
Plantar Pressure Variability and Asymmetry in Elderly Performing 60-Minute Treadmill Brisk-Walking: Paving the Way towards Fatigue-Induced Instability Assessment Using Wearable In-Shoe Pressure Sensors


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
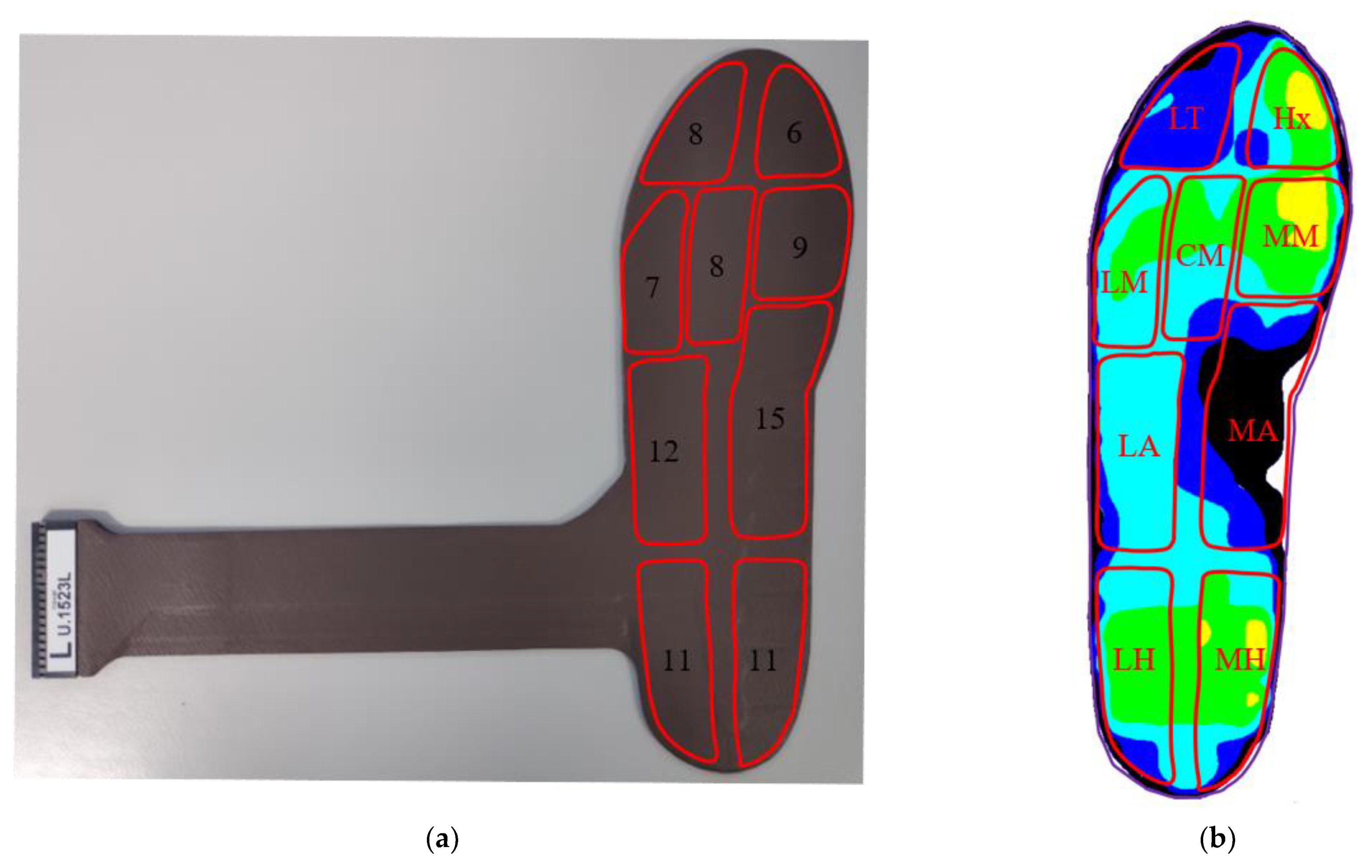
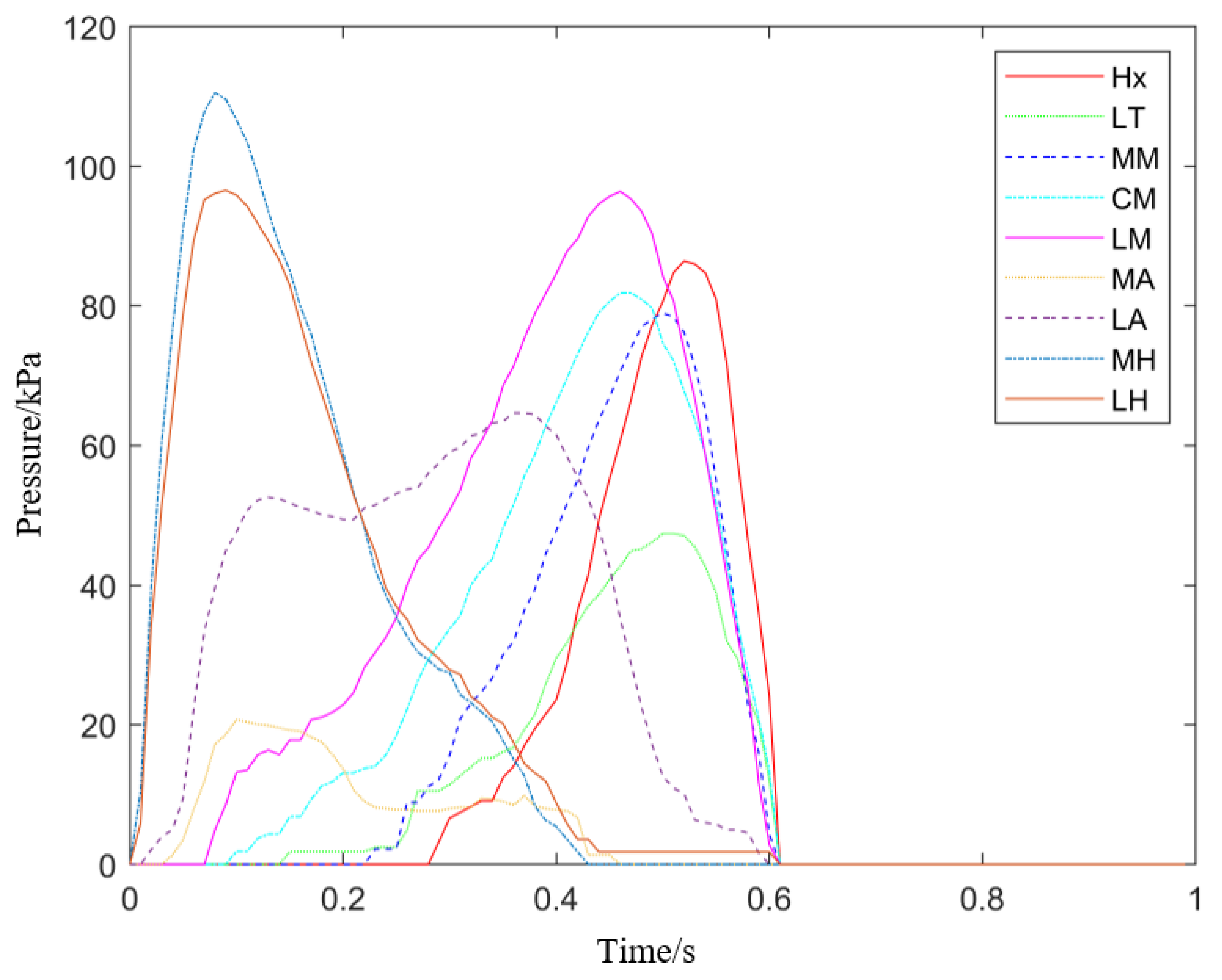
2.3. Data Processing
2.4. Statistical Analysis
3. Results
3.1. Contact Time, Maximum Pressure, and Impulse
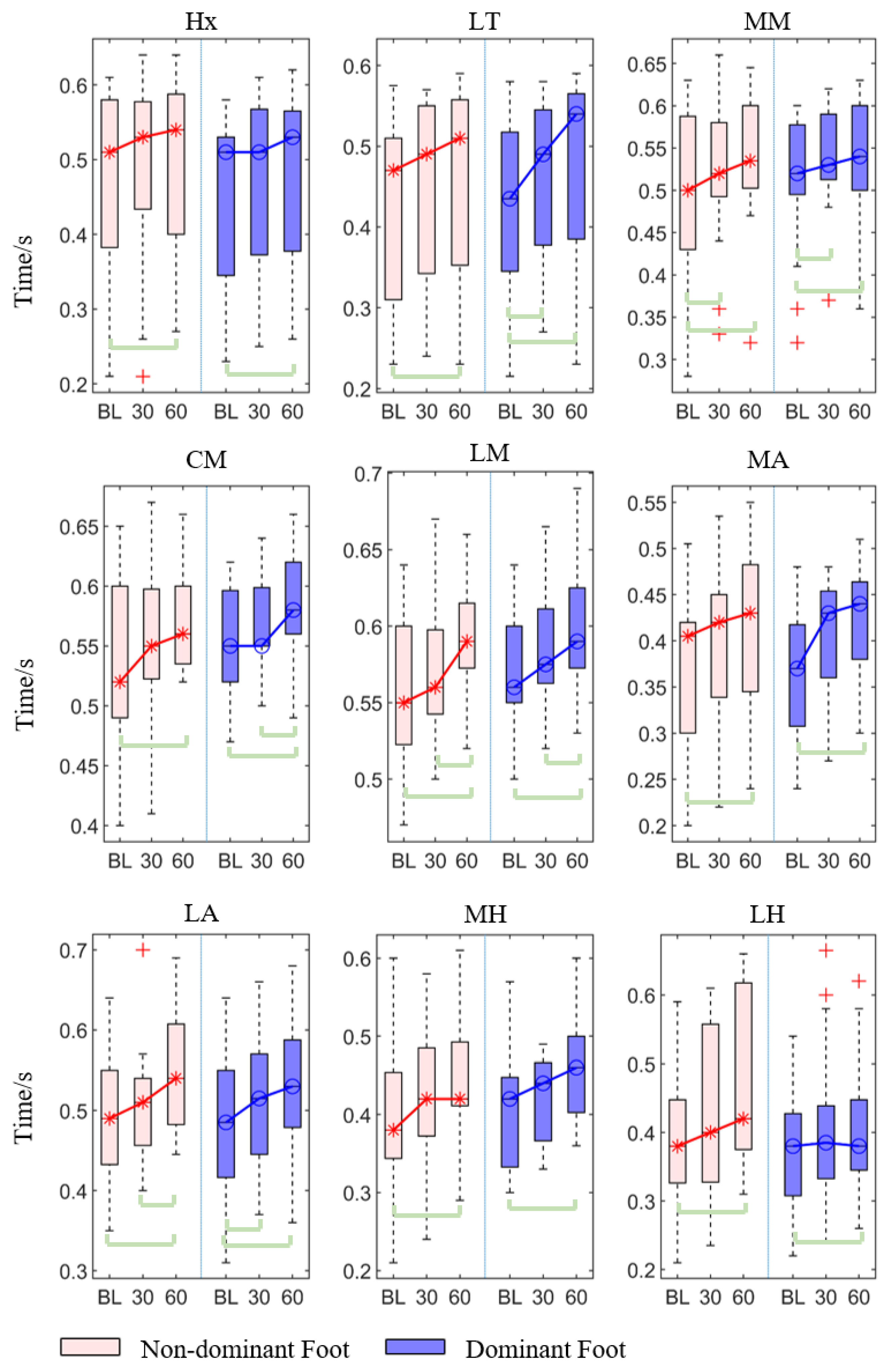
3.1.1. Contact Time
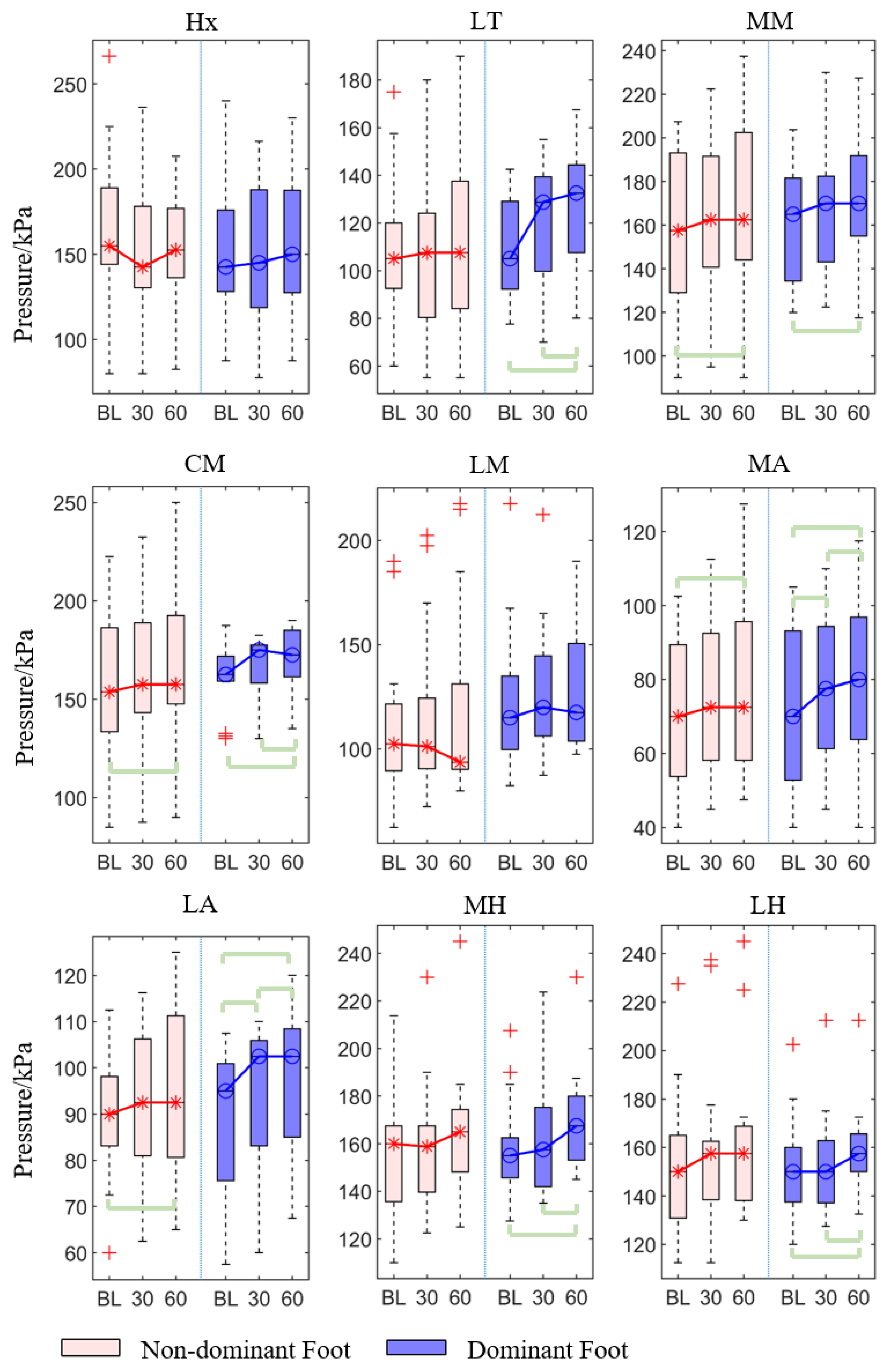
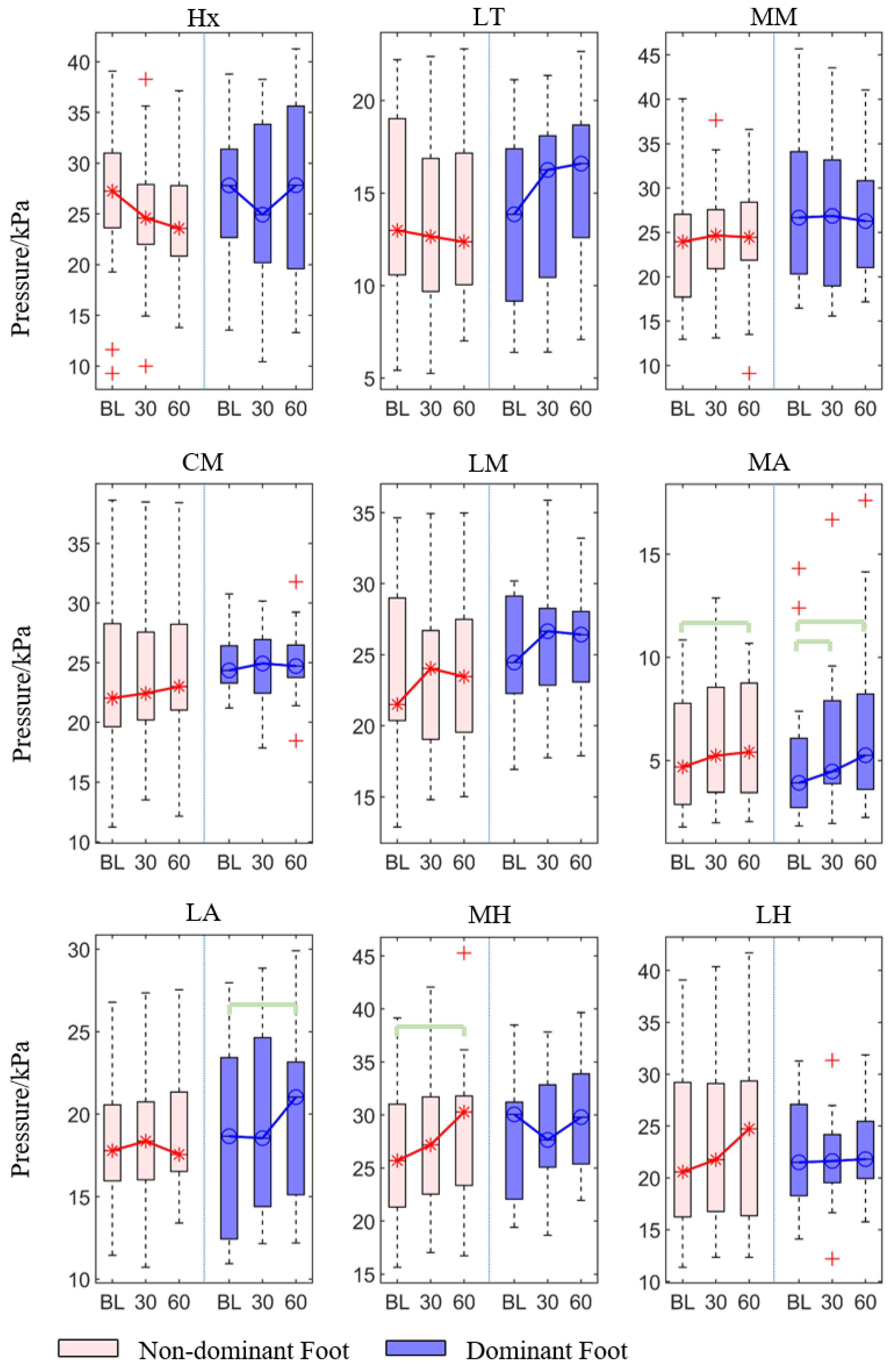
3.1.2. Peak Pressure
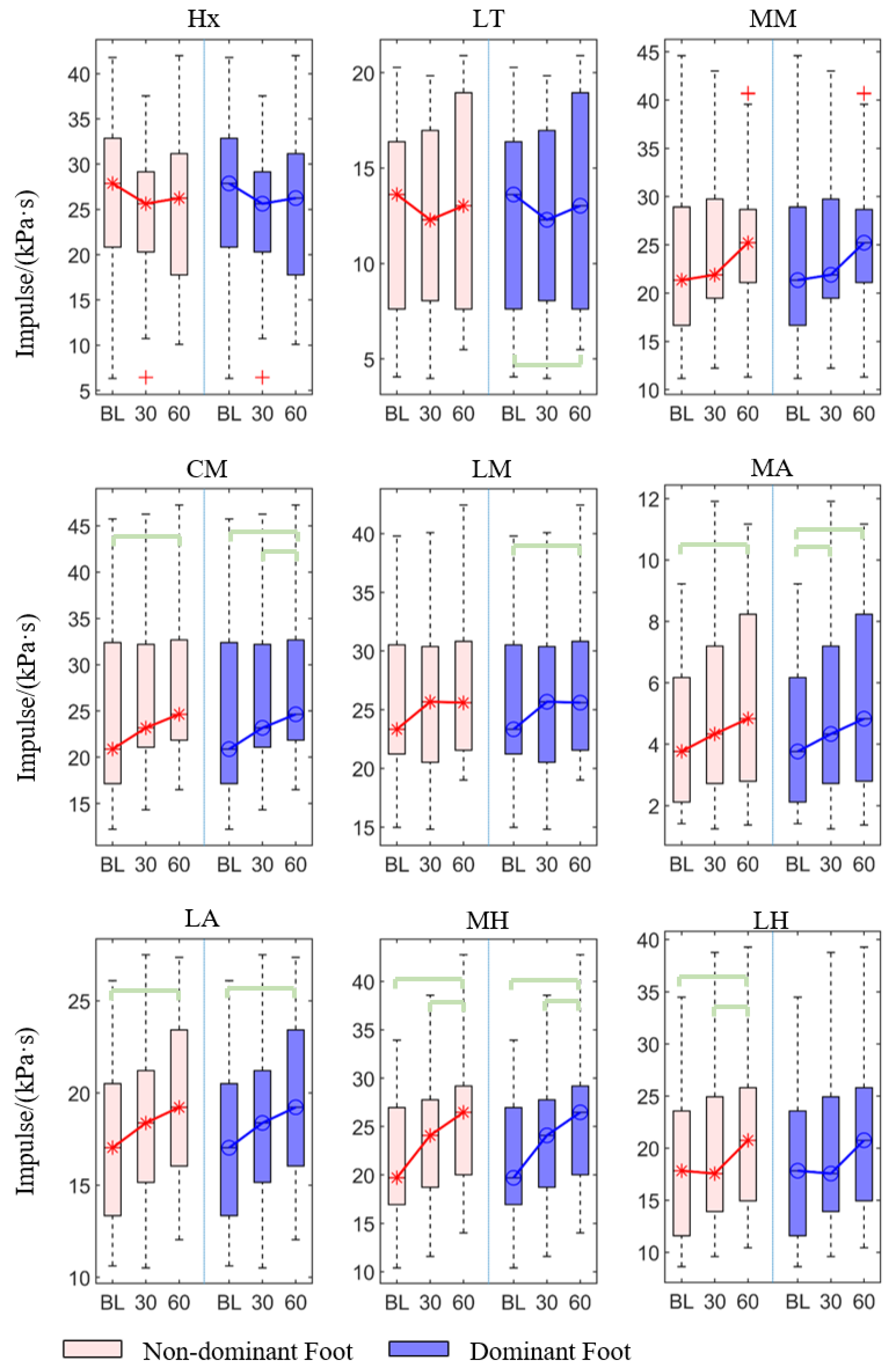
3.1.3. Impulse
3.2. Asymmetry Index and Variability
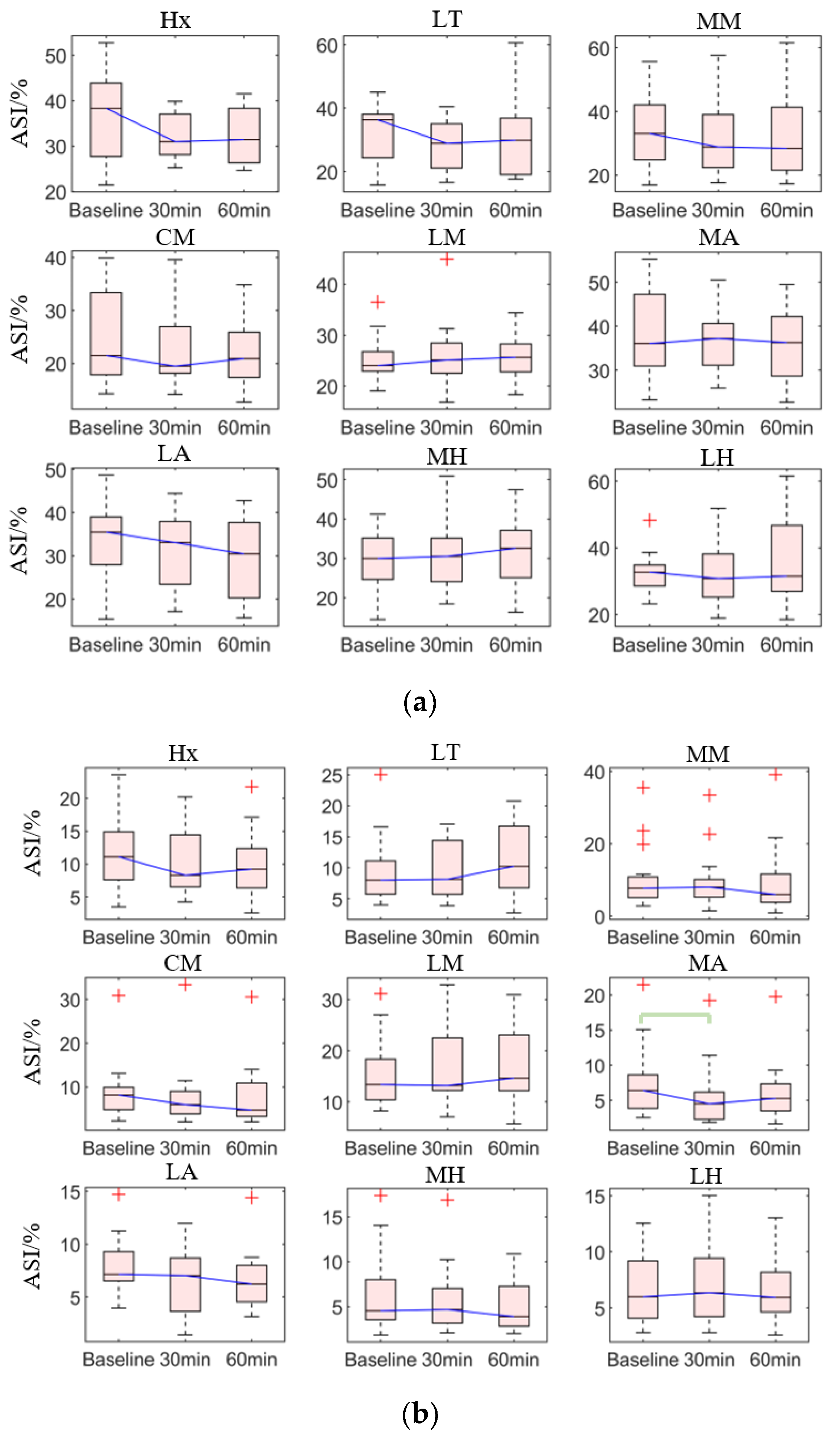
3.2.1. Asymmetry Index
3.2.2. Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Population Division of the United Nations Department of Economic and Social Affairs. World Population Ageing 2020 Highlights. Available online: https://www.un.org/development/desa/pd/news/world-population-ageing-2020-highlights (accessed on 20 January 2021).
- World Health Organization. Evidence and recommendations. In Integrated Care for Older People: Guidelines on Community-Level Interventions to Manage Declines in Intrinsic Capacity; World Health Organization: Geneva, Switzerland, 2017; p. 20. [Google Scholar]
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/dietphysicalactivity/global-PA-recs-2010.pdf (accessed on 20 January 2021).
- Mair, J.L.; De Vito, G.; Boreham, C.A. Low Volume, Home-Based Weighted Step Exercise Training Can Improve Lower Limb Muscle Power and Functional Ability in Community-Dwelling Older Women. J. Clin. Med. 2019, 8, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranyavalai, T.; Jalayondeja, C.; Jalayondeja, W.; Pichaiyongwongdee, S.; Kaewkungwal, J.; Laskin, J.J. Association between walking 5000 step/day and fall incidence over six months in urban community-dwelling older people. BMC Geriatr. 2020, 20, 194. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor-Locke, C.; Bassett, D.R. How many steps/day are enough? Sports Med. 2004, 34, 1–8. [Google Scholar] [CrossRef]
- Nagano, H.; James, L.; Sparrow, W.A.; Begg, R.K. Effects of walking-induced fatigue on gait function and tripping risks in older adults. J. Neuroeng. Rehabil. 2014, 11, 155. [Google Scholar] [CrossRef] [Green Version]
- Tirosh, O.; Sparrow, W. Age and walking speed effects on muscle recruitment in gait termination. Gait Posture 2005, 21, 279–288. [Google Scholar] [CrossRef]
- Barbieri, F.A.; Dos Santos, P.C.R.; Lirani-Silva, E.; Vitório, R.; Gobbi, L.T.B.; Van Diëen, J.H. Systematic review of the effects of fatigue on spatiotemporal gait parameters. J. Back Musculoskelet. Rehabil. 2013, 26, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Dayakidis, M.K.; Boudolos, K. Ground reaction force data in functional ankle instability during two cutting movements. Clin. Biomech. 2006, 21, 405–411. [Google Scholar] [CrossRef]
- Wong, D.W.-C.; Lam, W.-K.; Lee, W.C.-C. Gait asymmetry and variability in older adults during long-distance walking: Implications for gait instability. Clin. Biomech. 2019, 72, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Schütte, K.H.; Maas, E.A.; Exadaktylos, V.; Berckmans, D.; Venter, R.E.; Vanwanseele, B. Wireless Tri-Axial Trunk Accelerometry Detects Deviations in Dynamic Center of Mass Motion Due to Running-Induced Fatigue. PLoS ONE 2015, 10, e0141957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamacher, D.; Singh, N.; Van Dieën, J.; Heller, M.; Taylor, W. Kinematic measures for assessing gait stability in elderly individuals: A systematic review. J. R. Soc. Interface 2011, 8, 1682–1698. [Google Scholar] [CrossRef] [PubMed]
- Willson, J.D.; Kernozek, T.W. Plantar loading and cadence alterations with fatigue. Med. Sci. Sports Exerc. 1999, 31, 1828. [Google Scholar] [CrossRef] [PubMed]
- Barak, Y.; Wagenaar, R.C.; Holt, K.G. Gait Characteristics of Elderly People with a History of Falls: A Dynamic Approach. Phys. Ther. 2006, 86, 1501–1510. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Helbostad, J.L.; Moe-Nilssen, R.; Zijlstra, W.; Aminian, K. Does walking strategy in older people change as a function of walking distance? Gait Posture 2009, 29, 261–266. [Google Scholar] [CrossRef] [PubMed]
- England, S.A.; Granata, K.P. The influence of gait speed on local dynamic stability of walking. Gait Posture 2007, 25, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Greene, B.R.; McGrath, D.; Walsh, L.; Doheny, E.P.; McKeown, D.; Garattini, C.; Cunningham, C.; Crosby, L.; Caulfield, B.; Kenny, R.A. Quantitative falls risk estimation through multi-sensor assessment of standing balance. Physiol. Meas. 2012, 33, 2049–2063. [Google Scholar] [CrossRef]
- Elhadi, M.M.O.; Ma, C.Z.-H.; Wong, D.W.C.; Wan, A.H.P.; Lee, W.C.C. Comprehensive Gait Analysis of Healthy Older Adults Who Have Undergone Long-Distance Walking. J. Aging Phys. Act. 2017, 25, 367–377. [Google Scholar] [CrossRef]
- Ribeiro, F.; Mota, J.; Oliveira, J. Effect of exercise-induced fatigue on position sense of the knee in the elderly. Eur. J. Appl. Physiol. 2007, 99, 379–385. [Google Scholar] [CrossRef]
- Begg, R.K.; Palaniswami, M.; Owen, B. Support Vector Machines for Automated Gait Classification. IEEE Trans. Biomed. Eng. 2005, 52, 828–838. [Google Scholar] [CrossRef] [PubMed]
- Nagano, H.; Begg, R.K.; Sparrow, W.A.; Taylor, S. Ageing and limb dominance effects on foot-ground clearance during treadmill and overground walking. Clin. Biomech. 2011, 26, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R.; Mills, P.; Begg, R. A systematic review of the effect of ageing and falls history on minimum foot clearance characteristics during level walking. Gait Posture 2010, 32, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Wong, I.K.-K.; Chen, T.L.-W.; Hong, T.T.-H.; Wong, D.W.-C.; Peng, Y.; Yan, F.; Wang, Y.; Tan, Q.; Zhang, M. Identifying Fatigue Indicators Using Gait Variability Measures: A Longitudinal Study on Elderly Brisk Walking. Sensors 2020, 20, 6983. [Google Scholar] [CrossRef]
- Zhang, J.; Lockhart, T.E.; Soangra, R. Classifying Lower Extremity Muscle Fatigue During Walking Using Machine Learning and Inertial Sensors. Ann. Biomed. Eng. 2014, 42, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.-H.; Lin, C.-B.; Chen, Y.; Chen, W.; Huang, T.-S.; Hsu, C.-Y. An EMG Patch for the Real-Time Monitoring of Muscle-Fatigue Conditions during Exercise. Sensors 2019, 19, 3108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weist, R.; Eils, E.; Rosenbaum, D. The influence of muscle fatigue on electromyogram and plantar pressure patterns as an explanation for the incidence of metatarsal stress fractures. Am. J. Sports Med. 2004, 32, 1893–1898. [Google Scholar] [CrossRef]
- Valldecabres, R.; Richards, J.; De Benito, A.-M. The effect of match fatigue in elite badminton players using plantar pressure measurements and the implications to injury mechanisms. Sports Biomech. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, J.A.; Pérez-Soriano, P.; Llana, S.; Martínez-Nova, A.; Sánchez-Zuriaga, D. Effect of overground vs. treadmill running on plantar pressure: Influence of fatigue. Gait Posture 2013, 38, 929–933. [Google Scholar] [CrossRef]
- Bisiaux, M.; Moretto, P. The effects of fatigue on plantar pressure distribution in walking. Gait Posture 2008, 28, 693–698. [Google Scholar] [CrossRef]
- Sawacha, Z.; Guarneri, G.; Cristoferi, G.; Guiotto, A.; Avogaro, A.; Cobelli, C. Integrated kinematics–kinetics–plantar pressure data analysis: A useful tool for characterizing diabetic foot biomechanics. Gait Posture 2012, 36, 20–26. [Google Scholar] [CrossRef]
- Van Emmerik, R.E.; Miller, R.H.; Hamill, J. Dynamical Systems Analysis of Coordination. Res. Methods Biomech. 2014, 291–315. [Google Scholar] [CrossRef]
- Wafai, L.; Zayegh, A.; Woulfe, J.; Aziz, S.M.; Begg, R. Identification of Foot Pathologies Based on Plantar Pressure Asymmetry. Sensors 2015, 15, 20392–20408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.L.-W.; Wong, D.W.-C.; Wang, Y.; Tan, Q.; Lam, W.-K.; Zhang, M. Changes in segment coordination variability and the impacts of the lower limb across running mileages in half marathons: Implications for running injuries. J. Sport Health Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Buldt, A.K.; Allan, J.J.; Landorf, K.B.; Menz, H.B. The relationship between foot posture and plantar pressure during walking in adults: A systematic review. Gait Posture 2018, 62, 56–67. [Google Scholar] [CrossRef]
- Kemozek, T.; Zimmer, K. Reliability and Running Speed Effects of In-shoe Loading Measurements during Slow Treadmill Running. Foot Ankle Int. 2000, 21, 749–752. [Google Scholar] [CrossRef]
- Seeley, M.K.; Umberger, B.R.; Shapiro, R. A test of the functional asymmetry hypothesis in walking. Gait Posture 2008, 28, 24–28. [Google Scholar] [CrossRef]
- de Oliveira, C.F.; Soares, D.P.; Bertani, M.C.; Machado, L.J.R.; Vila-Boas, J.P. Effects of Fast-Walking on Muscle Activation in Young Adults and Elderly Persons. J. Nov. Physiother. Rehabil. 2017, 1, 012–019. [Google Scholar] [CrossRef] [Green Version]
- Mickelborough, J.; van der Linden, M.; Richards, J.; Ennos, A. Validity and reliability of a kinematic protocol for determining foot contact events. Gait Posture 2000, 11, 32–37. [Google Scholar] [CrossRef]
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; van Dieen, J.H. Assessing the stability of human locomotion: A review of current measures. J. R. Soc. Interface 2013, 10, 20120999. [Google Scholar] [CrossRef]
- Carpes, F.P.; Mota, C.B.; Faria, I.E. On the bilateral asymmetry during running and cycling—A review considering leg preference. Phys. Ther. Sport 2010, 11, 136–142. [Google Scholar] [CrossRef]
- Voloshin, A.S.; Mizrahi, J.; Verbitsky, O.; Isakov, E. Dynamic loading on the human musculoskeletal system—Effect of fatigue. Clin. Biomech. 1998, 13, 515–520. [Google Scholar] [CrossRef]
- Stolwijk, N.M.; Duysens, J.; Louwerens, J.W.K.; Keijsers, N.L.W. Plantar Pressure Changes after Long-Distance Walking. Med. Sci. Sports Exerc. 2010, 42, 2264–2272. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.W.; Lam, W.K.; Yeung, L.F.; Lee, W.C. Does long-distance walking improve or deteriorate walking stability of transtibial amputees? Clin. Biomech. 2015, 30, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Arndt, A.; Ekenman, I.; Westblad, P.; Lundberg, A. Effects of fatigue and load variation on metatarsal deformation measured in vivo during barefoot walking. J. Biomech. 2002, 35, 621–628. [Google Scholar] [CrossRef]
- Yeung, L.; Leung, A.K.; Zhang, M.; Lee, W.C. Long-distance walking effects on trans-tibial amputees compensatory gait patterns and implications on prosthetic designs and training. Gait Posture 2012, 35, 328–333. [Google Scholar] [CrossRef]
- Paterson, K.; Hill, K.; Lythgo, N. Stride dynamics, gait variability and prospective falls risk in active community dwelling older women. Gait Posture 2011, 33, 251–255. [Google Scholar] [CrossRef]
- Maki, B.E. Gait Changes in Older Adults: Predictors of Falls or Indicators of Fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef]
- Bruijn, S.M.; Bregman, D.J.; Meijer, O.G.; Beek, P.J.; van Dieën, J.H. Maximum Lyapunov exponents as predictors of global gait stability: A modelling approach. Med. Eng. Phys. 2012, 34, 428–436. [Google Scholar] [CrossRef]
- Finsterer, J.; Mahjoub, S.Z. Fatigue in Healthy and Diseased Individuals. Am. J. Hosp. Palliat. Med. 2014, 31, 562–575. [Google Scholar] [CrossRef]
- VanZant, R.S.; McPoil, T.G.; Cornwall, M.W. Symmetry of Plantar Pressures and Vertical Forces in Healthy Subjects during Walking. J. Am. Podiatr. Med. Assoc. 2001, 91, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Watt, J.R.; Franz, J.R.; Jackson, K.; Dicharry, J.; Riley, P.O.; Kerrigan, D.C. A three-dimensional kinematic and kinetic comparison of overground and treadmill walking in healthy elderly subjects. Clin. Biomech. 2010, 25, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Tan, Q.; Wang, Y.; Chen, T.L.-W.; Wong, D.W.-C.; Yan, F.; Li, Z.; Zhang, M. Exercise-Induced Hemodynamic Changes in Muscle Tissue: Implication of Muscle Fatigue. Appl. Sci. 2020, 10, 3512. [Google Scholar] [CrossRef]
- Rogers, A.; Morrison, S.C.; Gorst, T.; Paton, J.; Freeman, J.; Marsden, J.; Cramp, M.C. Repeatability of plantar pressure assessment during barefoot walking in people with stroke. J. Foot Ankle Res. 2020, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Franco, P.S.; da Silva, C.B.P.; da Rocha, E.S.; Carpes, F.P. Variability and repeatability analysis of plantar pressure during gait in older people. Rev. Bras. Reumatol. 2015, 55, 427–433. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Wan, A.H.-P.; Wong, D.W.-C.; Zheng, Y.-P.; Lee, W.C.-C. A Vibrotactile and Plantar Force Measurement-Based Biofeedback System: Paving the Way towards Wearable Balance-Improving Devices. Sensors 2015, 15, 31709–31722. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Hx | LT | MM | CM | LM | MA | LA | MH | LH |
|---|---|---|---|---|---|---|---|---|---|
| CTN | 0.001 * | 0.021 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.007 * |
| CTD | 0.023 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.002 * | 0.022 * |
| PPN | 0.437 | 0.492 | 0.003 * | 0.001 * | 0.252 | 0.001 * | 0.015 * | 0.061 | 0.148 |
| PPD | 0.402 | <0.001 * | 0.030 * | <0.001 * | 0.074 | <0.001 * | <0.001 * | 0.001 * | 0.003 * |
| IMN | 0.42 | 0.247 | 0.344 | 0.015 * | 0.155 | 0.001 * | 0.001 * | <0.001 * | 0.006 * |
| IMD | 0.074 | <0.001 * | 0.127 | <0.001 * | 0.002 * | <0.001 * | 0.001 * | <0.001 * | 0.038 * |
| ASIap | 0.074 | 0.549 | 0.549 | 0.420 | 0.420 | 0.420 | 0.627 | 0.449 | 0.247 |
| ASIpp | 0.282 | 0.344 | 0.282 | 0.074 | 0.282 | 0.008 * | 0.038 * | 0.766 | 0.247 |
| MADavg,N | 0.127 | 0.344 | 0.819 | 0.42 | 0.449 | 0.005 * | 0.038 * | 0.005 * | 0.057 |
| MADavg,D | 0.819 | 0.189 | 0.189 | 0.936 | 0.091 | <0.001 * | 0.015 * | 0.038 * | 0.155 |
| Variables | Regions | Baseline-30th min | Baseline-60th min | 30–60th min | |||
|---|---|---|---|---|---|---|---|
| p | p (Adjusted) | p | p (Adjusted) | p | p (Adjusted) | ||
| CTN | Hx | 0.075 | 0.225 | <0.001 | <0.001 * | 0.039 | 0.118 |
| LT | 0.519 | 1.000 | 0.008 | 0.023 * | 0.043 | 0.129 | |
| MM | 0.002 | 0.007 * | <0.001 | <0.001 * | 0.098 | 0.293 | |
| CM | 0.033 | 0.098 | <0.001 | <0.001 * | 0.016 | 0.047 * | |
| LM | 0.223 | 0.670 | <0.001 | <0.001 * | 0.009 | 0.026 * | |
| MA | 0.028 | 0.085 | <0.001 | <0.001 * | 0.028 | 0.085 | |
| LA | 0.043 | 0.129 | <0.001 | <0.001 * | 0.004 | 0.013 * | |
| MH | 0.053 | 0.160 | <0.001 | <0.001 * | 0.027 | 0.081 | |
| LH | 0.118 | 0.353 | 0.002 | 0.005 * | 0.118 | 0.353 | |
| CTD | Hx | 0.645 | 1.000 | 0.010 | 0.030 * | 0.034 | 0.103 |
| LT | 0.012 | 0.037 * | <0.001 | <0.001 * | 0.164 | 0.491 | |
| MM | 0.011 | 0.032 * | <0.001 | <0.001 * | 0.144 | 0.432 | |
| CM | 0.053 | 0.160 | <0.001 | <0.001 * | 0.013 | 0.039 * | |
| LM | 0.080 | 0.241 | <0.001 | <0.001 * | 0.004 | 0.013 * | |
| MA | 0.028 | 0.085 | <0.001 | <0.001 * | 0.028 | 0.085 | |
| LA | 0.010 | 0.030 * | <0.001 | <0.001 * | 0.021 | 0.064 | |
| MH | 0.144 | 0.432 | 0.001 | 0.002 * | 0.045 | 0.134 | |
| LH | 0.273 | 0.820 | 0.006 | 0.019 * | 0.100 | 0.301 | |
| PPN | MM | 0.162 | 0.485 | 0.001 | 0.002 * | 0.046 | 0.137 |
| CM | 0.089 | 0.267 | <0.001 | 0.001 * | 0.047 | 0.142 | |
| MA | 0.032 | 0.096 | <0.001 | 0.001 * | 0.126 | 0.377 | |
| LA | 0.190 | 0.569 | 0.004 | 0.011 * | 0.111 | 0.334 | |
| PPD | LT | 0.095 | 0.284 | <0.001 | <0.001 * | 0.002 | 0.007 * |
| MM | 0.083 | 0.250 | 0.009 | 0.028 * | 0.386 | 1.000 | |
| CM | 0.239 | 0.718 | <0.001 | <0.001 * | 0.008 | 0.024 * | |
| MA | 0.005 | 0.016 * | <0.001 | <0.001 * | 0.054 | 0.163 | |
| LA | 0.014 | 0.043 * | <0.001 | <0.001 * | 0.014 | 0.043 * | |
| MH | 0.773 | 1.000 | 0.001 | 0.002 * | 0.001 | 0.004 * | |
| LH | 0.437 | 1.000 | 0.001 | 0.003 * | 0.012 | 0.035 * | |
| IMN | CM | 0.584 | 1.000 | 0.006 | 0.019 * | 0.028 | 0.085 |
| MA | 0.100 | 0.301 | <0.001 | <0.001 * | 0.028 | 0.085 | |
| LA | 0.068 | 0.204 | <0.001 | 0.001 * | 0.068 | 0.204 | |
| MH | 0.201 | 0.604 | <0.001 | <0.001 * | 0.003 | 0.010 * | |
| LH | 0.715 | 1.000 | 0.003 | 0.010 * | 0.011 | 0.032 * | |
| IMD | LT | 0.028 | 0.085 | <0.001 | <0.001 * | 0.028 | 0.085 |
| CM | 0.584 | 1.000 | <0.001 | <0.001 * | 0.001 | 0.003 * | |
| LM | 0.045 | 0.134 | 0.001 | 0.002 * | 0.144 | 0.432 | |
| MA | 0.006 | 0.019 * | <0.001 | <0.001 * | 0.028 | 0.085 | |
| LA | 0.018 | 0.053 | <0.001 | 0.001 * | 0.201 | 0.604 | |
| MH | 0.201 | 0.604 | <0.001 | <0.001 * | 0.003 | 0.010 * | |
| LH | 0.715 | 1.000 | 0.045 | 0.134 | 0.018 | 0.053 | |
| Variables | Regions | Baseline-30th min | Baseline-60th min | 30–60th min | |||
|---|---|---|---|---|---|---|---|
| p | p (Adjusted) | p | p (Adjusted) | p | p (Adjusted) | ||
| ASIpp | MA | 0.002 | 0.006 * | 0.201 | 0.604 | 0.068 | 0.204 |
| LA | 0.018 | 0.053 | 0.045 | 0.134 | 0.715 | 1.000 | |
| MADavg,N | MA | 0.100 | 0.301 | 0.001 | 0.003 * | 0.100 | 0.301 |
| LA | 0.045 | 0.134 | 0.018 | 0.053 | 0.715 | 1.000 | |
| MH | 0.018 | 0.053 | 0.002 | 0.006 * | 0.465 | 1.000 | |
| MADavg,D | MA | 0.006 | 0.019 * | <0.001 | <0.001 * | 0.100 | 0.301 |
| LA | 0.028 | 0.085 | 0.006 | 0.019 * | 0.584 | 1.000 | |
| MH | 0.715 | 1.000 | 0.018 | 0.053 | 0.045 | 0.134 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, G.; Wong, D.W.-C.; Wong, I.K.-K.; Chen, T.L.-W.; Hong, T.T.-H.; Peng, Y.; Wang, Y.; Tan, Q.; Zhang, M. Plantar Pressure Variability and Asymmetry in Elderly Performing 60-Minute Treadmill Brisk-Walking: Paving the Way towards Fatigue-Induced Instability Assessment Using Wearable In-Shoe Pressure Sensors. Sensors 2021, 21, 3217. https://doi.org/10.3390/s21093217
Zhang G, Wong DW-C, Wong IK-K, Chen TL-W, Hong TT-H, Peng Y, Wang Y, Tan Q, Zhang M. Plantar Pressure Variability and Asymmetry in Elderly Performing 60-Minute Treadmill Brisk-Walking: Paving the Way towards Fatigue-Induced Instability Assessment Using Wearable In-Shoe Pressure Sensors. Sensors. 2021; 21(9):3217. https://doi.org/10.3390/s21093217
Chicago/Turabian StyleZhang, Guoxin, Duo Wai-Chi Wong, Ivy Kwan-Kei Wong, Tony Lin-Wei Chen, Tommy Tung-Ho Hong, Yinghu Peng, Yan Wang, Qitao Tan, and Ming Zhang. 2021. "Plantar Pressure Variability and Asymmetry in Elderly Performing 60-Minute Treadmill Brisk-Walking: Paving the Way towards Fatigue-Induced Instability Assessment Using Wearable In-Shoe Pressure Sensors" Sensors 21, no. 9: 3217. https://doi.org/10.3390/s21093217