Estimating Respiratory Rate in Post-Anesthesia Care Unit Patients Using Infrared Thermography: An Observational Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
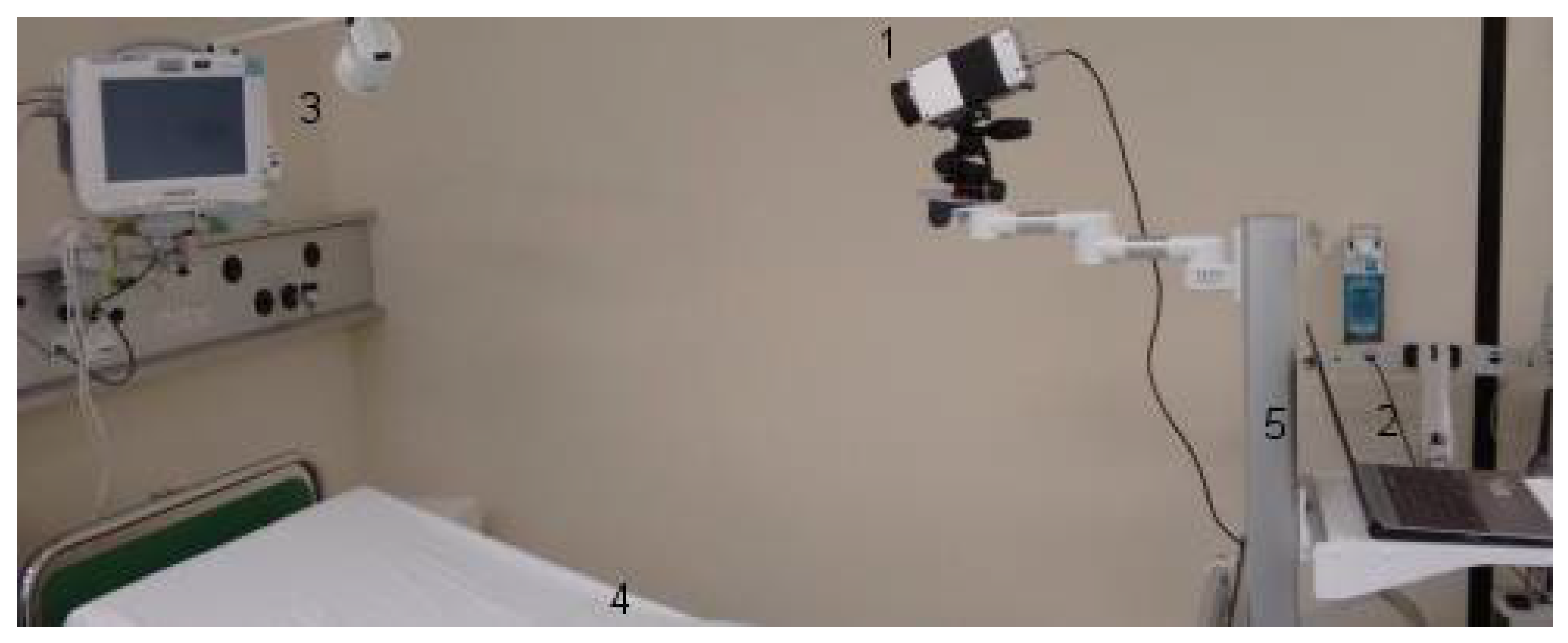
2.1. Study Design
2.2. Monitoring and Data Assessment
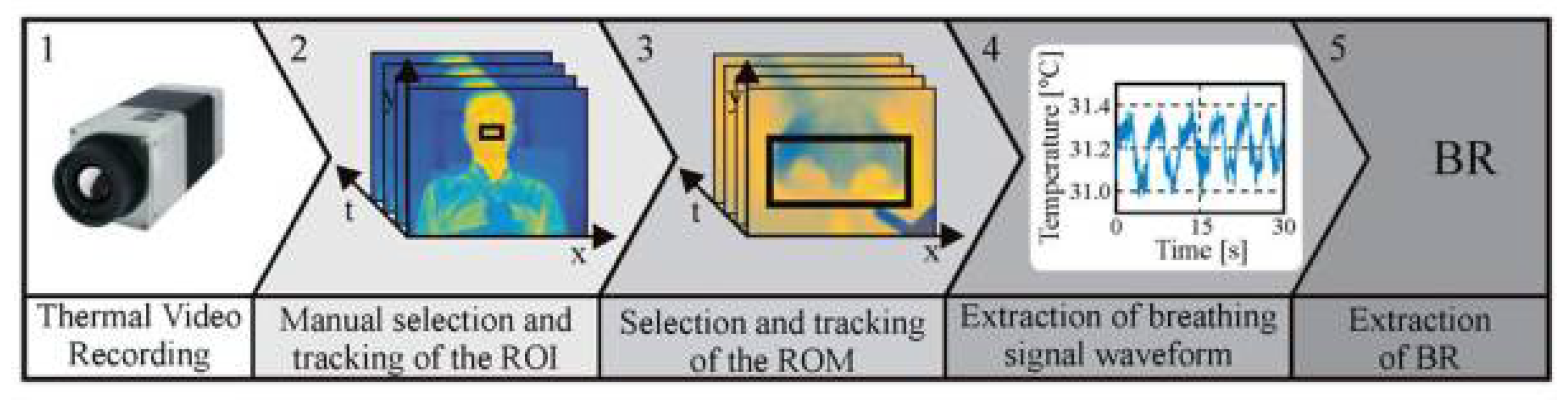
2.3. IRT Image Analysis
2.3.1. Region Selection and Tracking
2.3.2. Extraction of the Respiratory Waveform and Signal Processing
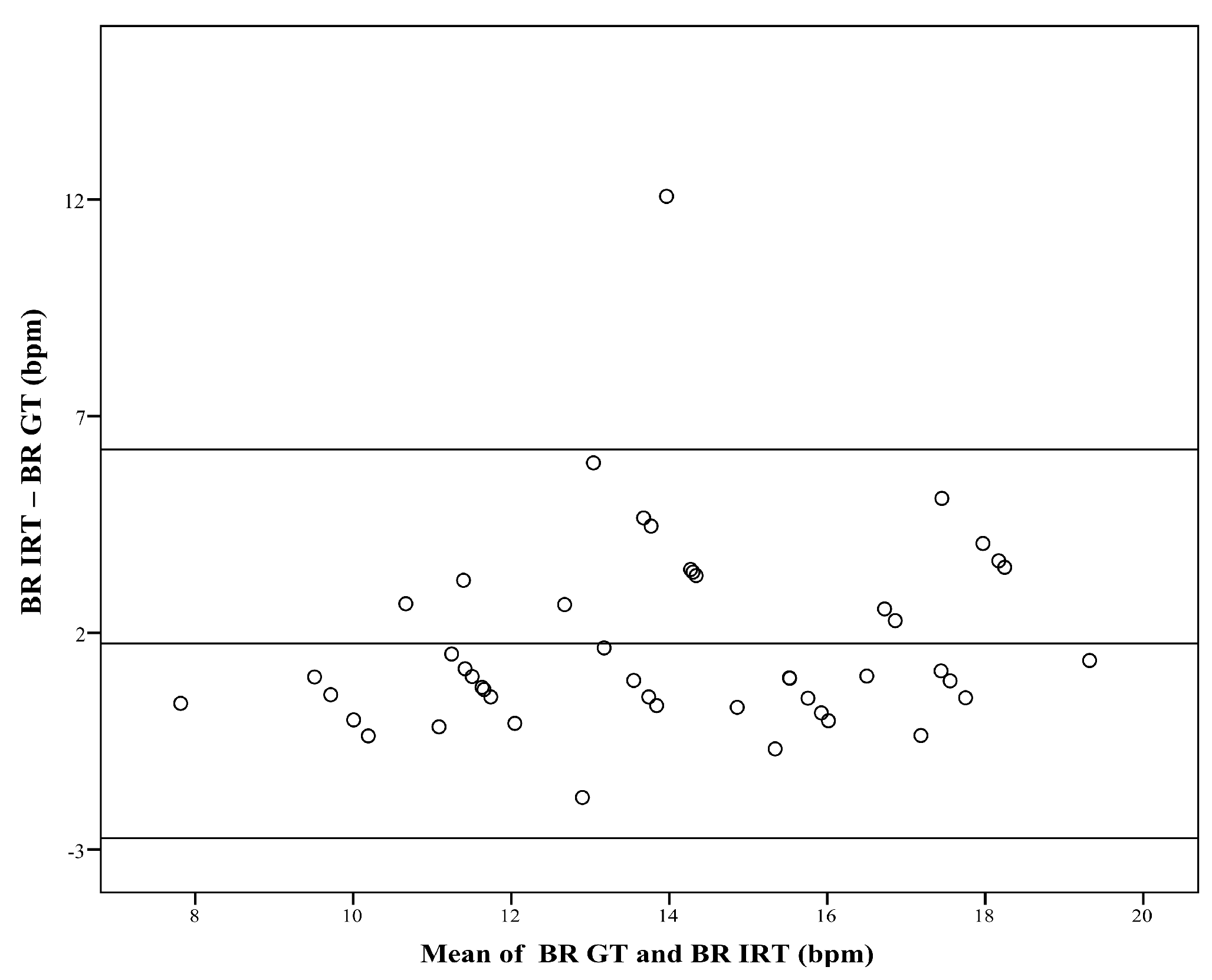
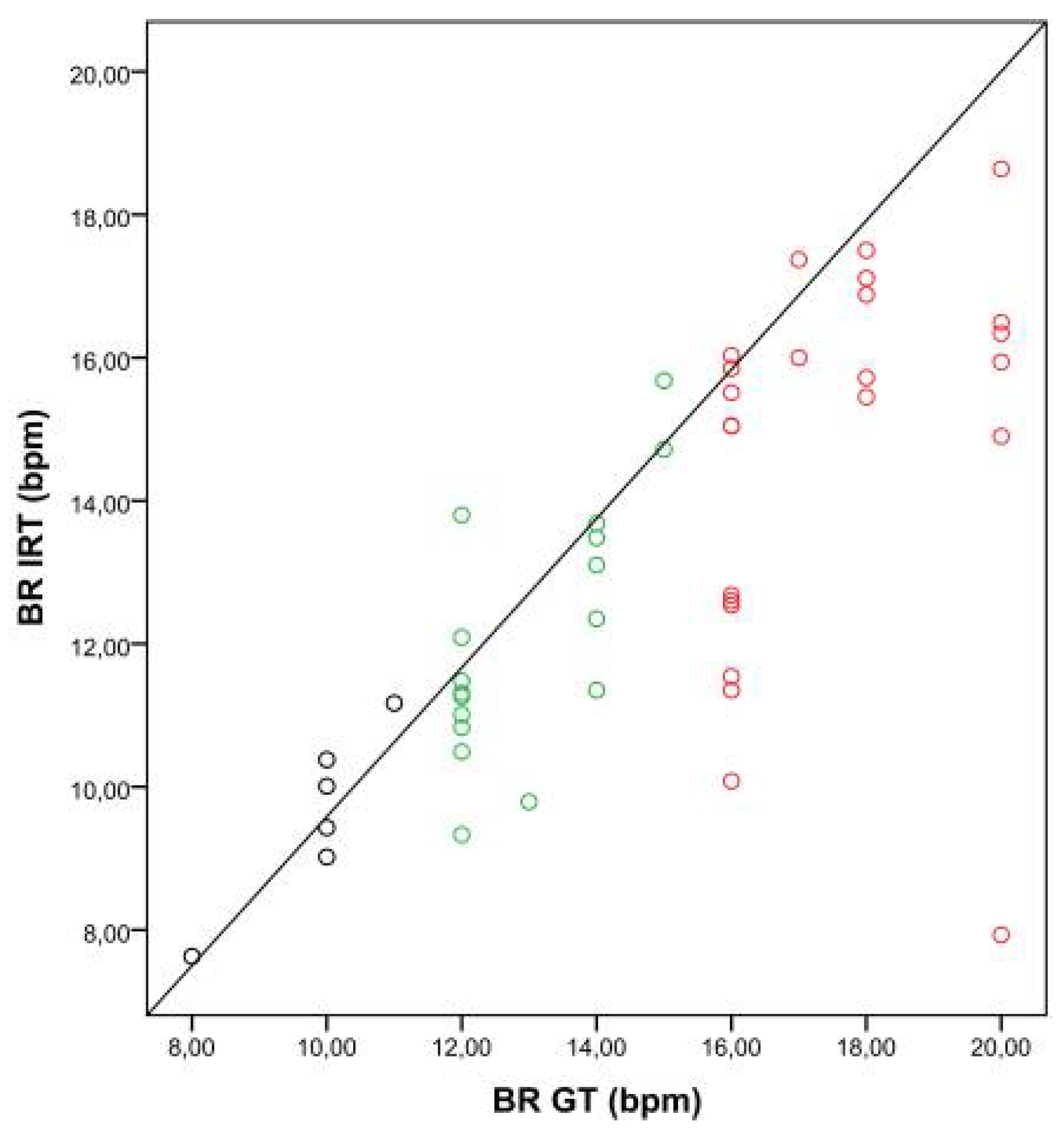
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Feldman, L.S.; Lee, L.; Fiore, J. What outcomes are important in the assessment of Enhanced Recovery after Surgery (ERAS) pathways? Can. J. Anaesth. 2015, 62, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Lalani, S.B.; Ali, F.; Kanji, Z. Prolonged-stay patients in the PACU: A review of the literature. J. Perianesthesia Nurs. 2013, 28, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.K.; Cohen, M.M.; Wigglesworth, D.F.; DeBoer, D.P. Critical respiratory events in the postanesthesia care unit. Patient, surgical, and anesthetic factors. Anesthesiology 1994, 81, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Karcz, M.; Papadakos, P.J. Respiratory complications in the postanesthesia care unit: A review of pathophysiological mechanisms. Can. J. Respir. Ther. 2013, 49, 21–29. [Google Scholar] [PubMed]
- Cavalcante, A.N.; Martin, Y.N.; Sprung, J.; Imsirovic, J.; Weingarten, T.N. Low minute ventilation episodes during anesthesia recovery following intraperitoneal surgery as detected by a non-invasive respiratory volume monitor. J. Clin. Monit. Comput. 2017. [Google Scholar] [CrossRef] [PubMed]
- Broens, S.J.; He, X.; Evley, R.; Olofsen, E.; Niesters, M.; Mahajan, R.P.; Dahan, A.; van Velzen, M. Frequent respiratory events in postoperative patients aged 60 years and above. Ther. Clin. Risk Manag. 2017, 13, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Sessler, D.I.; Dalton, J.E.; Devereaux, P.J.; Shahinyan, A.; Naylor, A.J.; Hutcherson, M.T.; Finnegan, P.S.; Tandon, V.; Darvish-Kazem, S.; et al. Postoperative Hypoxemia Is Common and Persistent: A Prospective Blinded Observational Study. Anesth. Analg. 2015, 121, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory rate: The neglected vital sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar] [PubMed]
- Al-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration rate monitoring methods: A review. Pediatr. Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Droitcour, A.D.; Seto, T.B.; Park, B.-K.; Yamada, S.; Vergara, A.; El Hourani, C.; Shing, T.; Yuen, A.; Lubecke, V.M.; Boric-Lubecke, O. Non-contact respiratory rate measurement validation for hospitalized patients. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC 2009), Minneapolis, MN, USA, 3–6 September 2009; pp. 4812–4815. [Google Scholar] [CrossRef]
- Tattersall, G.J. Infrared thermography: A non-invasive window into thermal physiology. Comp. Biochem. Physiol. A. Mol. Integr. Physiol. 2016, 202, 78–98. [Google Scholar] [CrossRef] [PubMed]
- Ko, L.N.; Raff, A.B.; Garza-Mayers, A.C.; Dobry, A.S.; Ortega-Martinez, A.; Anderson, R.R.; Kroshinsky, D. Skin Surface Temperatures Measured by Thermal Imaging Aid in the Diagnosis of Cellulitis. J. Investig. Dermatol. 2018, 138, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Drucker, A.M.; Piguet, V. Hot Stuff: Thermal Imaging Aids in Cellulitis Diagnosis. J. Investig. Dermatol. 2018, 138, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, R. Automatic analysis of the trunk thermal images from healthy subjects and patients with faulty posture. Comput. Biol. Med. 2015, 62, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Snekhalatha, U.; Rajalakshmi, T.; Gopikrishnan, M.; Gupta, N. Computer-based automated analysis of X-ray and thermal imaging of knee region in evaluation of rheumatoid arthritis. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.F.; Gatto, R.G.; Porges, S.W. A novel method for extracting respiration rate and relative tidal volume from infrared thermography. Psychophysiology 2011, 48, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Garbey, M.; Sun, N.; Merla, A.; Pavlidis, I. Contact-free measurement of cardiac pulse based on the analysis of thermal imagery. IEEE Trans. Biomed. Eng. 2007, 54, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Knobel, R.B.; Guenther, B.D.; Rice, H.E. Thermoregulation and thermography in neonatal physiology and disease. Biol. Res. Nurs. 2011, 13, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.B.; Czaplik, M.; Blanik, N.; Rossaint, R.; Blazek, V.; Leonhardt, S. Contact-free monitoring of circulation and perfusion dynamics based on the analysis of thermal imagery. Biomed. Opt. Express 2014, 5, 1075–1089. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.B.; Yu, X.; Czaplik, M.; Rossaint, R.; Blazek, V.; Leonhardt, S. Remote monitoring of breathing dynamics using infrared thermography. Biomed. Opt. Express 2015, 6, 4378–4394. [Google Scholar] [CrossRef] [PubMed]
- Fei, J.; Pavlidis, I. Thermistor at a distance: Unobtrusive measurement of breathing. IEEE Trans. Biomed. Eng. 2010, 57, 988–998. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.B.; Yu, X.; Blazek, V.; Leonhardt, S. Robust remote monitoring of breathing function by using infrared thermography. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4250–4253. [Google Scholar] [CrossRef]
- Mei, X.; Ling, H. Robust visual tracking and vehicle classification via sparse representation. IEEE Trans. Pattern Anal. Mach. Intell. 2011, 33, 2259–2272. [Google Scholar] [CrossRef] [PubMed]
- Brüser, C.; Winter, S.; Leonhardt, S. Robust inter-beat interval estimation in cardiac vibration signals. Physiol. Meas. 2013, 34, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Gaucher, A.; Frasca, D.; Mimoz, O.; Debaene, B. Accuracy of respiratory rate monitoring by capnometry using the Capnomask(R) in extubated patients receiving supplemental oxygen after surgery. Br. J. Anaesth. 2012, 108, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Marzec, M.; Koprowski, R.; Wróbel, Z. Methods of face localization in thermograms. Biocybern. Biomed. Eng. 2015, 35, 138–146. [Google Scholar] [CrossRef]
- Koprowski, R. Some selected quantitative methods of thermal image analysis in Matlab. J. Biophotonics 2016, 9, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, H. Motwani Image Segmentation for the Extraction of Face Using Haar Like Feature. Int. Arab J. Inf. Technol 2016, 13, 951–958. [Google Scholar]
- AL-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H. Tracking human face features in thermal images for respiration monitoring. In Proceedings of the 2010 IEEE/ACS International Conference on Computer Systems and Applications (AICCSA), Hammamet, Tunisia, 16–19 May 2010; pp. 1–6. [Google Scholar]
- Alkali, A.H.; Saatchi, R.; Elphick, H.; Burke, D. Thermal image processing for real-time non-contact respiration rate monitoring. IET Circuits Devices Syst. 2017, 11, 142–148. [Google Scholar] [CrossRef]
- Chauvin, R.; Hamel, M.; Brière, S.; Ferland, F.; Grondin, F.; Létourneau, D.; Tousignant, M.; Michaud, F. Contact-Free Respiration Rate Monitoring Using a Pan-Tilt Thermal Camera for Stationary Bike Telerehabilitation Sessions. IEEE Syst. J. 2016, 10, 1046–1055. [Google Scholar] [CrossRef]
- Hu, M.; Zhai, G.; Li, D.; Fan, Y.; Duan, H.; Zhu, W.; Yang, X. Combination of near-infrared and thermal imaging techniques for the remote and simultaneous measurements of breathing and heart rates under sleep situation. PLoS ONE 2018, 13, e0190466. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Julier, S.J.; Marquardt, N.; Bianchi-Berthouze, N. Robust tracking of respiratory rate in high-dynamic range scenes using mobile thermal imaging. Biomed. Opt. Express 2017, 8, 4480–4503. [Google Scholar] [CrossRef] [PubMed]
- Zaproudina, N.; Varmavuo, V.; Airaksinen, O.; Närhi, M. Reproducibility of infrared thermography measurements in healthy individuals. Physiol. Meas. 2008, 29, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Ring, E.F.J.; Ammer, K.; Wiecek, B.; Plassmann, P.; Jones, C.; Jung, A.; Murawski, P. Quality assurance for thermal imaging systems in medicine. Thermol. Int. 2007, 17, 103–106. [Google Scholar]
- Ring, E.F.J.; Ammer, K. The Technique of Infrared Imaging in Medicine. Thermol. Int. 2000, 10, 7–14. [Google Scholar] [CrossRef]
- Fernández-Cuevas, I.; Bouzas Marins, J.C.; Arnáiz Lastras, J.; Gómez Carmona, P.M.; Piñonosa Cano, S.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | BR Range | Number of Datasets | Spearman’s Rho Correlation | p Value |
|---|---|---|---|---|
| A | <12 bpm | 6 | 0.845 | 0.034 |
| B | 12–15 bpm | 17 | 0.651 | 0.005 |
| C | >15 bpm | 24 | 0.458 | 0.024 |
| Category | Number of Datasets | Spearman’s Rho Correlation | p Value |
|---|---|---|---|
| No Insufflation | 20 | 0.774 | <0.001 |
| Insufflation | 27 | 0.690 | <0.001 |
| Patient | Time Point | BR (bpm) | Relative Error | Insufflation | Region of Interest (ROI)—Fraction of Image (%) | Breathing Pattern/Patient Movement | |
|---|---|---|---|---|---|---|---|
| Ground Truth (GT) | Infrared Thermography (IRT) | ||||||
| 1 | 1 | 16.00 | 11.54 | 0.28 | no | 0.03 | shallow |
| 2 | 14.00 | 13.68 | 0.02 | no | 0.06 | normal | |
| 2 | 1 | 24.00 | n.a. | n.a. | no | n.a. | shallow |
| 2 | 16.00 | 16.03 | 0.00 | no | 0.07 | normal | |
| 3 | 1 | 16.00 | 12.54 | 0.22 | no | 0.09 | normal |
| 2 | 18.00 | n.a. | n.a. | no | n.a. | movement | |
| 4 | 1 | 20.00 | n.a. | n.a. | no | n.a. | movement |
| 2 | 12.00 | n.a. | n.a. | no | n.a. | movement | |
| 5 | 1 | 14.00 | 13.48 | 0.04 | no | 0.20 | normal |
| 2 | 14.00 | 12.35 | 0.12 | no | 0.20 | normal | |
| 6 | 1 | 18.00 | 17.11 | 0.05 | yes | 0.13 | normal |
| 2 | 20.00 | 18.64 | 0.07 | yes | 0.14 | normal | |
| 7 | 1 | 16.00 | 12.60 | 0.21 | no | 0.16 | shallow/movement |
| 2 | 16.00 | n.a. | n.a. | no | n.a. | movement | |
| 8 | 1 | 20.00 | 15.94 | 0.20 | yes | 0.25 | irregular |
| 2 | 20.00 | 16.49 | 0.18 | yes | 0.21 | irregular | |
| 9 | 1 | 15.00 | 15.68 | 0.05 | no | 0.12 | normal |
| 2 | 18.00 | 17.50 | 0.03 | no | 0.10 | normal | |
| 10 | 1 | 15.00 | 14.72 | 0.02 | yes | 0.12 | normal |
| 2 | 14.00 | 13.10 | 0.06 | yes | 0.13 | normal | |
| 11 | 1 | 17.00 | 16.00 | 0.06 | yes | 0.08 | normal |
| 2 | 11.00 | 11.17 | 0.02 | yes | 0.07 | normal | |
| 12 | 1 | 12.00 | 11.01 | 0.08 | no | 0.18 | normal |
| 2 | 12.00 | 10.49 | 0.13 | no | 0.14 | normal | |
| 13 | 1 | 17.00 | 17.37 | 0.02 | no | 0.12 | normal |
| 2 | 10.00 | 10.01 | 0.00 | no | 0.20 | normal | |
| 14 | 1 | 18.00 | 15.45 | 0.14 | no | 0.10 | normal |
| 2 | 16.00 | 15.85 | 0.01 | no | 0.19 | normal | |
| 15 | 1 | 16.00 | 15.51 | 0.03 | yes | 0.14 | normal |
| 2 | 16.00 | 15.04 | 0.06 | yes | 0.06 | normal | |
| 16 | 1 | 20.00 | n.a. | n.a. | yes | n.a. | no signal |
| 2 | 18.00 | 15.72 | 0.13 | yes | 0.08 | normal | |
| 17 | 1 | 10.00 | n.a. | n.a. | no | n.a. | movement |
| 2 | 12.00 | 13.80 | 0.15 | no | 0.24 | normal | |
| 18 | 1 | 20.00 | 14.90 | 0.26 | no | 0.05 | irregular |
| 2 | 18.00 | 16.88 | 0.06 | no | 0.07 | normal | |
| 19 | 1 | 10.00 | 9.02 | 0.10 | yes | 0.06 | normal |
| 2 | 12.00 | 11.48 | 0.04 | yes | 0.05 | normal | |
| 20 | 1 | 16.00 | 12.68 | 0.21 | yes | 0.04 | irregular |
| 2 | 12.00 | 12.09 | 0.01 | yes | 0.05 | normal | |
| 21 | 1 | 16.00 | 11.35 | 0.29 | yes | 0.13 | apnea |
| 2 | 16.00 | 10.08 | 0.37 | yes | 0.07 | apnea | |
| 22 | 1 | 12.00 | 11.26 | 0.06 | yes | 0.06 | normal |
| 2 | 16.00 | 15.05 | 0.06 | yes | 0.04 | normal | |
| 23 | 1 | 20.00 | 7.93 | 0.60 | yes | 0.10 | apnea |
| 2 | 10.00 | 9.43 | 0.06 | yes | 0.07 | normal | |
| 24 | 1 | 10.00 | 10.38 | 0.04 | yes | 0.16 | normal |
| 2 | 13.00 | 9.79 | 0.25 | yes | 0.13 | apnea | |
| 25 | 1 | n.a. | n.a. | n.a. | no | n.a. | lateral position |
| 2 | n.a. | n.a. | n.a. | no | n.a. | lateral position | |
| 26 | 1 | 20.00 | 16.34 | 0.18 | yes | 0.09 | movement |
| 2 | 12.00 | 11.31 | 0.06 | yes | 0.07 | normal | |
| 27 | 1 | 12.00 | 9.33 | 0.22 | no | 0.06 | movement |
| 2 | 8.00 | 7.63 | 0.05 | no | 0.11 | normal | |
| 28 | 1 | 14.00 | 11.35 | 0.19 | yes | 0.08 | normal |
| 2 | 12.00 | 10.83 | 0.10 | yes | 0.09 | normal | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hochhausen, N.; Barbosa Pereira, C.; Leonhardt, S.; Rossaint, R.; Czaplik, M. Estimating Respiratory Rate in Post-Anesthesia Care Unit Patients Using Infrared Thermography: An Observational Study. Sensors 2018, 18, 1618. https://doi.org/10.3390/s18051618
Hochhausen N, Barbosa Pereira C, Leonhardt S, Rossaint R, Czaplik M. Estimating Respiratory Rate in Post-Anesthesia Care Unit Patients Using Infrared Thermography: An Observational Study. Sensors. 2018; 18(5):1618. https://doi.org/10.3390/s18051618
Chicago/Turabian StyleHochhausen, Nadine, Carina Barbosa Pereira, Steffen Leonhardt, Rolf Rossaint, and Michael Czaplik. 2018. "Estimating Respiratory Rate in Post-Anesthesia Care Unit Patients Using Infrared Thermography: An Observational Study" Sensors 18, no. 5: 1618. https://doi.org/10.3390/s18051618