nandeesha, H. Insulin: A novel agent in the pathogenesis of prostate cancer. Int. Urol. Nephrol. 2009, 41, 267. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Michaud, D. The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology 2007, 132, 2208–2225. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.M.; Rimm, E.B.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 1994, 17, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Leung, P.-S.; Aronson, W.J.; Ngo, T.H.; Golding, L.A.; Barnard, R.J. Exercise alters the IGF axis in vivo and increases p53 protein in prostate tumor cells in vitro. J. Appl. Physiol. 2004, 96, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Zuniga, K.B.; Chan, J.M.; Ryan, C.J.; Kenfield, S.A. Diet and lifestyle considerations for patients with prostate cancer. Urol. Oncol. 2020, 38, 105–117. [Google Scholar] [CrossRef]
- Nobari, H.; Gandomani, E.E.; Reisi, J.; Vahabidelshad, R.; Suzuki, K.; Volpe, S.L.; Pérez-Gómez, J. Effects of 8 Weeks of High-Intensity Interval Training and Spirulina Supplementation on Immunoglobin Levels, Cardio-Respiratory Fitness, and Body Composition of Overweight and Obese Women. Biology 2022, 11, 196. [Google Scholar] [CrossRef]
- Kalender, A.; Selvaraj, A.; Kim, S.Y.; Gulati, P.; Brûlé, S.; Viollet, B.; Kemp, B.E.; Bardeesy, N.; Dennis, P.; Schlager, J.J. Metformin, independent of AMPK, inhibits mTORC1 in a rag GTPase-dependent manner. Cell Metab. 2010, 11, 390–401. [Google Scholar] [CrossRef] [Green Version]
- Nobari, H.; Fashi, M.; Eskandari, A.; Villafaina, S.; Murillo-Garcia, Á.; Pérez-Gómez, J. Effect of COVID-19 on Health-Related Quality of Life in Adolescents and Children: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4563. [Google Scholar] [CrossRef]
- Cooke, P.S.; Selvaraj, V.; Yellayi, S. Genistein, estrogen receptors, and the acquired immune response. J. Nutr. 2006, 136, 704–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvao, D.A.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Chee, R.; Peddle-Mcintyre, C.J.; Hart, N.H.; Baumann, F.T. Exercise preserves physical function in prostate cancer patients with bone metastases. Med. Sci. Sports Exerc. 2018, 50, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvão, D.A.; Nosaka, K.; Taaffe, D.R.; Peake, J.; Spry, N.; Suzuki, K.; Yamaya, K.; McGuigan, M.R.; Kristjanson, L.J.; Newton, R.U. Endocrine and immune responses to resistance training in prostate cancer patients. Prostate Cancer Prostatic Dis. 2008, 11, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Na, H.-K.; Surh, Y.-J. Modulation of Nrf2-mediated antioxidant and detoxifying enzyme induction by the green tea polyphenol EGCG. Food Chem. Toxicol. 2008, 46, 1271–1278. [Google Scholar] [CrossRef]
- Baudot, A.; Barth, N.; Colas, C.; Garros, M.; Garcin, A.; Oriol, M.; Roche, F.; Chauvin, F.; Mottet, N.; Hupin, D. The physical activity experience of prostate cancer patients: A multicentre peer motivation monitoring feasibility study. The Acti-Pair study. Pilot Feasibility Stud. 2022, 8, 12. [Google Scholar] [CrossRef]
- Galvao, D.A.; Nosaka, K.; Taaffe, D.R.; Spry, N.; Kristjanson, L.J.; McGuigan, M.R.; Suzuki, K.; Yamaya, K.; Newton, R.U. Resistance training and reduction of treatment side effects in prostate cancer patients. Med. Sci. Sports Exerc. 2006, 38, 2045–2052. [Google Scholar] [CrossRef]
- Liu, H.-W.; Chang, S.-J. Moderate exercise suppresses NF-κB signaling and activates the SIRT1-AMPK-PGC1a axis to attenuate muscle loss in diabetic db/db mice. Front. Physiol. 2018, 9, 636. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Medysky, M.E.; Campbell, K.L.; Bland, K.A.; Winters-Stone, K.M. Attention to the principles of exercise training in exercise studies on prostate cancer survivors: A systematic review. BMC Cancer 2019, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zhou, W. Roles and molecular mechanisms of physical exercise in cancer prevention and treatment. J. Sport Health Sci. 2021, 10, 201–210. [Google Scholar] [CrossRef]
- Nobari, H.; Ahmadi, M.; Sá, M.; Pérez-Gómez, J.; Clemente, F.M.; Adsuar, J.C.; Minasian, V.; Afonso, J. The effect of two types of combined training on bio-motor ability adaptations in sedentary females. J. Sports Med. Phys. Fit. 2021, 61, 1317–1325. [Google Scholar] [CrossRef]
- Hausmann, F.; Iversen, V.; Kristoffersen, M.; Gundersen, H.; Johannsson, E.; Vika, M. Combined aerobic and resistance training improves physical capacity in women treated for gynecological cancer. Support. Care Cancer 2018, 26, 3389–3396. [Google Scholar] [CrossRef] [PubMed]
- Segal, R.; Zwaal, C.; Green, E.; Tomasone, J.; Loblaw, A.; Petrella, T. Exercise for people with cancer: A clinical practice guideline. Curr. Oncol. 2017, 24, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buffart, L.M.; Sweegers, M.G.; May, A.M.; Chinapaw, M.J.; Van Vulpen, J.K.; Newton, R.U.; Galvão, D.A.; Aaronson, N.K.; Stuiver, M.M.; Jacobsen, P.B. Targeting exercise interventions to patients with cancer in need: An individual patient data meta-analysis. JNCI J. Natl. Cancer Inst. 2018, 110, 1190–1200. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Winters-Stone, K.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.; Matthews, C.; Ligibel, J.; Gerber, L. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, T.; Howatson, G.; West, D.J.; Stevenson, E.J. The potential benefits of red beetroot supplementation in health and disease. Nutrients 2015, 7, 2801–2822. [Google Scholar] [CrossRef]
- Rundqvist, H.; Johnson, R. Tumour oxygenation: Implications for breast cancer prognosis. J. Intern. Med. 2013, 274, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Santa Mina, D.; Alibhai, S.M.; Matthew, A.G.; Guglietti, C.L.; Pirbaglou, M.; Trachtenberg, J.; Ritvo, P. A randomized trial of aerobic versus resistance exercise in prostate cancer survivors. J. Aging Phys. Act. 2013, 21, 455–478. [Google Scholar] [CrossRef] [Green Version]
- Soliman, S.; Aronson, W.J.; Barnard, R.J. Analyzing serum-stimulated prostate cancer cell lines after low-fat, high-fiber diet and exercise intervention. Evid.-Based Complement. Altern. Med. 2011, 2011, 529053. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.E.; Vollaard, N.B.; Choueiri, T.; Wilson, M. Exercise, free radicals and oxidative stress. Biochem. Soc. Trans. 2002, 30, 280–285. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Richart, S.M. White blood cell counts mediate the effects of physical activity on prostate-specific antigen levels. Res. Q. Exerc. Sport 2014, 85, 409–413. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, J.A.; Wilund, K.R.; Martin, S.A.; Kistler, B.M. Exercise, inflammation and aging. Aging Dis. 2012, 3, 130. [Google Scholar] [PubMed]
- Guéritat, J.; Lefeuvre-Orfila, L.; Vincent, S.; Cretual, A.; Ravanat, J.-L.; Gratas-Delamarche, A.; Rannou-Bekono, F.; Rébillard, A. Exercise training combined with antioxidant supplementation prevents the antiproliferative activity of their single treatment in prostate cancer through inhibition of redox adaptation. Free Radic. Biol. Med. 2014, 77, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Antonelli, J.; Masko, E.M.; Broadwater, G.; Lascola, C.D.; Fels, D.; Dewhirst, M.W.; Dyck, J.R.; Nagendran, J.; Flores, C.T. Exercise modulation of the host-tumor interaction in an orthotopic model of murine prostate cancer. J. Appl. Physiol. 2012, 113, 263–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourke, L.; Smith, D.; Steed, L.; Hooper, R.; Carter, A.; Catto, J.; Albertsen, P.C.; Tombal, B.; Payne, H.A.; Rosario, D.J. Exercise for men with prostate cancer: A systematic review and meta-analysis. Eur. Urol. 2016, 69, 693–703. [Google Scholar] [CrossRef] [Green Version]
- Torti, D.C.; Matheson, G.O. Exercise and prostate cancer. Sports Med. 2004, 34, 363–369. [Google Scholar] [CrossRef]
- Mehra, K.; Berkowitz, A.; Sanft, T. Diet, physical activity, and body weight in cancer survivorship. Med. Clin. 2017, 101, 1151–1165. [Google Scholar] [CrossRef]
- Liu, R.H. Health benefits of fruit and vegetables are from additive and synergistic combinations of phytochemicals. Am. J. Clin. Nutr. 2003, 78, 517S–520S. [Google Scholar] [CrossRef]
- Lampe, J.W. Health effects of vegetables and fruit: Assessing mechanisms of action in human experimental studies. Am. J. Clin. Nutr. 1999, 70, 475s–490s. [Google Scholar] [CrossRef]
- Cai, Y.; Sun, M.; Corke, H. Antioxidant activity of betalains from plants of the Amaranthaceae. J. Agric. Food Chem. 2003, 51, 2288–2294. [Google Scholar] [CrossRef]
- Stintzing, F.C.; Carle, R. Functional properties of anthocyanins and betalains in plants, food, and in human nutrition. Trends Food Sci. Technol. 2004, 15, 19–38. [Google Scholar] [CrossRef]
- Kapadia, G.J.; Azuine, M.A.; Subba Rao, G.; Arai, T.; Iida, A.; Tokuda, H. Cytotoxic effect of the red beetroot (Beta vulgaris L.) extract compared to doxorubicin (Adriamycin) in the human prostate (PC-3) and breast (MCF-7) cancer cell lines. Anti-Cancer Agents Med. Chem. 2011, 11, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.C.S.; Ponte, L.G.S.; Silva, C.H.R.; Fagundes, I.; Pavan, I.C.B.; Romeiro, S.A.; da Silva, L.G.S.; Morelli, A.P.; Rostagno, M.A.; Simabuco, F.M. Beetroot and leaf extracts present protective effects against prostate cancer cells, inhibiting cell proliferation, migration, and growth signaling pathways. Phytother. Res. 2021, 35, 5241–5258. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.F.; Stoner, G.D. Red beetroot and betalains as cancer chemopreventative agents. Molecules 2019, 24, 1602. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.; Shi, J.; Xie, S.-Y.; Zhang, T.-Y.; Soladoye, O.P.; Aluko, R.E. Red beetroot betalains: Perspectives on extraction, processing, and potential health benefits. J. Agric. Food Chem. 2020, 68, 11595–11611. [Google Scholar] [CrossRef] [PubMed]
- Hadipour, E.; Taleghani, A.; Tayarani-Najaran, N.; Tayarani-Najaran, Z. Biological effects of red beetroot and betalains: A review. Phytother. Res. 2020, 34, 1847–1867. [Google Scholar] [CrossRef]
- Ravichandran, K.; Saw, N.M.M.T.; Mohdaly, A.A.; Gabr, A.M.; Kastell, A.; Riedel, H.; Cai, Z.; Knorr, D.; Smetanska, I. Impact of processing of red beet on betalain content and antioxidant activity. Food Res. Int. 2013, 50, 670–675. [Google Scholar] [CrossRef]
- Ahmad, R.; Ahmad, N.; Naqvi, A.A.; Shehzad, A.; Al-Ghamdi, M.S. Role of traditional Islamic and Arabic plants in cancer therapy. J. Tradit. Complement. Med. 2017, 7, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Sárváry, A.; Sárváry, A. Use of complementary and alternative medicine among breast cancer patients in Hungary: A descriptive study. Complement. Ther. Clin. Pract. 2019, 35, 195–200. [Google Scholar] [CrossRef]
- Milton-Laskibar, I.; Martínez, J.A.; Portillo, M.P. Current Knowledge on Beetroot Bioactive Compounds: Role of Nitrate and Betalains in Health and Disease. Foods 2021, 10, 1314. [Google Scholar] [CrossRef]
- Banez, M.J.; Geluz, M.I.; Chandra, A.; Hamdan, T.; Biswas, O.S.; Bryan, N.S.; Von Schwarz, E.R. A systemic review on the antioxidant and anti-inflammatory effects of resveratrol, curcumin, and dietary nitric oxide supplementation on human cardiovascular health. Nutr. Res. 2020, 78, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, G.J.; Rao, G.S. Anticancer effects of red beet pigments. In Red Beet Biotechnology; Springer: Berlin/Heidelberg, Germany, 2013; pp. 125–154. [Google Scholar]
- Da Silva, L.G.S.; Morelli, A.P.; Pavan, I.C.B.; Tavares, M.R.; Pestana, N.F.; Rostagno, M.A.; Simabuco, F.M.; Bezerra, R.M.N. Protective effects of beet (Beta vulgaris) leaves extract against oxidative stress in endothelial cells in vitro. Phytother. Res. 2020, 34, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.L.; Hamid, S.B.S. Beetroot as a Potential Functional Food for Cancer Chemoprevention, a Narrative Review. J. Cancer Prev. 2021, 26, 17. [Google Scholar] [CrossRef] [PubMed]
- El Gamal, A.A.; AlSaid, M.S.; Raish, M.; Al-Sohaibani, M.; Al-Massarani, S.M.; Ahmad, A.; Hefnawy, M.; Al-Yahya, M.; Basoudan, O.A.; Rafatullah, S. Beetroot (Beta vulgaris L.) extract ameliorates gentamicin-induced nephrotoxicity associated oxidative stress, inflammation, and apoptosis in rodent model. Mediat. Inflamm. 2014, 2014, 983952. [Google Scholar] [CrossRef] [Green Version]
- Yi, E.-Y.; Kim, Y.-J. Betaine inhibits in vitro and in vivo angiogenesis through suppression of the NF-κB and Akt signaling pathways. Int. J. Oncol. 2012, 41, 1879–1885. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Zhu, Y.; Hu, Z.; Wu, S.; Jin, C. Beetroot as a functional food with huge health benefits: Antioxidant, antitumor, physical function, and chronic metabolomics activity. Food Sci. Nutr. 2021, 9, 6406–6420. [Google Scholar] [CrossRef]
- Das, S.; Filippone, S.M.; Williams, D.S.; Das, A.; Kukreja, R.C. Beet root juice protects against doxorubicin toxicity in cardiomyocytes while enhancing apoptosis in breast cancer cells. Mol. Cell. Biochem. 2016, 421, 89–101. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Gkiouras, K.; Papageorgiou, S.Τ.; Myrogiannis, I.; Mykoniatis, I.; Papamitsou, T.; Bogdanos, D.P.; Goulis, D.G. Dietary Factors and Supplements Influencing Prostate-Specific Antigen (PSA) Concentrations in Men with Prostate Cancer and Increased Cancer Risk: An Evidence Analysis Review Based on Randomized Controlled Trials. Nutrients 2020, 12, 2985. [Google Scholar] [CrossRef]
- Barnes, M.S.; Cassidy, T. Diet, exercise and motivation in weight reduction: The role of psychological capital and stress: Diet, exercise and motivation in weight reduction. JOJ Nurse Health Care 2018, 9, 5. [Google Scholar]
- Crawford-Williams, F.; March, S.; Goodwin, B.C.; Ralph, N.; Galvao, D.A.; Newton, R.U.; Chambers, S.K.; Dunn, J. Interventions for prostate cancer survivorship: A systematic review of reviews. Psycho-Oncol. 2018, 27, 2339–2348. [Google Scholar] [CrossRef] [Green Version]
- Dufresne, S.; Guéritat, J.; Chiavassa, S.; Noblet, C.; Assi, M.; Rioux-Leclercq, N.; Rannou-Bekono, F.; Lefeuvre-Orfila, L.; Paris, F.; Rébillard, A. Exercise training improves radiotherapy efficiency in a murine model of prostate cancer. FASEB J. 2020, 34, 4984–4996. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.C.; Allen, K.; Deer, R.R.; Lyons, E.J.; Swartz, M.D.; Clifford, T. A narrative review on the potential of red beetroot as an adjuvant strategy to counter fatigue in children with cancer. Nutrients 2019, 11, 3003. [Google Scholar] [CrossRef] [Green Version]
- Woessner, M.N.; McIlvenna, L.C.; Ortiz de Zevallos, J.; Neil, C.J.; Allen, J.D. Dietary nitrate supplementation in cardiovascular health: An ergogenic aid or exercise therapeutic? Am. J. Physiol.-Heart Circ. Physiol. 2018, 314, H195–H212. [Google Scholar] [CrossRef]
- Van der Avoort, C.M.; van Loon, L.J.; Verdijk, L.B.; Poyck, P.P.; Thijssen, D.T.; Hopman, M.T. Acute Effects of Dietary Nitrate on Exercise Tolerance, Muscle Oxygenation, and Cardiovascular Function in Patients with Peripheral Arterial Disease. Int. J. Sport Nutr. Exerc. Metab. 2021, 31, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.K.; Alexander-Lindo, R.L.; Nair, M.G. Relative inhibition of lipid peroxidation, cyclooxygenase enzymes, and human tumor cell proliferation by natural food colors. J. Agric. Food Chem. 2005, 53, 9268–9273. [Google Scholar] [CrossRef] [PubMed]
- Sreekanth, D.; Arunasree, M.; Roy, K.R.; Reddy, T.C.; Reddy, G.V.; Reddanna, P. Betanin a betacyanin pigment purified from fruits of Opuntia ficus-indica induces apoptosis in human chronic myeloid leukemia Cell line-K562. Phytomedicine 2007, 14, 739–746. [Google Scholar] [CrossRef]
- Westerlind, K.; McCarty, H.; Gibson, K.; Strange, R. Effect of exercise on the rat mammary gland: Implications for carcinogenesis. Acta Physiol. Scand. 2002, 175, 147–156. [Google Scholar] [CrossRef]
- Cohen, L.A.; Boylan, E.; Epstein, M.; Zang, E. Voluntary exercise and experimental mammary cancer. Exerc. Calor. Fat Cancer 1992, 322, 41–59. [Google Scholar]
- Irwin, M.L.; Varma, K.; Alvarez-Reeves, M.; Cadmus, L.; Wiley, A.; Chung, G.G.; DiPietro, L.; Mayne, S.T.; Yu, H. Randomized controlled trial of aerobic exercise on insulin and insulin-like growth factors in breast cancer survivors: The Yale Exercise and Survivorship study. Cancer Epidemiol. Prev. Biomark. 2009, 18, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Wang, W. Potential mechanisms of cancer prevention by weight control. Biophys. Rev. Lett. 2008, 3, 421–437. [Google Scholar] [CrossRef] [Green Version]
- Han, Y. Analysis of the role of the Hippo pathway in cancer. J. Transl. Med. 2019, 17, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigley, A.B.; Spielmann, G.; LaVoy, E.C.; Simpson, R.J. Can exercise-related improvements in immunity influence cancer prevention and prognosis in the elderly? Maturitas 2013, 76, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Gleeson, M.; Woods, J.A.; Bishop, N.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goete, L. Position statement part one: Immune function and exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar] [PubMed]
- Esatbeyoglu, T.; Wagner, A.E.; Schini-Kerth, V.B.; Rimbach, G. Betanin—A food colorant with biological activity. Mol. Nutr. Food Res. 2015, 59, 36–47. [Google Scholar] [CrossRef]
- Lee, M.; Lin, W.; Wang, S.; Lin, L.; Yu, B.; Lee, T. Evaluation of potential antioxidant and anti-inflammatory effects of Antrodia cinnamomea powder and the underlying molecular mechanisms via Nrf2-and NF-κB-dominated pathways in broiler chickens. Poult. Sci. 2018, 97, 2419–2434. [Google Scholar] [CrossRef]
- Baker, R.; Hayden, M.; Ghosh, G. NF-κB, inflammation, and metabolic disease. Cell Met. 2011, 13, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Kapadia, G.J.; Rao, G.S.; Ramachandran, C.; Iida, A.; Suzuki, N.; Tokuda, H. Synergistic cytotoxicity of red beetroot (Beta vulgaris L.) extract with doxorubicin in human pancreatic, breast and prostate cancer cell lines. J. Complement. Integr. Med. 2013, 10, 113–122. [Google Scholar] [CrossRef]
- Suzuki, K. Chronic inflammation as an immunological abnormality and effectiveness of exercise. Biomolecules 2019, 9, 223. [Google Scholar] [CrossRef] [Green Version]




| Author (s) | Intervention | Sample | Results |
|---|---|---|---|
| Saedmocheshi et al. [5] | Five days a week, moderate-intensity aerobic exercise for eight weeks (low- to moderate-intensity aerobic exercise training on the treadmill, 5 d·week−1 for 45 min·d−1 (15 min work in three sets, interspersed 2-min rest periods between sets). | Rats | Decreased inflammatory factors (NF-κB), weight loss, prostate weight loss |
| Vahabzadeh et al. [6] | Five days a week, moderate-intensity aerobic exercise for eight weeks (low- to moderate-intensity aerobic exercise training on the treadmill, 5 d·week−1 for 45 min·d−1 (15 min work in three sets, interspersed 2-min rest periods between sets). | Rats | Improves oxidant/antioxidant balance |
| Guéritat et al. [55] | Five days a week of moderate-intensity aerobic exercise for four weeks (5 days a week in the afternoon, one week with 15 min at 20 m/min, two weeks with 40 min at 22 m/min, and 60 min at intensity of 25 m/min for two weeks) | Rats | Decreased cancer cell differentiation in prostate tissue, increased antioxidant defense in prostate tissue |
| Mancini et al. [65] | Beetroot (betalains and flavonoids). Treatment with 100 μg/mL of beetroot extract | DU-145 and PC-3 prostate cancer cell lines | Important anti-cancer effects against prostate cancer cells |
| Kapadia et al. [100,101] | Red beetroot (B. vulgaris L.) extract was described as red beetroot extract diluted with Dextrin, rendered acidic with citric acid, pH 5.4, and stabilized with ascorbic acid, Batch Number GA01 with specification: λmax 530.0–536.0 nm with 1.6 min absorbance. | Human prostate cancer cells | Cytotoxicity exhibited by the red beetroot extract |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nobari, H.; Saedmocheshi, S.; Johnson, K.; Suzuki, K.; Maynar-Mariño, M. A Brief Overview of the Effects of Exercise and Red Beets on the Immune System in Patients with Prostate Cancer. Sustainability 2022, 14, 6492. https://doi.org/10.3390/su14116492
Nobari H, Saedmocheshi S, Johnson K, Suzuki K, Maynar-Mariño M. A Brief Overview of the Effects of Exercise and Red Beets on the Immune System in Patients with Prostate Cancer. Sustainability. 2022; 14(11):6492. https://doi.org/10.3390/su14116492
Chicago/Turabian StyleNobari, Hadi, Saber Saedmocheshi, Kelly Johnson, Katsuhiko Suzuki, and Marcos Maynar-Mariño. 2022. "A Brief Overview of the Effects of Exercise and Red Beets on the Immune System in Patients with Prostate Cancer" Sustainability 14, no. 11: 6492. https://doi.org/10.3390/su14116492