

Assessment of the Performance of Ultrasonography for Detecting Myofascial Trigger Points

1
Department of Physical Therapy, Hungkuang University, Taichung 433304, Taiwan
2
Taiwan Myopain Academic Association, Tainan 704032, Taiwan
3
Department of Physical Therapy, China Medical University, Taichung 406040, Taiwan
*
Author to whom correspondence should be addressed.
Sensors 2024, 24(3), 718; https://doi.org/10.3390/s24030718
Submission received: 14 December 2023
/
Revised: 18 January 2024
/
Accepted: 19 January 2024
/
Published: 23 January 2024
(This article belongs to the Special Issue Ultrasonic Imaging and Sensors II)
Abstract
:Needle electromyogram (EMG) research has suggested that endplate noise (EPN) is a characteristic of myofascial trigger points (MTrPs). Although several studies have observed MTrPs through ultrasonography, whether they are hyperechoic or hypoechoic in ultrasound images is still controversial. Therefore, this study determined the echogenicity of MTrP ultrasonography. In stage 1, the MTrP of rat masseter muscle was identified through palpation and marked. Needle EMG was performed to detect the presence of EPN. When EPN was detected, ultrasound scans and indwelling needles were used to identify the nodule with a different grayscale relative to that of its surrounding tissue, and the echogenicity of the identified MTrP was determined. In stage 2, these steps were reversed. An ultrasound scan was performed to detect the nodule at the marked site, and an EMG needle was inserted into the nodule to detect EPN. There were 178 recordings in each stage, obtained from 45 rats. The stage 1 results indicate that the MTrPs in ultrasound images were hypoechoic with a 100% sensitivity of assessment. In stage 2, the accuracy and precision of MTrP detection through ultrasonography were 89.9% and 89.2%, respectively. The results indicate that ultrasonography produces highly accurate and precise MTrP detection results.
1. Introduction
Myofascial pain is a common cause of temporomandibular disorders (TMDs) [1]. Therefore, myofascial pain of chewing-related muscles should be treated before myogenic TMDs are managed. Myofascial pain is a common musculoskeletal condition characterized by the formation of myofascial trigger points (MTrPs), which are hyperirritable nodules that form in the taut bands of muscles [2,3]. Clinicians usually diagnose myofascial pain syndrome by identifying one or more MTrPs [4]. Previously, they often palpated a taut band and used the resulting referred pain as the basis for determining the location of an MTrP. This physical examination for locating MTrPs has been widely used [4,5]. However, numerous scholars have suggested that this method is unreliable [6].
In electrophysiological studies, spontaneous electrical activities, including endplate noise (EPN) and endplate spikes, were detected after a needle was inserted into an MTrP [7]. Additionally, the incidence of EPN is significantly higher at MTrPs than at non-MTrP sites [8], and EPN is positively correlated with MTrP irritability [9]. Consequently, scholars have asserted that EPN is a characteristic manifestation of MTrP that is helpful for diagnosing TMDs [8]; notably, it is not an absolute diagnostic standard. Although needle electromyography (EMG) can be used to identify MTrPs in a research setting, it is an impractical option in a general clinical setting [10].
Ultrasonography is also used to diagnose MTrP because it is straightforward, cost efficient, and radiation free. Elastography is a method for quantifying the viscoelasticity of soft tissue, which is achieved by observing the tissue’s response to external stress or vibration. Because an MTrP is stiffer than its surrounding tissue, its location can be determined on the basis of this characteristic [11,12,13]. Although studies have extensively demonstrated the application of ultrasonography for detecting MTrPs, this method requires additional induction and is still impractical for general clinical settings. By contrast, a more suitable clinical practice is to directly observe MTrP as two-dimensional (2D) images and to determine their location by differentiating the echo characteristics of MTrPs and their surrounding tissue; notably, the basis for image interpretation in this context remains controversial. Several studies have suggested that the ultrasound images of MTrPs exhibit hypoechogenicity [13,14]; however, others have reported that such images exhibit hyperechogenicity [15,16]. Hypoechogenicity occurs when an ultrasound produces less echogenicity upon encountering a tissue or substance and presents a darker image of the tissue or substance site relative to its surrounding tissues. For example, liquids such as urine are hypoechoic, whereas hard tissues such as bones are hyperechoic [17]. Therefore, this study examined the occurrence of EPN to determine the ultrasonography imaging characteristics of MTrPs and assess the performance of ultrasonography for detecting MTrPs.
2. Materials and Methods
2.1. Animal Care and Preparation
Experiments were performed on adult male Sprague–Dawley (SD) rats (250 to 300 g), purchased from BioLASCO, Taiwan. The animals were kept on an artificial 12 h light–dark cycle at a university animal center. Food and water were available ad libitum. Each animal was housed and cared for in accordance with the ethical guidelines of the International Association for the Study of Pain [18,19]. Effort was made to minimize the discomfort of the animals and to reduce the number of animals used. All animal experiments were conducted with the procedure approved by the Animal Care and Use Committee of the university, in accordance with the Guidelines for Animal Experimentation (No. 2018-059).
2.2. Identification of MTrPs
A specific hyperirritable spot (MTrP) in the masseter muscle of rats is similar to that located in the masseter muscle of humans. At this spot, local twitch responses can be elicited when a needle tip encounters a sensitive locus [20]. Similarly to human MTrPs, this sensitive spot of rats frequently exhibits spontaneous electrical activity (e.g., EPN) [8,21]. Before an anesthetic was administered, the most tender spots (i.e., MTrPs) of randomly selected masseter muscles were identified via finger pinching. An animal’s reaction (e.g., withdrawal of the lower limb, head turning, and screaming) was observed to confirm the exact location of an MTrP [22,23,24]. These painful regions were marked on the skin with an indelible marker, and the animals were anesthetized with isoflurane (AErrane, Baxter Healthcare of Puerto Rico, PR, USA) in oxygen flow (2% for induction and 0.5% for maintenance) [25]. Body temperature, which was monitored by inserting the thermistor probe of a thermometer (Physiotemp Instrument, Clifton, NJ, USA) into the rectum, was maintained at approximately 37.5 °C; this was achieved using a body temperature control system with a thermostatically regulated DC current heating pad and an infrared lamp. The masseter of the marked side of the face of a rat was held between the fingers from behind the muscle, and the muscle was palpated by gently rubbing (rolling) it between the fingers to identify a taut band. A taut band feels like a clearly delineated rope of muscle fibers (with a diameter of approximately 2–3 mm) to the touch. Such areas were designated for the evaluation of ultrasound images and electrophysiological recordings.
2.3. Electrophysiological Recording of EPN
For EPN assessment, a two-channel digital EMG machine (Neuro-MEP-Micro; Neurosoft, 5, Voronin Str, Ivanovo, Russia) and monopolar needle electrodes (37 mm disposable Teflon-coated model) were used. The gain was set to 20 μV per division for the recordings from both channels. Low-cut and high-cut frequency filters were set to 100 and 1000 Hz, respectively. Sweep speed was 10 ms per division. The search needle used for the EPN recording was inserted into the MTrP region and connected to the first channel of the EMG machine. The control needle was inserted into the same muscle in the non-taut band region near the MTrP and connected to the second channel. The common reference needle electrode for each channel was secured on the skin through an incision and connected to both channels through a y-connector.
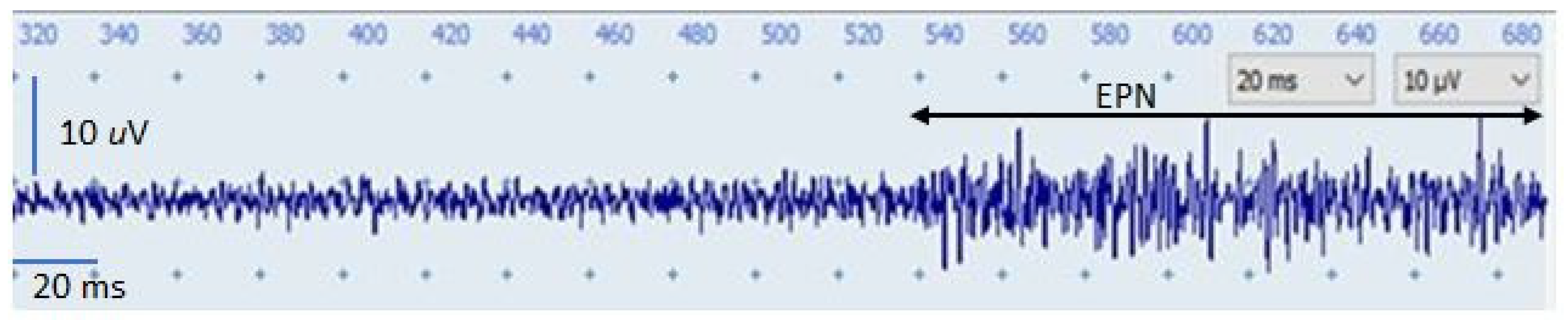
The search needle was inserted into the MTrP region parallel to the muscle fibers at an approximate 60° angle to the surface of the muscle. After its initial insertion to a depth just short of an MTrP or to a comparable depth at a control site, the needle was advanced very slowly, being simultaneously and slowly rotated in order to prevent it from suddenly grabbing and releasing tissue to advance with a large jump. Each advance covered only a minimal distance (approximately 1 mm). When the needle approached an active locus (EPN locus), a continuous distant electrical activity (i.e., EPN) was detected. When EPN with an amplitude of >10 μV was recorded, the examiner stopped advancing the needle and gently moved the needle minimally in a different direction; this change was made to obtain the EPN with the highest amplitude. If the desired result was not achieved, the needle was advanced to another site until an EPN with an optimal amplitude (usually >30 μV) was recorded. Subsequently, the needle was fixed in place (carefully and firmly taped onto the skin) to ensure the continuous run of the EPN on the recording screen at a constant amplitude. Throughout the experiment, continuous EPN tracing was performed so that EPN changes were continuously visualized on an EMG screen (Figure 1). If the EPN was unsustainable, the searching needle was moved to another site until a satisfactory EPN tracing result was obtained. This EPN recording procedure was performed by an investigator who was blinded to the group assignment.
2.4. Ultrasound Imaging
Morphological data on the MTrPs of masticatory muscles were mainly acquired through ultrasonography (Terason t3000 Ultrasound System, Ormond Beach, FL, USA). All ultrasonography evaluations performed in this study were performed by a single assessor who was familiar with ultrasonography operation and interpretation and was blinded to the grouping status of the tested animals. After the location of an MTrP on a rat was determined through palpation, a 7–12 MHz linear array transducer (Terason 12HL7, 25 mm hockey stick style, 128 elements) was placed on the masseter muscle parallel to its upper jaw with minimal pressure applied. Ultrasonography was conducted at a focal length range of 0.3–1.0 cm and an image depth of 1 cm. In our pilot study, the EPN locations detected using the EMG needle were scanned by performing an ultrasound, and the identified muscle nodules were mostly revealed to be hypoechoic (Figure 2). Therefore, the assessor determined that the hypoechoic nodules were MTrPs, captured the relevant images, and recorded them for further analysis.
2.5. Experimental Procedures
On the basis of the research purpose, the present experiment was divided into two stages. Stage 1 was performed to confirm whether the identified MTrPs were hypoechoic or hyperechoic. The assessor inserted the needle into the masseter muscle and moved it slowly depending on the signals that they observed. During EPN detection, an ultrasound scan was performed with an indwelling needle to locate the MTrP. The nodule with a grayscale that differed from that of its surrounding tissue was identified, and its image was captured and recorded for further analysis. In stage 2, the steps performed in stage 1 were reversed in order to assess the performance of ultrasonography for detecting MTrPs. Ultrasound images of MTrPs were captured and recorded on the basis of the characteristics as determined in stage 1. A needle was inserted into the MTrP site as identified under ultrasound guidance in order to record the electrical signal of the site.
2.6. Data Analysis
The parameter data obtained in this study exhibited both “positive” and “negative” when referring to the presence and absence of the phenomenon, respectively. In stage 1, the phenomenon indicated the presence of hypoechoic images on the site of the exhibited EPN. And the phenomenon indicated the presence of EPN on the site of hypoechogenicity in stage 2. All data were compiled in a crosstab, and their sensitivity, specificity, positive predictivity, negative predictivity, positive likelihood ratio, negative likelihood ratio, accuracy, and precision were calculated.
3. Results
A total of 45 rats were included. Bilateral masseter muscles of each rat were measured twice in each stage. However, two recordings were discarded due to poor quality. Therefore, there were 178 recordings for each stage. In stage 1, images indicating hypoechogenicity were obtained for the 148 MTrPs that exhibited EPN. Of the 30 MTrPs that did not exhibit EPN, images indicating nonhypoechogenicity and hypoechogenicity were obtained for twenty-eight and two MTrPs, respectively. In stage 2, among the 166 MTrPs for which hypoechoic images were obtained, 148 exhibited EPN, whereas 18 did not do so. The 12 MTrPs for which hypoechoic images were not obtained did not exhibit any EPN.
4. Discussion
4.1. Hypoechoic Characteristics of MTrPs
The results of stage 1 reveal that the images obtained from the ultrasonography of MTrPs, which was performed after an indwelling needle was inserted upon the detection of EPN, all indicated hypoechogenicity. Therefore, the MTrP sites of the masseter muscles of the rats appeared hypoechoic in ultrasound images. When an ultrasound detects tissue interfaces with varying densities, part of the emitted energy is reflected. The intensity of a grayscale image is determined by the amount of ultrasonic energy that is reflected. When more energy is reflected, an ultrasound image exhibits more hyperechogenicity; that is, bright spots appear whiter in the image. The strength of an ultrasound penetration or reflection is related to the ratio of acoustic impedance between tissue interfaces. A greater difference in acoustic impedance indicates a greater amount of reflected ultrasonic energy [26].
The integrated hypothesis posits that acetylcholine concentration considerably increases at the neuromuscular junction of an MTrP site [27]. The sustained contraction of muscle fibers causes local ischemia, hypoxia [28,29], and vasocontraction [30]. The ultrasound images of muscle injuries characterized by delayed onset muscle soreness revealed hyperechoic hematomas [31]. Therefore, the ischemia of MTrPs may explain the decreasing difference between their acoustic impedance and those of the surrounding tissues, which results in MTrP images exhibiting hypoechogenicity. In addition, the previous sono-histological research revealed that the hypoechogenicity of the MTrP could partially be explained by the fluids entrapped inside the micro-cracks and fissurations of the intercellular scaffold of the muscle [32].
4.2. Performance of Ultrasonography
In addition to revealing that the ultrasound images of MTrPs indicate hypoechogenicity, this study verified the performance of ultrasonography for detecting MTrPs. The verification process primarily occurred in stage 2, during which ultrasonographic MTrP images were captured and then a needle was inserted into an MTrP site (as identified under ultrasonic guidance) in order to detect EPN. In stage 1, ultrasonography was performed to verify the existence of MTrPs; this was achieved using the strong echo image of a needle tip that was generated during the search for MTrPs at a 100% sensitivity level. This same level of sensitivity was also observed in stage 2, indicating that ultrasound images exhibit hypoechogenicity when an MTrP is present in the muscle. This high-sensitivity feature is helpful for clinical interventions (e.g., guided dry needle therapy and injection), which require precise information on the location of an MTrP. Consequently, the ultrasound guidance is significant not only to locate the MTrP but also to accurately reach it with the needle while avoiding iatrogenic injuries to the surrounding tissues. The specificity (i.e., the proportion of correctly identified actual negatives) in stages 1 and 2 was 93.3%, and 40%, respectively. Therefore, when no MTrP is present in an observed muscle, the ultrasound images of the muscle may be misinterpreted, producing false-positive results. Accordingly, an ultrasonography-based MTrP evaluation should be combined with observations of clinical symptoms and palpation, all of which contribute to the location of MTrPs. Regarding the false-positive results, however, the scholars proposed that the hypoechogenicity also related to the presence of muscular fascicles with different spatial orientations. Some authors described an “oscillatory” technique with the ultrasound transducer in order to reduce the acoustic artifacts, and thus reduce the false-positive results [32]. Therefore, the technical aspect is very important for clinical application and a cross-match between clinical symptoms and sonographic findings should always be performed as a daily practice. Additionally, compressing the hypoechoic nodular findings with the ultrasound transducer to assess if the sonographically detected nodule is painful or not (i.e., sono-palpation) may provide better specificity [33].
A positive predictive value reflects the proportion of true positive results obtained in diagnostic tests. In the context of this study, it reflects the positive results obtained through the ultrasonic scan performed in stage 2, which revealed that the proportion of actual MTrPs was 89.2%. In stages 1 and 2, a negative predictive value of 100% indicates that when no MTrP is detected through ultrasonography, an evaluator can confidently determine that no MTrP is present in the ultrasound field of view of the examined muscle. The positive likelihood ratio of only 1.67 was obtained in stage 2, indicating that ultrasonography can be used to obtain hypoechoic images and that the probability of the presence of MTrP is only 1.67 times greater than that of the absence of an MRrP. Therefore, ultrasonography should be combined with an analysis of clinical symptoms and a palpation examination, both of which can help confirm the existence of MTrPs. A negative likelihood ratio of zero was obtained in this study, indicating that the use of ultrasound images to determine the presence of MTrPs produces robust results.
An evaluation of the use of ultrasonography in combination with EPN detection revealed that ultrasonography achieved an accuracy of up to 89.9% for detecting MTrPs. In addition, the precision (i.e., a reliability-related measure of the closeness of two or more measurements to each other) of MTrP detection through ultrasonography reached 89.2%. The results of this study indicate that ultrasonography is a highly accurate and precise method for detecting MTrPs.
4.3. Clinical Application
Numerous studies have proposed various treatments for MTrP, including laser therapy [22,34], dry needle therapy [35,36], extracorporeal shock wave therapy [37], and manual therapy [38]. The primary method for measuring the outcome of MTrP treatments is the pain index; however, pain index data are regarded as subjective data. If ultrasound images can be effectively used to detect MTrPs and can be combined with image analysis technology to obtain morphological data (e.g., MTrP area and thickness), this method can be applied to evaluate the outcomes of MTrP treatments. It is important for a clinician to put forward objective evidence that is of clinical efficacy, not only for professional recognition, but also for patient protection, which will help improve the quality of the treatment.
4.4. Limitations and Directions for Future Research
Ultrasonography is widely used in the clinical diagnosis of musculoskeletal diseases, including muscle strains, ligaments or tendon sprains, and muscle tumors. If it is validated, the use of 2D ultrasound images for MTrP detection provides a cost- and time-efficient method for the clinical diagnosis of MTrPs. In this study, rats were examined to detect the MTrPs of their chewing muscles, and the results obtained from rats cannot be directly extrapolated to humans because the active or latent status of MTrPs could not be determined in this study. That is, the effect of the active or latent status of MTrPs on the performance of ultrasonography for MTrP detection remains unclear. Therefore, to achieve a comprehensive understanding of the performance of ultrasonography for MTrP detection, studies should enroll human participants and apply the procedures used in this study.
In the present study, only the 2D ultrasound image was used for MTrP detection. Therefore, the other function of ultrasound, such as color/power Doppler or elastography, to identify MTrP are worthy of further investigation.
5. Conclusions
In this study, the EPN spontaneously generated by MTrPs was used to verify the characteristics of MTrP ultrasound images, which were revealed to be hypoechoic. The performance of ultrasonography for MTrP detection was satisfactory; specifically, a sensitivity level of 100% and accuracy and precision levels of >89% were achieved. We also demonstrated that ultrasonography is an excellent tool for diagnosing MTrPs; however, in this study, a specificity of only 40% was achieved, indicating that ultrasonography tends to produce false-positive results when an observed muscle has no MTrP. The use of ultrasonography to distinguish MTrPs from surrounding tissue should be further developed to facilitate the determination of MTrP morphology and provide a clinical framework for assessing the effects of MTrP treatments.
Author Contributions
Conceptualization, H.-Y.C. and Y.-L.H.; methodology, H.-Y.C., C.-Z.H. and Y.-L.H.; validation, H.-Y.C., C.-Z.H. and Y.-L.H.; formal analysis, H.-Y.C.; investigation, H.-Y.C.; resources, Y.-L.H.; writing—original draft preparation, H.-Y.C.; writing—review and editing, H.-Y.C. and Y.-L.H. visualization, H.-Y.C. and Y.-L.H.; supervision, Y.-L.H. and C.-Z.H.; project administration, H.-Y.C. and Y.-L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All animal experiments were conducted with the procedure approved by the Animal Care and Use Committee of the university in accordance with the Guidelines for Animal Experimentation (No. 2018-059).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.
Acknowledgments
We thank Andy Chien for assistance with experimental equipment.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Manfredini, D.; Guarda-Nardini, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research diagnostic criteria for temporomandibular disorders: A systematic review of axis I epidemiologic findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.Z.; Simons, D.G. Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch. Phys. Med. Rehabil. 1998, 79, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.G.; Travell, J.; Simons, L.S. Travell & Simons Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 1. Upper Half of Body, 2nd ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Shah, J.P.; Thaker, N.; Heimur, J.; Aredo, J.V.; Sikdar, S.; Gerber, L. Myofascial trigger points then and now: A historical and scientific perspective. PM R 2015, 7, 746–761. [Google Scholar] [CrossRef] [PubMed]
- Tough, E.A.; White, A.R.; Richards, S.; Campbell, J. Variability of criteria used to diagnose myofascial trigger point pain syndrome evidence from a review of the literature. Clin. J. Pain 2007, 23, 278–286. [Google Scholar] [CrossRef]
- Lucas, N.; Macaskill, P.; Irwig, L.; Moran, R.; Bogduk, N. Reliability of physical examination for diagnosis of myofascial trigger points: A systematic review of the literature. Clin. J. Pain 2009, 25, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.G. Do endplate noise and spikes arise from normal motor endplates? Am. J. Phys. Med. Rehabil. 2001, 80, 134–140. [Google Scholar] [CrossRef]
- Simons, D.G.; Hong, C.Z.; Simons, L.S. Endplate potentials are common to midfiber myofascial trigger points. Am. J. Phys. Med. Rehabil. 2002, 81, 212–222. [Google Scholar] [CrossRef]
- Kuan, T.S.; Hsieh, Y.L.; Chen, S.M.; Chen, J.T.; Yen, W.C.; Hong, C.Z. The myofascial trigger point region: Correlation between the degree of irritability and the prevalence of endplate noise. Am. J. Phys. Med. Rehabil. 2007, 86, 183–189. [Google Scholar] [CrossRef]
- Dommerholt, J.; Shah, J.P.; Ballantyne, J.C.; Rathmell, J.P.; Fishman, S.M. Myofascial Pain Syndrome, 4th ed.; Williams & Wilkins: Baltimore, MD, USA, 2010. [Google Scholar]
- Sikdar, S.; Shah, J.P.; Gebreab, T.; Yen, R.H.; Gilliams, E.; Danoff, J.; Gerber, L.H. Novel applications of ultrasound technology to visualize and characterize myofascial trigger points and surrounding soft tissue. Arch. Phys. Med. Rehabil. 2009, 90, 1829–1838. [Google Scholar] [CrossRef]
- Ballyns, J.J.; Turo, D.; Otto, P.; Shah, J.P.; Hammond, J.; Gebreab, T.; Gerber, L.H.; Sikdar, S. Office-based elastographic technique for quantifying mechanical properties of skeletal muscle. J. Ultrasound Med. 2012, 31, 1209–1219. [Google Scholar] [CrossRef]
- Turo, D.; Otto, P.; Shah, J.P.; Heimur, J.; Gebreab, T.; Zaazhoa, M.; Armstrong, K.; Gerber, L.H.; Sikdar, S. Ultrasonic characterization of the upper trapezius muscle in patients with chronic neck pain. Ultrason. Imaging 2013, 35, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Adigozali, H.; Shadmehr, A.; Ebrahimi, E.; Rezasoltani, A.; Naderi, F. Reliability of assessment of upper trapezius morphology, its mechanical properties and blood flow in female patients with myofascial pain syndrome using ultrasonography. J. Bodyw. Mov. Ther. 2017, 21, 35–40. [Google Scholar] [CrossRef]
- Lewis, J.; Tehan, P. A blinded pilot study investigating the use of diagnostic ultrasound for detecting active myofascial trigger points. Pain 1999, 79, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Shankar, H.; Reddy, S. Two- and three-dimensional ultrasound imaging to facilitate detection and targeting of taut bands in myofascial pain syndrome. Pain Med. 2012, 13, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L. Ultrasound Imaging for Rehabilitation of the Lumbopelvic Region. A Clinical Approach; Elsevier Ltd.: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Zimmermann, M. Ethical guidelines for investigations of experimental pain in conscious animals. Pain 1983, 16, 109–110. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M. Ethical considerations in relation to pain in animal experimentation. Acta Physiol. Scand. Suppl. 1986, 554, 221–233. [Google Scholar] [PubMed]
- Hong, C.Z.; Torigoe, Y. Electrophysiologic characteristics of localized twitch responses in responsive bands of rabbit skeletal muscle fibers. J. Musculoskelet. Pain 1994, 2, 17–43. [Google Scholar] [CrossRef]
- Simons, D.G.; Hong, C.Z.; Simons, L.S. Prevalence of spontaneous electrical activity at trigger spots and at control sites in rabbit skeletal muscle. J. Musculoskelet. Pain 1995, 3, 35–48. [Google Scholar] [CrossRef]
- Chen, K.H.; Hong, C.Z.; Kuo, F.C.; Hsu, H.C.; Hsieh, Y.L. Electrophysiologic effects of a therapeutic laser on myofascial trigger spots of rabbit skeletal muscles. Am. J. Phys. Med. Rehabil. 2008, 87, 1006–1014. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Chou, L.W.; Joe, Y.S.; Hong, C.Z. Spinal cord mechanism involving the remote effects of dry needling on the irritability of myofascial trigger spots in rabbit skeletal muscle. Arch. Phys. Med. Rehabil. 2011, 92, 1098–1105. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Yang, C.C.; Liu, S.Y.; Chou, L.W.; Hong, C.Z. Remote dose-dependent effects of dry needling at distant myofascial trigger spots of rabbit skeletal muscles on reduction of substance P levels of proximal muscle and spinal cords. BioMed Res. Int. 2014, 982121. [Google Scholar] [CrossRef] [PubMed]
- Wood, P.L. Animal models in analgesic testing. In Analgesics: Neurochemical, Behavioral and Clinical Perspectives (Central Nervous System Pharmacology; Kuhar, M.J., Pasternak, G.W., Eds.; Raven Press: New York, NY, USA, 1984; pp. 175–194. [Google Scholar]
- Jacobson, J.A. Fundamentals of Musculoskeletal Ultrasound; Sunders, Elsevier Inc.: Philadelphia, PA, USA, 2007. [Google Scholar]
- Simons, D.G. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J. Electromyogr. Kinesiol. 2004, 14, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.Z. Research on myofascial pain syndrome. Crit. Rev. Phys. Rehabil. Med. 2008, 20, 343–366. [Google Scholar] [CrossRef]
- Mense, S.; Gerwin, R.D. Muscle Pain: Understanding the Mechanisms; Springer: Berlin/Heidelberg, Germany, 2010; pp. 20–60. [Google Scholar]
- Kimura, Y.; Ge, H.Y.; Zhang, Y.; Kimura, M.; Sumikura, H.; Arendt-Nielsen, L. Evaluation of sympathetic vasoconstrictor response following nociceptive stimulation of latent myofascial trigger points in humans. Acta Physiol. 2009, 196, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.; Jacobson, J.A.; Fessell, D.P.; Mautner, K. Ultrasound findings of delayed-onset muscle soreness. J. Ultrasound Med. 2016, 35, 2517–2521. [Google Scholar] [CrossRef]
- Ricci, V.; Ricci, C.; Gervasoni, F.; Cocco, G.; Andreoli, A.; Özçakar, L. From Histoanatomy to Sonography in Myofascial Pain Syndrome: A EURO-MUSCULUS/USPRM Approach. Am. J. Phys. Med. Rehabil. 2023, 102, 92–97. [Google Scholar] [CrossRef]
- Pirri, C.; Pirri, N.; Stecco, C.; Macchi, V.; Porzionato, A.; De Caro, R.; Özçakar, L. Sono-palpation and sono-Tinel in musculoskeletal ultrasound examination: Use all “sono-senses”. A systematic review. Med. Ultrason. 2023, 25, 325–329. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Hong, C.Z.; Chou, L.W.; Yang, S.A.; Yang, C.C. Fluence-dependent effects of low-level laser therapy in myofascial trigger spots on modulation of biochemicals associated with pain in a rabbit model. Lasers Med. Sci. 2015, 30, 209–216. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Kao, M.J.; Kuan, T.S.; Chen, S.M.; Chen, J.T.; Hong, C.Z. Dry needling to a key myofascial trigger point may reduce the irritability of satellite MTrPs. Am. J. Phys. Med. Rehabil. 2007, 86, 397–403. [Google Scholar] [CrossRef]
- Vulfsons, S.; Ratmansky, M.; Kalichman, L. Trigger point needling: Techniques and outcome. Curr. Pain Headache Rep. 2012, 16, 407–412. [Google Scholar] [CrossRef]
- Ji, H.M.; Kim, H.J.; Han, S.J. Extracorporeal shock wave therapy in myofascial pain syndrome of upper trapezius. Ann. Rehabil. Med. 2012, 36, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Sarrafzadeh, J.; Ahmadi, A.; Yassin, M. The effects of pressure release, phonophoresis of hydrocortisone, and ultrasound on upper trapezius latent myofascial trigger point. Arch. Phys. Med. Rehabil. 2012, 93, 72–77. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Continuous EPN tracing and visualization of its changes on an EMG screen (EPN: endplate noise; EMG: electromyography).
Figure 1.
Continuous EPN tracing and visualization of its changes on an EMG screen (EPN: endplate noise; EMG: electromyography).

Figure 2.
(a) The myofascial trigger points are visualized as a hypoechoic region which the red arrow points to with an elliptical appearance in ultrasound imaging. (b) The ultrasound image shows both the needle tip and the myofascial trigger points as indicated by the yellow arrow in the picture. The location of the needle tip indicates the detection of continuous EPN; any nodule identified at this site is hypoechoic.
Figure 2.
(a) The myofascial trigger points are visualized as a hypoechoic region which the red arrow points to with an elliptical appearance in ultrasound imaging. (b) The ultrasound image shows both the needle tip and the myofascial trigger points as indicated by the yellow arrow in the picture. The location of the needle tip indicates the detection of continuous EPN; any nodule identified at this site is hypoechoic.


{kind=link}
{kind=link}
Table 1.
Crosstab of data obtained from stage 1.
| EPN | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| US Image | Positive | 148 | 2 | 150 |
| Negative | 0 | 28 | 28 | |
| Total | 148 | 30 | 178 | |
Table 2.
Crosstab of data obtained from stage 2.
| US Image | ||||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| EPN | Positive | 148 | 0 | 148 |
| Negative | 18 | 12 | 30 | |
| Total | 166 | 12 | 178 | |
Table 3.
Performance of ultrasonography for assessing myofascial trigger points.
| Ss | Sc | PPV | NPV | PLR | NLR | A | P | ||
|---|---|---|---|---|---|---|---|---|---|
| Stage | 1 | 100% | 93.3% | 98.7% | 100% | 15 | 0 | 98.9% | 98.7% |
| 2 | 100% | 40% | 89.2% | 100% | 1.67 | 0 | 89.9% | 89.2% | |
Ss: Sensitivity; Sc: Specificity; PPV: Positive predictive value; NPV: Negative predictive value; PLR: Positive likelihood ratio; NLR: Negative likelihood ratio; A: Accuracy; P: Precision.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, H.-Y.; Hong, C.-Z.; Hsieh, Y.-L. Assessment of the Performance of Ultrasonography for Detecting Myofascial Trigger Points. Sensors 2024, 24, 718. https://doi.org/10.3390/s24030718
AMA Style
Chen H-Y, Hong C-Z, Hsieh Y-L. Assessment of the Performance of Ultrasonography for Detecting Myofascial Trigger Points. Sensors. 2024; 24(3):718. https://doi.org/10.3390/s24030718
Chicago/Turabian StyleChen, Han-Yu, Chang-Zern Hong, and Yueh-Ling Hsieh. 2024. "Assessment of the Performance of Ultrasonography for Detecting Myofascial Trigger Points" Sensors 24, no. 3: 718. https://doi.org/10.3390/s24030718
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.