
Flywheel Training in Older Adults—A Systematic Review



1
Faculty of Sport, University Union, 18000 Belgrade, Serbia
2
Faculty of Kinesiology, University of Zagreb, 10000 Zagreb, Croatia
3
Faculty of Sport and Physical Education, University of Niš, 18000 Niš, Serbia
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(7), 4137; https://doi.org/10.3390/su14074137
Submission received: 16 February 2022
/
Revised: 27 March 2022
/
Accepted: 28 March 2022
/
Published: 30 March 2022
(This article belongs to the Special Issue Physical Activity and Behavior: Training and Education Models for Sustainable Health and Performance)
Abstract
:The process of healthy aging might be reconsidered, based on the nonfatal outcomes of falls in older adults. Flywheel training is a relatively new training method used by different age groups, which enables the muscles to contract at maximum force in minimum time. The study aim was to summarize the relevant literature about the effects of flywheel training in older adults and to determine its efficiency and feasibility. PRISMA guidelines were followed for both the search and analysis. Electronic databases (Google Scholar, PubMed, Science Direct, Scopus, Web of Science and SPORTDiscuss) yielded 9915 studies, but we have included studies published in English between 2005 and 2021, cross-sectional and pre-post treatments, with older adults (≥60 years) as the sample, where flywheel training was conducted. A total of nine studies have met the pre-defined criteria and entered the systematic review, with a total of 216 participants, both male and female. After analyzing the obtained results, it can be concluded that flywheel training showed physical, neuromuscular, and functional improvements in older adults. However, the review did not reveal an optimal duration, frequency, intensity, or volume. Furthermore, it can be stated that this training method can be considered as an appropriate form of activity in older adults, as a tool for improving overall health.
1. Introduction
It is estimated that the number of older adults, who are 60 years and older, will double by 2050 [1]. Since the population is aging, the importance of investigating methods that promote healthy aging is rising, especially regarding the individual’s abilities to perform daily tasks, their functionality, and quality of life [2]. The World Health Organization (WHO) emphasizes that the key to healthy aging is maintaining functional and cognitive abilities, which includes the ability to satisfy basic needs, learn, grow, make decisions, stay mobile, build relationships, and contribute to society [3]. Muscle strength and power are generally reducing with age, causing less daily activity and lower functional abilities [4]. The aging process consists of a progressive decline in neuromuscular function, higher risk of falling and bone fracturing, and functional abilities disturbance, as well as losing independence [5]. Regardless of the statistical data, the aging process often includes physiological and neuromuscular changes. The progressive decline of strength that comes with age (which typically accelerates after 65 years) might expose elderly people to falls, due to the strong correlation of strength with the speed of walking, dynamic balance, and endurance [6]. Some of the nonfatal outcomes of falls, such as bone fracturing, depression, immobilization, and social isolation in older adults, might question the process of healthy aging [3].
Luckily, different types of exercise interventions can either completely reverse or, at least, mitigate health declining which comes with age [7]. Exercise has various benefits for older adults, including physical strength and muscle coordination and control improvement [8]. It is well-known that these effects contribute to improved preventive fall strategies and improved functional performance [9]. However, effectiveness of different strategies depend also on the activity level of an individual [3]. Additionally, as the aging process is associated with a consistent and progressive decline in muscle mass, strength, and power, the appropriate exercise interventions targeted at the aforementioned abilities might slow down the aging process.
Flywheel training is a relatively new training method used by different age groups [10]. Using a flywheel enables the muscles to contract at maximum force in minimum time [11]. This isoinertial type of resistance facilitates optimal muscle force generation throughout all the angles of a movement [12]. Among the methods that emphasize the eccentric action, isoinertial devices, which are based on the Flywheel Paradigm [13], should be highlighted. This paradigm implies that the force applied during the concentric phase of the movement unwinds a cord/strap connected to a shaft with the rotating flywheel, which starts to rotate and store energy. Kinetic energy will increase as a function of the inertial load used, and the rotational speed is achieved. Once the whole range of motion of the concentric action is performed, the cord/strap rewinds, and the person must resist the pull of the rotating flywheel/s by performing a braking eccentric muscle action [14]. If the movement is performed correctly (delaying the braking action to the last phases of the eccentric action), flywheel devices allow to produce the so-called eccentric overload [15].
There are a number of studies about flywheel training in different athletes’ groups [16,17,18,19]. In addition, an adequate choice of intensity and volume is crucial, with the optimal duration of the experimental program and the choice of exercises being adapted to older adults [20]. According to the above-given facts, flywheel training is gaining importance. However, according to the authors’ knowledge, there are no studies that have summarized the previous studies in one place, especially in older adults. Therefore, the aim of this study is to summarize the relevant literature about the effects of flywheel training in older adults and, on the basis of the same, to determine its efficiency and feasibility in the mentioned population.
2. Materials and Methods
2.1. Literature Identification
Studies were searched and analyzed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [21,22], along with the registration number 26-06-01/2020-1. The research included studies conducted from 2005 to 2021, the search was conducted until 31 December 2021, and the final reconsideration was done on January 2022. Likewise, the literature relevant for this type of research, available with the following databases: Google Scholar, PubMed, Science Direct, Scopus, Web of Science, and SPORTDiscuss.
The following keywords were used to search for the articles reporting on the usage of flywheel training in older adults: (“flywheel training” OR “flywheel treatment” OR “eccentric training”) AND (“exercise” OR “physical activity” OR “strength” OR “endurance”) AND (“aerobic exercise” OR “cycle type”) AND (“older adults” OR “elderly” OR “aging” OR “older women” OR “older men”).
In order to include the relevant studies and analyze the obtained data, a descriptive method was used. Likewise, to increase sensitivity, we had to adapt to the particular database. The sensitivity, i.e., the search filters in every database, were based on year of publication, which was set from 2005 until 2021. Then, there were the extracted studies published in English (pre-post treatments and cross-sectional studies), with a sample of participants older than 60 years. After a detailed identification process, studies were considered to be relevant if they met the inclusion criteria.
The search for studies were accordingly of their value, and data extraction was conducted independently by two authors (D.Đ and M.S.), and the lists of references from previously assessed and original research were also reviewed. After that, each author cross-examined the found works, which were then taken for further analysis or rejected.
2.2. Inclusion Criteria
In order for the study to be included in the final analysis, it had to meet the following criteria: published studies between 2005 and 2021, which were randomized, with non-randomized controlled studies and intervention studies; the studies had to be published in English, the sample of participants had to be older adults (≥60 years), and flywheel training had to have been conducted. Eligibility criteria were also presented in the Table 1, according to the PICOS model for eligibility criteria (participant, intervention, control, outcome, and study design).
2.3. Exclusion Criteria
The exclusion criteria were related to studies conducted before 2005, studies that were written in a language other than English, and studies with participants younger than 60 years, as well as studies that had any other training regime except the flywheel.
2.4. Bias Risk Assessment
The risk of bias was assessed according to the PRISMA guidelines, that is, using the PEDro scale [23] to determine the quality of reviewed studies and the potential risk of bias (Table 2). Two independent authors (D.Ð. and M.S.) assessed the quality and risk of bias using checklists. Concordance between reviewers was estimated using k-statistics data to review the full text and assess relativity and risk of bias. In case of discordance in the findings of the risk of bias assessment, the obtained data were assessed by the third reviewer (D.P.), who also gave the final decision. The k rate of concordance between reviewers’ findings was k = 0.92.
2.5. Data Extraction
After finished cross-examination, all adequate information were transferred to an Excel spreadsheet. A standardized data extraction protocol (Cochrane Consumer and Communication Review Group’s) was implemented, in order to extract the study authors, year of publication, and study aim, along with the sample information (size and age), exercise program (duration, intensity and frequency), study measurements, and study results.
3. Results
3.1. Study Quality
All 9 studies included in the quantitative analysis were longitudinal. Based on the points each study scored on the PEDro scale, the final study quality assessment scores, were defined [33]. Two studies presented fair quality, and the remaining seven of them presented good quality.
3.2. Selection and Characteristics of Studies
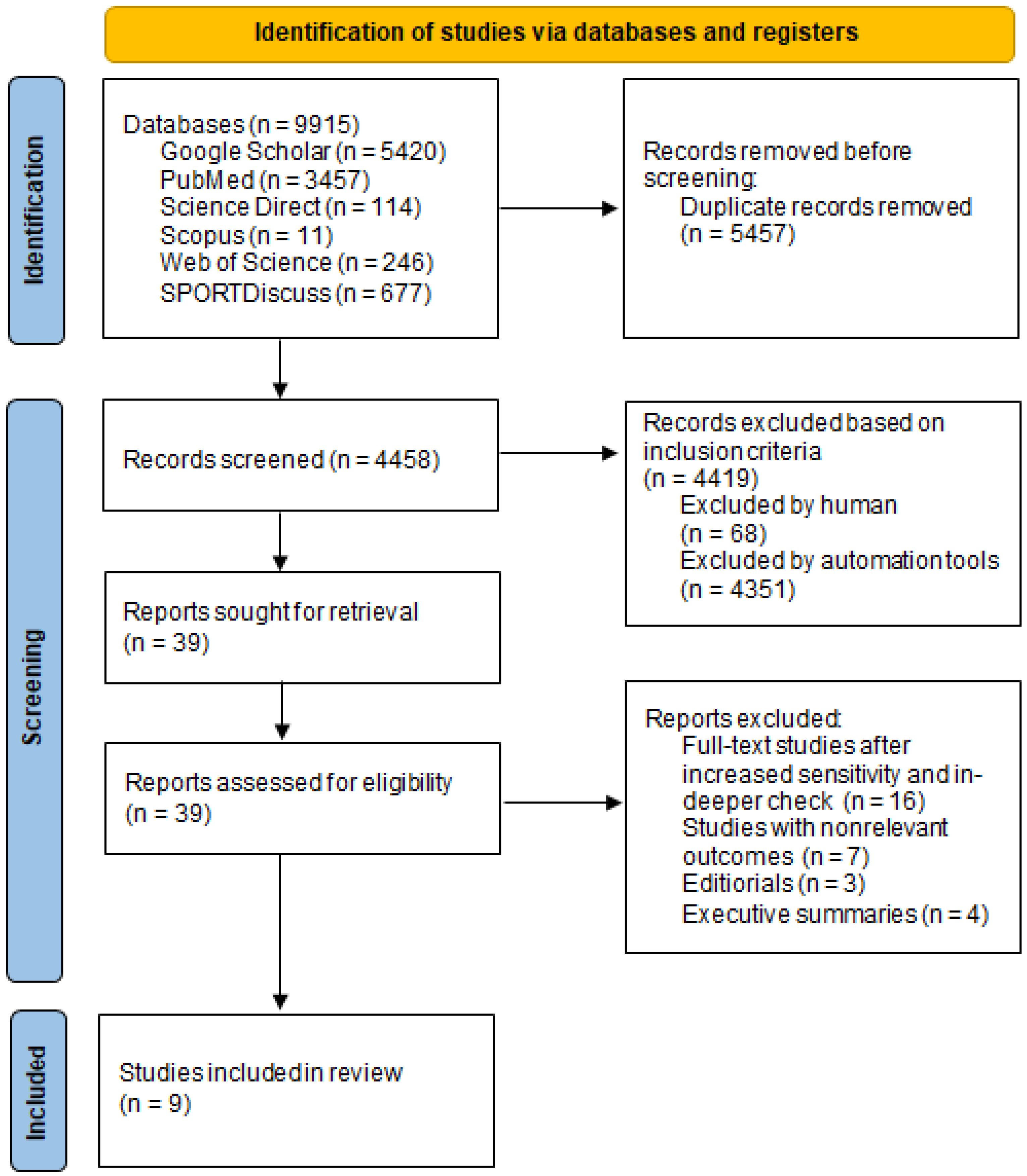
A search of electronic databases and scanning the reference lists yielded 9915 relevant studies. After removing duplicates, 4458 studies were screened. Then, 39 studies were selected and screened for eligibility, based on the inclusion criteria. Lastly, nine relevant studies were included in the systematic review, presented in Figure 1 and Table 3.
There was a total of 216 participants. The highest number of participants was 45 [25], while the lowest was 12 [26,27,28]. A female sample of participants only was found in two studies [25,31], a male sample was found in two studies as well [27,28], while the rest of the five studies had a mixed gender sample [24,26,29,30,32]. The participants were healthy in most of the included studies, and the physically active were found in five studies [25,27,28,29,32], except the case of Fernandez-Gonzalo et al. [26], where the sample consisted of chronic stroke patients. The longest experimental program lasted 13 weeks [32], while the shortest was 4 weeks [25]. Trainings per week were not more than three times and not less than two times, and only one study did not show that information [31]. The sets varied from 1 to 4, and the repetition within also varied from 7 to 22 or from 2 to 7 repetitions maximum. Based on given sets and repetitions, the resting period between the sets varied from 1 to 5 min.
In addition, three studies had more than one experimental group [24,25,31], while a couple of studies included participants who all underwent the same experimental intervention [26,27,28]. Several studies have also conducted a comparison of flywheel training with some other training method, such as traditional weight-based training [24,31,32], high-intensity [27], and high-intensity interval training [28].
As for the control groups, three studies [26,27,28] did not have any, and two studies conducted traditional weight training [24,31]. One study’s [25] control group had organized classes (gymnastic, swimming, Nordic walking), while two studies [30,32] had conducted daily physical activities. Only one study [29] did not state the activities of their control group.
4. Discussion
The aim of the current review was to determine the effects of flywheel training in older adults on various functional tests. Physical exercise was found to provide benefits to individuals, from preventing many non-communicable diseases and creating better mood, to mental and emotional satisfaction, improving health, and improving physical and functional fitness [35]. Regarding flywheel training, although there is a lack of included studies, the findings are consistent concerning the physical, neuromuscular, and functional improvements in older adults. Despite the growing interest in flywheel training method [14,36,37], this is one of the first systematic reviews to focus on older adults.
A key factor related to the improvement or maintenance of quality of life is resistance training, since it can ease age-related impairments (muscle atrophy, strength decreases, etc.) [38], by improving neuromuscular function, strength, balance, power, and movement capacity [39,40]. Flywheel training benefits are associated with the combination of concentric contractions with the presence of an eccentric overload [41], which is the main reason why this modality may be an alternative for improvement of determinant health-related capacities in older populations [42]. Onambele et al. [24] obtained moderate improvements in isometric quadriceps strength (8%), large improvements in knee-extension (28%), and very large improvements in in tendon stiffness (136%) which improved balance performance. Moreover, Sanudo et al. [30] showed increases in power performance (63%) and velocity (48%), as well as in balance (13%). Since these results are similar to previous findings in balance responses [43], a possible explanation could be attributed to the muscles activated in each exercise. Important to note is that older adults tend to rely more on hip strategies (hip and knee extensions) for more balance control, which are most activated by inertial systems. Thus, the squat modality may have more a great impact (e.g., hip abductors and adductors) that has a greater influence on balance [44]. Further, exercises that are performed with a high speed promote greater improvements in functional task performance [45], highlighting the relevance. Increasing the velocity component of peak power improved the performance of many functional tasks [46], and this may have clinical consequences, as aging is associated with a decline in neural processing that can diminish the ability for rapid force development and, therefore, limit the response to postural challenges [47].
As some other previous studies examined effects of flywheel training on functional markers, such as a timed up and go test [24], 30 s sit to stand test [48], and 5 times sit to stand test [49], it is crucial to use functional tests as a tool to assess fitness level [50], monitored training [51], and rehabilitation in older adults [52]. In addition, completing a greater number of repetitions suggests the training has reduced fatigability which is also an important risk factor for falls [53]. Regarding the sit to stand test, Spudić et al. [31] found improvements of 16% and Odeleye [32] of 35–47%, as well as a large-magnitude reduction [29], which was similar to those observed by Fernandez-Gonzalo et al. [54]. Such given results can be attributed to a specific motoric pattern that appears during executing a squat in the mentioned tests. This is due to two similar kinematic and kinetic motions that take place during both motion techniques, which cause similar muscle responses [55].
Two studies [31,32] have observed a 6 min walk test, where both of them showed no improvements. These studies are in contrast with previously conducted studies by Raj et al. [56], Fernandez-Gonzalo et al. [54], and Dias et al. [57]. Two studies [31,32] conducted functional reach test, where also no improvements were observed. The lack of improvements could be a high level of baseline fitness and activity, which may result in a reduction in the likelihood to detect differences. In addition, Mueller et al. [58] have also observed similar limitation as well, although they have been using different functional performance measures. With that being said, differences in participants’ physical and fitness levels in the baseline measurements should be taken into consideration when applying flywheel technology.
The gains in strength, hypertrophy, muscle activation, and muscle length will lead to positive adaptations and muscle healing; the flywheel is an effective tool for individuals who shows restricted mobility [59,60] and, for sensitive ones, with increased falls [61]. Flywheel training will strengthen muscles and improve muscle power as well as muscle reactivity. Strength, power, and reactivity are all important for older adults to keep them moving functionally, prevent them from falling, and maintain muscle health [62]. The results of Bruseghini et al. [27] suggest an increase in strength, which happened due to hypertrophy of the trained muscles. Flywheel resistance training elicits a greater muscle activation of the involved muscles during isometric maximal contraction. In addition, muscular activation during both concentric and eccentric contraction seems to be maximal even in the early phases of training over the entire range of movement [11].
Although there were already observed significant improvements in functional performances (timed up and go test and 30 s chair stand test) by Fernandez-Gonzalo et al. [26], this type of training has been found to be effective for increasing muscular performance of the lower limb extensor in older adults [24,28]. As we all know, the increase in muscular strength after several weeks is also a functional adaptation that results from several morphological and neural mechanisms that intervene during training itself [63]. Likewise, results in strength outcomes may possibly be due to several differences in maximal neural activation, and the individual ability to recover between sessions [64], since there were two–three sessions a week.
Papa et al. [65] defined resistance training as a strength training exercise with the use of progressive overload in which the muscles create the force against external load. In our case, older adults often experience age, inactivity, and disability association declines of functional capacity and lean body mass, which could be largely offset with regular participation in resistance training programs [66]. A couple of studies [24,31,32] have conducted resistance training and, in comparison to the flywheel, better results have been shown by the flywheel in postural stability, as well as in maximal peak isokinetic knee extensors [24], sit to stand test, timed up and go, and 6 m walk test [31]. Only in terms of Odeleye [32], similar results were presented for overall power, sit to stand test, and up and down stair climb test. The possible reason for the given results may lie in the fact that only Odeleye’s [32] control group was conducting regular physical activity, compared to the first two, which had no such intervention. In addition, in order to explain the rationale for the different results of resistance training and the flywheel, two things can be said. First, a higher force in the eccentric part is developed by the flywheel, since the time in executing the eccentric contraction repetitions is shorter than the concentric. This means that in order to gain higher forces in the eccentric part of repetition, the participant needs to actively decelerate the weight in a shorter amount of time that they spend moving the weight into rotation in the concentric part of the exercise. Second, the overly extended joint, when the load was highest during weight training, simply puts the quadriceps muscle at a mechanical disadvantage, which further is diminishing both the contractile forces that could be produced and the stimulus to increase the muscle strength [67].
High-intensity training is a time-effective alternative to traditional exercise programs, which involves a low to moderate intensity training of long duration. High-intensity interval training, a specific form of high-intensity training, is characterized by brief repetitions of high intensity exercise, alternated with a period of rest or low-intensity exercise [68]. In terms of their comparison to the flywheel [27,28], the flywheel has an induced significant increase in muscle strength and volume, maximal voluntary isometric torque, and the isokinetic concentric–eccentric torque of limb extensors. Although those interventions do not seem to abate or repeal the beneficial effects of aerobic training, it is also important to increase strength in older adults, which will further improve the quality of life and independency. Hence, in order to identify the real effects of mentioned programs and, most importantly, on same/similar parameters, future studies are needed.
The main limitations of this study are that the optimal strategy for applying flywheel training remains unclear [41,64] and that there is no specified an adequate choice of intensity and volume, with the optimal duration of the experimental program for older adults [20]. Furthermore, it is recommended that, in the future, the validity and reliability of devices and tests be considered when measuring performance changes [69].
5. Conclusions
This is one of the first studies that has summarized the effects of flywheel training in older adults. This systematic review reported improvements in physical, neuromuscular and functional performance in older adults following different flywheel protocols. The review also suggests that the mentioned training method can be effectively implemented in the mentioned population, which proves its feasibility. Although the current review did not reveal an optimal duration, frequency, intensity, or volume, we can conclude that this training method can be considered as an appropriate form of activity in older adults, as a tool for improving overall health. Further research is required in order to make standardized recommendations for this specific population.
Author Contributions
Conceptualization, N.Č. and M.H.; methodology, N.Č.; software, M.H.; validation, D.P. and M.H.; formal analysis, D.P.; investigation, M.S.; resources, M.S.; data curation, D.Đ.; writing–original draft preparation, D.Đ.; writing–review and editing, D.Đ. and M.S.; visualization, D.P.; supervision, M.H.; project administration, N.Č. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Desa, U. United nations department of economic and social affairs, population division. In World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; Online Ed UN DESA: New York, NY, USA, 2015. [Google Scholar]
- Algilani, S.; Östlund-Lagerström, L.; Kihlgren, A.; Blomberg, K.; Brummer, R.J.; Schoultz, I. Exploring the concept of optimal functionality in old age. J. Multidiscip. Healthc. 2014, 7, 69. [Google Scholar] [PubMed] [Green Version]
- Kulkarni, D.; Gregory, S.; Evans, M. Effectiveness of eccentric-biased exercise interventions in reducing the incidence of falls and improving functional performance in older adults: A systematic review. Eur. Geriatr. Med. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hairi, N.N.; Cumming, R.G.; Naganathan, V.; Handelsman, D.J.; Le Couteur, D.G.; Creasey, H.; Waite, L.M.; Seibel, M.J.; Sambrook, P.N. Loss of muscle strength, mass (sarcopenia), and quality (specific force) and its relationship with functional limitation and physical disability: The Concord Health and Ageing in Men Project. J. Am. Geriatr. Soc. 2010, 58, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Vetrovsky, T.; Steffl, M.; Stastny, P.; Tufano, J.J. The efficacy and safety of lower-limb plyometric training in older adults: A systematic review. Sport Med. 2019, 49, 113–131. [Google Scholar] [CrossRef] [Green Version]
- Ward, R.E.; Leveille, S.G.; Beauchamp, M.K.; Travison, T.; Alexander, N.; Jette, A.M.; Bean, J.F. Functional performance as a predictor of injurious falls in older adults. J. Am. Geriatr. Soc. 2015, 63, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Zhang, L.; Ding, Z.; Qiu, L.; Li, A. Falls and risk factors of falls for urban and rural community-dwelling older adults in China. BMC Geriatr. 2019, 19, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Harridge, S.D.R.; Lazarus, N.R. Physical activity, aging, and physiological function. Physiology 2017, 32, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.W.; Roberts, M.; Price, M.J.; Kay, A.D. Effects of Flywheel Training With Eccentric Overload on Standing Balance, Mobility, Physical Function, Muscle Thickness, and Muscle Quality in Older Adults. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef]
- Norrbrand, L.; Pozzo, M.; Tesch, P.A. Flywheel resistance training calls for greater eccentric muscle activation than weight training. Eur. J. Appl. Physiol. 2010, 110, 997–1005. [Google Scholar] [CrossRef]
- Wonders, J. Flywheel training in musculoskeletal rehabilitation: A clinical commentary. Int. J. Sports Phys. Ther. 2019, 14, 994. [Google Scholar] [CrossRef] [PubMed]
- Berg, H.E.; Tesch, A. A gravity-independent ergometer to be used for resistance training in space. Aviat. Space Environ. Med. 1994, 65, 752–756. [Google Scholar] [PubMed]
- Maroto-Izquierdo, S.; García-López, D.; Fernandez-Gonzalo, R.; Moreira, O.C.; González-Gallego, J.; de Paz, J.A. Skeletal muscle functional and structural adaptations after eccentric overload flywheel resistance training: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Romero-Rodriguez, D.; Gual, G.; Tesch, P.A. Efficacy of an inertial resistance training paradigm in the treatment of patellar tendinopathy in athletes: A case-series study. Phys. Ther. Sport 2011, 12, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Allen, W.J.C.; De Keijzer, K.L.; Raya-González, J.; Castillo, D.; Coratella, G.; Beato, M. Chronic effects of flywheel training on physical capacities in soccer players: A systematic review. Res. Sport Med. 2021, 1–21. [Google Scholar] [CrossRef] [PubMed]
- De Keijzer, K.; McErlain-Naylor, S.A.; Brownlee, T.E.; Raya-González, J.; Beato, M. Perception and application of flywheel training by professional soccer practitioners. Biol. Sport 2021, 39, 809–817. [Google Scholar] [CrossRef]
- Maroto-Izquierdo, S.; McBride, J.M.; Gonzalez-Diez, N.; García-López, D.; González-Gallego, J.; de Paz, J.A. Comparison of Flywheel and Pneumatic Training on Hypertrophy, Strength, and Power in Professional Handball Players. Res. Q. Exerc. Sport 2020, 93, 1–15. [Google Scholar] [CrossRef]
- Arede, J.; Gonzalo-Skok, O.; Bishop, C.; Schollhorn, W.; Leite, N. Rotational flywheel training in youth female team sport athletes: Could inter-repetition movement variability be beneficial? J. Sports Med. Phys. Fit. 2020, 60, 1444–1452. [Google Scholar] [CrossRef]
- Trajković, N.; Đorđević, D.; Stanković, M.; Petrušič, T.; Bogataj, Š.; Peršič, V. Exercise-Based Interventions in Middle-Aged and Older Adults after Myocardial Infarction: A Systematic Review. Life 2021, 11, 928. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 1–19. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Onambélé, G.L.; Maganaris, C.N.; Mian, O.S.; Tam, E.; Rejc, E.; McEwan, I.M.; Narici, M.V. Neuromuscular and balance responses to flywheel inertial versus weight training in older persons. J. Biomech. 2008, 41, 3133–3138. [Google Scholar] [CrossRef] [PubMed]
- Brzenczek-Owczarzak, W.; Naczk, M.; Arlet, J.; Forjasz, J.; Jedrzejczak, T.; Adach, Z. Estimation of the efficacy of inertial training in older women. J. Aging Phys. Act. 2013, 21, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Gonzalo, R.; Nissemark, C.; Åslund, B.; Tesch, P.A.; Sojka, P. Chronic stroke patients show early and robust improvements in muscle and functional performance in response to eccentric-overload flywheel resistance training: A pilot study. J. Neuroeng. Rehabil. 2014, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bruseghini, P.; Calabria, E.; Tam, E.; Milanese, C.; Oliboni, E.; Pezzato, A.; Pogliaghi, S.; Salvagno, G.L.; Schena, F.; Mucelli, R.P.; et al. Effects of eight weeks of aerobic interval training and of isoinertial resistance training on risk factors of cardiometabolic diseases and exercise capacity in healthy elderly subjects. Oncotarget 2015, 6, 16998. [Google Scholar] [CrossRef] [Green Version]
- Bruseghini, P.; Capelli, C.; Calabria, E.; Rossi, A.P.; Tam, E. Effects of High-Intensity Interval Training and Isoinertial Training on Leg Extensors Muscle Function, Structure, and Intermuscular Adipose Tissue in Older Adults. Front. Physiol. 2019, 10, 1260. [Google Scholar] [CrossRef]
- Roberts, M. Effect of Eccentric Flywheel Training on Musculoskeletal Characteristics and Physical Function in Older Adults. 2019. Available online: https://pure.coventry.ac.uk/ws/portalfiles/portal/31210514/Roberts_Pure.pdf (accessed on 11 December 2021).
- Sañudo, B.; González-Navarrete, Á.; Álvarez-Barbosa, F.; De Hoyo, M.; Del Pozo, J.; Rogers, M.E. Effect of flywheel resistance training on balance performance in older adults. A randomized controlled trial. J. Sports Sci. Med. 2019, 18, 344. [Google Scholar]
- Spudić, D.; Hadžić, V.; Vodičar, J.; Carruthers, J.; Pori, P. Influence of Inertial Resistance Squat Exercise Protocol Based on Novel Exercise Intensity Determination on Physical Fitness of Older Adult Women. Exerc. Qual. Life 2019, 11, 29–36. [Google Scholar] [CrossRef]
- Odeleye, O.O. A Comparative Study on the Effects of Eccentric Flywheel Overload and Traditional Resistance Training on the Physiological/Functional Performance in Healthy Older Adults. Univ. Sask. 2020. Available online: https://harvest.usask.ca/bitstream/handle/10388/12773/ODELEYE-THESIS-2020.pdf?sequence=1 (accessed on 17 December 2021).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Hicks, G.E.; Shardell, M.; Alley, D.E.; Miller, R.R.; Bandinelli, S.; Guralnik, J.; Lauretani, F.; Simonsick, E.M.; Ferrucci, L. Absolute strength and loss of strength as predictors of mobility decline in older adults: The InCHIANTI study. J. Gerontol. Ser. A Biomed Sci. Med. Sci. 2012, 67, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Tanaka, K.; Yabushita, N.; Sakai, T.; Shigematsu, R. Effects of exercise frequency on functional fitness in older adult women. Arch. Gerontol. Geriatr. 2007, 44, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Vicens-Bordas, J.; Esteve, E.; Fort-Vanmeerhaeghe, A.; Bandholm, T.; Thorborg, K. Is inertial flywheel resistance training superior to gravity-dependent resistance training in improving muscle strength? A systematic review with meta-analyses. J. Sci. Med. Sport 2018, 21, 75–83. [Google Scholar] [CrossRef]
- Raya-González, J.; Castillo, D.; Beato, M. The flywheel paradigm in team sports: A soccer approach. Strength Cond. J. 2021, 43, 12–22. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9. [Google Scholar] [CrossRef]
- Howe, T.E.; Rochester, L.; Neil, F.; Skelton, D.A.; Ballinger, C. Exercise for improving balance in older people. Cochrane Database Syst. Rev. 2011, 11. [Google Scholar] [CrossRef]
- Beato, M.; Dello Iacono, A. Implementing flywheel (isoinertial) exercise in strength training: Current evidence, practical recommendations, and future directions. Front. Physiol. 2020, 11, 569. [Google Scholar] [CrossRef]
- González, J.R.; de Keijzer, K.; Beato, M. Effects of flywheel training on strength-related variables in female populations. A systematic review. Res. Sports Med. 2020, 1–18. [Google Scholar] [CrossRef]
- Hess, J.A.; Woollacott, M.; Shivitz, N. Ankle force and rate of force production increase following high intensity strength training in frail older adults. Aging Clin. Exp. Res. 2006, 18, 107–115. [Google Scholar] [CrossRef]
- Orr, R.; Raymond, J.; Singh, M.F. Efficacy of progressive resistance training on balance performance in older adults. Sports Med. 2008, 38, 317–343. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.; Izquierdo, M.; Silva, A.J.; Costa, A.M.; Bastos, E.; González-Badillo, J.; Marques, M.C. Effects of high-speed power training on functional capacity and muscle performance in older women. Exp. Gerontol. 2012, 47, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Sayers, S.P.; Gibson, K. High-speed power training in older adults: A shift of the external resistance at which peak power is produced. J. Strength Cond. Res. Strength Cond. Assoc. 2014, 28, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, R. Contribution of muscle weakness to postural instability in the elderly. Eur. J. Phys. Rehabil. Med. 2010, 46, 183–220. [Google Scholar] [PubMed]
- Van Roie, E.; Delecluse, C.; Coudyzer, W.; Boonen, S.; Bautmans, I. Strength training at high versus low external resistance in older adults: Effects on muscle volume, muscle strength, and force–velocity characteristics. Exp. Gerontol. 2013, 48, 1351–1361. [Google Scholar] [CrossRef]
- Schlicht, J.; Camaione, D.N.; Owen, S.V. Effect of intense strength training on standing balance, walking speed, and sit-to-stand performance in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M281–M286. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, N.; Nakatani, T.; Okamoto, Y.; Iwamoto, J.; Saeki, K.; Kurumatani, N. Increasing the number of steps walked each day improves physical fitness in Japanese community-dwelling adults. Int. J. Sports Med. 2010, 31, 277–282. [Google Scholar] [CrossRef]
- Özkaya, G.Y.; Aydin, H.; Toraman, F.N.; Kizilay, F.; Özdemir, Ö.; Cetinkaya, V. Effect of strength and endurance training on cognition in older people. J. Sports Sci. Med. 2005, 4, 300. [Google Scholar]
- Nyland, J.; Frost, K.; Quesada, P.; Angeli, C.; Swank, A.; Topp, R.; Malkani, A.L. Self-reported chair-rise ability relates to stair-climbing readiness of total knee arthroplasty patients: A pilot study. J. Rehabil. Res. Dev. 2007, 44, 751–759. [Google Scholar] [CrossRef]
- Millor, N.; Lecumberri, P.; Gómez, M.; Martínez-Ramírez, A.; Izquierdo, M. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. J. Neuroeng. Rehabil. 2013, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Gonzalo, R.; Lundberg, T.R.; Alvarez-Alvarez, L.; de Paz, J.A. Muscle damage responses and adaptations to eccentric-overload resistance exercise in men and women. Eur. J. Appl. Physiol. 2014, 114, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, S.; Salem, G.J.; Wang, M.-Y.; Sanker, S.E.; Greendale, G.A. Squatting exercises in older adults: Kinematic and kinetic comparisons. Med. Sci. Sports Exerc. 2003, 35, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raj, I.S.; Bird, S.; Westfold, B.; Shield, A. Effects of eccentrically biased versus conventional weight training in older adults. Med. Sci. Sports Exerc. 2012, 44, 1167–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, C.P.; Toscan, R.; de Camargo, M.; Pereira, E.P.; Griebler, N.; Baroni, B.M.; Tiggemann, C.L. Effects of eccentric-focused and conventional resistance training on strength and functional capacity of older adults. Age 2015, 37, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Mueller, M.; Breil, F.A.; Vogt, M.; Steiner, R.; Lippuner, K.; Popp, A.; Klossner, S.; Hoppeler, H.; Däpp, C. Different response to eccentric and concentric training in older men and women. Eur. J. Appl. Physiol. 2009, 107, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Foldvari, M.; Clark, M.; Laviolette, L.C.; Bernstein, M.A.; Kaliton, D.; Castaneda, C.; Pu, C.T.; Hausdorff, J.M.; Fielding, R.A.; Singh, M.A.F. Association of muscle power with functional status in community-dwelling elderly women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M192–M199. [Google Scholar] [CrossRef]
- Md, J.F.B.; Kiely, D.K.; Herman, S.; Leveille, S.G.; Mizer, K.; Frontera, W.R.; Fielding, R.A. The relationship between leg power and physical performance in mobility-limited older people. J. Am. Geriatr. Soc. 2002, 50, 461–467. [Google Scholar] [CrossRef]
- Tesch, P.A.; Fernandez-Gonzalo, R.; Lundberg, T.R. Clinical applications of iso-inertial, eccentric-overload (YoYoTM) resistance exercise. Front. Physiol. 2017, 8, 241. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, D.; Morrison, S. Current concepts in periodization of strength and conditioning for the sports physical therapist. Int. J. Sports Phys. Ther. 2015, 10, 734. [Google Scholar]
- Folland, J.P.; Williams, A.G. Morphological and neurological contributions to increased strength. Sport Med. 2007, 37, 145–168. [Google Scholar] [CrossRef]
- Petré, H.; Wernstål, F.; Mattsson, C.M. Effects of flywheel training on strength-related variables: A meta-analysis. Sport Med. 2018, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: A systematic review. Clin. Interv. Aging 2017, 12, 955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurley, B.F.; Roth, S.M. Strength training in the elderly: Effects on risk factors for age-related diseases. Sports Med. 2000, 30, 249–268. [Google Scholar] [CrossRef]
- Van Eijden, T.; Weijs, W.A.; Kouwenhoven, E.K.; Verburg, J. Forces acting on the patella during maximal voluntary contraction of the quadriceps femoris muscle at different knee flexion/extension angles. Cells Tissues Organs. 1987, 129, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.; Buchheit, M. Science and Application of High-Intensity Interval Training; Human Kinetics: Champagn, IL, USA, 2019. [Google Scholar]
- Beato, M.; Fleming, A.; Coates, A.; Dello Iacono, A. Validity and reliability of a flywheel squat test in sport. J. Sports Sci. 2021, 39, 482–488. [Google Scholar] [CrossRef]
Figure 1.
Study identification procedure, based on the pre-defined criteria (PRISMA flow chart).


{kind=link}
Table 1.
PICOS model of eligibility criteria.
| Inclusion | Exclusion | |
|---|---|---|
| Population | Older adults (≥60 years) Males and females | Children, youth, adolescents, adults |
| Intervention | Flywheel training | Flexibility training, plyometric training, speed training |
| Control | - | - |
| Outcome | Post-flywheel intervention, strengh, balance, posture control, mobility, functional and cardiovascular performance, body composition | - |
| Study design | Randomized non-randomized studies, controlled studies, intervention studies | Case studies, systematic reviews, meta-analysis, case reports, Editorals, non-English studies |
Table 2.
PEDro scale results.
| Criterion | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ∑ |
| Onambele et al. (2008) [24] | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | 8 |
| Brzenczek-Owczarzak et al. (2013) [25] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Fernandez-Gonzalo et al. (2014) [26] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Bruseghini et al. (2015) [27] | Y | N | N | Y | N | N | N | Y | Y | Y | Y | 5 |
| Bruseghini et al. (2019) [28] | Y | N | Y | Y | N | N | N | Y | Y | Y | Y | 6 |
| Roberts et al. (2019) [29] | Y | Y | Y | Y | N | Y | N | Y | Y | Y | Y | 8 |
| Sanudo et al. (2019) [30] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Spudić et al. (2019) [31] | Y | Y | Y | Y | N | Y | N | N | Y | Y | Y | 7 |
| Odeleye et al. (2020) [32] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
Legend: 1—eligibility criteria; 2—random allocation to groups; 3—concealed allocation; 4—baseline group similarity at baseline; 5—blinding of all subjects; 6—blinding of all therapists; 7—blinding of all assessors; 8—dropouts (more than 80%); 9—intention to treat; 10—reported comparisons between groups; 11—point measures and measures of variability; Y—satisfied criterion; N—not satisfied criterion; ∑—total points sum.
Table 3.
Studies included in the systematic review.
| First Author and Year of Publication | Aim | Sample of Participants | Exercise Program | Measurements | Results | ||
|---|---|---|---|---|---|---|---|
| Number and Groups | Age (Years) | ||||||
| Onambele et al. (2008) [24] | Effects of F inertial loading and comaparation with WT, on KE (indices of quadriceps strength) | N-24 M-12 F-12 E1-12 E2-12 | 69.9 ± 1.3 | 3x a week 12 weeks 1–4 sets 8–12 rep. ≈5 mrbs | PS tests, maximal peak isokinetic KE function, EMG recordings | ** E1 Maximal peak isokinetic KE (28%, p < 0.01) PS (45%, p < 0.01) | |
| Brzenczek-Owczarzak et al. (2013) [25] | To estimate the efficiency of short-term inertial training using ITMS | F-45 E1-17 E2-10 C-18 | E1-62.2 ± 5.4 E2-64.1 ± 5.4 C-63.4 ± 4 | 3x a week 4 weeks 45 min 3 sets 10 rep. ≈2 mrbs | Maximal torque, P | Maximal torque (Da) E1 ** (21.9%) E2 ** # (6.9%) C (2.2%) (NDa) E1 ** (10.7%) | PWR (Da) E1 ** (34.3%) E2 ** # (9.8%) C (−1.4%) (NDa) E1 ** (27.6%) E2 ** (18.2%) C (0.6%) |
| Fernandez-Gonzalo et al. (2014) [26] | To estimate the efficacy of ECC-overload F RE training to improve force, P, B, and FP in physically active chronic stroke patients | N-12 M-9 F-3 | 63.3 ± 8.1 | 2x a week 8 weeks 4 sets 7 max. rep. ≈3 mrbs | B, FP, spasticity and RPE, isometric and isokinetic KE torque, peak P isometric leg press force | Peak PWR ** ECC (34%, p = 0.009) CON (44%, p = 0.003) Isokinetic torque ECC ** (p = 0.0005) CON (p = 0.002) Isometric leg press 10–20% (p < 0.05) | |
| Bruseghini et al. (2015) [27] | Effect of 8 weeks of HIT and IRT on CVF, MS mass, and risk factors of metabolic syndrome | M-12 | 68 ± 4 | 3x a week 8 weeks 3–4 sets 7 max. rep. ≈3 mrbs | BC, muscle structure, MS, maximal test, exercise efficiency | MS ** (HIT, IRT #) CON 60° (p = 0.0004) 120° (0.0049) ECC 60° (p = 0.0102) 120° (0.0010) | |
| Bruseghini et al. (2019) [28] | Comparation of effects of HIIT and IRT on strength, mass, architecture, IMAT quality, and Na | M-12 | 69.3 ± 4.2 | 3x a week 8 weeks 3 sets 7 rep. ≈3 mrbs | VO2max, muscle volume, IMAT, Na MS, muscle architecture | IRT muscle volume (p = 0.003), HIIT muscle volume (p = 0.001) IRT IMAT (p = 0.001) HIIT IMAT (p = 0.003) | |
| Roberts (2019) [29] | To determine the effectiveness of a short period of F eccentric RE and to compare changes in MS and mass, physical function, and fall risk | N-21 M-10 F-11 E-13 C-8 | 62.52 ± 6.72 | 2x a week 6 weeks 4 sets 8–12 rep. | 30 sec Sts, TUAG, 5x Sts, isometric strength | 30 sec Sts (p = 0.248) TUAG (p = 0.157) 5x Sts (p = 0.389) | |
| Sanudo et al. (2019) [30] | To assess the effects of F RE training on PS and M | N-34 E-17 C-17 | 65 ± 4 E-64.4 ± 3.61 C-66.38 ± 4.85 | 2–3x a week 6 weeks 4 sets 9 rep. ≈3 mrbs | PS, P | E ** # TUAG (p < 0.01) PWR (p < 0.05) | |
| Spudić et al. (2019) [31] | To examine the effects of inertial device exercies protocol compared to the traditional weight-based, on KE MS, agility, B, CVE, and RPE | F-37 E1-14 E2-12 C-11 | E1-71.6 ± 6.4 E2-68.8 ± 6.4 C-67.3 ± 4.5 | 8 weeks 2–4 sets 10–22 rep. ≈1.5 mrbs | 6MWT, Sts, TUAG, FR, RPE | E2 # Sts (p = 0.018) RPE # (E1,E2,C, p > 0.05)TUAG (ES% = −0.44) 6MWT (ES% = 0.47) | |
| Odeleye (2020) [32] | To compare the effects of eccentric Fly overload training and traditional RE on MS, muscle thickness, BC, and FP | N-19 M-6 F-13 E-11 C-8 | E1-63.2 ± 7.8 C-63.8 ± 5.2 | 3x a week 13 weeks 3 + 3 + 3 + 3 max. reps ≈1 mrbs | MS of quadriceps (KE), FP (shuttle walk test, FR, 30 sec Sts, up and down stair climb P test) | (E1, E2) ** (p < 0.001) (PWR, Sts, up and down stair climb) | |
Legend: N—total number of participants, M—males, F—females, E—experimental group, C—control group, ITMS—Inertial Training and Measurement System, ECC—exercise comprising eccentric, CON-exercise comprising concentric, RE-resistance exercise, HIT-high interval training, HIIT-high-intensity interval training, IRT—isoinertial resistance training, CVF—cardiovascular fitness, CVE—cardiovascular endurance, IMAT—intermuscular adipose tissue, RPE—rate of perceived exertion, WT—weight training, KE—knee extensors, M—mobility, MS—muscle strength, Fly—flywheel, B—balance, PS—postural stability tests, FP—functional performance, BC—body composition, PWR—power, avg—average, EMG—electromiography, 6MWT—6 m walk test, TUAG—timed up and go, FR—functional reach, Na—neuromuscular activation, Sts—sit to stand test, Gs—grip strength, Da—dominant arm, NDa—nondominant arm, mrbs—minutes recovery between sets, rep.—repetition, **—statistical significance from baseline, #—statistical significance between groups, ES%—effect size.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Čokorilo, N.; Horvatin, M.; Đorđević, D.; Stanković, M.; Pekas, D. Flywheel Training in Older Adults—A Systematic Review. Sustainability 2022, 14, 4137. https://doi.org/10.3390/su14074137
AMA Style
Čokorilo N, Horvatin M, Đorđević D, Stanković M, Pekas D. Flywheel Training in Older Adults—A Systematic Review. Sustainability. 2022; 14(7):4137. https://doi.org/10.3390/su14074137
Chicago/Turabian StyleČokorilo, Nebojša, Maja Horvatin, Dušan Đorđević, Mima Stanković, and Damir Pekas. 2022. "Flywheel Training in Older Adults—A Systematic Review" Sustainability 14, no. 7: 4137. https://doi.org/10.3390/su14074137
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.