
Mouthwash with Tagetes lucida Cav. for Control of Chronic Periodontitis in Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
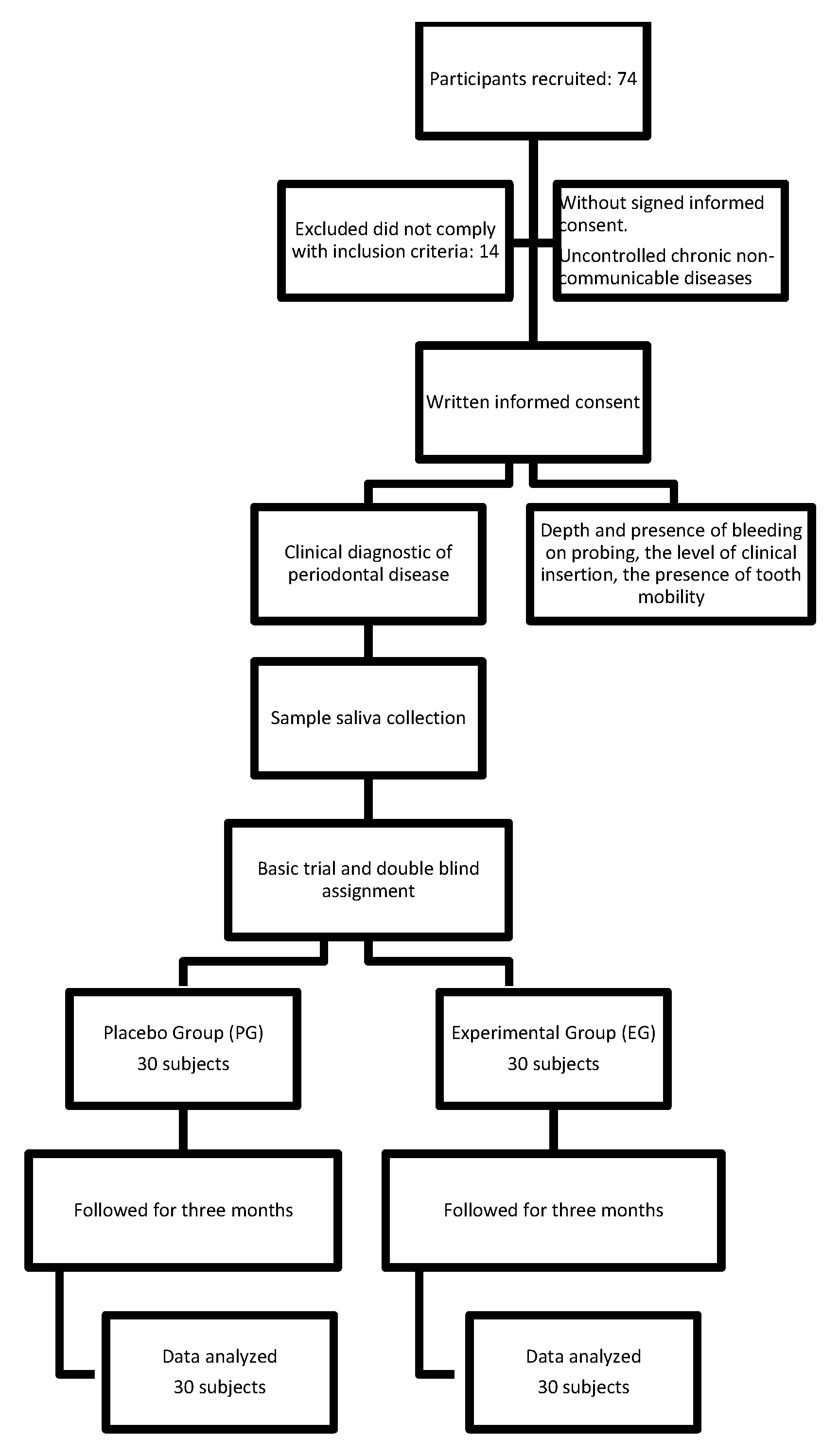
2.1. Subjects and Design
2.2. Sample Size
- N = 2 2
- Assuming that:
- z α = Z value corresponding to alpha error (p 0.05 = 1.96)
- z β = Z value corresponding to beta error (20%)
- SD = Standard deviation (0.01)
- µ1 = Group A mean (0.029 µmol/L)
- µ2 = Group B mean (0.025 µmol/L)
- n = 28 per group
2.3. Extraction and Preparation of T. lucida
2.4. Phytochemical Characterization
2.5. Clinical Evaluation
2.6. Saliva Samples and Biochemical Techniques
2.7. TBARS
2.8. Saliva Total Antioxidant Status (TAS)
2.9. Saliva Superoxide Dismutase (SOD)
2.10. Quantification of Cytokines
2.11. Statistical Analysis
3. Results
3.1. Clinical Changes Related to Treatment
3.2. Effect of T. lucida on Oxidative Stress Markers
3.3. Effect of T. lucida on Inflammatory Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dahiya, P.; Kamal, R.; Gupta, R.; Bhardwaj, R.; Chaudhary, K.; Kaur, S. Reactive oxygen species in periodontitis. J. Indian Soc. Periodontol. 2013, 17, 411–416. [Google Scholar] [CrossRef]
- Chapple, I.L.; Matthews, J.B. The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontology 2007, 43, 160–232. [Google Scholar] [CrossRef]
- Kim, S.C.; Kim, O.S.; Kim, O.J.; Kim, Y.J.; Chung, H.J. Antioxidant profile of whole saliva after scaling and root planning in periodontal disease. J. Periodontal. Implant. Sci. 2010, 40, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Brock, G.R.; Butterworth, C.J.; Matthews, J.B.; Chapple, I.L. Local and systemic total antioxidant capacity in periodontitis and health. J. Clin. Periodontol. 2004, 31, 515–521. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Navarrete-Hernández, J.J.; Veras-Hernández, M.A.; Casanova-Rosado, J.F.; Minaya-Sánchez, M.; Casanova-Rosado, A.J.; Fernández-Barrera, M.A.; Medina-Solís, C.E. Indicators of oral health in older adults with and without the presence of multimorbidity: A cross-sectional study. Clin. Interv. Aging. 2019, 14, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Aslani, A.; Ghannadi, A.; Najafi, H. Desing, formulation and evaluation of a mucoadhesive gel from Quercus brantii L. and Coriandrum sativum L. as periodontal drug delivery. Adv. Biomed. Res. 2013, 2, 21. [Google Scholar] [CrossRef] [PubMed]
- Yagnini, J.; Shahabooei, M.; Aslani, A.; Zadeh, M.R.; Kiani, S.; Naghsh, N. Efficacy of local- drug delivery gel containing extracts of Quercus brantii and Coriandrum sativum as an adjunct to scaling and root planning in moderate chronic periodontitis patients. J. Res. Pharm. Pract. 2014, 3, 67–71. [Google Scholar]
- Kumar, G.; Jalaluddin, M.; Rout, P.; Mohanty, R.; Dileep, C.L. Emerging trends of herbal care in dentistry. J. Clin. Diagn. Res. 2013, 7, 1827–1829. [Google Scholar]
- Regalado, E.L.; Fernández, M.D.; Pino, J.A.; Mendiola, J.; Echemendia, O.A. Chemical composition and biological properties of the leaf essential oil of Tagetes lucida Cav. from Cuba. J. Essent. Oil. Res. 2011, 23, 63–67. [Google Scholar] [CrossRef]
- Salehi, B.; Valussi, M.; Morais-Braga, M.F.B.; Carneiro, J.N.P.; Leal, A.L.A.B.; Coutinho, H.D.M.; Vitalini, S.; Kręgiel, D.; Antolak, H.; Sharifi-Rad, M.; et al. Tagetes spp. essential oils and other extracts: Chemical characterization and biological activity. Molecules 2018, 23, 2847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facultad de Estudios Superiores Zaragoza. Tagetes lucida Cav. Herbario de la FES ZARAGOZA—UNAM con el número de colección 156999. 2017. Available online: https://www.zaragoza.unam.mx/herbario/ (accessed on 16 October 2017).
- U.S. FUD and Drug Administration. Substance Registration System. Unique Ingredient Identifier UNII: N4052J8NFR; 2019. Available online: https://fdasis.nlm.nih.gov/srs/unii/N4052J8NFR (accessed on 19 August 2019).
- Céspedes, C.L.; Avila, J.G.; Martínez, A.; Serrato, B.; Calderón-Mugica, J.C.; Salgado-Garciglia, R. Antifungal and antibacterial activities of Mexican tarragon (Tagetes lucida). J. Agric. Food Chem. 2006, 54, 3521–3527. [Google Scholar] [CrossRef]
- Bonilla-Jaime, H.; Guadarrama-Cruz, G.; Alarcon-Aguilar, F.J.; Limón-Morales, O.; Vazquez-Palacios, G. Antidepressant-like activity of Tagetes lucida Cav. is mediated by 5-HT(1A) and 5-HT(2A) receptors. J. Nat. Med. 2015, 69, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ortega, G.; González-Trujano, M.E.; Ángeles-López, G.E.; Brindis, F.; Vibrans, H.; Reyes-Chilpa, R. Tagetes lucida Cav.: Ethnobotany, phytochemistry and pharmacology of its tranquilizing properties. J. Ethnopharmacol. 2016, 181, 221–228. [Google Scholar] [CrossRef]
- Guadarrama-Cruz, G.; Alarcón-Aguilar, J.; Vaga-Ávila, E.; Vázquez-Palacios, G.; Bonilla-Jaime, H. Antidepressant-like effect of Tagetes lucida Cav. extract in rats: Involvement of the serotonergic system. Am. J. Chin. Med. 2012, 40, 753–768. [Google Scholar]
- Aquino, R.; Cáceres, A.; Morelli, S.; Luca Rastrelli, L. An extract of Tagetes lucida and its phenolic constituents as antioxidants. J. Nat. Prod. 2002, 65, 1773–1776. [Google Scholar] [CrossRef]
- Monterrosas-Brisson, N.; Herrera-Ruiz, M.; Jiménez-Ferrer, E.; Bahena-Pérez, R.; Avilés-Flores, M.; Fuentes-Mata, M.; Martínez-Duncker, I.; González-Cortazar, M. Anti-inflammatory activity of coumarins isolated from Tagetes lucida Cav. Nat. Prod. Res. 2019. [Google Scholar] [CrossRef]
- Scull, R.; Gutiérrez, Y.I.; Sánchez, A.; Montes, A. Análisis farmacognóstico de Tagetes lucida Cav. y sus extractos hidroalcohólicos. Rev. Cienc. Farm. Aliment. 2016, 2, 1–13. [Google Scholar]
- Ramfjord, S.P. The Periodontal Disease Index (PDI). J. Periodontol. 1967, 38, S602–S610. [Google Scholar] [CrossRef]
- Arana, C.; Cutando, A.; Ferrera, M.J.; Gómez-Moreno, G.; Worf, C.V.; Bolaños, M.J.; Escames, G.; Acuña-Castroviejo, D. Parameters of oxidative stress in saliva from diabetic and parenteral drug addict patients. J. Oral Pathol Med. 2006, 35, 554–559. [Google Scholar] [CrossRef]
- Jentzsch, A.M.; Bachmann, H.; Fürst, P.; Biesalski, H.K. Improved analysis of malondialdehyde in human body fluids. Free Radic. Biol. Med. 1996, 20, 251–256. [Google Scholar] [CrossRef]
- Mendoza-Núñez, V.M.; Ruiz-Ramos, M.; Sánchez-Rodríguez, M.A.; Retana-Ugalde, R.; Muñoz-Sánchez, J.L. Aging-related oxidative stress in healthy humans. Tohoku J. Exp. Med. 2007, 213, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Karim, S.; Pratibha, P.K.; Kamath, S.; Bhat, G.S.; Kamath, U.; Dutta, B.; Sharma, N.; Archana, B.; Bhat, K.M.; Guddattu, V. Superoxide dismutase enzyme and thiol antioxidants in gingival crevicular fluid and saliva. Dent. Res. J. (Isfahan) 2012, 9, 266–272. [Google Scholar]
- Cook, E.B.; Stahl, J.L.; Lowe, L.; Chen, R.; Morgan, E.; Wilson, J.; Varro, R.; Chan, A.; Graziano, F.M.; Barney, N.P. Simultaneous measurement of six cytokines in a single sample of human tears using microparticle-based flow cytometry: Allergics vs. non-allergics. J. Immunol. Methods. 2001, 254, 109–118. [Google Scholar] [CrossRef]
- Park, E.; Cho, M.; Ki, C.S. Correct use of repeated measures analysis of variance. Korean J. Lab. Med. 2009, 1, 1–9. [Google Scholar] [CrossRef]
- Khiste, S.V.; Ranganath, V.; Nichani, A.S.; Rajani, V. Critical analysis of biomarkers in the current periodontal practice. J. Indian Soc. Periodontol. 2011, 15, 104–110. [Google Scholar] [CrossRef]
- Kinane, D.F.; Marshall, G.J. Periodontal manifestations of systemic disease. Aust. Dent. J. 2001, 46, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Grossi, S.G.; Genco, R.J. Periodontal disease and diabetes mellitus: A two-way relationship. Ann. Periodontol. 1998, 3, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Battino, M.; Bullon, P.; Wilson, M.; Newman, H. Oxidative injury and inflammatory periodontal diseases: The challenge of anti-oxidants to free radicals and reactive oxygen species. Crit. Rev. Oral Biol. Med. 1999, 10, 458–476. [Google Scholar] [CrossRef] [PubMed]
- Cannizzo, E.S.; Clement, C.C.; Sahu, R.; Follo, C.; Santambrogio, L. Oxidative stress, inflamm-aging and immunosenescence. J. Proteomics. 2011, 74, 2313–2323. [Google Scholar] [CrossRef]
- Guadarrama-Cruz, G.; Alarcon-Aguilar, F.J.; Lezama-Velasco, R.; Vázquez-Palacios, G.; Bonilla-Jaime, H. Antidepressant-like effects of Tagetes lucida cav. In the forced swimming test. J. Ethnopharmacol. 2008, 120, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Atabay, V.E.; Lutfioğlu, M.; Avci, B.; Sakallioglu, E.E.; Aydoğdu, A. Obesity and oxidative stress in patients with different periodontal status: A case-control study. J. Periodontal. Res. 2017, 52, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, D.; Zhang, X.L.; Wang, Y.Z.; Yang, C.X.; Chen, G. Lipid peroxidation levels, total oxidant status and superoxide dismutase in serum, saliva and crevicular fluid in chronic periodontitis patients before and after periodontal therapy. Aust. Dent. J. 2010, 55, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Guentsch, A.; Preshaw, P.M.; Bremer-Streck, S.; Klinger, G.; Glockmann, E.; Sigusch, B.W. Lipid peroxidation and antioxidant activity in saliva of periodontitis patients: Effect of smoking and periodontal treatment. Clin. Oral Investig. 2008, 12, 345–352. [Google Scholar] [CrossRef]
- de Oliveira, J.S.; Pinto, M.E.; Santana, L.A.; Pinto, A.S.; di Lenardo, D.; Vasconcelos, D.F. Biological effects of medicinal plants on induced periodontitis: A systematic review. Int. J. Dent. 2016, 3719879. [Google Scholar] [CrossRef]
- Tsai, C.C.; Chen, H.S.; Chen, S.L.; Ho, Y.P.; Ho, K.Y.; Wu, Y.M. Lipid peroxidation a possible role in the induction and progression of chronic periodontitis. J. Periodont. Res. 2005, 40, 378–384. [Google Scholar] [CrossRef]
- Waddington, R.J.; Moseley, R.; Embery, G. Periodontal disease mechanisms: Reactive oxygen species: A potential role in the pathogenesis of periodontal diseases. Oral Dis. 2000, 6, 138–151. [Google Scholar] [CrossRef]
- Rittié, L.; Monboisse, J.C.; Gorisse, M.C.; Gillery, P. Malondialdehyde binding to proteins dramatically alters fibroblast functions. J. Cell Physiol. 2002, 191, 227–236. [Google Scholar] [CrossRef]
- Moore, S.; Calder, K.A.; Miller, N.J.; Rice-Evans, C.A. Antioxidant activity of saliva and periodontal disease. Free Radic. Res. 1994, 21, 417–425. [Google Scholar] [CrossRef]
- Jimi, E.; Aoki, K.; Saito, H.; D’Acquisto, F.; May, M.J.; Nakamura, I.; Sudo, T.; Kojima, T.; Okamoto, F.; Fukushima, H.; et al. Selective inhibition of NF-kappa B blocks osteoclastogenesis and prevents inflammatory bone destruction in vivo. Nat. Med. 2004, 10, 617–624. [Google Scholar] [CrossRef]
- Hrishi, T.S.; Kundapur, P.P.; Naha, A.; Thomas, B.S.; Kanath, S.; Bhat, G.S. Effect of adjunctive use of Green tea dentifrice in periodontitis patients—A randomized controlled pilot study. Int. J. Dent. Hyg. 2016, 14, 178–183. [Google Scholar] [CrossRef]
- Mascitti, M.; Coccia, E.; Vignini, A.; Aquilanti, L.; Santarelli, A.; Salvolini, E.; Sabbatinelli, J.; Mazzanti, L.; Procaccini, M.; Rappelli, G. Anorexia, oral health and antioxidant salivary system: A clinical study on adult female subjects. Dent. J. 2019, 7, 60. [Google Scholar] [CrossRef] [Green Version]
- Tóthová, L.; Kamodyová, N.; Červenka, T.; Celec, P. Salivary markers of oxidative stress in oral diseases. Front. Cell Infect. Microbiol. 2015, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Wen, Q.; Xue, J.; Ding, Y. Alveolar bone regeneration potential of a traditional chinese medice, Bu-Shen-Gu-Chi–Wan, in experimental periodontitis. J. Periodontal. Res. 2014, 49, 382–389. [Google Scholar] [CrossRef]
- Moradi, J.; Abbasipour, F.; Zaringhalam, J.; Maleki, B.; Ziaee, N.; Khodadoustan, A.; Janahmadi, M. Anethole a medicinal plant compound, decreases the production of pro- inflammatory TNF-α and IL-1β in rat model of LPS-induced periodontitis. Iran. J. Pharm Res. 2014, 13, 1319–1325. [Google Scholar] [PubMed]
- Elburki, M.S.; Rossa, C.; Guimaraes, M.R.; Goodenough, M.; Lee, H.M.; Curylofo, F.A.; Zhang, Y.; Johnson, F.; Golub, L.M. A novel chemically modified curcumin reduces severity of experimental periodontal disease in rats: Initial observations. Mediat. Inflamm. 2014, 959471. [Google Scholar] [CrossRef] [PubMed]
- Sulistyani, H.; Fujita, M.; Nakazawa, F. Effect of roselle caliyx extract on gingipain activity, production of inflammatory cytokines, and oral bacterial morphology. J. Microbiol. Biotech. Food Sci. 2016, 6, 961–965. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T.; Chen, D.; Li, Q.; Sun, X.; Song, Y.; Wang, C. Curcumin inhibits inflammatory response and bone loss during experimental periodontitis in rats. Acta Odontol. Scand. 2013, 71, 349–356. [Google Scholar] [CrossRef]
- Gunsolley, J.C. Clinical efficacy of antimicrobial mouthrinses. J. Dent. 2010, 38 (Suppl. 1), S6–S10. [Google Scholar] [CrossRef]
- Barbosa, S.I.; Coury, S.C.H.; Collantes, D.I.E. Can mouth washes containing chlorhexidine 0.12% be used as synonym of a water solution of chlorhexidine 0.12%? Braz. J. Pharm. Sci. 2015, 51, 2. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Placebo Group (n = 30) | Experimental Group (n = 30) | |||||
|---|---|---|---|---|---|---|
| Baseline | Post-Treatment | Differences | Baseline | Post-Treatment | Differences | |
| PPD (mm) | 5.1 ± 0.64 | 5.7 ± 0.87 | 0.6 ± 0.23 | 5.2 ± 0.81 | 3.1 ± 0.43 * | −2.1 ± 0.38 |
| CAL (mm) | 6.6 ± 1.10 | 7.4 ± 1.30 | 0.8 ± 0.20 | 6.6 ± 1.90 | 2.1 ± 1.50 * | −4.5 ± 0.40 |
| Placebo Group (n = 30) | Experimental Group (n = 30) | |||
|---|---|---|---|---|
| Baseline | Post-Treatment | Baseline | Post-Treatment | |
| DM f (%) | ||||
| Yes | 17 (57) | 21 (70) | 20 (68) | 2 (8) * |
| No | 13 (43) | 9 (30) | 10 (32) | 28 (92) |
| BOP f (%) | ||||
| Yes | 16 (52) | 12 (40) | 16 (53) | 2 (7) * |
| No | 14 (48) | 18 (60) | 14 (47) | 28 (93) |
| Placebo Group (n = 30) | Experimental Group (n = 30) | |||
|---|---|---|---|---|
| Baseline | Post-Treatment | Baseline | Post-Treatment | |
| LPO (µmol/L) | 0.049 ± 0.02 | 0.054 ± 0.06 | 0.056 ± 0.03 | 0.034 ± 0.02 * |
| TAS (mmol/L) | 0.55 ± 0.39 | 0.66 ± 0.42 | 0.58 ± 0.36 | 0.71 ± 0.47 |
| SOD (IU/L) | 1.60 ± 0.52 | 1.50 ± 0.54 | 1.56 ± 0.52 | 1.64 ± 0.49 |
| Placebo Group (n = 30) | Experimental Group (n = 30) | |||
|---|---|---|---|---|
| Baseline | Post-Treatment | Baseline | Post-Treatment | |
| IL-1β (pg/mL) | 774 ± 1332 | 661 ± 483 | 871 ± 1126 | 462 ± 800.9 * |
| IL-8 (pg/mL) | 448 ± 343 | 571 ± 310 | 827 ± 647 | 624 ± 494 * |
| TNF-α (pg/mL) | 3.7 ± 1.5 | 4.4 ± 1.6 | 5.2 ± 2.6 | 3.3 ± 0.84 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macías-Camacho, T.; Retana-Ugalde, R.; Legorreta-Herrera, M.; Ruiz-Ramos, M.; Mendoza-Núñez, V.M. Mouthwash with Tagetes lucida Cav. for Control of Chronic Periodontitis in Older Adults. Sustainability 2021, 13, 1650. https://doi.org/10.3390/su13041650
Macías-Camacho T, Retana-Ugalde R, Legorreta-Herrera M, Ruiz-Ramos M, Mendoza-Núñez VM. Mouthwash with Tagetes lucida Cav. for Control of Chronic Periodontitis in Older Adults. Sustainability. 2021; 13(4):1650. https://doi.org/10.3390/su13041650
Chicago/Turabian StyleMacías-Camacho, Thalia, Raquel Retana-Ugalde, Martha Legorreta-Herrera, Mirna Ruiz-Ramos, and Víctor Manuel Mendoza-Núñez. 2021. "Mouthwash with Tagetes lucida Cav. for Control of Chronic Periodontitis in Older Adults" Sustainability 13, no. 4: 1650. https://doi.org/10.3390/su13041650