
Coactivation of the Pelvic Floor and Gluteus Medius Muscles While Walking and Running in Female Runners

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
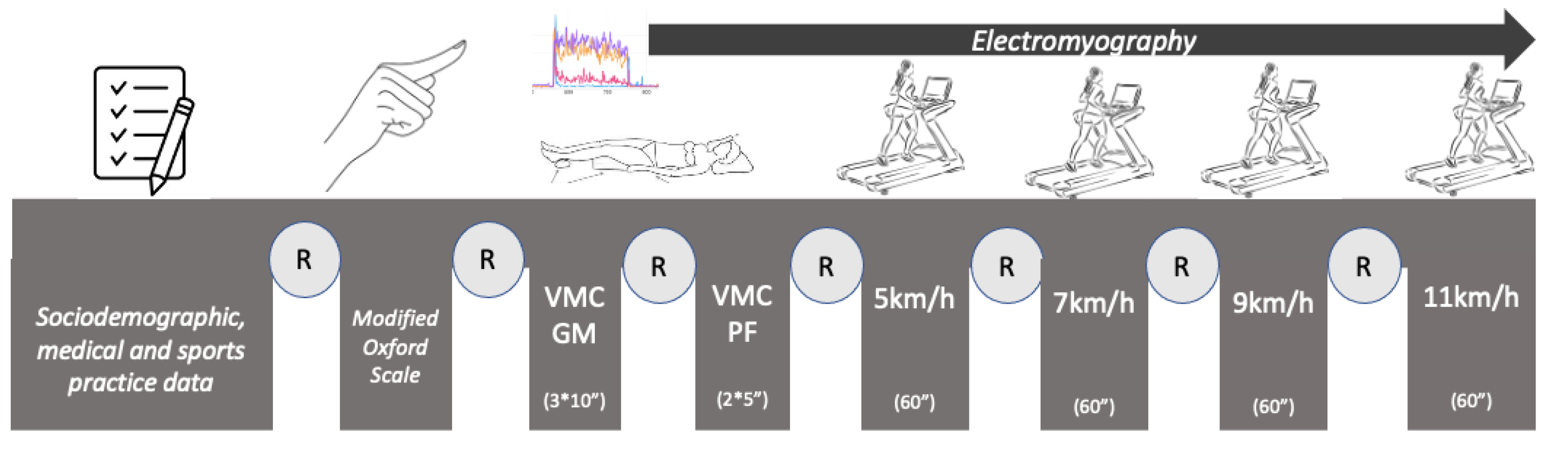
2.1. Study Design
2.2. Participants
2.3. Instrumentation and Data Collection
2.3.1. Sociodemographic, Medical, and Sports Practice Data
2.3.2. Pelvic-Floor-Muscle Assessment: Modified Oxford Scale
2.3.3. Electromyography
- -
- Maximum voluntary isometric contractions (MVCs) of the GM [40]: Three MVCs were measured, each held for 10 s and with a 60 s rest between each contraction [41,42]. From the data reported in the EMG, the maximum amplitude (MVCpeak) and the result of the arithmetic mean of the three maximum peaks of each contraction for the right and left GM muscles (MVCpeak_GM_RGM and MVCpeak_GM_LGM) and for the right and left PFMs (MVCpeak_GM_RPFM and MVCpeak_GM_LPFM) were calculated. The mean amplitude (MVCmean) was the result of the average muscle activity during the 10 s of each contraction for the right and left GM muscles (MVC-mean_GM_LGM and MVCmean_GM_RGM) and for the right and left PFMs (MVCmean_GM_RPFM and MVCmean_GM_LPFM).
- -
- Maximum voluntary contractions (MVCs) of the PFMs [35,43,44]: Two MVCs were measured, each held for 5 s and with a 30 s rest between each contraction [44]. The reference value set as 100% for EMG normalization (MVCpeak) was calculated as the mean of the peak values of two maximum voluntary contractions (30 s) for the GM (MVCpeak_PFM_RGM and MVCpeak_PFM_LGM) and the PFMs (MVCpeak_PFM_RPFM and MVCpeak_PFM_LPFM). The mean amplitude (MVCmean) was the result of the average muscle activity during the 30 s of each contraction for the right and left GM muscles (MVCmean_PFM_RGM and MVCmean_PFM_LGM) and for the right and left PFMs (MVCmean_PFM_RPFM and MVCmean_PFM_LPFM).
- -
- Muscle ratio: The muscle relationships were calculated by dividing the muscles into pairs. For example, the ratio of the average amplitude during the maximum-GM-contraction test of the right PFM to the right GM was calculated as “Ratio_RGM_RPFM = MVCmean_GM_RGM/MVC-mean_GM_RPFM”. This was replicated for each value.
2.3.4. Recording of EMG Activity at Different Walking Speeds
2.4. Statistical Analysis
3. Results
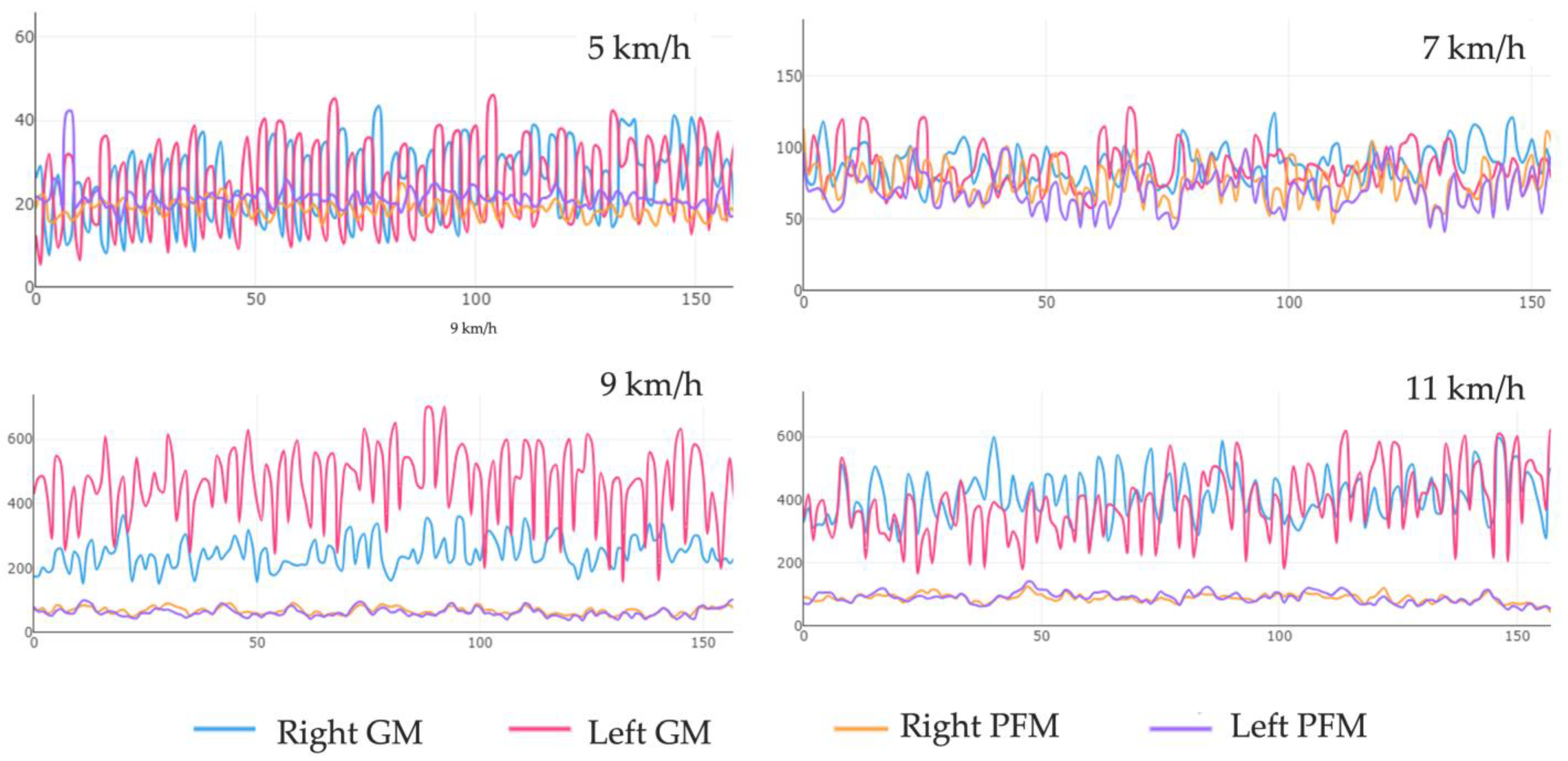
3.1. Isolated-Muscle Activation of the GM and PF in Static Tests and at Different Walking and Running Speeds
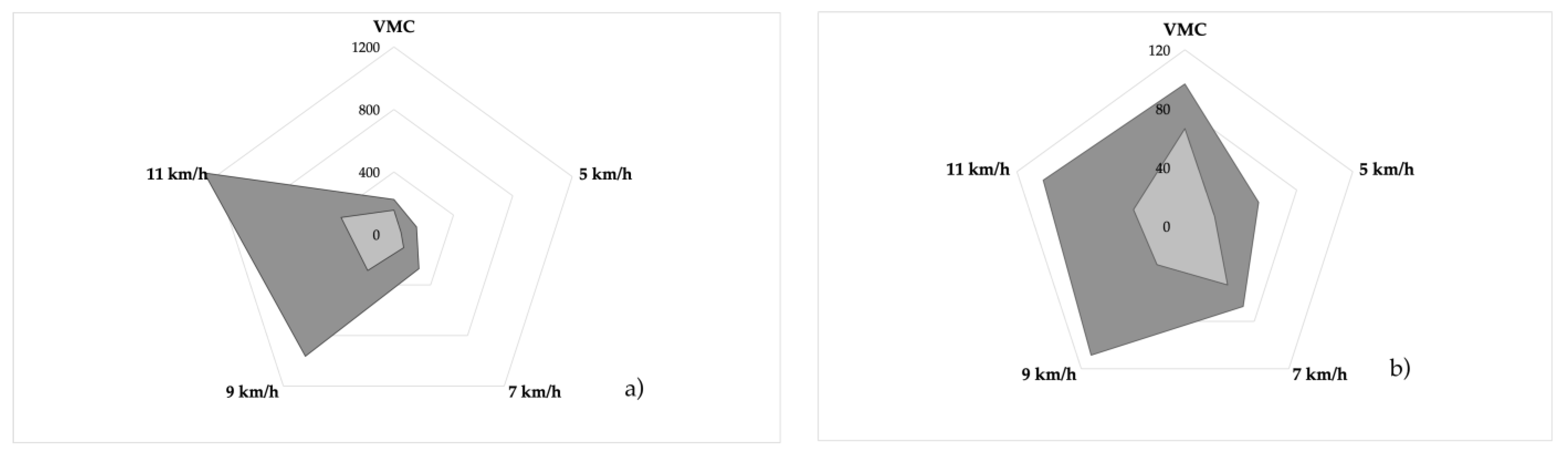
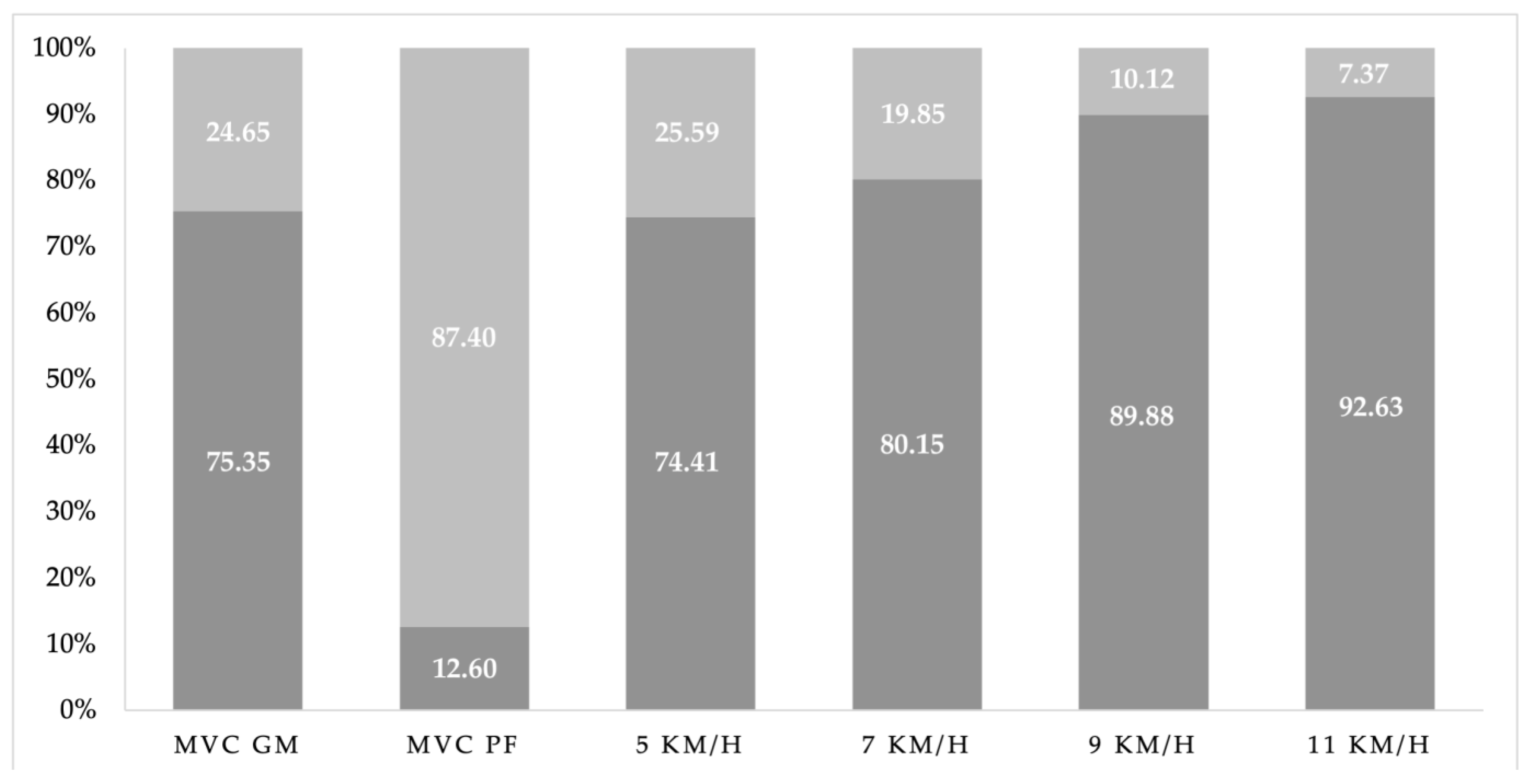
3.2. Isolated-Muscle Ratios of the GM and PF in Static Tests and at Different Running Speeds
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stafford, R.E.; Ashton-Miller, J.A.; Sapsford, R.; Hodges, P.W. Activation of the Striated Urethral Sphincter to Maintain Continence during Dynamic Tasks in Healthy Men. Neurourol. Urodyn. 2012, 31, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Leetun, D.T.; Ireland, M.L.; Willson, J.D.; Ballantyne, B.T.; Davis, I.M. Core stability measures as risk factors for lower extremity injury in athletes. Med. Sci. Sports Exerc. 2004, 36, 926–934. [Google Scholar] [CrossRef]
- Grimaldi, A. Assessing lateral stability of the hip and pelvis. Man. Ther. 2011, 16, 26–32. [Google Scholar] [CrossRef]
- Junginger, B.; Baessler, K.; Sapsford, R.; Hodges, P.W. Effect of Abdominal and Pelvic Floor Tasks on Muscle Activity, Abdominal Pressure and Bladder Neck. Int. Urogynecol. J. 2010, 21, 69–77. [Google Scholar] [CrossRef]
- Bø, K.; Stien, R. Needle Emg Registration of Striated Urethral Wall and Pelvic Floor Muscle Activity Patterns during Cough, Valsalva, Abdominal, Hip Adductor, and Gluteal Muscle Contractions in Nulliparous Healthy Females. Neurourol. Urodyn. 1994, 13, 35–41. [Google Scholar] [CrossRef]
- Carvalhais, A.; Jorge, R.N.; Bø, K. Performing High-Level Sport Is Strongly Associated with Urinary Incontinence in Elite Athletes : A Comparative Study of 372 Elite Female Athletes and 372 Controls. Br. J. Sports Med. 2018, 52, 1586–1590. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.B.D.; Szkudlarek, A.C.; Gallo, R.B.S.; Valadão, A.P.M.; Avila, M.A.; Driusso, P.K.R. Verbal and Visual Feedback Immediately Affect the Electromyographic Activity of Female Pelvic Floor Muscles. J. Manip. Physiol. Ther. 2021, 44, 743–750. [Google Scholar] [CrossRef]
- Tscharner, V. Von Intensity Analysis in Time-Frequency Space of Surface Myoelectric Signals by Wavelets of Specified Resolution. J. Electromyogr. Kinesiol. 2000, 10, 433–445. [Google Scholar] [CrossRef]
- Koenig, I.; Eichelberger, P.; Blasimann, A.; Hauswirth, A.; Baeyens, J.P.; Radlinger, L. Wavelet Analyses of Electromyographic Signals Derived from Lower Extremity Muscles While Walking or Running: A Systematic Review. PLoS ONE 2018, 13, e0206549. [Google Scholar] [CrossRef]
- Von Tscharner, V.; Goepfert, B. Estimation of the Interplay between Groups of Fast and Slow Muscle Fibers of the Tibialis Anterior and Gastrocnemius Muscle While Running. J. Electromyogr. Kinesiol. 2006, 16, 188–197. [Google Scholar] [CrossRef]
- Madill, S.J.; McLean, L. Quantification of Abdominal and Pelvic Floor Muscle Synergies in Response to Voluntary Pelvic Floor Muscle Contractions. J. Electromyogr. Kinesiol. 2008, 18, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W.; Sapsford, R.; Pengel, L.H.M. Postural and Respiratory Functions of the Pelvic Floor Muscles. Neurourol. Urodyn. 2007, 26, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl, J.; Kvist, J.; Gutke, A.; Oberg, B. The Postural Response of the Pelvic Floor Muscles during Limb Movements: A Methodological Electromyography Study in Parous Women without Lumbopelvic Pain. Clin. Biomech. 2009, 24, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U. Is There an Association between the Quality of Life of Incontinence Symptoms and the Hip Joint Muscles Strength in Women with Stress Urinary Incontinence? J. Musculoskelet. Sci. Technol. 2022, 6, 15–21. [Google Scholar] [CrossRef]
- Martinez, R.F.L.; Sato, T.O.; Silva, J.B.D.; Figueiredo, V.B.D.; Avila, M.A.; Driusso, P. Pelvic Floor Muscle Activity during Coughing and Valsalva Maneuver in Continent Women and Women with Stress Urinary Incontinence: A Systematic Review. Phys. Ther. Rev. 2023, 28, 39–48. [Google Scholar] [CrossRef]
- Berger, R.E. Urologic Myofascial Pain Syndromes. J. Urol. 2005, 174, 942. [Google Scholar] [CrossRef] [PubMed]
- Jantos, M. Pelvic Floor Disorders: A Multidisciplinary Textbook; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Ojukwu, C.P.; Ojukwu, C.S.; Okemuo, A.J.; Igwe, S.E.; Ede, S.S.; Ezeigwe, A.U.; Mbah, C.G. Comparative Effects of Selected Abdominal and Lower Limb Exercises in the Recruitment of the Pelvic Floor Muscles: Determining Adjuncts to Kegel’s Exercises. J. Bodyw. Mov. Ther. 2022, 29, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Kinney, A.L.; Giel, M.; Harre, B.; Heffner, K.; McCullough, T.; Savino, M.; Scott, A.; Barrios, J.A. Surface Electromyography of the Internal and External Oblique Muscles during Isometric Tasks Targeting the Lateral Trunk. J. Sport Rehabil. 2020, 30, 255–260. [Google Scholar] [CrossRef]
- Williams, A.M.M.; Sato-Klemm, M.; Deegan, E.G.; Eginyan, G.; Lam, T. Characterizing Pelvic Floor Muscle Activity During Walking and Jogging in Continent Adults: A Cross-Sectional Study. Front. Hum. Neurosci. 2022, 16, 912839. [Google Scholar] [CrossRef]
- Floyd, W.F.; Walls, W.E. Electromyography of the Sphincter Ani Externus in Man. J. Physiol. 1953, 122, 599–609. [Google Scholar] [CrossRef]
- Peschers, U.M.; Gingelmaier, A.; Jundt, K.; Leib, B.; Dimpfl, T. Evaluation of Pelvic Floor Muscle Strength Using Four Different Techniques. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2001, 12, 27–30. [Google Scholar] [CrossRef]
- Betsch, M.; Wild, M.; Große, B.; Rapp, W.; Horstmann, T. The Effect of Simulating Leg Length Inequality on Spinal Posture and Pelvic Position: A Dynamic Rasterstereographic Analysis. Eur. Spine J. 2012, 21, 691–697. [Google Scholar] [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Laycock, J.; Jerwood, D. Pelvic Floor Muscle Assessment: The PERFECT Scheme. Physiotherapy 2001, 87, 631–642. [Google Scholar] [CrossRef]
- Ferreira, C.H.J.; Barbosa, P.B.; de Oliveira Souza, F.; Antônio, F.I.; Franco, M.M.; Bø, K. Inter-Rater Reliability Study of the Modified Oxford Grading Scale and the Peritron Manometer. Physiotherapy 2011, 97, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Dumoulin, C.; Hay-Smith, J. Pelvic Floor Muscle Training versus No Treatment, or Inactive Control Treatments, for Urinary Incontinence in Women. Cochrane Database Syst. Rev. 2010, 10, CD005654. [Google Scholar] [CrossRef]
- Voorham, J.C.; De Wachter, S.; Van den Bos, T.W.L.; Putter, H.; Lycklama, À.; Nijeholt, G.A.; Voorham-van der Zalm, P.J. The Effect of EMG Biofeedback Assisted Pelvic Floor Muscle Therapy on Symptoms of the Overactive Bladder Syndrome in Women: A Randomized Controlled Trial. Neurourol. Urodyn. 2017, 36, 1796–1803. [Google Scholar] [CrossRef]
- Hollman, J.H.; Galardi, C.M.; Lin, I.H.; Voth, B.C.; Whitmarsh, C.L. Frontal and Transverse Plane Hip Kinematics and Gluteus Maximus Recruitment Correlate with Frontal Plane Knee Kinematics during Single-Leg Squat Tests in Women. Clin. Biomech. 2014, 29, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Banos, O.; Moral-Munoz, J.A.; Diaz-Reyes, I.; Arroyo-Morales, M.; Damas, M.; Herrera-Viedma, E.; Hong, C.S.; Lee, S.; Pomares, H.; Rojas, I.; et al. MDurance: A Novel Mobile Health System to Support Trunk Endurance Assessment. Sensors 2015, 15, 13159–13183. [Google Scholar] [CrossRef] [PubMed]
- Molina-Molina, A.; Ruiz-Malagón, E.J.; Carrillo-Pérez, F.; Roche-Seruendo, L.E.; Damas, M.; Banos, O.; García-Pinillos, F. Validation of mDurance, A Wearable Surface Electromyography System for Muscle Activity Assessment. Front. Physiol. 2020, 11, 1556. [Google Scholar] [CrossRef]
- Carrillo-Perez, F.; Diaz-Reyes, I.; Damas, M.; Banos, O.; Soto-Hermoso, V.M.; Molina-Molina, A. A Novel Automated Algorithm for Computing Lumbar Flexion Test Ratios Enhancing Athletes Objective Assessment of Low Back Pain. In Proceedings of the 6th International Congress on Sport Sciences Research and Technology Support, Seville, Spain, 20–21 September 2018; pp. 34–39. [Google Scholar]
- Filter, A.; Olivares-Jabalera, J.; Santalla, A.; Morente-Sánchez, J.; Robles-Rodríguez, J.; Requena, B.; Loturco, I. Curve Sprinting in Soccer: Kinematic and Neuromuscular Analysis. Int. J. Sports Med. 2020, 41, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Koenig, I.; Eichelberger, P.; Leitner, M.; Moser, H.; Kuhn, A.; Taeymans, J.; Radlinger, L. Pelvic Floor Muscle Activity Patterns in Women with and without Stress Urinary Incontinence While Running. Ann. Phys. Rehabil. Med. 2020, 63, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Luginbuehl, H.; Naeff, R.; Zahnd, A.; Baeyens, J.P.; Kuhn, A.; Radlinger, L. Pelvic Floor Muscle Electromyography during Different Running Speeds: An Exploratory and Reliability Study. Arch. Gynecol. Obstet. 2016, 293, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Ben Ami, N.; Dar, G. What Is the Most Effective Verbal Instruction for Correctly Contracting the Pelvic Floor Muscles? Neurourol. Urodyn. 2018, 37, 2904–2910. [Google Scholar] [CrossRef] [PubMed]
- Sadler, S.; Spink, M.; De Jonge, X.J.; Chuter, V. An Exploratory Study Investigating the Effect of Foot Type and Foot Orthoses on Gluteus Medius Muscle Activity. BMC Musculoskelet. Disord. 2020, 21, 655. [Google Scholar] [CrossRef]
- Bussey, M.D.; Aldabe, D.; Adhia, D.; Mani, R. Reliability of Surface Electromyography Activity of Gluteal and Hamstring Muscles during Sub-Maximal and Maximal Voluntary Isometric Contractions. Musculoskelet. Sci. Pract. 2018, 34, 103–107. [Google Scholar] [CrossRef]
- Merletti, R.; Hermens, H. Introduction to the Special Issue on the SENIAM European Concerted Action. J. Electromyogr. Kinesiol. 2000, 10, 283–286. [Google Scholar] [CrossRef]
- Boren, K.; Conrey, C.; Le Coguic, J.; Paprocki, L.; Voight, M.; Robinson, T.K. Electromyographic Analysis of Gluteus Medius and Gluteus Maximus during Rehabilitation Exercises. Int. J. Sports Phys. Ther. 2011, 6, 206–223. [Google Scholar]
- Andersson, E.A.; Oddsson, L.I.E.; Grundström, H.; Nilsson, J.; Thorstensson, A. EMG Activities of the Quadratus Lumborum and Erector Spinae Muscles during Flexion-Relaxation and Other Motor Tasks. Clin. Biomech. 1996, 11, 392–400. [Google Scholar] [CrossRef]
- Sadler, S.; Cassidy, S.; Peterson, B.; Spink, M.; Chuter, V. Gluteus Medius Muscle Function in People with and without Low Back Pain: A Systematic Review. BMC Musculoskelet. Disord. 2019, 20, 463. [Google Scholar] [CrossRef]
- Ballmer, C.; Eichelberger, P.; Leitner, M.; Moser, H.; Luginbuehl, H.; Kuhn, A.; Radlinger, L. Electromyography of Pelvic Floor Muscles with True Differential versus Faux Differential Electrode Configuration. Int. Urogynecol. J. 2020, 31, 2051–2059. [Google Scholar] [CrossRef]
- Leitner, M.; Moser, H.; Eichelberger, P.; Kuhn, A.; Radlinger, L. Evaluation of Pelvic Floor Muscle Activity during Running in Continent and Incontinent Women: An Exploratory Study. Neurourol. Urodyn. 2017, 36, 1570–1576. [Google Scholar] [CrossRef]
- Bussey, M.D.; Aldabe, D.; Ribeiro, D.C.; Madill, S.; Woodley, S.; Hammer, N. Is Pelvic Floor Dysfunction Associated With Development of Transient Low Back Pain During Prolonged Standing? A Protocol. Clin. Med. Insights Womens Health 2019, 12, 1179562X1984960. [Google Scholar] [CrossRef] [PubMed]
- Bird, A.R.; Bendrups, A.P.; Payne, C.B. The Effect of Foot Wedging on Electromyographic Activity in the Erector Spinae and Gluteus Medius Muscles during Walking. Gait Posture 2003, 18, 81–91. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Sobota, G.; Kwaśna, K.; Błaszczak, E.; Taradaj, J.; Juras, G. Impact of Different Body Positions on Bioelectrical Activity of the Pelvic Floor Muscles in Nulliparous Continent Women. Biomed. Res. Int. 2015, 2015, 905897. [Google Scholar] [CrossRef] [PubMed]
- Frawley, H.C.; Galea, M.P.; Phillips, B.A.; Sherburn, M.; Bø, K. Effect of Test Position on Pelvic Floor Muscle Assessment. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2006, 17, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.L.; Souza, R.B.; Rauh, M.J.; Fredericson, M.; Rosenthal, M.D. Differences in Knee and Hip Adduction and Hip Muscle Activation in Runners With and Without Iliotibial Band Syndrome. PM&R 2018, 10, 1032–1039. [Google Scholar] [CrossRef]
- Kelly, L.A.; Sebastien, R.; Craig, M.T.; Justin, G.; Hakim, C. Augmented Low Dye Taping Changes Muscle Activation Patterns and Plantar Pressure during Treadmill Running. J. Orthop. Sports Phys. Ther. 2010, 40, 648–655. [Google Scholar] [CrossRef]
- Foch, E.; Aubol, K.; Milner, C.E. Relationship between Iliotibial Band Syndrome and Hip Neuromechanics in Women Runners. Gait Posture 2020, 77, 64–68. [Google Scholar] [CrossRef]
- Hagio, S.; Fukuda, M.; Kouzaki, M. Identification of Muscle Synergies Associated with Gait Transition in Humans. Front. Hum. Neurosci. 2015, 9, 48. [Google Scholar] [CrossRef]
- Kibushi, B. Muscle Coordination Patterns in Regulation of Medial Gastrocnemius Activation during Walking. Hum. Mov. Sci. 2023, 90, 103116. [Google Scholar] [CrossRef]
- Soljanik, I.; Janssen, U.; May, F.; Fritsch, H.; Stief, C.G.; Weissenbacher, E.R.; Friese, K.; Lienemann, A. Functional Interactions between the Fossa Ischioanalis, Levator Ani and Gluteus Maximus Muscles of the Female Pelvic Floor: A Prospective Study in Nulliparous Women. Arch. Gynecol. Obstet. 2012, 286, 931–938. [Google Scholar] [CrossRef]
- Keshwani, N.; McLean, L. A Differential Suction Electrode for Recording Electromyographic Activity from the Pelvic Floor Muscles: Crosstalk Evaluation. J. Electromyogr. Kinesiol. 2013, 23, 311–318. [Google Scholar] [CrossRef]
- Vesentini, G.; El Dib, R.; Righesso, L.A.R.; Piculo, F.; Marini, G.; Ferraz, G.A.R.; Calderon, I.d.M.P.; Barbosa, A.M.P.; Rudge, M.V.C. Pelvic Floor and Abdominal Muscle Cocontraction in Women with and without Pelvic Floor Dysfunction: A Systematic Review and Meta-Analysis. Clinics 2019, 74, e1319. [Google Scholar] [CrossRef]
- Lee, S.K.; Lee, S.Y.; Jung, J.M. Muscle Activity of the Gluteus Medius at Different Gait Speeds. J. Phys. Ther. Sci. 2014, 26, 1915–1917. [Google Scholar] [CrossRef]
- Yani, M.S.; Wondolowski, J.H.; Eckel, S.P.; Kulig, K.; Fisher, B.E.; Gordon, J.E.; Kutch, J.J. Distributed Representation of Pelvic Floor Muscles in Human Motor Cortex. Sci. Rep. 2018, 8, 1–16. [Google Scholar] [CrossRef]
- Asavasopon, S.; Rana, M.; Kirages, D.J.; Yani, M.S.; Fisher, B.E.; Hwang, D.H.; Lohman, E.B.; Berk, L.S.; Kutch, J.J. Cortical Activation Associated with Muscle Synergies of the Human Male Pelvic Floor. J. Neurosci. 2014, 34, 13811–13818. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Nygaard, I.E. Is Physical Activity Good or Bad for the Female Pelvic Floor? A Narrative Review. Sports Med. 2020, 50, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Ashton-Miller, J.A.; DeLancey, J.O.L. Functional Anatomy of the Female Pelvic Floor, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2015; ISBN 9780702044434. [Google Scholar]
- Moretti, E.; de Moura Filho, A.G.; de Almeida, J.C.; Araujo, C.M.; Lemos, A. Electromyographic Assessment of Women’s Pelvic Floor: What Is the Best Place for a Superficial Sensor? Neurourol. Urodyn. 2017, 36, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Saeuberli, P.W.; Schraknepper, A.; Eichelberger, P.; Luginbuehl, H.; Radlinger, L. Reflex Activity of Pelvic Floor Muscles during Drop Landings and Mini-Trampolining-Exploratory Study. Int. Urogynecol. J. 2018, 29, 1833–1840. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muscle | MVC | 5 km/h | 7 km/h | 9 km/h | 11 km/h | p-Value * | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) a | 95% CI | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | ||
| RGM | 224.88 (118.92) | 139.8–309.95 | 159.02 (70.83) | 108.3–209.7 | 101.35 (95.38) | 282.2 (90.48) | 212.6–351.7 | 175.43 (150.63) | 1069.06 (1036.32) | 327.7–1810.4 | 796.85 (1289.96) | 1199.94 (960.80) | 512.6–1887.2 | 848.23 (1182.10) | <0.001 |
| LGM | 221.30 (126.49) | 130.8–311.8 | 146.94 (52.75) | 109.2–184.6 | 79.59 (48.77) | 262.21 (102.81) | 183.1–341.2 | 172.17 (110.77) | 857.90 (763.90) | 311.4–1404.3 | 538.43 (666.13) | 1347.4 (1492.6) | 279.6–2415.2 | 986.82 (1350.93) | <0.001 |
| RPF | 101.26 (35.40) | 75.9–126.5 | 48.34 (29.59) | 27.17–69.5 | 52.92 (39.96) | 66.68 (53.93) | 25.2–108.1 | 76.03 (71.79) | 106.602 (71.42) | 55.5–157.6 | 116.83 (85.70) | 106.716 (43.12) | 75.86–137.5 | 119.64 (66.60) | <0.001 |
| LPF | 92.17 (40.86) | 62.9–121.4 | 56.88 (30.55) | 35.0–78.7 | 70.04 (42.87) | 68.14 (43.84) | 34.4–101.8 | 76.02 (59.31) | 110.29 (87.33) | 47.8–172.7 | 115.09 (54.04) | 95.96 (52.58) | 58.3–133.5 | 112.71 (48.25) | 0.137 |
| Muscle | MVC | 5 km/h | 7 km/h | 9 km/h | 11 km/h | p-Value * | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) a | 95% CI | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | Mean (SD) a | 95% CI | %MVC | ||
| RGM | 149.43 (73.20) | 97.1–201.8 | 50.16 (27.8) | 30.2–70.0 | 52.12 (67.15) | 96.48 (49.39) | 58.5–134.4 | 89.98 (83.08) | 315.081 (236.06) | 146.2–483.9 | 345.3 (538.22) | 349.21 (278.77) | 149.7–548.6 | 392.48 (602.20) | <0.001 |
| LGM | 162.10 (83.91) | 102.0–222.13 | 43.55 (30.9) | 21.4–65.7 | 39.23 (53.32) | 114.41 (107.94) | 31.44–197.3 | 114.58 (163.79) | 254.76 (197.71) | 113.3–396.2 | 234.75 (322.90) | 359.06 (359.76) | 101.7–616.4 | 352.83 (515.71) | <0.001 |
| RPF | 68.92 (26.005) | 50.3–87.5 | 22.06 (11.0) | 14.2–29.9 | 36.99 (26.01) | 26.63 (19.72) | 11.4–41.7 | 46.21 (43.51) | 31.33 (13.29) | 21.8–40.8 | 52.19 (32.48) | 36.69 (18.34) | 23.2–49.8 | 61.44 (40.14) | <0.001 |
| LPF | 63.91 (29.30) | 42.9–84.88 | 20.66 (8.50) | 14.5–26.7 | 38.23 (22.35) | 71.85 (35.09) | 31.9–75.6 | 84.12 (13.72) | 33.06 (15.20) | 22.1–43.9 | 56.52 (22.34) | 36.85 (18.97) | 23.2–50.4 | 63.25 (26.43) | 0.137 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porrón-Irigaray, A.; Rodríguez-López, E.S.; Acevedo-Gómez, M.B.; Ojedo-Martín, C.; Benito-de-Pedro, M. Coactivation of the Pelvic Floor and Gluteus Medius Muscles While Walking and Running in Female Runners. Sensors 2024, 24, 1356. https://doi.org/10.3390/s24051356
Porrón-Irigaray A, Rodríguez-López ES, Acevedo-Gómez MB, Ojedo-Martín C, Benito-de-Pedro M. Coactivation of the Pelvic Floor and Gluteus Medius Muscles While Walking and Running in Female Runners. Sensors. 2024; 24(5):1356. https://doi.org/10.3390/s24051356
Chicago/Turabian StylePorrón-Irigaray, Avelaine, Elena Sonsoles Rodríguez-López, María Barbaño Acevedo-Gómez, Cristina Ojedo-Martín, and María Benito-de-Pedro. 2024. "Coactivation of the Pelvic Floor and Gluteus Medius Muscles While Walking and Running in Female Runners" Sensors 24, no. 5: 1356. https://doi.org/10.3390/s24051356