Comparative Effects of High-Intensity Interval Training vs Moderate-Intensity Continuous Training in Phase III of a Tennis-Based Cardiac Rehabilitation Program: A Pilot Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
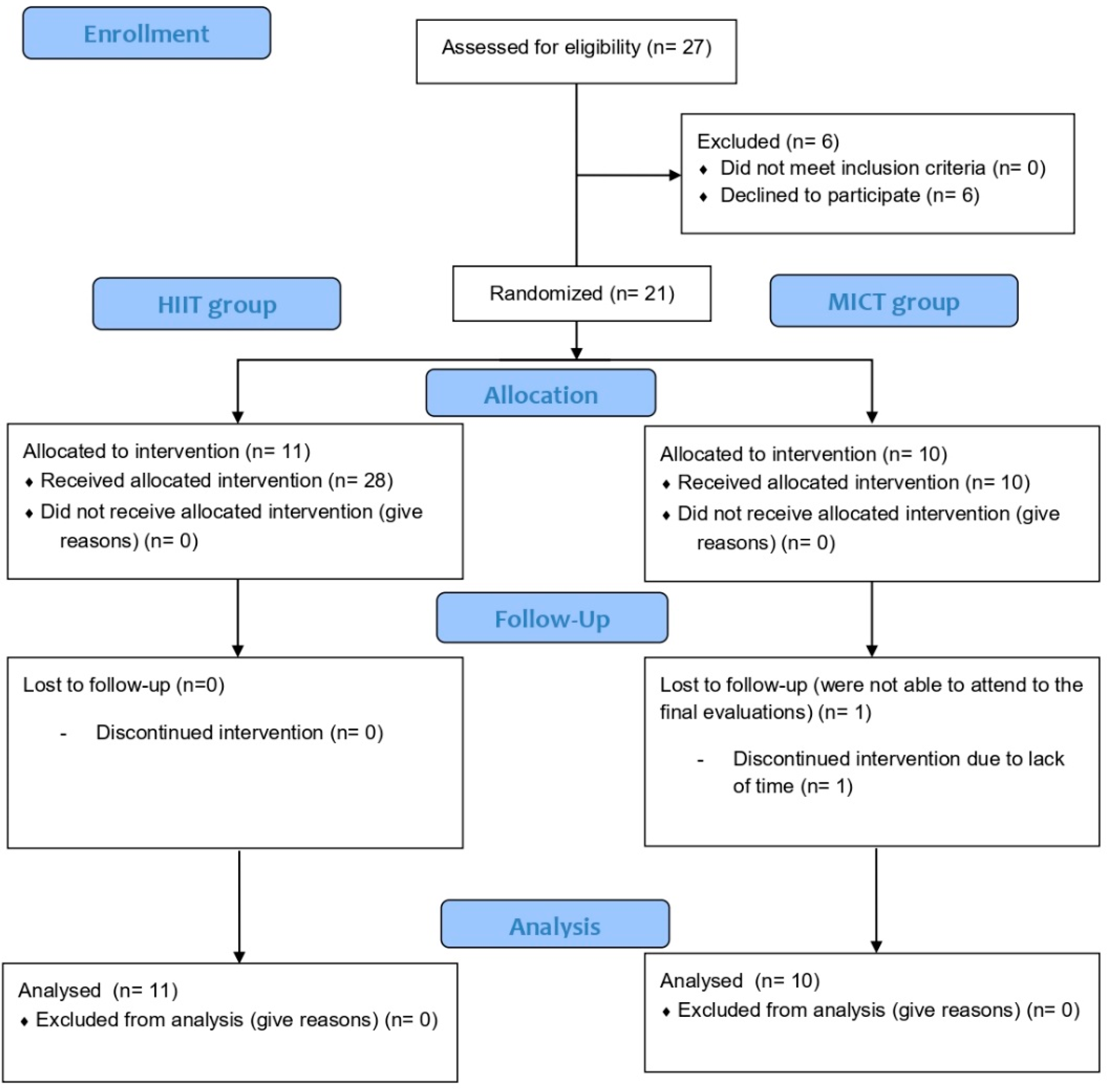
2.1. Trial Design
2.2. Participants
- Had previously completed phase II of the cardiac rehabilitation program.
- Had read, accepted, and signed the written informed consent.
- Had a condition that would make the high-intensity exercises contraindicated, such as retinopathy, musculoskeletal injuries, or major balance problems.
2.3. Intervention
- -
- HIIT: The training started with 8 min of warm-up. For the first 5 min, participants perform joint mobility, walk, or run at 50%HRmax. Then, three sets of three repetitions (each repetition lasted 10 s at 80%HRmax) with one minute of active recovery at 50%HRmax. After 5 min of active recovery, 10 sets of 15 s with 15 s of active recovery at 85%–90%HRmax were performed. The calm-down consisted of 3 min of active (walking around the tennis court) and 7 min of passive recovery. All the exercises performed under the HIIT approach were based on tennis.
- -
- MICT: The training started with 8 min of warm-up. For the first 5 min, participants have to perform joint mobility, walk, or run at 50%HRmax. Then, participants have to perform 40 min of tennis-based exercises. Since tennis is an intermittent sport, following the recommendation of Casasola [23] and García, Giraldo, Barrado, and Casasola [22], some adaptations were performed to maintain the intensity at 70%–85%HRmax during the session. For example, participants were allowed to let the ball bounce twice or using mainly doubles rather than singles games. Moreover, four different on-court movement intensities were introduced (i.e., walking slowly, walking fast, jogging, and running), to maintain the effort within the heart rate limits. Lastly, the calm-down consisted of 3 min of active (walking around the tennis court) and 7 min of passive recovery.
2.4. Outcomes
2.4.1. Physical Fitness and Body Composition
2.4.2. Heart Rate Variability
2.4.3. Quality of Life
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J. Executive summary: Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Dégano, I.R.; Elosua, R.; Kaski, J.C.; Fernández-Bergés, D.J.; Grau, M.; Marrugat, J. Estabilidad de la placa aterosclerótica y la paradoja del sur de Europa. Rev. Española Cardiol. 2013, 66, 56–62. [Google Scholar] [CrossRef]
- Cequier, Á. El registro MASCARA desenmascara la realidad asistencial del manejo de los síndromes coronarios agudos en España. Rev. Española Cardiol. (Engl. Ed.) 2008, 61, 793–796. [Google Scholar] [CrossRef] [Green Version]
- Dégano, I.R.; Elosua, R.; Marrugat, J. Epidemiology of acute coronary syndromes in Spain: Estimation of the number of cases and trends from 2005 to 2049. Rev. Española Cardiol. (Engl. Ed.) 2013, 66, 472–481. [Google Scholar] [CrossRef]
- Selig, S.E.; Levinger, I.; Williams, A.D.; Smart, N.; Holland, D.J.; Maiorana, A.; Green, D.J.; Hare, D.L. Exercise & Sports Science Australia Position Statement on exercise training and chronic heart failure. J. Sci. Med. Sport 2010, 13, 288–294. [Google Scholar]
- Thompson, D.R.; Yu, C.-M. Quality of life in patients with coronary heart disease-I: Assessment tools. Health Qual. Life Outcomes 2003, 1, 42. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Corra, U.; Dendale, P.; Frederix, I.; Prescott, E.; Schmid, J.P.; Cupples, M.; Deaton, C.; Doherty, P.; Giannuzzi, P.; et al. Challenges in secondary prevention after acute myocardial infarction: A call for action. Eur. J. Prev. Cardiol. 2016, 23, 1994–2006. [Google Scholar] [CrossRef]
- Francis, T.; Kabboul, N.; Rac, V.; Mitsakakis, N.; Pechlivanoglou, P.; Bielecki, J.; Alter, D.; Krahn, M. The effect of cardiac rehabilitation on health-related quality of life in patients with coronary artery disease: A meta-analysis. Can. J. Cardiol. 2019, 35, 352–364. [Google Scholar] [CrossRef]
- Lear, S.A.; Spinelli, J.J.; Linden, W.; Brozic, A.; Kiess, M.; Frohlich, J.J.; Ignaszewski, A. The Extensive Lifestyle Management Intervention (ELMI) after cardiac rehabilitation: A 4-year randomized controlled trial. Am. Heart J. 2006, 152, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Giannuzzi, P.; Temporelli, P.L.; Marchioli, R.; Maggioni, A.P.; Balestroni, G.; Ceci, V.; Chieffo, C.; Gattone, M.; Griffo, R.; Schweiger, C. Global secondary prevention strategies to limit event recurrence after myocardial infarction: Results of the GOSPEL study, a multicenter, randomized controlled trial from the Italian Cardiac Rehabilitation Network. Arch. Intern. Med. 2008, 168, 2194–2204. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, L.R.; Olsen, R.H.; Anholm, C.; Astrup, A.; Eugen-Olsen, J.; Fenger, M.; Simonsen, L.; Walzem, R.L.; Haugaard, S.B.; Prescott, E. Effects of 1 year of exercise training versus combined exercise training and weight loss on body composition, low-grade inflammation and lipids in overweight patients with coronary artery disease: A randomized trial. Cardiovasc. Diabetol. 2019, 18, 127. [Google Scholar] [CrossRef] [PubMed]
- Molino-Lova, R.; Pasquini, G.; Vannetti, F.; Paperini, A.; Forconi, T.; Polcaro, P.; Zipoli, R.; Cecchi, F.; Macchi, C. Effects of a structured physical activity intervention on measures of physical performance in frail elderly patients after cardiac rehabilitation: A pilot study with 1-year follow-up. Intern. Emerg. Med. 2013, 8, 581–589. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, D.; Forman, D.E. The importance of physical function as a clinical outcome: Assessment and enhancement. Clin. Cardiol. 2020, 43, 108–117. [Google Scholar] [CrossRef]
- Munk, P.S.; Butt, N.; Larsen, A.I. High-intensity interval exercise training improves heart rate variability in patients following percutaneous coronary intervention for angina pectoris. Int. J. Cardiol. 2010, 145, 312–314. [Google Scholar] [CrossRef]
- Fiogbe, E.; Ferreira, R.; Sindorf, M.A.G.; Tavares, S.A.; de Souza, K.P.; de Castro Cesar, M.; Lopes, C.R.; Moreno, M.A. Water exercise in coronary artery disease patients, effects on heart rate variability, and body composition: A randomized controlled trial. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2018, 23, e1713. [Google Scholar] [CrossRef]
- Thayer, J.F.; Ahs, F.; Fredrikson, M.; Sollers, J.J., III; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Dekker, J.M.; Crow, R.S.; Folsom, A.R.; Hannan, P.J.; Liao, D.; Swenne, C.A.; Schouten, E.G. Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes—The ARIC study. Circulation 2000, 102, 1239–1244. [Google Scholar] [CrossRef]
- Fang, S.C.; Wu, Y.L.; Tsai, P.S. Heart Rate Variability and Risk of All-Cause Death and Cardiovascular Events in Patients with Cardiovascular Disease: A Meta-Analysis of Cohort Studies. Biol. Res. Nurs. 2020, 22, 45–56. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Corra, U.; Benzer, W.; Bjarnason-Wehrens, B.; Dendale, P.; Gaita, D.; McGee, H.; Mendes, M.; Niebauer, J.; Zwisler, A.-D.O. Secondary prevention through cardiac rehabilitation: From knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- García, J.P.F.; Giraldo, V.M.A.; Barrado, J.J.G.; Casasola, C.D. Tennis training sessions as a rehabilitation instrument for patients after acute myocardial infarction. J. Sports Sci. Med. 2013, 12, 316. [Google Scholar] [PubMed]
- Casasola, C.D. Analysis of heart rate during a tennis training session and its relationship with heart-healthy index. J. Sport Health Res. 2010, 2, 26–34. [Google Scholar]
- Ribeiro, P.A.B.; Boidin, M.; Juneau, M.; Nigam, A.; Gayda, M. High-intensity interval training in patients with coronary heart disease: Prescription models and perspectives. Ann. Phys. Rehabil. Med. 2017, 60, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Keech, A.; Holgate, K.; Fildes, J.; Indraratna, P.; Cummins, L.; Lewis, C.; Yu, J. High-intensity interval training for patients with coronary artery disease: Finding the optimal balance. Int. J. Cardiol. 2020, 298, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Liou, K.; Ho, S.; Fildes, J.; Ooi, S.-Y. High intensity interval versus moderate intensity continuous training in patients with coronary artery disease: A meta-analysis of physiological and clinical parameters. Heart Lung Circ. 2016, 25, 166–174. [Google Scholar] [CrossRef]
- Hannan, A.L.; Hing, W.; Simas, V.; Climstein, M.; Coombes, J.S.; Jayasinghe, R.; Byrnes, J.; Furness, J. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis. Open Access J. Sports Med. 2018, 9, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Xie, B.; Yan, X.; Cai, X.; Li, J. Effects of high-intensity interval training on aerobic capacity in cardiac patients: A systematic review with meta-analysis. BioMed Res. Int. 2017, 2017, 5420840. [Google Scholar] [CrossRef]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Yan, A.T.; Yan, R.T.; Tan, M.; Casanova, A.; Labinaz, M.; Sridhar, K.; Fitchett, D.H.; Langer, A.; Goodman, S.G. Risk scores for risk stratification in acute coronary syndromes: Useful but simpler is not necessarily better. Eur. Heart J. 2007, 28, 1072–1078. [Google Scholar] [CrossRef]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Alfen, The Netherlands, 2017. [Google Scholar]
- Pauole, K.; Madole, K.; Garhammer, J.; Lacourse, M.; Rozenek, R. Reliability and validity of the T-test as a measure of agility, leg power, and leg speed in college-aged men and women. J. Strength Cond. Res. 2000, 14, 443–450. [Google Scholar]
- Phillips, W.T. Senior fitness test manual. J. Aging Phys. Act. 2002, 10, 110–111. [Google Scholar]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Hanson, L.C.; McBurney, H.; Taylor, N.F. The retest reliability of the six-minute walk test in patients referred to a cardiac rehabilitation programme. Physiother. Res. Int. 2012, 17, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.M.; Murthy, J.N.; Wollak, I.D.; Jackson, A.S. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm. Med. 2010, 10, 31. [Google Scholar] [CrossRef] [Green Version]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar]
- Da Costa de Rezende Barbosa, M.P.; da Silva, N.T.; de Azevedo, F.M.; Pastre, C.M.; Marques Vanderlei, L.C. Comparison of Polar ((R)) RS800G3 heart rate monitor with Polar ((R)) S810i and electrocardiogram to obtain the series of RR intervals and analysis of heart rate variability at rest. Clin. Physiol. Funct. Imaging 2016, 36, 112–117. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV–heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Ware, J., Jr.; Kosinski, M.; Turner-Bowker, D.J.R.I.Q.I. How to Score Version 2 of the SF-12® Health Survey (with a Supplement Documenting Version 1); Lincoln: Dearborn, MI, USA, 2002. [Google Scholar]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ (Clin. Res. Ed.) 2009, 338, b2393. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coolican, H. Research Methods and Statistics in Psychology; Psychology Press: Oxford, UK, 2017. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 289–300. [Google Scholar] [CrossRef]
- Tuna, H.D.; Edeer, A.O.; Malkoc, M.; Aksakoglu, G. Effect of age and physical activity level on functional fitness in older adults. Eur. Rev. Aging Phys. Act. 2009, 6, 99. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.J.; Schachter, C.L.; Overend, T.J.; Peloso, P.M.; Barber, K.A. Exercise for fibromyalgia: A systematic review. J. Rheumatol. 2008, 35, 1130–1144. [Google Scholar] [PubMed]
- Buckner, S.L.; Dankel, S.J.; Bell, Z.W.; Abe, T.; Loenneke, J.P. The Association of Handgrip Strength and Mortality: What Does It Tell Us and What Can We Do with It? Rejuvenation Res. 2019, 22, 230–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavasini, R.; Serenelli, M.; Celis-Morales, C.A.; Gray, S.R.; Izawa, K.P.; Watanabe, S.; Colin-Ramirez, E.; Castillo-Martínez, L.; Izumiya, Y.; Hanatani, S. Grip strength predicts cardiac adverse events in patients with cardiac disorders: An individual patient pooled meta-analysis. Heart 2019, 105, 834–841. [Google Scholar] [CrossRef]
- LiQiang, S.; JinMei, F.; ShunLi, S.; GuangGao, Z.; Wei, C.; ChuanChuan, D.; MingHui, Q. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Merellano-Navarro, E.; Gusi, N. Physical Exercise Improves Heart Rate Variability in Patients with Type 2 Diabetes: A Systematic Review. Curr. Diabetes Rep. 2017, 17, 110. [Google Scholar] [CrossRef]
- Hernando, D.; Kähönen, M.; Lázaro, J.; Lehtinen, R.; Nieminen, T.; Nikus, K.; Lehtimäki, T.; Bailón, R.; Viik, J. Coronary artery disease diagnosis by means of heart rate variability analysis using respiratory information. In EMBEC & NBC 2017; Springer: Berlin, Germany, 2017; pp. 270–273. [Google Scholar]
- Badrov, M.B.; Wood, K.N.; Lalande, S.; Sawicki, C.P.; Borrell, L.J.; Barron, C.C.; Vording, J.L.; Fleischhauer, A.; Suskin, N.; McGowan, C.L. Effects of 6 Months of Exercise-Based Cardiac Rehabilitation on Autonomic Function and Neuro-Cardiovascular Stress Reactivity in Coronary Artery Disease Patients. J. Am. Heart Assoc. 2019, 8, e012257. [Google Scholar] [CrossRef]
- Sandercock, G.R.H.; Hodges, L.D.; Das, S.K.; Brodie, D.A. The impact of short term supervised and home-based walking programmes on heart rate variability in patients with peripheral arterial disease. J. Sports Sci. Med. 2007, 6, 471–476. [Google Scholar]
- Currie, K.D.; Rosen, L.M.; Millar, P.J.; McKelvie, R.S.; MacDonald, M.J. Heart rate recovery and heart rate variability are unchanged in patients with coronary artery disease following 12 weeks of high-intensity interval and moderate-intensity endurance exercise training. Appl. Physiol. Nutr. Metab. 2013, 38, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Hottenrott, K.; Hoos, O.; Esperer, H.D. Heart rate variability and physical exercise. Current status. Herz 2006, 31, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Collado-Mateo, D.; Domínguez-Muñoz, F.J.; Gusi, N.; Fuentes-Garcia, J.P. Effects of exergames on heart rate variability of women with fibromyalgia: A randomized controlled trial. Sci. Rep. 2020, 10, 5168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de la Cuerda, R.C.; Diego, I.M.A.; Martín, J.J.A.; Sánchez, A.M.; Page, J.C.M. Cardiac rehabilitation programs and health-related quality of life. State of the art. Rev. Española Cardiol. (Engl. Ed.) 2012, 65, 72–79. [Google Scholar] [CrossRef]
- Seki, E.; Watanabe, Y.; Sunayama, S.; Iwama, Y.; Shimada, K.; Kawakami, K.; Sato, M.; Sato, H.; Mokuno, H.; Daida, H. Effects of phase III cardiac rehabilitation programs on health-related quality of life in elderly patients with coronary artery disease. Circ. J. 2003, 67, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Villelabeitia Jaureguizar, K.; Vicente-Campos, D.; Ruiz Bautista, L.; Hernandez de la Pena, C.; Arriaza Gómez, M.J.; Calero Rueda, M.J.; Fernandez Mahillo, I. Effect of high-intensity interval versus continuous exercise training on functional capacity and quality of life in patients with coronary artery disease. J. Cardiopulm. Rehabil. Prev. 2016, 36, 96–105. [Google Scholar] [CrossRef]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-intensity interval training in cardiac rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Smith, J.; Garton-Smith, J.; Briffa, T.; Maiorana, A. The development of a new cardiac rehabilitation needs assessment tool (CRNAT) for individualised secondary prevention. Heart Lung Circ. 2015, 24, 458–464. [Google Scholar] [CrossRef]
- Reid, R.D.; Morrin, L.I.; Higginson, L.A.J.; Wielgosz, A.; Blanchard, C.; Beaton, L.J.; Nelson, C.; McDonnell, L.; Oldridge, N.; Wells, G.A. Motivational counselling for physical activity in patients with coronary artery disease not participating in cardiac rehabilitation. Eur. J. Prev. Cardiol. 2012, 19, 161–166. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Fiala, B.; Conner, M. A review and meta-analysis of affective judgments and physical activity in adult populations. Ann. Behav. Med. 2009, 38, 180–204. [Google Scholar] [CrossRef]
- Ryan, R.M.; Williams, G.C.; Patrick, H.; Deci, E.L. Self-determination theory and physical activity: The dynamics of motivation in development and wellness. Hell. J. Psychol. 2009, 6, 107–124. [Google Scholar]


{kind=link}
| All (n = 21) | HIIT Group (n = 11) | MICT Group (n = 10) | p-value * | |
|---|---|---|---|---|
| Age (years) | 55.85 (5.69) | 55.27 (7.13) | 56.55 (3.50) | 0.148 |
| Weight (kg) | 86.67 (13.68) | 87.87 (16.64) | 85.34 (10.23) | 0.751 |
| BMI (kg/m2) | 30.54 (4.22) | 31.04 (5.14) | 29.98 (3.11) | 0.438 |
| 6-MWT (m) | 583.26 (72.40) | 584.09 (82.71) | 603.54 (83.62) | 0.218 |
| SDNN | 40.88 (19.19) | 50.89 (22.71) | 40.18 (21.66) | 0.425 |
| MCS | 35.24 (5.64) | 35.91 (6.56) | 35.01 (4.73) | 0.573 |
| PCS | 35.48 (5.64) | 35.99 (7.53) | 34.41 (2.42) | 0.888 |
| Variables | Within Group Comparison | Between Group Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Z | p-value * | Effect Size | Z | p-value * | Effect Size | ||
| Body composition | |||||||||
| BMI (kg/m2) | HIIT | 31.04 (5.14) | 31.34 (5.33) | −1.736 | 0.083 | −0.523 | −1.096 | 0.273 | −0.239 |
| MICT | 29.98 (3.11) | 29.92 (3.16) | −0.256 | 0.798 | −0.080 | ||||
| Fat Mass (%) | HIIT | 26.52 (6.54) | 27.69 (6.07) | −1.511 | 0.131 | −0.455 | −1.797 | 0.144 | −0.392 |
| MICT | 27.04 (4.56) | 26.23 (5.51) | −0.051 | 0.959 | −0.016 | ||||
| Physical Fitness | |||||||||
| Bimanual Handgrip (kg) | HIIT | 85.91 (13.40) | 86.82 (13.04) | −0.934 | 0.350 | −0.281 | −2.113 | 0.035* | −0.461 |
| MICT | 81.32 (9.71) | 78.77 (9.26) | −1.478 | 0.139 | −0.467 | ||||
| Horizontal Jump (m) | HIIT | 1.79 (0.45) | 1.82 (0.39) | −0.204 | 0.838 | −0.061 | −0.681 | 0.496 | −0.149 |
| MICT | 1.67 (0.38) | 1.73 (0.25) | −0.700 | 0.484 | −0.221 | ||||
| T-test (s) | HIIT | 14.90 (1.98) | 11.89 (1.56) | −2.934 | 0.003* | −0.884 | −1.620 | 0.157 | −0.353 |
| MICT | 14.94 (1.92) | 13.27 (1.17) | −1.988 | 0.047* | −0.629 | ||||
| Back scratch (cm) | HIIT | −14.09 (14.00) | −10.09 (12.09) | −2.548 | 0.011* | −0.768 | −1.420 | 0.155 | −0.310 |
| MICT | − 8.00 (12.89) | −5.65 (8.17) | −1.785 | 0.074 | −0.564 | ||||
| Sit and reach (cm) | HIIT | −7.64 (15.49) | 2.27 (11.38) | −2.934 | 0.008* | −0.884 | −0.247 | 0.805 | −0.054 |
| MICT | −7.60 (18.07) | −5.65 (8.17) | −0.667 | 0.505 | −0.211 | ||||
| 6-MWT (m) | HIIT | 584.09 (82.71) | 603.54 (83.62) | −1.156 | 0.248 | −0.348 | −1.479 | 0.139 | −0.322 |
| MICT | 569.22 (41.53) | 560.94 (53.13) | −0.866 | 0.386 | −0.273 | ||||
| VO2max estimation (mL/kg/min) | HIIT | 18.38 (1.90) | 18.83 (1.92) | −1.156 | 0.248 | −0.348 | −0.991 | 0.322 | −0.216 |
| MICT | 18.01 (1.01) | 17.95 (1.25) | −0.420 | 0.674 | −0.133 | ||||
| HRV Measures | Within Group Comparison | Between Group Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Z | p-value * | Effect Size | Z | p-value * | Effect Size | ||
| Heart Rate (bpm) | HIIT | 64.16 (7.10) | 62.93 (10.31) | −0.711 | 0.477 | −0.214 | −0.563 | 0.573 | −0.123 |
| MICT | 67.55 (13.60) | 67.84 (11.18) | −0.255 | 0.799 | −0.081 | ||||
| SDNN | HIIT | 50.89 (22.71) | 43.87 (19.75) | −0.978 | 0.328 | −0.295 | −0.423 | 0.673 | −0.092 |
| MICT | 40.18 (21.66) | 39.60 (19.39) | −0.968 | 0.330 | −0.306 | ||||
| RMSSD | HIIT | 34.14 (23.54) | 34.40 (21.59) | −0.178 | 0.859 | −0.054 | −0.810 | 0.418 | −0.177 |
| MICT | 25.74 (18.38) | 25.30 (25.90) | −1.478 | 0.139 | −0.467 | ||||
| Pnn50 | HIIT | 12.34 (16.01) | 13.40 (19.50) | −0.178 | 0.859 | −0.054 | −0.493 | 0.622 | −0.108 |
| MICT | 6.93 (13.22) | 7.63 (15.31) | −1.423 | 0.155 | −0.450 | ||||
| HF | HIIT | 28.00 (15.11) | 36.06 (20.19) | −1.334 | 0.182 | −0.402 | −1.972 | 0.100 | −0.430 |
| MICT | 28.60 (18.22) | 22.78 (11.03) | −1.326 | 0.185 | −0.419 | ||||
| LF | HIIT | 71.89 (15.07) | 63.77 (20.23) | −1.334 | 0.182 | −0.402 | −1.831 | 0.100 | −0.400 |
| MICT | 71.32 (18.27) | 74.90 (12.94) | −0.764 | 0.445 | −0.242 | ||||
| LF/HF | HIIT | 3.58 (2.32) | 3.32 (3.97) | −0.800 | 0.424 | −0.241 | −1.408 | 0.159 | −0.307 |
| MICT | 4.24 (4.13) | 6.51 (9.66) | −0.968 | 0.333 | −0.306 | ||||
| SD1 | HIIT | 24.19 (16.69) | 24.37 (15.30) | −0.178 | 0.859 | −0.054 | −0.986 | 0.324 | −0.215 |
| MICT | 18.22 (13.00) | 17.48 (17.75) | −1.478 | 0.139 | −0.467 | ||||
| SD2 | HIIT | 67.25 (28.82) | 56.27 (25.18) | −1.245 | 0.213 | −0.375 | −0.352 | 0.725 | −0.077 |
| MICT | 52.97 (29.06) | 52.86 (23.77) | −0.764 | 0.445 | −0.242 | ||||
| SampEn | HIIT | 1.46 (0.19) | 1.45 (0.34) | −0.178 | 0.859 | −0.054 | −0.986 | 0.324 | −0.215 |
| MICT | 1.32 (0.22) | 1.18 (0.27) | −1.784 | 0.074 | −0.564 | ||||
| Quality of Life | Within Group Comparison | Between Group Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Z | p-value * | Effect Size | Z | p-value * | Effect Size | ||
| Summary Scores | |||||||||
| MCS | HIIT | 35.99 (7.53) | 54.47 (3.38) | −2.934 | 0.003 * | −0.884 | −0.070 | 0.944 | −0.015 |
| MICT | 34.41 (2.42) | 53.44 (4.78) | −2.803 | 0.005 * | −0.886 | ||||
| PCS | HIIT | 35.91 (6.56) | 28.47 (3.90) | −2.934 | 0.003 * | −0.884 | −0.282 | 0.778 | −0.061 |
| MICT | 35.01 (4.73) | 27.77 (3.70) | −2.599 | 0.009 * | −0.822 | ||||
| SF-12v2 domains | |||||||||
| PF | HIIT | 22.73 (28.40) | 13.64 (17.19) | −1.081 | 0.279 | −0.326 | −1.120 | 0.263 | −0.244 |
| MICT | 20.00 (32.91) | 16.67 (25.00) | −0.447 | 0.655 | −0.141 | ||||
| RP | HIIT | 70.45 (14.00) | 81.82 (23.29) | −1.172 | 0.241 | −0.353 | 0.349 | 0.727 | 0.076 |
| MICT | 65.00 (19.36) | 73.61 (19.21) | −1.421 | 0.155 | −0.449 | ||||
| BP | HIIT | 18.18 (25.23) | 2.27 (7.54) | −2.121 | 0.034 * | −0.639 | −0.676 | 0.499 | −0.147 |
| MICT | 15.00 (26.87) | 5.56 (11.02) | −1.633 | 0.102 | −0.516 | ||||
| GH | HIIT | 52.73 (19.28) | 64.09 (20.59) | −1.769 | 0.077 | −0.533 | −0.301 | 0.763 | −0.006 |
| MICT | 50.50 (20.88) | 58.89 (24.59) | −1.852 | 0.064 | −0.585 | ||||
| VF | HIIT | 31.82 (29.77) | 75.00 (15.81) | −2.595 | 0.009 * | −0.782 | −1.184 | 0.237 | −0.258 |
| MICT | 37.50 (21.24) | 63.89 (18.16) | −1.852 | 0.064 | −0.585 | ||||
| SF | HIIT | 29.55 (33.20) | 6.82 (16.17) | −1.638 | 0.101 | −0.494 | −0.845 | 0.398 | −0.184 |
| MICT | 20.00 (22.97) | 11.11 (22.05) | −1.300 | 0.194 | −0.411 | ||||
| RE | HIIT | 78.41 (19.44) | 79.54 (20.37) | −0.322 | 0.748 | −0.010 | −1.011 | 0.312 | −0.220 |
| MICT | 75.00 (22.82) | 86.11 (17.05) | −1.469 | 0.142 | −0.464 | ||||
| MH | HIIT | 19.32 (15.17) | 86.36 (11.80) | −2.952 | 0.003 * | −0.890 | −0.231 | 0.817 | −0.050 |
| MICT | 15.00 (19.36) | 79.17 (21.65) | −2.533 | 0.011 * | −0.801 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villafaina, S.; Giménez-Guervós Pérez, M.J.; Fuentes-García, J.P. Comparative Effects of High-Intensity Interval Training vs Moderate-Intensity Continuous Training in Phase III of a Tennis-Based Cardiac Rehabilitation Program: A Pilot Randomized Controlled Trial. Sustainability 2020, 12, 4134. https://doi.org/10.3390/su12104134
Villafaina S, Giménez-Guervós Pérez MJ, Fuentes-García JP. Comparative Effects of High-Intensity Interval Training vs Moderate-Intensity Continuous Training in Phase III of a Tennis-Based Cardiac Rehabilitation Program: A Pilot Randomized Controlled Trial. Sustainability. 2020; 12(10):4134. https://doi.org/10.3390/su12104134
Chicago/Turabian StyleVillafaina, Santos, María José Giménez-Guervós Pérez, and Juan Pedro Fuentes-García. 2020. "Comparative Effects of High-Intensity Interval Training vs Moderate-Intensity Continuous Training in Phase III of a Tennis-Based Cardiac Rehabilitation Program: A Pilot Randomized Controlled Trial" Sustainability 12, no. 10: 4134. https://doi.org/10.3390/su12104134