
Relationship between Car-Sickness Susceptibility and Postural Activity: Could the Re-Weighting Strategy between Signals from Different Body Sensors Be an Underlying Factor?

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
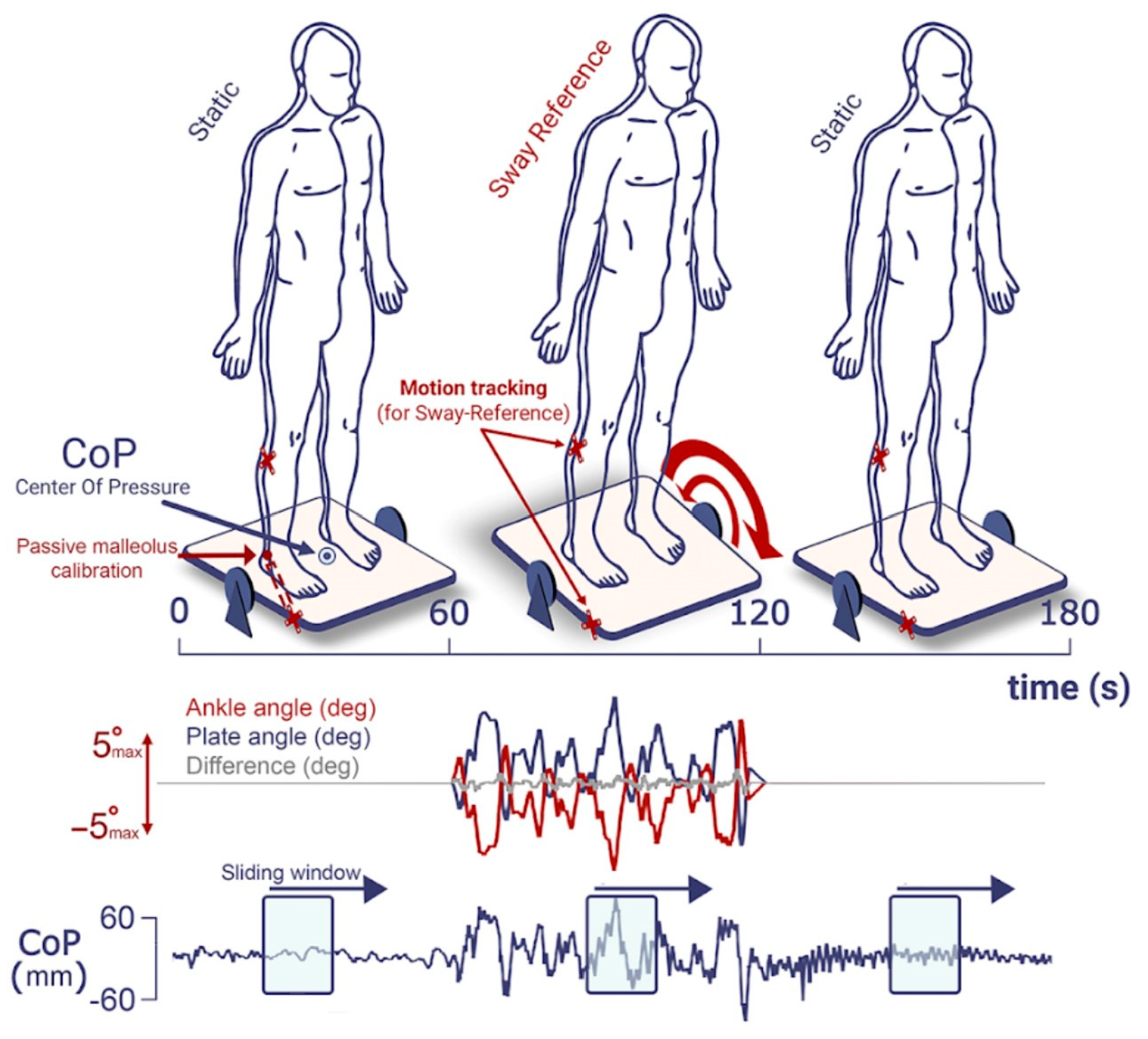
2.2. Experimental Setup
2.3. Procedure
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
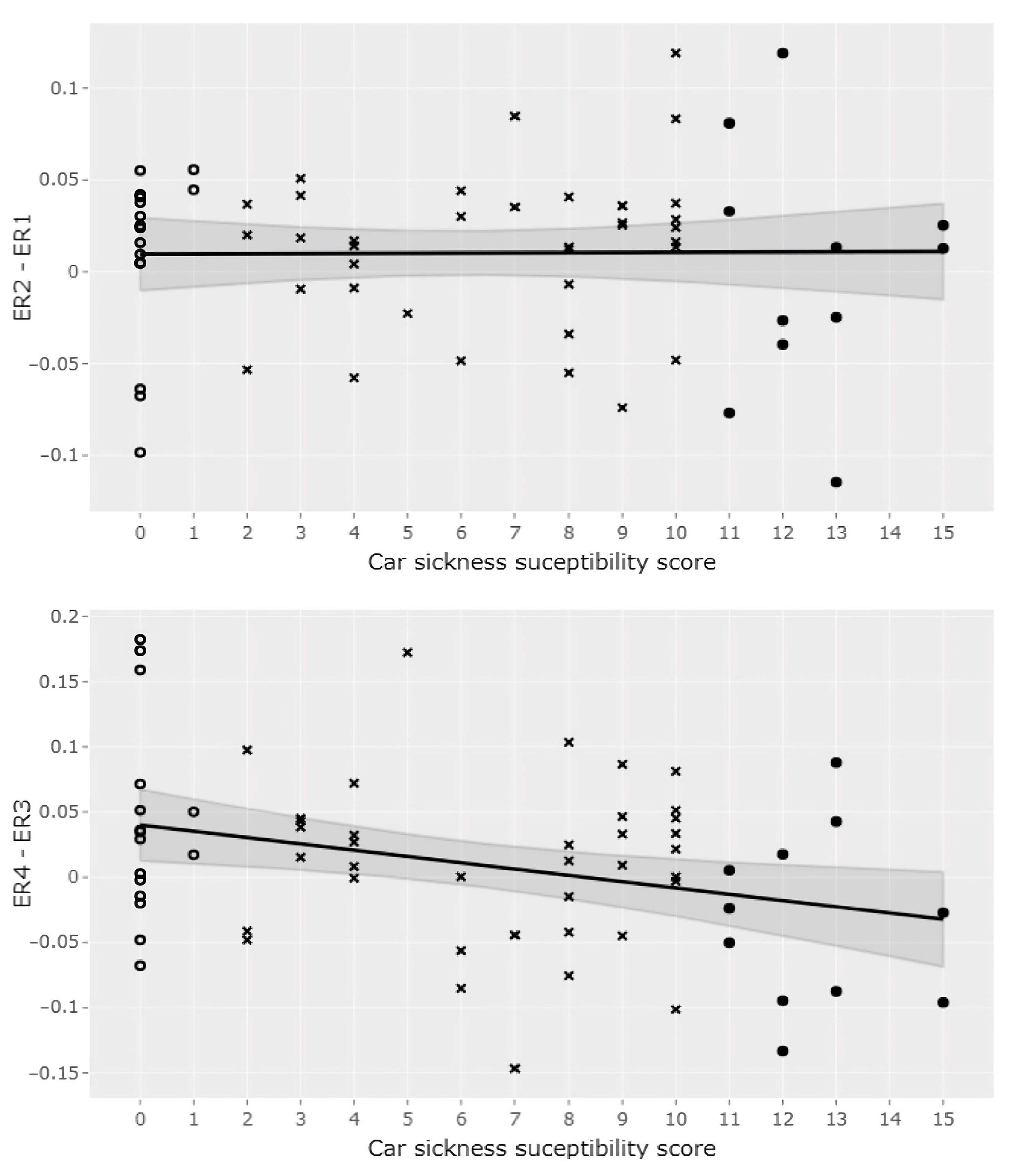
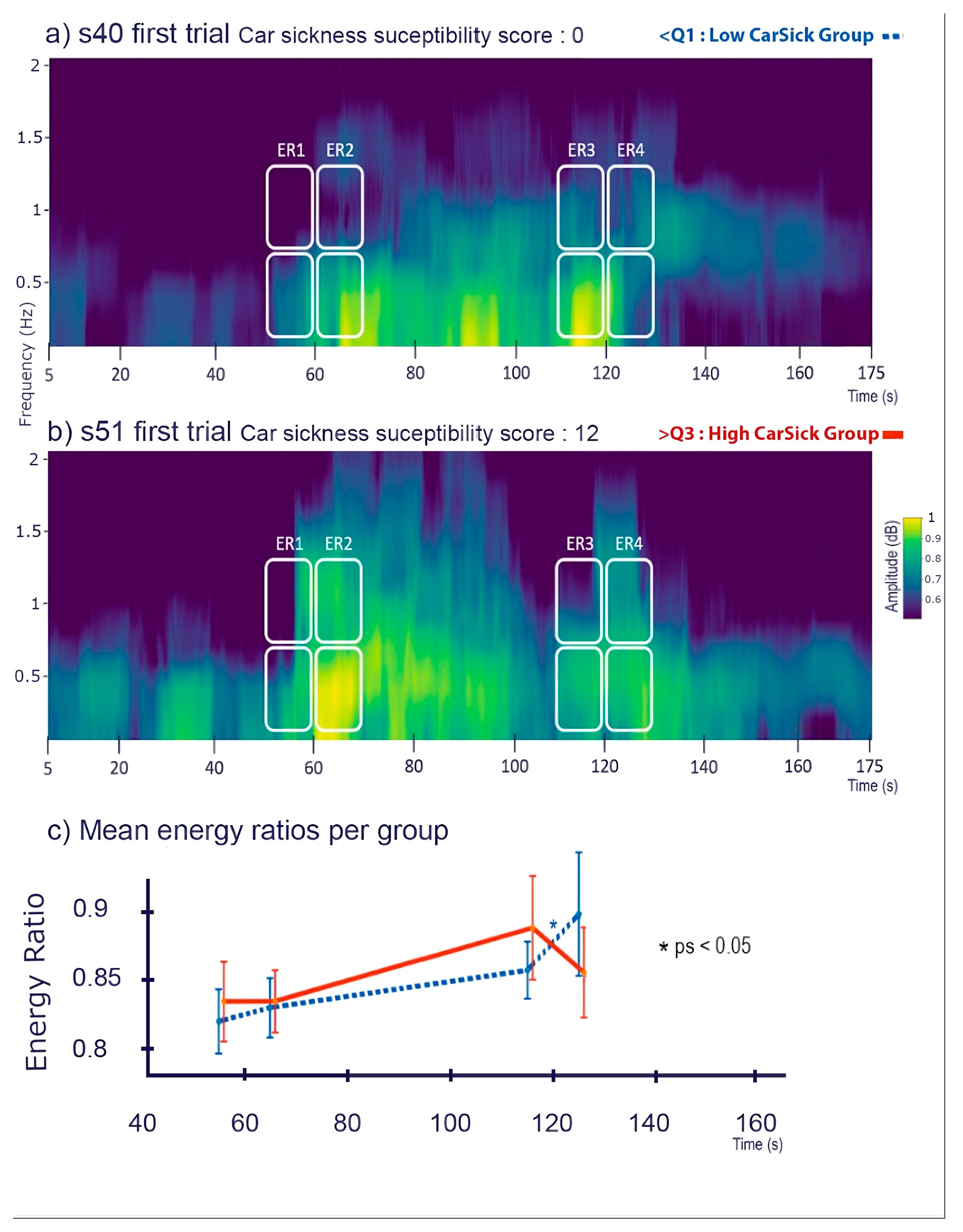
3.1. Relation between Car-Sickness Susceptibility and Energy Ratios in Phases of Transition
3.2. Postural Differences between Subjects with High and Low Sensitivity
3.3. Postural Differences between Women and Men: A Complementary Analysis
4. Discussion
4.1. Sensory Re-Weighting as a Potential Predictor of Car-Sickness Susceptibility
4.2. Sex Differences in Susceptibility to Car-Sickness
4.3. Relevance of the Car-Sickness Questionnaire
4.4. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laboissière, R.; Letievant, J.C.; Ionescu, E.; Barraud, P.A.; Mazzuca, M.; Cian, C. Relationship between Spectral Characteristics of Spontaneous Postural Sway and Motion Sickness Susceptibility. PLoS ONE 2015, 10, e0144466. [Google Scholar] [CrossRef]
- Weech, S.; Varghese, J.P.; Barnett-Cowan, M. Estimating the sensorimotor components of cybersickness. J. Neurophysiol. 2018, 120, 2201–2217. [Google Scholar] [CrossRef]
- Stoffregen, T.A.; Chen, F.C.; Varlet, M.; Alcantara, C.; Bardy, B.G. Getting Your Sea Legs. PLoS ONE 2013, 8, e66949. [Google Scholar] [CrossRef] [PubMed]
- Dida, M.; Cian, C.; Barraud, P.A.; Guerraz, M.; Laboissière, R. Idiosyncratic multisensory reweighting as the common cause for motion sickness susceptibility and adaptation to postural perturbation. PLoS ONE 2021, 16, e0260863. [Google Scholar] [CrossRef] [PubMed]
- Tal, D.; Bar, R.; Nachum, Z.; Gil, A.; Shupak, A. Postural dynamics and habituation to seasickness. Neurosci. Lett. 2010, 479, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Nachum, Z.; Shupak, A.; Letichevsky, V.; Ben-David, J.; Tal, D.; Tamir, A.; Talmon, Y.; Gordon, C.R.; Luntz, M. Mal de débarquement and posture: Reduced reliance on vestibular and visual cues. Laryngoscope 2004, 114, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Nashner, L.; Berthoz, A. Visual contribution to rapid motor responses during postural control. Brain Res. 1978, 150, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Assländer, L.; Peterka, R.J. Sensory reweighting dynamics in human postural control. J. Neurophysiol. 2014, 111, 1852–1864. [Google Scholar] [CrossRef] [PubMed]
- Carver, S.; Kiemel, T.; Jeka, J.J. Modeling the dynamics of sensory reweighting. Biol. Cybern. 2006, 95, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Day, B.L.; Guerraz, M.; Cole, J. Sensory interactions for human balance control revealed by galvanic vestibular stimulation. In Sensorimotor Control of Movement and Posture; Springer: Berlin/Heidelberg, Germany, 2002; pp. 129–137. [Google Scholar] [CrossRef]
- Day, B.L.; Guerraz, M. Feedforward versus feedback modulation of human vestibular-evoked balance responses by visual self-motion information. J. Physiol. 2007, 582, 153–161. [Google Scholar] [CrossRef]
- Jeka, J.J.; Oie, K.S.; Kiemel, T. Asymmetric adaptation with functional advantage in human sensorimotor control. Exp. Brain Res. 2008, 191, 453–463. [Google Scholar] [CrossRef]
- Mahboobin, A.; Loughlin, P.; Atkeson, C.; Redfern, M. A mechanism for sensory re-weighting in postural control. Med. Biol. Eng. Comput. 2009, 47, 921–929. [Google Scholar] [CrossRef]
- Maurer, C.; Mergner, T.; Peterka, R.J. Multisensory control of human upright stance. Exp. Brain Res. 2005, 171, 231. [Google Scholar] [CrossRef] [PubMed]
- Oie, K.S.; Kiemel, T.; Jeka, J.J. Multisensory fusion: Simultaneous re-weighting of vision and touch for the control of human posture. Cogn. Brain Res. 2002, 14, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Peterka, R.J.; Loughlin, P.J. Dynamic regulation of sensorimotor integration in human postural control. J. Neurophysiol. 2004, 91, 410–423. [Google Scholar] [CrossRef] [PubMed]
- Polastri, P.F.; Barela, J.A.; Kiemel, T.; Jeka, J.J. Dynamics of inter-modality re-weighting during human postural control. Exp. Brain Res. 2012, 223, 99–108. [Google Scholar] [CrossRef] [PubMed]
- van der Kooij, H.; Jacobs, R.; Koopman, B.; van der Helm, F. An adaptive model of sensory integration in a dynamic environment applied to human stance control. Biol. Cybern. 2001, 84, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Mahboobin, A.; Loughlin, P.J.; Redfern, M.S.; Sparto, P.J. Sensory re-weighting in human postural control during moving-scene perturbations. Exp. Brain Res. 2005, 167, 260–267. [Google Scholar] [CrossRef]
- Weech, S.; Calderon, C.M.; Barnett-Cowan, M. Sensory down-weighting in visual-postural coupling is linked with lower cybersickness. Front. Virtual Real. 2020, 1, 10. [Google Scholar] [CrossRef]
- Turner, M.; Griffin, M.J. Motion sickness in public road transport: The effect of driver, route and vehicle. Ergonomics 1999, 42, 1646–1664. [Google Scholar] [CrossRef]
- Bos, J.E.; MacKinnon, S.N.; Patterson, A. Motion sickness symptoms in a ship motion simulator: Effects of inside, outside, and no view. Aviat. Space Environ. Med. 2005, 76, 1111–1118. [Google Scholar]
- Barbour, A.J.; Parker, R.L. Psd: Adaptive, sine multitaper power spectral density estimation for R. Comput. Geosci. 2014, 63, 18. [Google Scholar] [CrossRef]
- Fitzpatrick, R.C.; Gorman, R.B.; Burke, D.; Gandevia, S.C. Postural proprioceptive reflexes in standing human subjects: Bandwidth of response and transmission characteristics. J. Physiol. 1992, 458, 69–83. [Google Scholar] [CrossRef]
- Hyndman, R.J.; Fan, Y. Sample Quantiles in Statistical Packages. Am. Stat. 1996, 50, 361. [Google Scholar] [CrossRef]
- Peterka, R.J. Sensory integration for human balance control. Handb. Clin. Neurol. 2018, 159, 27–42. [Google Scholar] [CrossRef]
- Kitazaki, M.; Kimura, T. Effects of long-term adaptation to sway-yoked visual motion and galvanic vestibular stimulation on visual and vestibular control of posture. Presence 2010, 19, 544–556. [Google Scholar] [CrossRef]
- Riccio, G.E.; Stoffregen, T.A. An ecological theory of Motion Sickness and postural instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Oman, C.M. A Heuristic Mathematical Model for the Dynamics of Sensory Conflict and Motion Sickness Hearing in Classical Musicians. Acta Oto-Laryngol. 1982, 94, 4–44. [Google Scholar] [CrossRef]
- Reason, J.T. Motion sickness adaptation: A neural mismatch model. J. R. Soc. Med. 1978, 71, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Reason, J.T.; Brand, J.J. Motion Sickness; Academic Press: London, UK; New York, NY, USA; San Francisco, CA, USA, 1975. [Google Scholar]
- Owen, N.; Leadbetter, A.G.; Yardley, L. Relationship between postural control and motion sickness in healthy subjects. Brain Res. Bull. 1998, 47, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Golding, J.F. Predicting individual differences in motion sickness susceptibility by questionnaire. Pers. Indiv Differ. 2006, 41, 237–248. [Google Scholar] [CrossRef]
- Park, A.H.; Hu, S. Gender differences in motion sickness history and susceptibility to optokinetic rotation-induced motion sickness. Aviat. Space Environ. Med. 1999, 70, 1077–1080. [Google Scholar]
- Kennedy, R.S.; Lanham, D.S.; Massey, C.J.; Drexler, J.M.; Lilienthal, M.G. Gender differences in simulator sickness incidence: Implications for military virtual reality systems. Safe 1995, 25, 69–76. [Google Scholar]
- Lawther, A.; Griffin, M.J. A survey of the occurrence of motion sickness amongst passengers at sea. Aviat. Space Environ. Med. 1998, 59, 399–406. [Google Scholar]
- Koslucher, F.C.; Haaland, E.; Malsch, A.; Webeler, J.; Stoffregen, T.A. Sex differences in the incidence of motion sickness induced by linear visual oscillation. Aviat. Med. Hum. Perf. 2015, 86, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Matchock, R.L.; Levine, M.E.; Gianaros, P.J.; Stern, R.M. Susceptibility to nausea and motion sickness as a function of the menstrual cycle. Womens Health Issues 2008, 18, 328–335. [Google Scholar] [CrossRef]
- Era, P.; Sainio, P.; Koskinen, S.; Haavisto, P.; Vaara, M.; Aromaa, A. Postural balance in a random sample of 7979 subjects aged 30 years and over. Gerontology 2006, 52, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Chiari, L.; Rocchi, L.; Cappello, A. Stabilometric parameters are affected by anthropometry and foot placement. Clin. Biomech. 2002, 17, 666–677. [Google Scholar] [CrossRef]
- Kim, J.W.; Eom, G.M.; Kim, C.S.; Kim, D.H.; Lee, J.H.; Park, B.K.; Hong, J. Sex differences in the postural sway characteristics of young and elderly subjects during quiet natural standing. Geriat. Geront. Int. 2010, 10, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.V.; Rose, J.; Rohlfing, T.; Pfefferbaum, A. Postural sway reduction in aging men and women: Relation to brain structure, cognitive status, and stabilizing factors. Neurobiol. Aging 2009, 30, 793–807. [Google Scholar] [CrossRef] [PubMed]
- Koslucher, F.; Haaland, E.; Stoffregen, T.A. Sex differences in visual performance and postural sway precede sex differences in visually induced motion sickness. Exp. Brain Res. 2016, 234, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Catanzariti, J.F.; Guyot, M.A.; Massot, C.; Khenioui, H.; Agnani, O.; Donzé, C. Evaluation of motion sickness susceptibility by motion sickness susceptibility questionnaire in adolescents with idiopathic scoliosis: A case-control study. Eur. Spine J. 2016, 25, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Mittelstaedt, J.M. Individual predictors of the susceptibility for motion-related sickness: A systematic review. J. Vest. Res. 2020, 30, 165–193. [Google Scholar] [CrossRef] [PubMed]
- Graybiel, A. Susceptibility to acute motion sickness in blind persons. Aerosp. Med. 1970, 41, 650–653. [Google Scholar]
- Mayo, A.M.; Wade, M.G.; Stoffregen, T.A. Postural effects of the horizon on land and at sea. Psychol. Sci. 2011, 22, 118–124. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dida, M.; Guerraz, M.; Barraud, P.-A.; Cian, C. Relationship between Car-Sickness Susceptibility and Postural Activity: Could the Re-Weighting Strategy between Signals from Different Body Sensors Be an Underlying Factor? Sensors 2024, 24, 1046. https://doi.org/10.3390/s24041046
Dida M, Guerraz M, Barraud P-A, Cian C. Relationship between Car-Sickness Susceptibility and Postural Activity: Could the Re-Weighting Strategy between Signals from Different Body Sensors Be an Underlying Factor? Sensors. 2024; 24(4):1046. https://doi.org/10.3390/s24041046
Chicago/Turabian StyleDida, Merrick, Michel Guerraz, Pierre-Alain Barraud, and Corinne Cian. 2024. "Relationship between Car-Sickness Susceptibility and Postural Activity: Could the Re-Weighting Strategy between Signals from Different Body Sensors Be an Underlying Factor?" Sensors 24, no. 4: 1046. https://doi.org/10.3390/s24041046