1. Introduction
Balance and mobility are fundamental contributors to independent living throughout the lifespan. In adults over the age of sixty-five, falls are the leading cause of fatal and non-fatal injuries [
1], which is particularly troubling as is it predicted that by 2030, older adults will outnumber children for the first time in U.S. history [
2]. Therefore, much research has endeavored to develop effective rehabilitative practices to mitigate, or even eliminate, mobility impairments in aging and neurodegenerative populations [
3,
4,
5].
One therapeutic approach used to improve mobility in clinical populations is the use of transcutaneous electric nerve stimulation (TENS). TENS is a relatively new approach to improving sensorimotor function that has shown promising results and is emerging as a wearable system aimed at improving wellness and health outcomes in many populations [
6,
7,
8]. TENS has historically been used to manage pain [
9] and muscle spasticity [
10], but has recently been applied to improve gait and balance in various populations [
6,
7,
8,
11]. TENS is a method of electrical stimulation in which the applied current is targeted directly at the sensory nerve fibers. When applied to improve the sensorimotor function of mobility, electrodes are placed on the muscles of the lower limbs and the applied current is set at a level below the motor threshold to minimize any evoked muscle contractions. Used in this way, action potentials in several sensory receptors are elicited both in and around the targeted muscle [
12,
13].
Recent research has found that, when applied concurrently with the clinical metrics of mobility, TENS improved the performance compared to the same metrics without TENS [
6,
7,
8]. Almuklass and colleagues [
7] applied continuous pulses just below the motor threshold in people with multiple sclerosis as well as age-matched controls as they performed metrics of sensorimotor function. The authors found that both groups (MS and controls) improved in the 6-min walk test and the MS group also improved in a timed chair rise test when compared to performing with no TENS. Additionally, Elboim-Gabyzon et al. [
6] showed that patients recovering from hip surgery walked further during a 2-min walk test when receiving TENS than a group that received no stimulation. Finally, in a review article including 11 studies and 439 stroke survivors, Kwong et al. [
8] concluded that TENS is beneficial to walking and mobility and improves the patients’ walking capacity.
While there is ample evidence of the benefit that TENS has on gait and mobility, the underlying mechanisms that lead to these improvements are not understood. Commonly when performing research with TENS, the amplitude is set at a level below the motor threshold (i.e., the minimal intensity of stimulation that generates an involuntary motor response) [
13]. Thus, the argument that any benefit comes from the direct excitation of additional muscle activation is unlikely. Recent work has provided evidence that sensory input has a much larger impact on the overall motor function than has previously been understood [
14,
15,
16,
17,
18]. Thus, the observed benefits in gait and mobility that result from the use of TENS may be due to increased sensory input relaying additional information about body orientation. However, it is not clear how the additional information is used by the central nervous system (CNS) to inform the body position awareness or construct motor plans. One hypothesis is that the additional sensory input decreases the total noise in the incoming sensory data, leading to less uncertainty in the central nervous system’s (CNS) estimation of body orientation. If this were the case, the observed benefits that accompany the use of TENS would be due to improved positional awareness, leading to more efficient motor plans. Though this hypothesis seems conceptually valid, identifying a way to measure and quantify it requires robust assessment.
Bayesian inference is a statistical model that has been used by researchers to understand how the CNS estimates body position based on uncertain sensory information [
19,
20]. Simply put, Bayesian inference posits that the most likely estimate of an unknown parameter comes by combining the available data with previously collected data to minimize the amount of uncertainty in the final estimate. Specific to the context of motor control, this suggests that the most certain estimate for the location of a body part is calculated by considering the incoming sensory information as well as the expected body positions based on previous movement attempts. Past research has shown that the CNS calculates the body position in a way consistent with Bayesian inference [
19,
21]. Additionally, we have shown in previous research that the CNS estimates the position of the center of mass (CoM) during full body stepping movements in a way that is consistent with Bayesian inference [
22]. Using the Bayesian methods in a novel way, we hope to expose some of the underlying perceptual mechanisms that are benefited by the addition of TENS on the lower extremities during mobility related movements.
The purpose of this study was to clarify the underlying mechanisms that lead to the benefits of using TENS to improve gait and mobility. Using the model of Bayesian inference in motor control, we expected that the participants would display less uncertainty in their responses when estimating their CoM position during a stepping movement. Additionally, in line with previous research [
22], we expected that participants would display better static balance when receiving TENS than without TENS.
3. Results
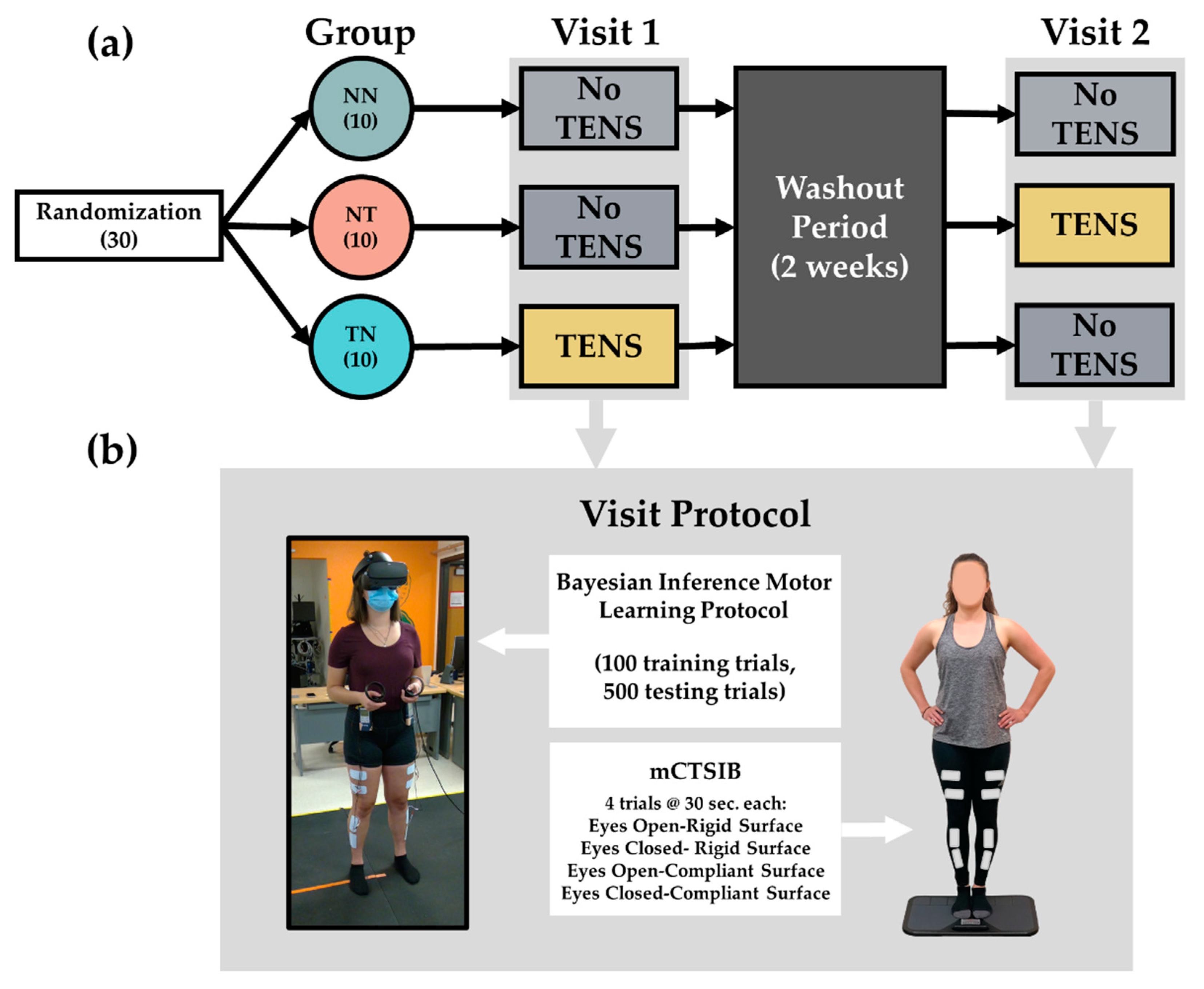
In total, 30 neurotypical healthy adult participants were included in the final analysis. Characteristics of all of the study participants and groups are presented in
Table 1. To assess the differences in the uncertainty of the participants’ responses across study visits and groups, we performed a three by two repeated measures ANOVA. The results of that ANOVA showed a main effect for visit (F
(1,207) = 37.28,
p < 0.001). The corresponding means indicated that response uncertainty, on average across all participants irrespective of group, decreased from visit 1 to visit 2 (
Figure 3). Additionally, we found evidence of a visit by group interaction effect (F
(2,207) = 3.29,
p = 0.039). The corresponding means indicated that the change in uncertainty across visits was not the same for each group. Follow-up pairwise comparisons indicated that the groups that received TENS, whether in the first or second visit (NT and TN), both decreased in their response uncertainty from visit 1 to visit 2. Results from the post hoc comparison estimated that the uncertainty metric for the NT group in visit 1 (
M = 2.78,
SD = 0.57) decreased in visit 2 (
M = 2.24,
SD = 0.47) by 0.54 cm (
d = 1.17,
p < 0.001) and the TN group from visit 1 (
M = 2.43, SD = 0.75) to visit 2 (
M = 2.05,
SD = 0.71) decreased by 0.39 cm (
d = 0.84,
p < 0.001). However, there was not enough evidence to conclude that the group that received no TENS on both visits (NN) reduced their response uncertainty from visit 1 (
M = 2.57,
SD = 0.59) to visit 2 (
M = 2.40,
SD = 0.76) (
d = 0.36,
p = 0.108). These results corroborate our first hypothesis that TENS would decrease the uncertainty in the participants’ estimates for where they were in space. However, since there was also a main effect of visit, we performed two additional hypothesis tests to further estimate the effect of TENS on the uncertainty metric of all groups. The first hypothesis test considered the means from all three groups at the first visit. For the first visit, two groups (NT and NN) did not receive TENS and one group (TN) received TENS. To estimate the TENS effect using visit 1 only, we subtracted the sample mean of the TN group at visit 1 from the average of the means from both groups who did not receive TENS on visit 1 (Equation (1)):
where
represents the sample mean from group NT on visit 1,
represents the sample mean from group NN on visit 1; and
represents the sample mean from group NT on visit 1.
The estimate from computing Equation (1) was 0.24 cm. This estimate indicates that the TENS group had a lower uncertainty than the average of the non-TENS groups at visit 1. While there was not enough evidence to conclude that this effect was different from 0 (p = 0.263), the 95% confidence interval [−0.19, 0.67] suggests that the TENS could slightly increase the uncertainty (−0.19 cm) or provide a substantial reduction (0.67 cm).
The second custom hypothesis test that we performed was conducted to isolate the TENS effects across visits. To do this, we compared the differences in RMSE between visits for group NT and group NN. Even though our pairwise comparison between visits for the NN group did not indicate a significant decrease in uncertainty, the results of our ANOVA showed a main effect of visit, indicating that the uncertainty value decreased from visit 1 to visit 2 regardless of group. The difference in means between visit 2 and visit 1 for the NN group represents an estimate of the visit effect on the uncertainty metric. The difference in means between visit 2 and visit 1 for the NT group represents an estimate of the visit effect plus the TENS effect. To identify the TENS effect across visits, we subtracted the difference in means in the NN group from the difference in means in the NT group (Equation (2)):
where
represents the sample mean from group NT on visit 2 and
represents the sample mean from group NN on visit 2.
The estimate from computing Equation (2) was 0.371 cm. This estimate suggests that the change in uncertainty due to TENS was 0.371 cm larger than the change in uncertainty due to repeated visits (0.16 cm) (CI [0.02, 0.72], p = 0.037). We note that the p values (or significance levels) from these custom hypothesis tests were not adjusted to account for multiple comparisons.
Taken together, we believe that the results of our study provide enough evidence to conclude that TENS decreases the amount of uncertainty present in the participants’ estimates of their CoM position as they perform stepping movements.
We also hypothesized that TENS would result in participants performing better in a static test of balance. This would be measured by an increase in the VTC measurement when TENS was applied compared to when TENS was not applied. The sample means for the VTC values across the mCTSIB conditions are reported in
Table 2. The results of the two by four repeated measures ANOVA with random effects indicated no significant main effect for TENS on the VTC measurement (F(1,18)= 0.320,
p = 0.579), a significant main effect for the mCTSIB condition (F(3,54) = 73.62,
p < 0.001), but no significant TENS by the mCTSIB condition interaction effect (F(3,54) = 0.260,
p = 0.852). Follow-up pairwise comparisons between the mCTSIB conditions, regardless of group, all showed significant decreases from condition one to condition four (
p < 0.001), except for conditions two and three (rigid surface eyes closed vs. compliant surface eyes open), which provided a significance level of
p = 0.960. This decrease in VTC across mCTSIB conditions suggests a decrease in balance performance across the conditions and is in line with previous research [
27].
4. Discussion
The purpose of this study was to clarify the underlying mechanisms that lead to the observed improvements in gait and balance that are seen with the use of TENS. To address this purpose, we applied a theoretical model of Bayesian inference to measure and assess sensory uncertainty and how it influences the body position estimates during a full body stepping movement. Furthermore, we applied a crossover study design that consisted of three study groups performing the Bayesian motor learning assessment on two separate visits either with or without the addition of concurrent TENS. The results of our analyses are in line with our hypothesis that TENS decreases the uncertainty that participants showed as they estimated their body position in our assessment. The following section will elaborate on the main findings gathered from this study and discuss future applications for how this knowledge can be used to benefit this field of research.
Taking all of the results from our analyses in this study together, we concluded that the amount of uncertainty in the participants’ estimations of their CoM position during a stepping movement was decreased with the addition of TENS. This main finding provides insights into the perceptual mechanisms that are affected by TENS and leads to the observed improvements in motor performance with its application [
7,
28]. With less sensorimotor uncertainty regarding the position of the involved body parts, the CNS can make more efficient motor and plans to execute the movements involved in goal-oriented motor skills. For example, when navigating through a crowded grocery store, the CNS has a clearer estimate for the foot’s position when forced to avoid tripping on a fellow shopper’s cart. This increased clarity may also lead to improvements in movement efficacy in populations known to have sensory and motor impairments due to disease or injury such as multiple sclerosis and diabetes [
7,
28]. The low cost of a TENS unit makes this a simple form of therapeutic intervention that may have a serious benefit to multiple populations. Future research will continue to investigate how improvements in sensorimotor uncertainty can benefit motor performance in various populations as well as the best practices of applying this technology to maximize its effects.
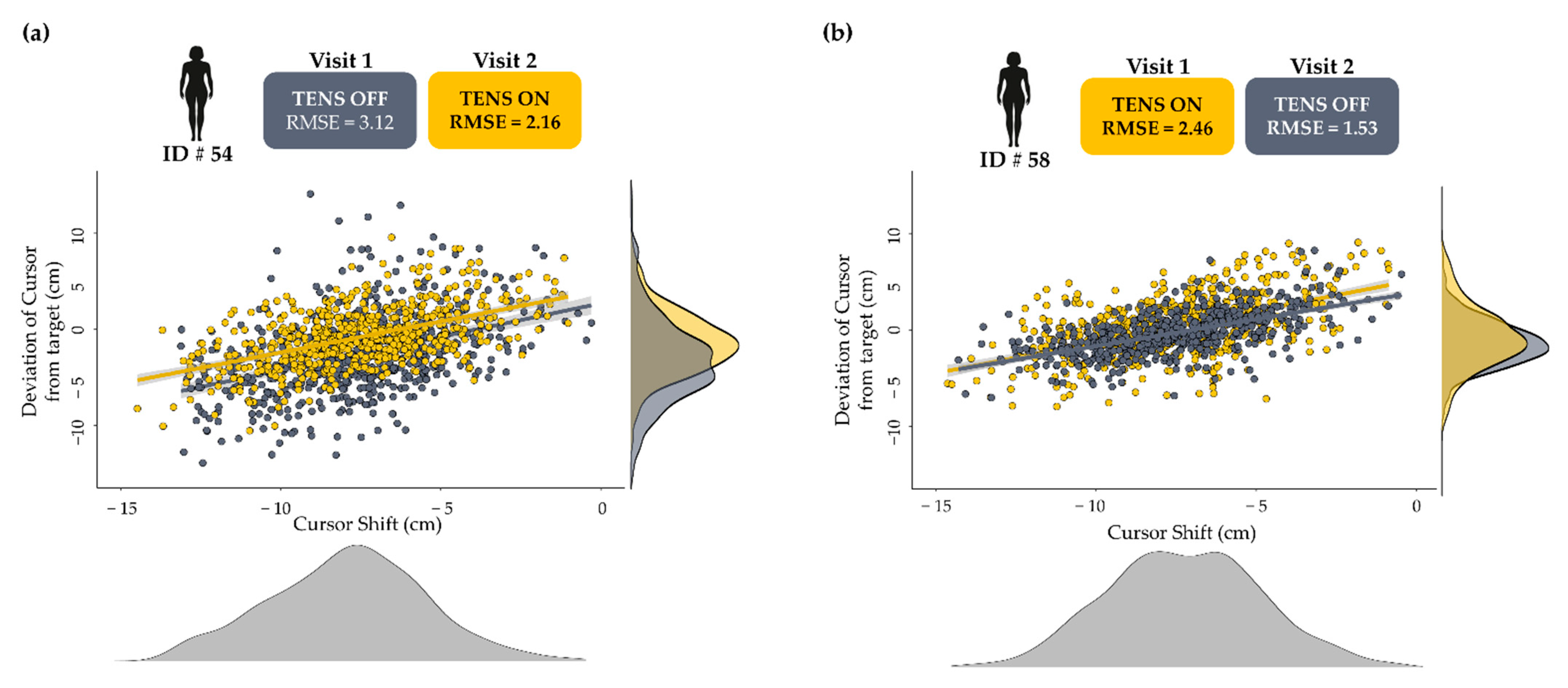
Furthermore, we showed that group TN, who received TENS on their first visit only, demonstrated the least response uncertainty in their first visit when compared to other groups on the same visit. Interestingly, group TN went on to further decrease their response uncertainty in the second visit without TENS and still reported less uncertainty than both groups on the second visit.
Figure 4 shows the individual data from a participant in both groups who received TENS and exemplifies the advantage of receiving TENS on the first visit and the continued benefit after 2 weeks. A constant concern that is associated with many forms of sensory augmentation is whether any observed benefits will persist once the additional sensory stimulus is removed. One implication of our findings is that, at least in certain circumstances, the benefit that is gained from the addition of TENS while learning and performing a new movement is retained in future performances of the same movement. Furthermore, when compared to group NT, who received TENS on their second visit, it seems that TENS is most beneficial when it is applied early in the motor learning process. Recent work has shown that when learning a new motor skill, functional changes occur in the somatosensory cortex to process incoming sensory data prior to any observed changes in the specific motor areas of the brain [
16,
29]. Taken together, this further emphasizes the importance of sensory input to motor performance and specifically to motor learning. As mentioned previously, Bayesian motor control theory posits that the CNS combines incoming sensory information with learned expectations of body position based on previous attempts.
However, when performing a novel movement, expectations of body position are often ill-informed or absent altogether. In this case, learning the physical and sensory consequences of a new motor skill is a priority to ensure accurate position estimation and movement performance. From this perspective, it seems logical that enhancing the incoming sensory information with TENS would assist the CNS in identifying pertinent sensory information that informs it of bodily states while performing new movements. The finding that this benefit is retained and even continues to improve following a two-week washout period is compelling and merits the need for further examination. An intervention as simple and cost-effective as TENS could be incredibly beneficial to clinical populations striving to learn, or re-learn, new motor skills in response to injury or disease.
Interestingly, we found that the addition of TENS had no effect on static balance, as assessed by the mCTSIB. Much previous research has found external electric stimulation of the lower limbs to be effective at improving balance metrics [
13,
30,
31]. However, Paillard et al. [
32] recently found that the participants’ responsiveness to the electrical stimulation of sensory nerves to improve balance depends on their baseline balance abilities. Our study included only young participants that historically have exceptional balance abilities. It is possible that any effect of TENS on the balance performance in this healthy population goes unnoticed because they are already proficient at controlling balance. Additionally, it is of interest that much of the previous research that has shown improvements in performance with the addition of TENS included methods of assessment that were more dynamic in nature, requiring the movement of many joints in multiple planes of motion, in contrast to the static conditions inherent to our balance assessment [
7,
8].
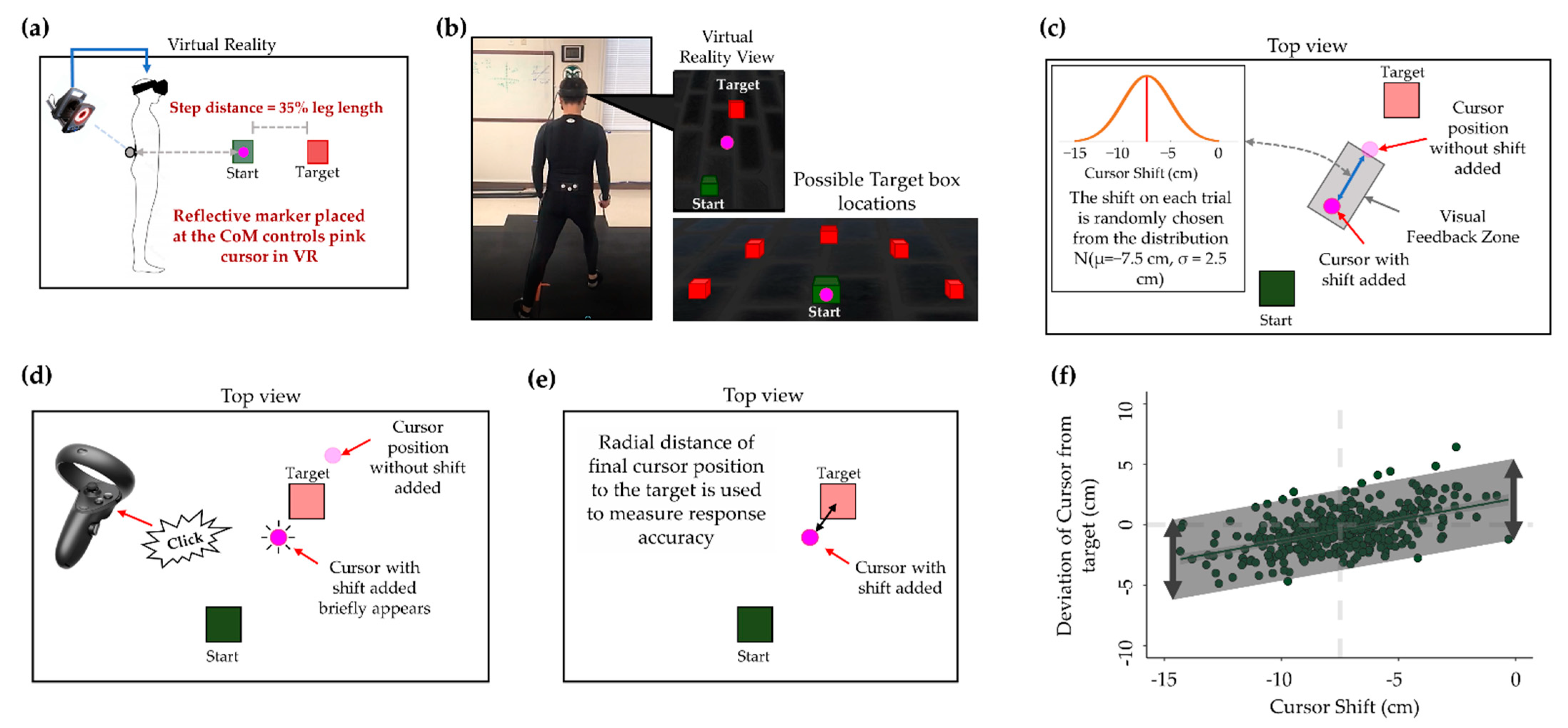
With the findings from this study, we can conclude that the addition of TENS to the muscles of the lower extremities leads to a decrease in sensorimotor uncertainty for the position of the CoM during a stepping movement. This conclusion is based on the results of a repeated measures ANOVA that we performed as well as the follow-up pairwise comparisons. When interpreting these results, the reader must bear in mind a few key principles. First, it needs reminding that the uncertainty metric that we used as our outcome metric is from the RMSE of a regression line of each participant’s response in their study visits. The RMSE is meant to represent the variability in the estimate made by the CNS of the CoM position throughout a stepping movement based on the incoming sensory information as well as the learned expectations for the CoM position. We acknowledge that the true metric of uncertainty for each participant is a latent variable that cannot be directly observed, but rather, must be inferred through carefully designed methods. We are seeking to measure a perception that is built upon sensory information and demonstrated through skilled behavioral patterns that arise through many trials. Though novel and unique, we are confident in the results of this study and the conclusions drawn from them about how sensory information can be manipulated to improve performance.
Next, we based our main conclusions on the results of the four statistical tests that we performed. The results of the ANOVA that we calculated indicated that the three groups responded significantly different in their uncertainty measurement across visits 1 and 2. We also performed Tukey’s honest significance tests, which revealed that both groups who received TENS reduced their uncertainty values from visit 1 and visit 2, whereas the NN group did not. However, because there was evidence of an overall visit effect in the ANOVA (p < 0.001), it is possible that the number of trials and participants included in this study were not enough to see a significant difference in this metric. Through further follow-up analyses on subgroups in our study, we performed custom hypothesis tests designed to isolate the TENS effect on uncertainty. We showed that the TENS led to a decrease in uncertainty for the group who received TENS on the first visit, although this was not a significant decrease. However, with the reported confidence interval, we can be 95% confident that the true change in uncertainty was between +0.19 cm (an increase) and −0.67 cm (a decrease) because of TENS. In isolation, this would not be sufficient data to conclude that TENS decreases uncertainty, however, it has sparked interest into further analyses to parse out the TENS effect. To this end, we performed an additional hypothesis test seeking to estimate the TENS effect across visits. We found that TENS led to a decrease in uncertainty from visit 1 to visit 2. As mentioned previously, we did not adjust for multiple comparisons, which increases our chances of a Type I error. However, as this analysis was exploratory in nature, we feel confident that taking all of these results in total, we can conclude that the addition of TENS to the muscles of the lower limbs leads to a decrease in sensorimotor uncertainty for the position of the CoM during a stepping movement. We invite future research to be performed to further identify the effects of TENS on sensory uncertainty.
The exact mechanisms that lead to the decrease in positional uncertainty due to TENS remain to be seen. Previous work using various methods of peripheral stimulation of sensory fibers have suggested stochastic resonance may be a large reason for the benefits that accompany these types of sensory augmentation [
13,
33]. In this sense, the electrical stimulation provided by TENS may add low-level noise that enhances the detection and transmission of weak sensory signals by amplifying the total signal and, as a result, the sensory cues most important to coordinating the current motor task. Furthermore, Paillard [
32] suggests that this also can change the ion permeability of the mechanoreceptors (group Ia and IIa afferents of muscle spindles), priming them, in a sense, to make them more likely to fire action potentials and increase sensory input to the brain and spinal cord. Applying a similar study purpose to decrease sensory uncertainty, Macerello and colleagues applied peripheral nerve stimulation with high-frequency vibration to the muscle of the wrist as healthy and clinical participants completed a battery of upper extremity motor tasks [
34]. They found that both groups decreased the completion time of the motor tasks and showed a decrease in the EEG beta power over the sensorimotor cortices as they received the stimulation. Altogether, our results combined with previous research, support the hypothesis that TENS, and other methods of afferent stimulation, improve motor performance by decreasing the noise inherent to sensory data and permitting users to be more certain of their body position as they perform motor tasks.








{kind=link}
{kind=link}
{kind=link}
{kind=link}