
Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Attitude towards the selected technology to define whether or not the proposed technology (robot, wearable sensors, app and devices, etc.) will be used if integrated into the services.
- Prioritize the proposed service to preliminary assess the impact of PHArA-ON’s solutions and prioritize the development phase.
2.1. Interview Guidelines
- 1.
- Informed consent
- Acquire informed consent;
- Turn on the video/phone recording system;
- Verify informed consent orally with the tape recorder on;
- Reconfirm the participant’s consent while the tape recorder is still on.
- 2.
- Part 1: Introduction
- Ask questions about socio-demographic information: age, sex, level of education;
- First investigation of interest in the technology (Table 1): current use of technological devices, technologies of greatest interest as needed;
- Support devices: To what extent the support devices (robots and/or sensors) could be useful.
- 3.
- Description of PHArA-ON project and Services
- If the interview was conducted by phone, the interviewer read a story, whereas if the interview was conducted by videoconference system, a slide presentation was used.
- 4.
- Part 2: Interview on PHArA-ON services
- Section A: Demographic information;
- Section B: Use of Technology and definition of main and secondary purposes about each proposed technology;
- Section C: Devices of the support, what I think of the potential of PHArA-ON’s services;
- Section D: Impact of PHArA-ON. After showing presentation slides for the identified services, the participants are asked to what extent PHArA-ON can be useful;
- Section E: Users’ needs and priorities, using the Goal Model framework. Indeed, the Goal Model can be considered as a container of four components: functional goals, quality goals, emotional goals and stakeholder roles [19].The objective is to identify the respondent’s needs in terms of physical, cognitive and social assistance, and acceptance level of technology;
- Section F: Conclusions and notes on the interview.
- 5.
- Thanks and conclusion of the interview
- Greetings
- Turn-off the video recording.
2.2. Recruitment Criteria for Respondents
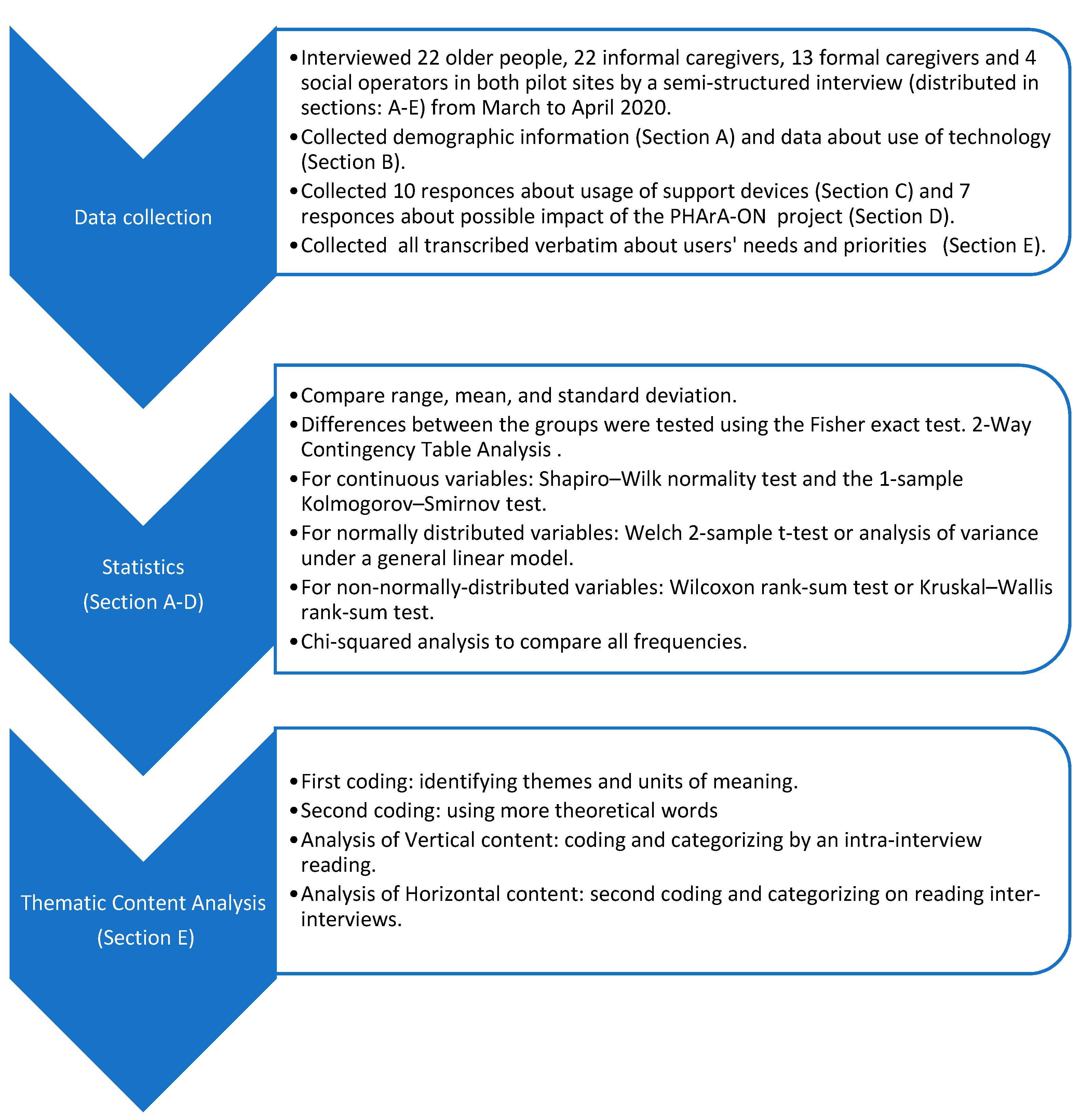
2.3. Data Analysis
3. Results
3.1. Attitudes towards the Technologies
3.2. Opinions on the Usefulness of Support Devices
3.3. Impact of PHArA-ON
3.4. Users’Needs and Priorities
- ➢
- The specific needs for heath management are the following:
- ▪
- Stimulation (high priority): This could improve the assistance provided with home physical and cognitive rehabilitation programs. It could fill a gap due to the lack of operators who can perform this type of care at home and reduce the number of times the patient has to go to the hospital for cognitive stimulation. Programs could be tailored to the clinical condition of each older person. This service will stimulate older adults to engage in a healthier lifestyle by referring to good practices on a daily basis. The devices should be very usable by the patients: “for example, if physical exercises are proposed, the screen must be large, you must see well and hear well, and maybe even… it would be fantastic if, in the face of an exercise that is requested, the device itself also gives feedback on whether it was done well…” (CSS-P01); “It would make possible to maintain physical and cognitive training” (CSS-E04); “It would help me to do physical exercise with the help of a robot or be stimulated with exercises” (UP-E03). Concerning emotional goals, older adults will be involved and empowered. The technical requirements are the following: (1) The system should propose a selection of physical and cognitive exercises that the users can access on their smart TV and/or personal device; (2) The caregiver can select the exercises for the users on the system; (3) The system will analyse the statistics related to the number and performance of exercises completed.
- ▪
- Monitoring (high priority): Both the doctor and family members could know the health status of the older adult (be aware). This could improve pharmacological compliance and monitor physical exercise and nutrition with a consequent reduction in the workload of caregivers. It will allow older persons to receive remote psychological support in a timelier manner. It will be possible to detect a consequent state of empowerment, safe and reassured. “[…] therefore, the sensors could monitor the conditions and allow the family member to go away for daily tasks. The robot could also have video surveillance functions” (UP-I04); “The safety devices could help the older adult in their autonomy as well as the technologies for the administration of drugs; but also, the equipment for monitoring and implementing individualized care plans” (UP-P03); “It would anticipate hospital practices” (CSS-E07). The technical requirements are the following: (1) Through the Smartphone, Tablet or Smart TV user interface, the older person should be able to videoconference the doctor (or nurse); (2) The system should monitor patients’ total movement in real-time, using data collected by a Smart watch; (3) The aggregate data should be visualized on the caregiver interface; (4) The caregiver should be able to access, over the caregiver interface, the “history” of total movements performed throughout the day.
- ▪
- Monitoring the environment (medium priority): Monitoring of environmental conditions (through systems for controlling temperature, gas-smoke, light, humidity, entrance-exit of the main doors, etc.), as well as improving safety and well-being, will allow a better organization of care and support. For example, by detecting an ambient temperature that is too high in the home, the system could suggest that the older adult drink more water to hydrate and avoid dehydration (which is one of the most common causes of mortality, particularly frequent in the summer season). All this will lead to a reduction in stress for the older adult and the caregiver, and a reduction in the workload of the latter. It will be possible to allow a consequent state of safety and reassurance. “More than anything else, the control (monitoring of the environment) could create the optimal situation for the safety of the person” (UP-I03). The technical requirements are the following: (1) Some environmental parameters such as humidity, temperature could be measured by the sensors installed in the system; (2) Movement sensors are requested to monitor the total movement within a specific environment; (3) The system should integrate all the sensors and make the collected data available on the caregiver dashboard; (4) Parameters’ pattern analysis (Anomalies detection) was requested.
- ▪
- Emergency call (low priority): Activation of an emergency call that allows both to intervene in emergencies on time and to contact family members. All this would avoid accidents. The older adults will be remotely supervised 24 h a day and there will be an interaction between the older adults, the referring medical centre and family members, granting everyone a state of reassurance. “Alarm sensors. Screen with video explanation, connection with external via video camera” (UP-P08).
- ➢
- For Socialisation, the specific need is “To promote social inclusion” with a high priority:
- ▪
- To reduce isolation and promote socialisation, a fundamental brick is necessary (knowledge of the person’s history and what his hobbies and habits are).
- ▪
- Prevent loneliness: “The system should be able to detect an effective phenomenon of isolation, which is often difficult to intercept if we see the patient once every six months” (CSS-P01). Furthermore, it should be more reliable than the observation and the story of the same individual or some family member. With or without the presence of isolation, the system tries to promote the connection with family and friends through participation in social groups or through the reporting of events (selected according to the interests of the individual person) in which to participate, of which the older adult is not aware of.
- ▪
- Information: The service should send information useful for health. “For example, during seasonal flu, send specific messages on that topic. Or, messages/advice every 4/5 days like << please go out because there are so many activities you can do outdoors rather than at home… move more>>” (CSS-P02). It would be useful to periodically send information to the elderly to keep the communication channel alive with the project and with a structure that follows the project. In addition, the elderly may receive reports of activities in which they can participate, in which they could acquire a new intellectual and/or manual ability through courses that teach them to do something more than what they already know.
4. Discussion
5. Conclusions
- -
- To design and evaluate technology in the context of healthy and active ageing;
- -
- To acquire relevant knowledge on user needs to develop technologies that can handle real life situations of older people;
- -
- Useful insights about the attitude and availability of end-users in using technologies in clinical practice;
- -
- To provide important guidelines to improve the PHArA-ON system while specific experimentation stages are expected to be carried out;
- -
- To understand which kind of technology is more acceptable;
- -
- To provide feedback regarding the development priority related to the impact of the proposed services.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Decade of Healthy Ageing Baseline Report. Available online: https://www.who.int/publications/i/item/9789240017900 (accessed on 22 January 2021).
- World Health Organization. Ageing. Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 22 January 2021).
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 22 January 2021).
- Iancu, I.; Iancu, B. Elderly in the Digital Era. Theor. Perspect. Ass. Technol. 2017, 5, 60. [Google Scholar]
- Lin, Y.; Chu, H.; Yang, C.Y.; Chen, C.H.; Chen, S.G.; Chang, H.J.; Hsieh, C.J.; Chou, K.R. Effectiveness of group music intervention against agitated behavior in older persons with dementia. Int. J. Geriat. Psych. 2011, 26, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Broekens, J.; Heerink, M.; Rosendal, H. Assistive social robots in older care: A review. Gerontech 2009, 8, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Kelley, E.; Hurst, J. Health Care Quality Indicators Project: Conceptual Framework Paper; Organization for Economic Co-Operation and Development (OECD): Paris, France, 2006. [Google Scholar]
- Misselhorn, C.; Pompe, U.; Stapelton, M. Ethical considerations regarding the use of social robots in the fourth age. J. Gerontopsychol. Geriatr. Psychiatry 2013, 26, 121–133. [Google Scholar] [CrossRef]
- Ljungblad, S.; Nylander, S.; Nørgaard, M. Beyond Speculative Ethics in HRI? Ethical Considerations and the Relation to Empirical Data. In Proceedings of the 6th International Conference on Human Robot Interaction, Lausanne, Switzerland, 6–9 March 2011. [Google Scholar]
- Schinazi, V. Representing Space: The Development, Content and Accuracy of Mental Representations by the Blind and Visually Impaired. Ph.D. Thesis, University College London, London, UK, 2008. [Google Scholar]
- Real, S.; Araujo, A. Navigation Systems for the Blind and Visually Impaired: Past Work, Challenges, and Open Problems. Sensors 2019, 19, 3404. [Google Scholar] [CrossRef] [Green Version]
- García-Peñalvo, F.J.; Franco-Martín, M. Sensor Technologies for Caring People with Disabilities. Sensors 2019, 19, 4914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, N.A. Navigating without Vision: Principles of Blind Spatial Cognition. In Handbook of Behavioral and Cognitive Geography; Edward Elgar Publishing: Cheltenham, UK; Northampton, MA, USA, 2018; pp. 260–288. [Google Scholar]
- Chirico, I.; Chattat, R.; Dostálová, V.; Povolná, P.; Holmerová, I.; de Vugt, M.E.; Janssen, N.; Dassen, F.; Sánchez-Gómez, M.C.; García-Peñalvo, F.J.; et al. The Integration of Psychosocial Care into National Dementia Strategies across Europe: Evidence from the Skills in DEmentia Care (SiDECar) Project. Int. J. Environ. Res. Public Health 2021, 18, 3422. [Google Scholar] [CrossRef]
- Langefors, B. Management Information System Design. IAG Q. 1969, 2, 4. [Google Scholar]
- Ackoff, R.L. Management Misinformation Systems. Manag. Sci. 1967, 14, B-147. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.; Pedell, S.; Lopez-Lorca, A.A.; Mendoza, A.; Sterling, L.; Keirnan, A. Emotion-led modelling for people-oriented requirements engineering: The case study of emergency systems. J. Syst. Softw. 2015, 105, 54–71. [Google Scholar] [CrossRef] [Green Version]
- Gavard-Perret, M.L.; Gotteland, D.; Haon, C.; Jolibert, A. Méthodologie de la recherche. In Réussir son Mémoire ou sa thèse en Sciences de Gestion; Pearson Éducation: Paris, France, 2008. [Google Scholar]
- Fretwell, M. The Consensus Conference on Comprehensive Geriatric Assessment: A dialogue is the beginning of consensus. J. Am. Geriatr. Soc. 1988, 36, 377–379. [Google Scholar]
- von Terzi, P.; Tretter, S.; Uhde, A.; Hassenzahl, M.; Diefenbach, S. Technology-Mediated Experiences and Social Context: Relevant Needs in Private Vs. Public Interaction and the Importance of Others for Positive Affect. Front. Psychol. 2021, 1, 718315. [Google Scholar] [CrossRef]
- Hassenzahl, M.; Diefenbach, S. Well-being, need fulfillment, and Experience Design. Des. Well-Being Workshop 2012, 25, 2013. [Google Scholar]
- Hassenzahl, M.; Wiklund-Engblom, A.; Bengs, A.; Hägglund, S.; Diefenbach, S. Experience-oriented and product-oriented evaluation: Psychological need fulfillment, positive affect, and product perception. Int. J. Hum. Comp. Interact. 2015, 31, 530–544. [Google Scholar] [CrossRef]
- Blinka, M.D.; Buta, B.; Bader, K.; Hanley, C.L.; Schoenborn, N.; McNabney, M.; Xue, Q.L. Developing a sensor-based mobile application for in-home frailty assessment: A qualitative study. Innov. Aging 2019, 3 (Suppl. 1), S831–S832. [Google Scholar] [CrossRef] [Green Version]
- Aloulou, H.; Mokhtari, M.; Abdulrazak, B. Pilot Site Deployment of an IoT Solution for Older Adults’ Early Behavior Change Detection. Sensors 2020, 20, 1888. [Google Scholar] [CrossRef] [Green Version]
- Kekade, S.; Hseieh, C.H.; Islam, M.M.; Atique, S.; Mohammed Khalfan, A.; Li, Y.C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Prog. Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef]
- Teixeira, E.; Fonseca, H.; Diniz-Sousa, F.; Veras, L.; Boppre, G.; Oliveira, J.; Pinto, D.; Alves, A.J.; Barbosa, A.; Mendes, R.; et al. Wearable Devices for Physical activity and Healthcare Monitoring in Elderly People: A Critical Review. Geriatrics 2021, 6, 38. [Google Scholar] [CrossRef]
- Lehoux, P.; Grimard, D. When robots care: Public deliberations on how technology and humans may support independent living for older adults. Soc. Sci. Med. 2018, 211, 330–337. [Google Scholar] [CrossRef]
- Vandemeulebroucke, T.; Dzi, K.; Gastmans, C. Older adults’ experiences with and perceptions of the use of socially assistive robots in aged care: A systematic review of quantitative evidence. Arch. Gerontol. Geriatr. 2021, 95, 104399. [Google Scholar] [CrossRef]
- Nakaoku, Y.; Ogata, S.; Murata, S.; Nishimori, M.; Ihara, M.; Iihara, K.; Takegami, M.; Nishimura, K. AI-Assisted In-House Power Monitoring for the Detection of Cognitive Impairment in Older Adults. Sensors 2021, 21, 6249. [Google Scholar] [CrossRef]
- Ye, J.; Ma, Q. The Effects and Patterns among Mobile Health, Social Determinants, and Physical activity: A Nationally Representative Cross-Sectional Study. AMIA Annu. Symp. Proc. 2021, 2021, 653–662. [Google Scholar]
- van Genderen, M.E.; Vlake, J.H. Virtuelegezondheidszorg [Virtual healthcare; use of virtual, augmented and mixed reality]. Ned. Tijdschr. Geneeskd. 2018, 162, D3229. [Google Scholar] [PubMed]
- Pilotto, A.; D’Onofrio, G.; Benelli, E.; Zanesco, A.; Cabello, A.; Margelí, M.C.; Wanche-Politis, S.; Seferis, K.; Sancarlo, D.; Kilias, D. Information and communication technology systems to improve quality of life and safety of Alzheimer’s disease patients: A multicenter international survey. J. Alzheimers Dis. 2011, 23, 131–141. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Sancarlo, D.; Raciti, M.; Burke, M.; Teare, A.; Kovacic, T.; Cortis, K.; Murphy, K.; Barrett, E.; Whelan, S.; et al. MARIO Project: Validation and Evidence of Service Robots for Older People with Dementia. J. Alzheimers Dis. 2019, 68, 1587–1601. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.T.; Fu, S.H.; Hsieh, P.L.; Lin, Y.L.; Yang, S.Y. Investigating the Relationship between Media Usage, Depression, and Quality of Life among Older Adults. Healthcare 2021, 9, 1154. [Google Scholar] [CrossRef] [PubMed]
- Tong, F.; Yu, C.; Wang, L.; Chi, I.; Fu, F. Systematic Review of Efficacy of Interventions for Social Isolation of Older Adults. Front. Psychol. 2021, 12, 554145. [Google Scholar] [CrossRef]
- D’Onofrio, G.; Fiorini, L.; de Mul, M.; Fabbricotti, I.; Okabe, Y.; Hoshino, H.; Limosani, R.; Vitanza, A.; Greco, F.; Giuliani, F.; et al. Agile Co-Creation for Robots and Aging (ACCRA) Project: New technological solutions for older people. Eur. Geriatr. Med. 2018, 9, 795–800. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Area of Intervention | Description of Service | System Components |
|---|---|---|
| Remote monitoring |
|
|
| Facilitating socialization |
|
|
| Cognitive and physical stimulation program |
|
|
| Support caregiver at work |
|
|
| Service | System Components |
|---|---|
| Managing and storing health data |
|
| Remote monitoring |
|
| Facilitating interactions |
|
| Personalized service at seniors’ home and in the domestic environment |
|
| Need Category | Specific Need | Activities | Emotional Goals | O | I | P | Final Priority | Technical Requirement | Technologies |
|---|---|---|---|---|---|---|---|---|---|
| Manage Health | Emergency call | 1. Make an emergency call. | Reassured Safe | 0 | 2 | 3 | Low (5) | The system sends Email, messages or pop-up to family and/or caregivers if anomalies are detected. | Caregivers’ Tablet or Smartphone; Caregiver’s interface; Anomalies detection system |
| Older adults will use the app to make an alert call to the caregiver. | Older person’s Tablet or Smartphone; Robot; Caregiver’s interface; Older adult’s interface | ||||||||
| Stimulation | 1. The older adult is stimulated to perform physical exercises. | Involved | 2 | 5 | 6 | High (13) | The older person should be able through the Smart TV (browser or app) to selectphysical exercises. | Smart TV; Older adults’ Tablet or Smartphone Caregiver’s Tablet or Smartphone Older adult’s interfaceCaregiver’s interface; Physical exercises system | |
| The caregiver can select the exercises for the users on the system. | |||||||||
| The system will analyse the statistical related to the number of exercises performed. | |||||||||
| The system will analyse the performance of the exercise. | |||||||||
| 2. The older adult is stimulated to perform cognitive exercises. | Empowered | 3 | 5 | 6 | High (14) | The system should propose a selection of cognitive exercises that the users can access on his Smart TV and/or personal device. | Smart TV; Older adult’s Tablet or Smartphone Caregiver’s Tablet or Smartphone Cognitive exercises systemCaregiver’s interface | ||
| The caregiver can select the exercises for the users on the system | |||||||||
| The system will analyse the statistical related to the number of exercises performed. | |||||||||
| The system will analyse the output of the cognitive stimulation/assessment performed. | |||||||||
| Monitoring | 1. Psychological support. | Reassured Empowered | 6 | 4 | 3 | High (13) | Through the Smart TV user Interface the older person should be able to call in videoconference the doctor (or nurse). | Smart TV Older adult’s Tablet or Smartphone; Older adult’s interface; Caregiver’s Tablet or Smartphone | |
| Through the Smartphone or Tablet the older person should be able to call in videoconference the doctor (or nurse). | |||||||||
| 2. The caregiver monitors physical activities of older adult. | Safe | 3 | 5 | 3 | High (11) | The system should monitor patients’ total movement in real time, by means of data collected by Smartwatch. | SmartwatchCaregiver’s Tablet or Smartphone Caregiver’s interface; Analysis system | ||
| The aggregate data should be visualized on the Caregiver interface. | |||||||||
| The caregiver should be able to access over the Caregiver interface also to the “history” of total movements performed over the day. | |||||||||
| 3. Monitoring the environment | Reassured Safe | 3 | 5 | 2 | Medium (10) | Some environmental parameters like Humidity, Temperature are measured by the sensors installed in the system. | Sensors; Caregiver’s Tablet or Smartphone Caregiver’s interfaceAnalysis system | ||
| PIR movement are requested to monitor the total movement in a space. | |||||||||
| The system should integrate all the sensors and make the collected data available on the caregiver dashboard. | |||||||||
| Parameters’ pattern analysis (Anomalies detection). | |||||||||
| Socialize | To promote social inclusion | 1. Support by the informal caregiver in inserting information about patient’s life | Empowered | 6 | 5 | 3 | High (14) | The Smart TV will show information about his hobbies. Additionally, he can also see some old photos. | Smart TV Smartphone or tablet |
| The older person can insert his photo in the system. | |||||||||
| 2. Maintaining relationships with friends | Involved | The older should call and see his friends by using the television. | Smart TV Older adult’s Tablet or Smartphone Older adult’s interface | ||||||
| The older can create on his interface small groups of friends to video call. | |||||||||
| 3. Information | Involved Cared of | The system should give advice on local events such as contain courses and news about good health practices. | Smart TV |
| Older Adults | Caregivers | Aligned with Previous Studies [Ref.] | |||
|---|---|---|---|---|---|
| UP | CSS | UP | CSS | ||
| Technology goal: | |||||
| - Robot | [21,22,23,24,25,26,27,28] | ||||
| To perform care and assistance tasks | 58.30% | 40.00% | 52.60% | - | |
| Helping operators in their work | - | - | - | 46.70% | |
| Helping family members | 41.70% | 30.00% | 33.30% | 26.70% | |
| - IoT | |||||
| Improving self-care | 36.40% | - | - | 26.70% | |
| Staying in communication with others | - | 50.00% | - | - | |
| Helping family members | 33.30% | - | - | - | |
| Helping operators in their work | - | 30.00% | 40.00% | - | |
| Staying in communication with others | 25.00% | 30.00% | 33.30% | 46.70% | |
| - AI | |||||
| Performing care and assistance tasks | 41.50% | - | - | 33.30% | |
| Improving self-care | 25.00% | 40.00% | 40.00% | 26.70% | |
| Helping operators in their work | - | 30.00% | 40.00% | - | |
| - App and mobile devices | |||||
| Having social opportunities | 27.30% | 30.00% | - | 40.00% | |
| Helping operators in their work and family members | 41.70% | - | - | - | |
| Staying in communication with others | - | 30.00% | 31.60% | 46.70% | |
| Improving self-care | - | - | 15.00% | - | |
| - Wearable sensors | |||||
| Improving self-care | 36.40% | 40.00% | 44.40% | 46.70% | |
| Helping family members | 33.30% | 30.00% | 38.90% | - | |
| Performing care and assistance tasks | - | - | - | 33.30% | |
| - Virtual/augmented reality | |||||
| Performing care and assistance tasks | 58.30% | - | 33.30% | - | |
| Helping operators in their work | - | 40.00% | 38.90% | 26.70% | |
| Helping family members | 41.70% | - | - | - | |
| Having social opportunities | - | 50.00% | - | - | |
| Staying in communication with others | - | - | - | 33.3%). | |
| Support devices to: | [29] | ||||
| - Monitor rest and movements | 83.30% | 90.00% | 77.30% | 66.70% | |
| - Taking medications | 83.30% | 80.00% | 81.80% | 51.80% | |
| - Environmental conditions | 66.70% | 100.00% | 77.30% | 60.00% | |
| - Physical/cognitive impairment | 33.3%/41.7% | 90.0%/80.0% | 72.7%/77.3% | 86.7%/73.3% | |
| - Perform a Comprehensive Geriatric Assessment | - | - | 59.10% | 46.70% | |
| - Connect to care programs | - | 80.00% | - | 73.30% | |
| - Keep in touch with friends and family | 91.70% | 80.00% | 72.70% | 60.00% | |
| Impact of PHARA.On on: | [30] | ||||
| - Improving quality of life | 66.70% | 90.00% | 72.70% | 86.70% | |
| - Improving quality of care | 91.70% | 70.00% | 77.30% | 86.70% | |
| - Improving safety in daily living activities | 91.70% | 100.00% | 81.80% | 73.30% | |
| - Sending emergency alert/communication messages | 91.70% | 90.00% | 90.90% | 93.30% | |
| - Improving the assistance | 58.30% | 50.00% | 72.70% | 80.00% | |
| - Detecting when a person is lonely and isolated | 58.30% | 90.00% | 54.50% | 86.70% | |
| - Detecting changes in health status | 83.30% | 90.00% | 72.70% | 93.30% | |
| Need category | Specific needs | Priority level | Emotional goal | ||
| Users’ needs and priorities | Manage health | Stimulation | High | Involved | [33] |
| Monitoring | High | Reassured | [33] | ||
| Socialize | To promote social inclusion | High | Empowered | [31,32] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Onofrio, G.; Fiorini, L.; Toccafondi, L.; Rovini, E.; Russo, S.; Ciccone, F.; Giuliani, F.; Sancarlo, D.; Cavallo, F. Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs. Sensors 2022, 22, 163. https://doi.org/10.3390/s22010163
D’Onofrio G, Fiorini L, Toccafondi L, Rovini E, Russo S, Ciccone F, Giuliani F, Sancarlo D, Cavallo F. Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs. Sensors. 2022; 22(1):163. https://doi.org/10.3390/s22010163
Chicago/Turabian StyleD’Onofrio, Grazia, Laura Fiorini, Lara Toccafondi, Erika Rovini, Sergio Russo, Filomena Ciccone, Francesco Giuliani, Daniele Sancarlo, and Filippo Cavallo. 2022. "Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs" Sensors 22, no. 1: 163. https://doi.org/10.3390/s22010163