Mobile Computing Technologies for Health and Mobility Assessment: Research Design and Results of the Timed Up and Go Test in Older Adults

 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
1.1. Background
1.2. Motivation
1.3. Prior Work
1.4. Structure of the Study
2. Methods
2.1. Study Design and Participants
2.2. Description of the Timed-Up and Go Test and Data Acquisition and Processing
2.3. Statistical Analysis
3. Results
3.1. Data Acquisition with a Mobile Application
3.2. Requirements
3.3. Comparison of Different Acquired Data
- The minimum value or amount of the magnitude of the vector of the accelerometer, calculated after the reaction time;
- The minimum absolute value of the z-axis of the magnetometer, calculated after the reaction time.
- Pressure sensor: reaction time, whole test time;
- Magnetometer: total acquisition time, turning around instant by the magnitude of the vector, turning around moment by the absolute value of z-axis;
- Accelerometer: reaction time, total test time, duration of turning around, going time, return time, the average acceleration during going time, the average acceleration during return time, the average velocity during going time, the average speed during return time, the average force during going time, the average force during return time, the average power during going time, the average power during return time;
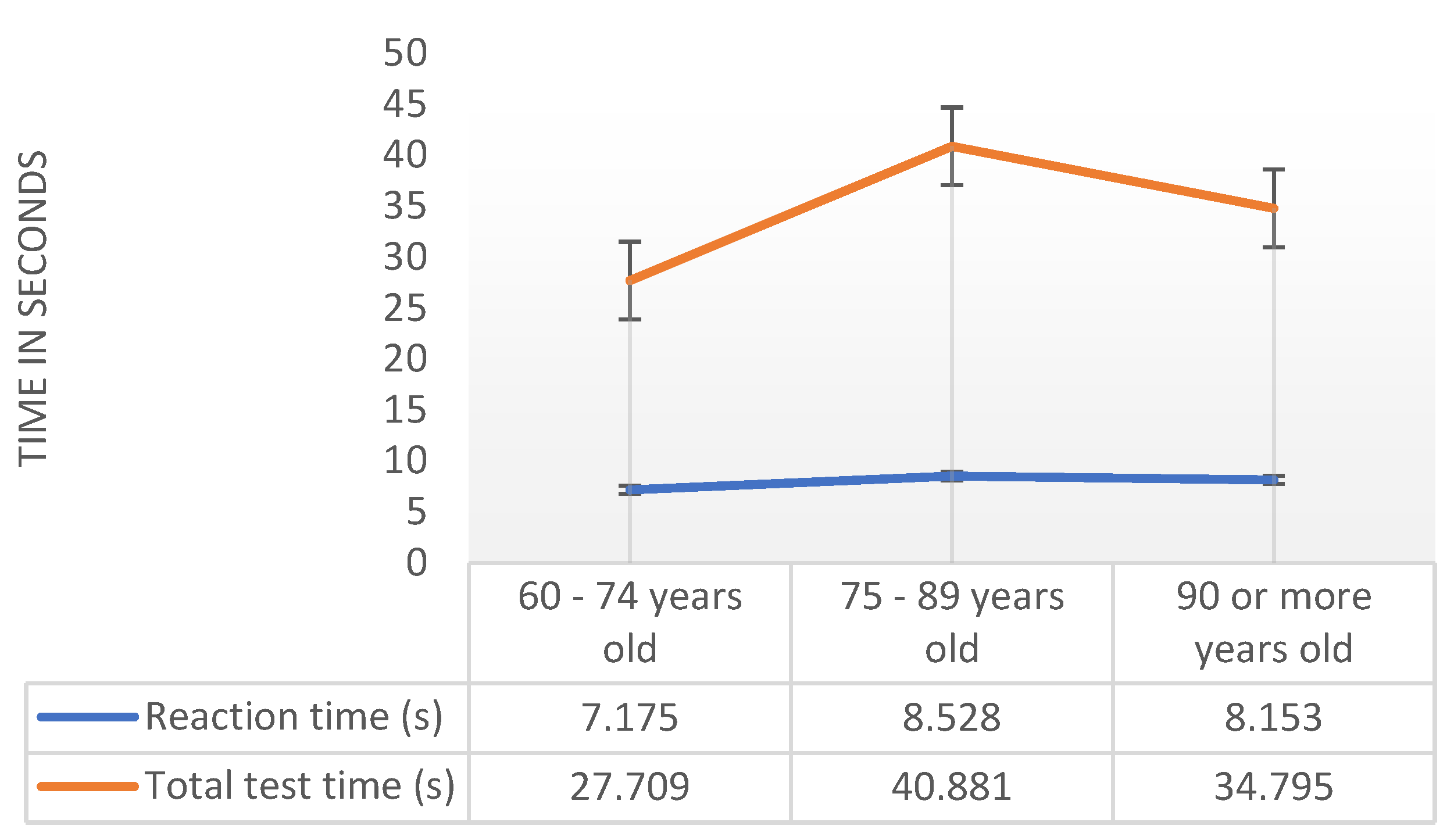
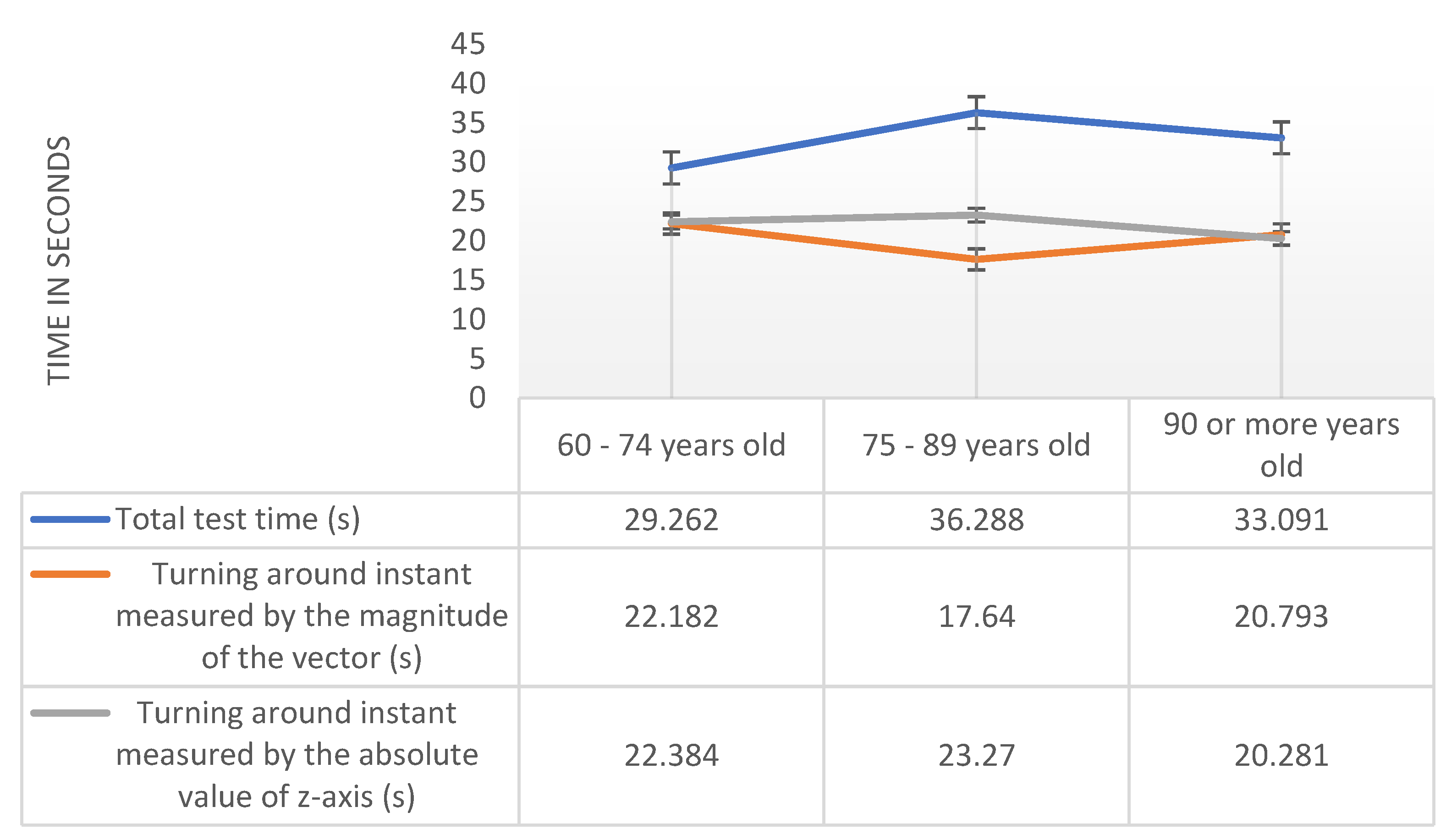
3.3.1. Results by Age
3.3.2. Results by Institution
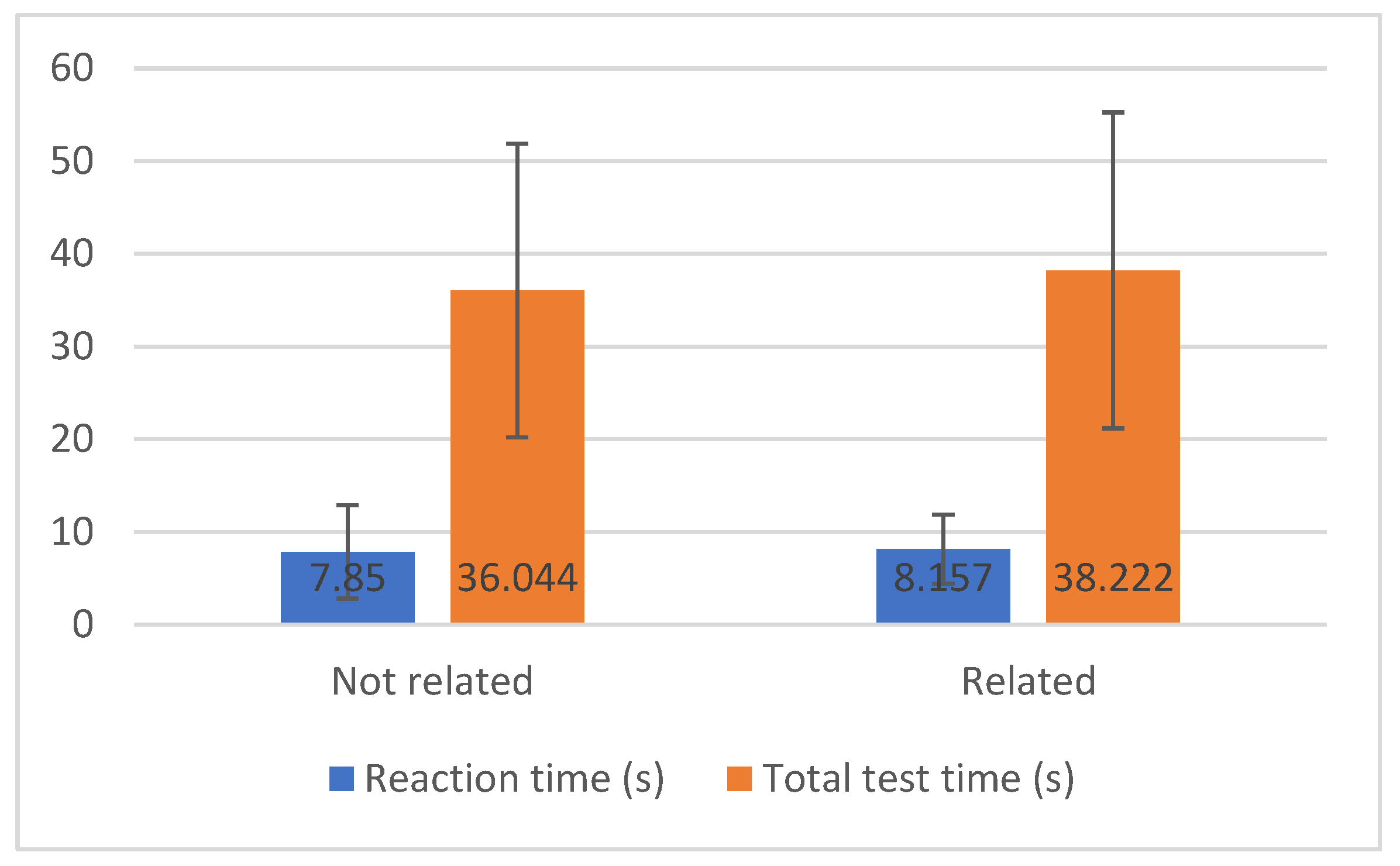
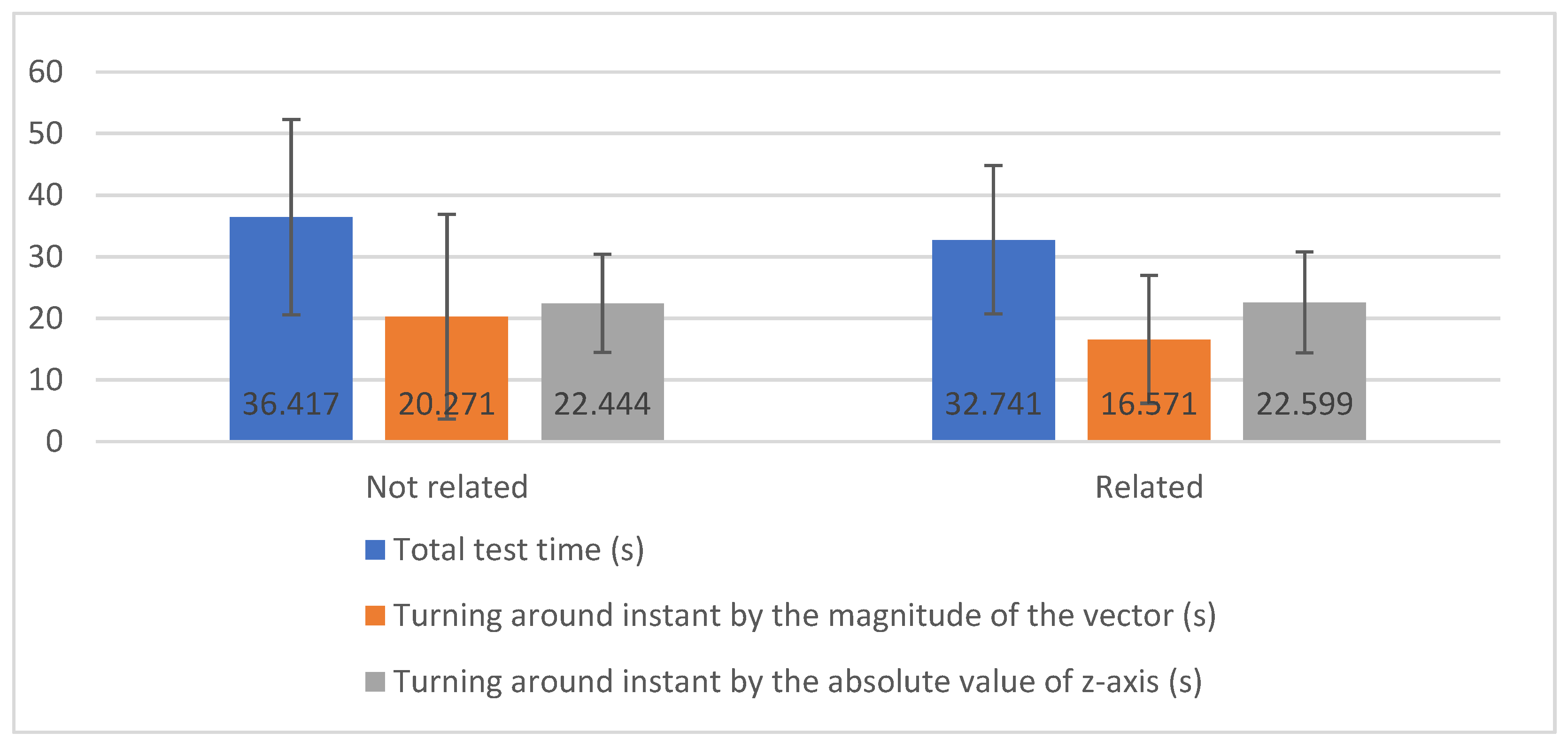
3.3.3. Results by Disease
- The total test time (s) has homogeneous variances between the groups of diseases not related and related to mobility (Pr (F > F-test) = 0.459 > 0.05), and the average is statistically equal (Pr (|T| > t-test = 0.490 > 0.05);
- The turning around instant by the magnitude of the vector (s) has non-homogeneous variances between the groups of diseases not related and related to mobility (Pr (F > F-test) = 0.029 < 0.05), but the average is statistically equal (Pr (|T| > t-test = 0.642 > 0.05);
- The turning around instant by the absolute value of the z-axis (s) has homogeneous variances between the groups of diseases not related and related to mobility (Pr (F > F-test = 0.628 > 0.05), and the average is statistically equal (Pr (|T| > t-test = 0.961 > 0.05).
4. Discussion
4.1. Main Findings
4.2. Limitations
4.3. Comparison with Prior Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Studies | Number of Studies |
|---|---|---|
| Duration of the test | [17,32,49,51,52,54,55,58] | 8 |
| Maximum | [17,45,56,57,58] | 5 |
| Mean | [46,49,54,56,58] | 5 |
| Duration of each stage | [17,47,50,51,56] | 5 |
| Root Mean Square (RMS) | [45,46,56,58] | 4 |
| Standard deviation | [45,46,56,58] | 4 |
| Velocity | [32,44] | 2 |
| Time of sit-to-stand transition | [44,48] | 2 |
| Minimum | [45,57] | 2 |
| Energy | [45,46] | 2 |
| Entropy | [45,46] | 2 |
| Mobility angles | [32,48] | 2 |
| Time of stand-to-sit | [53,55] | 2 |
| Time of prepare-to-sit | [53,55] | 2 |
| Time of sit-down | [53,55] | 2 |
| Time of lift-up | [53,55] | 2 |
| Maximum change of the trunk angle | [51,55] | 2 |
| Maximum angular velocity during the lean forward and lift-up phases | [51,55] | 2 |
| Median deviation | [45] | 1 |
| Skewness | [45] | 1 |
| Interquartile range (IQR) | [45] | 1 |
| Kurtosis | [45] | 1 |
| Maximum and second maximum frequencies and amplitudes of the Fast Fourier Transform (FFT) | [45] | 1 |
| Number of times that the amplitude of the magnitude of the vector of accelerometer signal crosses the mean value | [45] | 1 |
| Mean of peak height | [45] | 1 |
| Correlation | [46] | 1 |
| Pitch | [46] | 1 |
| Signal Magnitude Area (SMA) | [46] | 1 |
| Signal Vector Magnitude (SVM) | [46] | 1 |
| Angular velocity of the mobility of the arm | [50] | 1 |
| Time to perform turn-to-sit | [50] | 1 |
| Time of lean forward phase | [53] | 1 |
| Time of the walking phase | [53] | 1 |
| Maximum angular velocities during lean forward and lift-up phases | [53] | 1 |
| Maximum change of trunk angle during the lean forward phase | [53] | 1 |
| Total number of steps during the walking phase and before the turn | [53] | 1 |
| Stride length | [32] | 1 |
| Distance traveled | [32] | 1 |
| Length of the lean forward period | [55] | 1 |
| Number of steps during | [55] | 1 |
| Coefficient of variation | [56] | 1 |
| Jerk | [58] | 1 |
| Institution | Person ID | Diseases | Diseases Related to Mobility | Age (Years) | Test Conditions |
|---|---|---|---|---|---|
| Centro Comunitário das Lameiras | 1 | Arthrosis | Yes | 85 | Chair without supports. Spacious place. Floor with the right conditions. Good mobile network coverage. A physical therapist monitored the test. |
| Centro Comunitário das Lameiras | 2 | Gastroenteritis | No | 92 | |
| Centro Comunitário das Lameiras | 3 | Arterial hypertension; Arthrosis | Yes | 85 | |
| Centro Comunitário das Lameiras | 4 | Arterial hypertension; Cardiac arrhythmia | No | 92 | |
| Centro Comunitário das Lameiras | 5 | Arterial hypertension; Cardiac arrhythmia; Diabetes mellitus Type II; Scoliosis | Yes | 92 | |
| Centro Comunitário das Lameiras | 6 | Scoliosis | Yes | 85 | |
| Centro Comunitário das Lameiras | 7 | Osteoporosis | Yes | 83 | |
| Centro Comunitário das Lameiras | 8 | Arthrosis | Yes | 87 | |
| Others | 9 | Scoliosis | Yes | 60 | Excellent quality of mobile network coverage. Tight space in the kitchen. Chair with supports. |
| Others | 10 | Right leg amputation; Diabetes mellitus Type II | Yes | 77 | |
| Lar Aldeia de Joanes | 11 | N/D | - | N/D | Weak mobile network coverage. Test site with the right physical conditions. The test was carried out in a place with other older adults. Chair with supports. |
| Lar Minas | 12 | Arterial hypertension | No | 88 | Mobile network coverage does not exist. Test site with Good physical condition of the test site. The test was carried out in a living room with other older adults. Chair with supports. |
| Lar Minas | 13 | Arterial hypertension; Cardiac arrhythmia; Arteriosclerotic coronary disease; Heart failure | No | 84 | |
| Lar Minas | 14 | N/D | - | 65 | |
| Lar da Misericórdia | 15 | N/D | - | 91 | The basement of a building with little mobile network coverage. Chair with supports. Flat ground with a slight slope. |
| Lar da Misericórdia | 16 | N/D | - | 84 | |
| Lar da Misericórdia | 17 | Hernioplasty in 2010; Sarcoidosis | No | 87 | |
| Lar da Misericórdia | 18 | Chronic obstructive pulmonary disease; Chronic bronchitis; Osteoarthritis | Yes | 73 | |
| Lar da Misericórdia | 19 | Cirrhosis; Anemia; Chronic kidney disease; Umbilical hernia; Inguinal hernia | Yes | 79 | |
| Lar da Misericórdia | 20 | Right leg amputation; Umbilical hernia; Arterial hypertension | Yes | 88 | |
| Lar da Misericórdia | 21 | Prostate Cancer; Parkinson’s disease; Post-traumatic stress | Yes | 76 | |
| Lar da Misericórdia | 22 | Arterial hypertension; Diabetes mellitus Type II | No | 86 | |
| Lar da Misericórdia | 23 | Prostate Cancer; Osteoporosis; Chronic Venous Insufficiency of the lower limbs; Chronic bronchitis | Yes | 92 | |
| Lar da Misericórdia | 24 | Diabetes mellitus Type II; Arterial hypertension; Depression; Sequelae of surgery to brain injury | No | 83 | |
| Lar da Misericórdia | 25 | Diabetes mellitus Type II; Vertigo syndrome; Chronic headaches; Osteoarthritis; Prosthesis in the right humeral; Osteoporosis; Arterial hypertension | Yes | 81 | |
| Lar da Misericórdia | 26 | Arterial hypertension; Anemia | No | 91 | |
| Lar da Misericórdia | 27 | Osteoarthritis; Depression; Heart failure; Arterial hypertension; Osteoporosis | Yes | 89 | |
| Lar da Misericórdia | 28 | N/D | - | N/D | |
| Lar da Nossa Senhora de Fátima | 29 | Diabetes mellitus Type II; | No | 86 | The test location was narrow. The mobile network coverage was of good quality. The floor and width of the test site were very tight. The chair had no supports. |
| Lar da nossa senhora de Fátima | 30 | Dementia of vascular etiology; Prostate Cancer; Arterial hypertension; Vertigo syndrome | Yes | N/D | |
| Lar da nossa senhora de Fátima | 31 | Depression; Osteoporosis | Yes | 83 | |
| Lar da Nossa Senhora de Fátima | 32 | Diabetes mellitus Type II; Osteoarthritis | Yes | 87 | |
| Lar da Nossa Senhora de Fátima | 33 | Diabetes mellitus Type II; Arterial hypertension; Heart failure; Hyperuricemia; Depression; Bilateral gonarthrosis | Yes | N/D | |
| Lar da nossa senhora de Fátima | 34 | Prostate cancer | No | 88 | |
| Lar da Nossa Senhora de Fátima | 35 | Heart failure; Chronic obstructive pulmonary disease; Bilateral gonarthrosis | Yes | 97 | |
| Lar da nossa senhora de Fátima | 36 | Diabetes mellitus Type II; Arterial hypertension | No | 71 | |
| Lar da nossa senhora de Fátima | 37 | Arterial hypertension | No | 74 | |
| Lar da Nossa Senhora de Fátima | 38 | Osteoarthritis; Lumbar hernias; Depression; Gastric ulcer | Yes | 82 | |
| Lar da Nossa Senhora de Fátima | 39 | Heart failure; Arterial hypertension; Pulmonary fibrosis; Hyperuricemia; Anemia; Chronic kidney disease; Cardiac arrhythmia; Acute myocardial infarction; Hypocoagulated | Yes | N/D | |
| Lar da nossa senhora de Fátima | 40 | Chronic kidney disease | No | 90 |
References
- Marques, G.; Pitarma, R.; Garcia, N.M.; Pombo, N. Internet of Things Architectures, Technologies, Applications, Challenges, and Future Directions for Enhanced Living Environments and Healthcare Systems: A Review. Electronics 2019, 8, 1081. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 27 December 2019).
- United Nations, Dept. of Economic and Social Affairs. World Population Ageing, 1950–2050; United Nations Publications: Herndon, VA, USA, 2002. [Google Scholar]
- Portugal é o sexto país mais envelhecido do mundo. Available online: https://www.publico.pt/2013/11/08/sociedade/noticia/portugal-e-o-sexto-pais-mais-envelhecido-do-mundo-1611852 (accessed on 27 December 2019).
- Blackman, S.; Matlo, C.; Bobrovitskiy, C.; Waldoch, A.; Fang, M.L.; Jackson, P.; Mihailidis, A.; Nygård, L.; Astell, A.; Sixsmith, A. Ambient Assisted Living Technologies for Aging Well: A Scoping Review. J. Intell. Syst. 2015, 25, 55–69. [Google Scholar] [CrossRef]
- Majumder, S.; Deen, M.J. Smartphone Sensors for Health Monitoring and Diagnosis. Sensors 2019, 19, 2164. [Google Scholar] [CrossRef] [Green Version]
- Kakria, P.; Tripathi, N.K.; Kitipawang, P. A Real-Time Health Monitoring System for Remote Cardiac Patients Using Smartphone and Wearable Sensors. Int. J. Telemed. Appl. 2015, 2015, 373474. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P. Smartphone Applications for Patients’ Health and Fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Ben-Zeev, D.; Scherer, E.A.; Wang, R.; Xie, H.; Campbell, A.T. Next-generation psychiatric assessment: Using smartphone sensors to monitor behavior and mental health. Psychiatr. Rehabil. J. 2015, 38, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Gautschi, O.P.; Stienen, M.N.; Corniola, M.V.; Joswig, H.; Schaller, K.; Hildebrandt, G.; Smoll, N.R. Assessment of the Minimum Clinically Important Difference in the Timed Up and Go Test After Surgery for Lumbar Degenerative Disc Disease. Neurosurgery 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Whitney, J.C.; Lord, S.R.; Close, J.C.T. Streamlining assessment and intervention in a falls clinic using the Timed Up and Go Test and Physiological Profile Assessments. Age Ageing 2005, 34, 567–571. [Google Scholar] [CrossRef] [Green Version]
- Marques, G. Ambient Assisted Living and Internet of Things. In Harnessing the Internet of Everything (IoE) for Accelerated Innovation Opportunities; Cardoso, P.J.S., Monteiro, J., Semião, J., Rodrigues, J.M.F., Eds.; IGI Global: Hershey, PA, USA, 2019; pp. 100–115. ISBN 978-1-5225-7332-6. [Google Scholar]
- Haghi, M.; Thurow, K.; Stoll, R. Wearable Devices in Medical Internet of Things: Scientific Research and Commercially Available Devices. Healthc. Inform. Res. 2017, 23, 4. [Google Scholar] [CrossRef]
- Andrews, R.G. Mobile Sensor Data Measurements and Analysis for Fall Detection in Elderly Health Care; Aalto University: Espoo, Finland, 2017; Available online: http://urn.fi/URN:NBN:fi:aalto-201712187878 (accessed on 27 December 2019).
- Guo, J.; Zhou, X.; Sun, Y.; Ping, G.; Zhao, G.; Li, Z. Smartphone-Based Patients’ Activity Recognition by Using a Self-Learning Scheme for Medical Monitoring. J. Med. Syst. 2016, 40, 140. [Google Scholar] [CrossRef]
- Dziak, D.; Jachimczyk, B.; Kulesza, W. IoT-Based Information System for Healthcare Application: Design Methodology Approach. Appl. Sci. 2017, 7, 596. [Google Scholar] [CrossRef]
- Mellone, S.; Tacconi, C.; Schwickert, L.; Klenk, J.; Becker, C.; Chiari, L. Smartphone-based solutions for fall detection and prevention: The FARSEEING approach. Z. Gerontol. Geriatr. 2012, 45, 722–727. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F.; Spinsante, S.; Teixeira, M.C.; Zdravevski, E. Recognition of Activities of Daily Living and Environments Using Acoustic Sensors Embedded on Mobile Devices. Electronics 2019, 8, 1499. [Google Scholar] [CrossRef] [Green Version]
- Zdravevski, E.; Lameski, P.; Trajkovik, V.; Kulakov, A.; Chorbev, I.; Goleva, R.; Pombo, N.M. Garcia Improving Activity Recognition Accuracy in Ambient-Assisted Living Systems by Automated Feature Engineering. IEEE Access 2017, 5, 5262–5280. [Google Scholar] [CrossRef]
- Pires, I.M.; Teixeira, M.C.; Pombo, N.; Garcia, N.M.; Flórez-Revuelta, F.; Spinsante, S.; Goleva, R.; Zdravevski, E. Android Library for Recognition of Activities of Daily Living: Implementation Considerations, Challenges, and Solutions. Open Bioinform. J. 2018, 11, 61–88. [Google Scholar] [CrossRef] [Green Version]
- Pires, I.M.; Pombo, N.; Garcia, N.M.; Flórez-Revuelta, F. Multi-Sensor Mobile Platform for the Recognition of Activities of Daily Living and their Environments based on Artificial Neural Networks. In Proceedings of the Twenty-Seventh International Joint Conference on Artificial Intelligence ${$IJCAI-18$}$, Stockholm, Sweden, 13–19 July 2018. [Google Scholar]
- Pires, I.M.; Andrade, M.; Garcia, N.M.; Crisóstomo, R.; Florez-Revuelta, F. Measurement of heel-rise test results using a mobile device. In Proceedings of the Doctoral Consortium—DCPhyCS, (PhyCS 2015), Angers, France, 11–13 February 2015; SciTePress (INSTICC): Angers, France, 2015; pp. 9–18. [Google Scholar]
- Herman, T.; Giladi, N.; Hausdorff, J.M. Properties of the ‘Timed Up and Go’ Test: More than Meets the Eye. Gerontology 2011, 57, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Kotagal, V.; Albin, R.L.; Muller, M.L.T.M.; Koeppe, R.A.; Studenski, S.; Frey, K.A.; Bohnen, N.I. Advanced Age, Cardiovascular Risk Burden, and Timed Up and Go Test Performance in Parkinson Disease. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1569–1575. [Google Scholar] [CrossRef] [Green Version]
- Montes, J.; Cheng, B.; Diamond, B.; Doorish, C.; Mitsumoto, H.; Gordon, P.H. The Timed Up and Go test: Predicting falls in ALS. Amyotroph. Lateral Scler. 2007, 8, 292–295. [Google Scholar] [CrossRef]
- Joshua, A.M.; Karnad, S.D.; Nayak, A.; Suresh, B.V.; Mithra, P.; Unnikrishnan, B. Effect of foot placements during sit to stand transition on timed up and go test in stroke subjects: A cross sectional study. NeuroRehabilitation 2017, 40, 355–362. [Google Scholar] [CrossRef]
- Givens, D.L.; Eskildsen, S.; Taylor, K.E.; Faldowski, R.A.; Del Gaizo, D.J. Timed Up and Go test is predictive of Patient-Reported Outcomes Measurement Information System physical function in patients awaiting total knee arthroplasty. Arthroplast. Today 2018, 4, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Son, K.Y.; Shin, D.W.; Lee, J.E.; Kim, S.H.; Yun, J.M.; Cho, B. Association of timed up and go test outcomes with future incidence of cardiovascular disease and mortality in adults aged 66 years: Korean national representative longitudinal study over 5.7 years. BMC Geriatr. 2020, 20, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vervoort, D.; Vuillerme, N.; Kosse, N.; Hortobágyi, T.; Lamoth, C.J.C. Multivariate Analyses and Classification of Inertial Sensor Data to Identify Aging Effects on the Timed-Up-and-Go Test. PLoS ONE 2016, 11, e0155984. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Li, X.; Sangaiah, A.K.; Xu, L.; Kumari, S.; Wu, L.; Shen, J. A lightweight and robust two-factor authentication scheme for personalized healthcare systems using wireless medical sensor networks. Future Gener. Comput. Syst. 2018, 82, 727–737. [Google Scholar] [CrossRef]
- Jagadeeswari, V.; Subramaniyaswamy, V.; Logesh, R.; Vijayakumar, V. A study on medical Internet of Things and Big Data in personalized healthcare system. Health Inf. Sci. Syst. 2018, 6, 14. [Google Scholar] [CrossRef]
- Williams, B.; Allen, B.; True, H.; Fell, N.; Levine, D.; Sartipi, M. A real-time, mobile timed up and go system. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–6. [Google Scholar]
- McGough, E.L.; Kelly, V.E.; Logsdon, R.G.; McCurry, S.M.; Cochrane, B.B.; Engel, J.M.; Teri, L. Associations Between Physical Performance and Executive Function in Older Adults With Mild Cognitive Impairment: Gait Speed and the Timed “Up & Go” Test. Phys. Ther. 2011, 91, 1198–1207. [Google Scholar] [CrossRef]
- Kwan, M.M.-S.; Lin, S.-I.; Chen, C.-H.; Close, J.C.T.; Lord, S.R. Sensorimotor function, balance abilities and pain influence Timed Up and Go performance in older community-living people. Aging Clin. Exp. Res. 2011, 23, 196–201. [Google Scholar] [CrossRef]
- Hui, E.; Chui, B.T.; Woo, J. Effects of dance on physical and psychological well-being in older persons. Arch. Gerontol. Geriatr. 2009, 49, e45–e50. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.; Todd, K.; Aitchison, T.C.; Kelly, P.; Stoddart, D. The effects of a 12-week group exercise programme on physiological and psychological variables and function in overweight women. Public Health 2004, 118, 31–42. [Google Scholar] [CrossRef]
- Tiedemann, A.; Sherrington, C.; Lord, S.R. Physiological and Psychological Predictors of Walking Speed in Older Community-Dwelling People. Gerontology 2005, 51, 390–395. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Sebastião, E.; Sandroff, B.M.; Learmonth, Y.C.; Motl, R.W. Validity of the Timed Up and Go Test as a Measure of Functional Mobility in Persons With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2016, 97, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Pires, I.; Felizardo, V.; Pombo, N.; Garcia, N.M. Limitations of energy expenditure calculation based on a mobile phone accelerometer. In Proceedings of the 2017 International Conference on High Performance Computing & Simulation (HPCS), Genoa, Italy, 17–21 July 2017; pp. 124–127. [Google Scholar]
- Pires, I.M.; Garcia, N.M.; Pombo, N.; Flórez-Revuelta, F. Limitations of the Use of Mobile Devices and Smart Environments for the Monitoring of Ageing People. In Proceedings of the 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health; SCITEPRESS—Science and Technology Publications: Funchal, Madeira, Portugal, 22–23 April 2018; pp. 269–275. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N.; Spinsante, S.; Crisóstomo, R. Smartphone-based automatic measurement of the results of the Timed-Up and Go test. In Proceedings of the 5th EAI International Conference on Smart Objects and Technologies for Social Good, Valencia, Spain, 25–27 September 2019; pp. 239–242. [Google Scholar]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Garcia, N.M.; Pombo, N. Non-invasive measurement of results of timed-up and go test: Preliminary results. In Proceedings of the Ageing Congress 2019, Kuala Lumpur, Malaysia, 22–23 April 2019. [Google Scholar]
- Bao, T.; Carender, W.J.; Kinnaird, C.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Kabeto, M.; Seidler, R.D.; Sienko, K.H. Effects of long-term balance training with vibrotactile sensory augmentation among community-dwelling healthy older adults: A randomized preliminary study. J. NeuroEng. Rehabil. 2018, 15, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, J.; Sousa, I. Instrumented timed up and go: Fall risk assessment based on inertial wearable sensors. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016; IEEE: Benevento, Italy, 2016; pp. 1–6. [Google Scholar]
- Hellmers, S.; Izadpanah, B.; Dasenbrock, L.; Diekmann, R.; Bauer, J.; Hein, A.; Fudickar, S. Towards an Automated Unsupervised Mobility Assessment for Older People Based on Inertial TUG Measurements. Sensors 2018, 18, 3310. [Google Scholar] [CrossRef] [Green Version]
- Chigateri, N.G.; Kerse, N.; Wheeler, L.; MacDonald, B.; Klenk, J. Validation of an accelerometer for measurement of activity in frail older people. Gait Posture 2018, 66, 114–117. [Google Scholar] [CrossRef]
- Mellone, S.; Tacconi, C.; Chiari, L. Validity of a Smartphone-based instrumented Timed Up and Go. Gait Posture 2012, 36, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Beyea, J.; McGibbon, C.A.; Sexton, A.; Noble, J.; O’Connell, C. Convergent Validity of a Wearable Sensor System for Measuring Sub-Task Performance during the Timed Up-and-Go Test. Sensors 2017, 17, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salarian, A.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Aminian, K. iTUG, a Sensitive and Reliable Measure of Mobility. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milosevic, M.; Jovanov, E.; Milenkovic, A. Quantifying Timed-Up-and-Go test: A smartphone implementation. In Proceedings of the 2013 IEEE International Conference on Body Sensor Networks, Cambridge, MA, USA, 6–9 May 2013; pp. 1–6. [Google Scholar]
- Suppa, A.; Kita, A.; Leodori, G.; Zampogna, A.; Nicolini, E.; Lorenzi, P.; Rao, R.; Irrera, F. l-DOPA and Freezing of Gait in Parkinson’s Disease: Objective Assessment through a Wearable Wireless System. Front. Neurol. 2017, 8, 406. [Google Scholar] [CrossRef]
- Madhushri, P.; Dzhagaryan, A.A.; Jovanov, E.; Milenkovic, A. A Smartphone Application Suite for Assessing Mobility. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3117–3120. [Google Scholar]
- Galán-Mercant, A.; Cuesta-Vargas, A.I. Clinical frailty syndrome assessment using inertial sensors embedded in smartphones. Physiol. Meas. 2015, 36, 1929–1942. [Google Scholar] [CrossRef]
- Dzhagaryan, A.; Milenkovic, A.; Jovanov, E.; Milosevic, M. Smart Button: A wearable system for assessing mobility in elderly. In Proceedings of the 2015 17th International Conference on E-health Networking, Application & Services (HealthCom), Boston, MA, USA, 14–17 October 2015; pp. 416–421. [Google Scholar]
- Tacconi, C.; Mellone, S.; Chiari, L. Smartphone-Based Applications for Investigating Falls and Mobility. In Proceedings of the 5th International ICST Conference on Pervasive Computing Technologies for Healthcare, Dublin, Ireland, 23–26 May 2011. [Google Scholar]
- Galán-Mercant, A.; Cuesta-Vargas, A.I. Mobile Romberg test assessment (mRomberg). BMC Res. Notes 2014, 7, 640. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, L.; Mellone, S.; Rocchi, L.; Chiari, L. Dimensionality reduction for the quantitative evaluation of a smartphone-based Timed Up and Go test. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 7179–7182. [Google Scholar]
- Batista, D.; Silva, H.; Fred, A. Experimental characterization and analysis of the BITalino platforms against a reference device. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; IEEE: Seogwipo, Korea, 2017; pp. 2418–2421. [Google Scholar]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. (2000). Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2001, 80, 896–903. [Google Scholar] [CrossRef] [Green Version]
- Sow, M.T. Using ANOVA to Examine the Relationship between Safety & Security and Human Development. J. Int. Bus. Econ. 2014, 2. [Google Scholar] [CrossRef] [Green Version]
- Spitzner, D.J.; Marron, J.S.; Essick, G.K. Mixed-Model Functional ANOVA for Studying Human Tactile Perception. J. Am. Stat. Assoc. 2003, 98, 263–272. [Google Scholar] [CrossRef]
- Hafsteinsdóttir, T.B.; Rensink, M.; Schuurmans, M. Clinimetric Properties of the Timed Up and Go Test for Patients with Stroke: A Systematic Review. Top. Stroke Rehabil. 2014, 21, 197–210. [Google Scholar] [CrossRef] [Green Version]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S.; Sarkar, B. Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. 2018, 18, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprint, G.; Cook, D.J.; Weeks, D.L. Toward Automating Clinical Assessments: A Survey of the Timed Up and Go. IEEE Rev. Biomed. Eng. 2015, 8, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, R.A.; Williams, H.A.; Broberg, J.S.; Lanting, B.A.; McIsaac, K.A.; Teeter, M.G. Machine Learning Groups Patients by Early Functional Improvement Likelihood Based on Wearable Sensor Instrumented Preoperative Timed-Up-and-Go Tests. J. Arthroplast. 2019, 34, 2267–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Number of Occurrences | Related with Mobility | ||
|---|---|---|---|
| Osteoarticular diseases (Total of 17 individuals) | Arthrosis | 4 | Yes |
| Scoliosis | 2 | Yes | |
| Leg amputation | 2 | Yes | |
| Bilateral gonarthrosis | 2 | Yes | |
| Osteoarthritis | 4 | Yes | |
| Lumbar hernias | 1 | Yes | |
| Prosthesis in the right humeral | 1 | Yes | |
| Osteoporosis | 4 | Yes | |
| Cardiovascular diseases (Total of 18 individuals) | Arterial hypertension | 16 | No |
| Cardiac arrhythmia | 4 | No | |
| Arteriosclerotic coronary disease | 1 | No | |
| Heart failure | 5 | Yes | |
| Acute myocardial infarction | 1 | No | |
| Chronic Venous Insufficiency of the lower limbs | 1 | No | |
| Lung diseases (Total of four individuals) | Pulmonary fibrosis | 1 | No |
| Chronic obstructive pulmonary disease | 2 | Yes | |
| Chronic bronchitis | 2 | Yes | |
| Neurological and balance disease (Total of six individuals) | Parkinson | 3 | Yes |
| Dementia | 1 | Yes | |
| Chronic headaches | 1 | No | |
| Sequelae of surgery to brain injury | 1 | No | |
| Psychiatric illnesses (Total of six individuals) | Post-traumatic stress | 1 | No |
| Depression | 5 | No | |
| Nephro-urological disease (Total of nine individuals) | Hypocoagulated | 1 | No |
| Anemia | 3 | No | |
| Chronic kidney disease | 3 | No | |
| Prostate cancer | 4 | No | |
| Digestive system and abdominal wall disease (Total of three individuals) | Umbilical hernia | 2 | No |
| Inguinal hernia | 1 | Yes | |
| Cirrhosis | 1 | No | |
| Gastroenteritis | 1 | No | |
| Metabolic disorder (Total of 10 individuals) | Hyperuricemia | 2 | No |
| Diabetes mellitus Type II | 9 | No |
| Related to Mobility | Not Related to Mobility |
|---|---|
|
|
| Sensors | Parameters | Analysis | ||
|---|---|---|---|---|
| By Age | By Institution | By Diseases | ||
| Pressure sensor | Reaction time | - | It is higher in Lar Aldeia de Joanes and Lar Minas (14.860 s), and lower in Lar Nossa Senhora de Fátima (5.948 s) | It is higher in persons with sequelae of surgery to brain injury (16.830 s), and lower in persons with pulmonary fibrosis, acute myocardial infarction, and hypocoagulated (3.477 s) |
| Total test time | It is lower in an individual of 60-years-old with scoliosis (21.070 s) | - | It is higher in an individual with a leg amputation and diabetes mellitus Type II (92.950 s). | |
| Magnetometer sensor | Total test time | It is lower in an individual of 60-years-old with scoliosis (19.761 s) | It is lower in Centro Comunitário das Lameiras (28.778 s), and higher in institutions with poor conditions (74.053 s) | It is higher in people with osteoarticular pathology and a prosthesis in the right humeral (66.947 s), and lower in people with arthrosis (24.528 s) |
| Turnaround measured by the magnitude of the vector | The time is higher in an individual of 89-years-old with problems related to mobility (51.742 s) | The instant is lower in Lar da Misericórdia (2.591 s) | The instance is higher in people with congestive heart failure (28.886 s), and lower in people with osteoarticular pathology and prosthesis in the right humeral (3.836 s), and the time is higher in people with lumbar hernias and a gastric ulcer (30.643 s) | |
| Turning around instant measured by the absolute value of the z-axis | It is higher in participants with osteoarthritis of 87-years-old (39.649 s). | It is lower in Centro Comunitário das Lameiras (8.433 s), and it is higher in Lar Nossa Senhora de Fátima (39.649 s). | It is lower in people with osteoarticular pathology and a prosthesis in the right humeral (8.704 s), and it is higher in people with osteoarthritis (39.649 s) | |
| Accelerometer sensor | Times | Average of 10.521 s in reaction time, 45.538 s in total test time, 13.272 s in going time, and 21.944 s in return time | ||
| Turning around | In average, the duration is 0.436 s, and the instant is 23.566 s | |||
| Acceleration | Average of 9.96 m/s2 in going time, and −11.43 m/s2 in return time. | |||
| Velocity | Average of 15.12 m/s in going time, and −5.51 m/s in return time. | |||
| Force | Average of 713.37 N in going time, and −1886.03 N in return time. | |||
| Power | Average of 6233.21 J in going time, and −8491.09 J in return time. | |||
| Origin | Limitation |
|---|---|
| Individuals | Different health conditions. |
| Environment | The experiments were performed in uncontrolled environments. |
| Technical | The Internet connecting is needed for data synchronization. |
| Bluetooth connected reported some failures. | |
| A large volume of data needs to be processed in the mobile device. | |
| Data cannot be processed in real-time. | |
| Sometimes it was not possible to consistently synchronize the timestamps of the acquired data, because Bitalino does not have real timestamps. |
| Study | Differences Compared to Our Study | Advantages of Our Study |
|---|---|---|
| [45] | The study is related to the fall risk assessment, and our research is associated with the analysis of the performance of the Timed-Up and Go test for the creation of patterns by age, disease, and institution. | Our study proved that a relation between diseases related to mobility and the performance of the Timed-Up and Go test exists, allowing the creation of different patterns with the inertial sensors. |
| [49] | The study identified the different phases of Timed-Up and Go sensors. The authors also calculated the Minimal Detectable Change based on the speed, where we identified the various stages, and measured the force, power, and acceleration of the movement. | The older adults sometimes performed more force and power than the other population. The measurement of these parameters is vital to identify the reliability of the test in the different repetitions. |
| [32] | The study tracks the different stages of the Timed-Up and Go test, and the angles of the knee and ankle. Our study identified the different phases and made other measurements. | Our study is focused on older adults that commonly have different pathologies, performing different measurements and relationships between diseases. |
| [67] | The authors implemented machine learning methods for the distribution of the individuals in different groups to cluster the types of diseases. | Our study performed the analysis of the different features extracted with a focus on the diseases related to the movement. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Villasana, M.V.; Crisóstomo, R.; Canavarro Teixeira, M.; Zdravevski, E. Mobile Computing Technologies for Health and Mobility Assessment: Research Design and Results of the Timed Up and Go Test in Older Adults. Sensors 2020, 20, 3481. https://doi.org/10.3390/s20123481
Ponciano V, Pires IM, Ribeiro FR, Villasana MV, Crisóstomo R, Canavarro Teixeira M, Zdravevski E. Mobile Computing Technologies for Health and Mobility Assessment: Research Design and Results of the Timed Up and Go Test in Older Adults. Sensors. 2020; 20(12):3481. https://doi.org/10.3390/s20123481
Chicago/Turabian StylePonciano, Vasco, Ivan Miguel Pires, Fernando Reinaldo Ribeiro, María Vanessa Villasana, Rute Crisóstomo, Maria Canavarro Teixeira, and Eftim Zdravevski. 2020. "Mobile Computing Technologies for Health and Mobility Assessment: Research Design and Results of the Timed Up and Go Test in Older Adults" Sensors 20, no. 12: 3481. https://doi.org/10.3390/s20123481