
Tobacco Profile and Evaluation of the DS14 Scale in Patients with Coronary Syndrome

1
Faculty of Nursing and Professional Health Studies, Slovak Medical University in Bratislava, 833 03 Bratislava, Slovakia
2
Department of Acute Cardiology-Coronary Care, National Institute for Cardiovascular Diseases, 833 48 Bratislava, Slovakia
*
Author to whom correspondence should be addressed.
Psych 2021, 3(4), 694-702; https://doi.org/10.3390/psych3040044
Submission received: 29 September 2021
/
Revised: 11 November 2021
/
Accepted: 17 November 2021
/
Published: 20 November 2021
Abstract
:Background: the prevalence of current smokers in patients with coronary syndrome is high. This risk behaviour significantly increases the risk of cardiovascular complications. In the recommendations for the management of cardiovascular diseases, psychosocial and psychological factors are still neglected in practice. The aim of study was to verify the prevalence of tobacco use in hospitalized patients with coronary syndrome, notably to verify the type-D personality and tobacco use in the groups obtained from the evaluation of the DS14 scale. Methods: in this cross-sectional study, we addressed 100 hospitalized patients with coronary syndrome. Results: in the cohort, 48% patient were current smokers, 21% were never smokers, 24% were former smokers, 4% were occasional smokers, and 3% were quitters. Based on the evaluation of DS14, 21% of patients were classified as type-D personality and 38% as non-type-D; we identified two subtypes: the NA group at 23% and the SI group at 18%. In the group of the current smokers, 81% declared that they wanted to quit smoking, 15% of the patients were undecided, and 4% of current smokers did not want to quit. Conclusions: cardiac patients are aware that their disease is related to smoking; despite the severity of their disease, patients’ motivation to change their risky behaviour is low.
1. Introduction
Atherosclerotic cardiovascular disease (ASCVD) incidence and mortality rates are declining in many countries in Europe, but it is still a major cause of morbidity and mortality. Over the past few decades, major ASCVD risk factors have been identified. The most important way to prevent ASCVD is to promote a healthy lifestyle throughout life, especially not smoking [1]. Seventy to eighty percent of smokers are tobacco dependent [2] according to the International Classification of Diseases 10 diagnosis code F17. In recommendations for the prevention of cardiovascular disease (CVD), the European Society of Cardiology considers smoking to be the most important risk factor for CVD [3]. Regular smoking kills 50% of its consumers, and almost half of them die from CVD. Regular smokers live 10 to 15 years shorter than non-smokers [4]. The prevalence of current smokers in the general population in Slovakia over 15 years of age is about 23% [5]. Regular tobacco use is one of the leading causes of non-communicable chronic diseases [6]. Second-hand smoke has a 30% risk of developing acute coronary syndrome (ACS) and as much as an 80% negative impact on blood vessels as active smoking [7]. Smoking cessation before the age of 40 reduces the risk of premature death by approximately 90%, and before the age of 60 reduces this risk by 40% [8]. Approximately 70% of smokers want to quit, and 44% attempt to quit annually, with successful quitting in approximately 4–7% of smokers without professional support [9].
Research on the relationship between psychosocial stress and coronary heart disease (CHD) was dominated in the seventies and eighties by work on the type-A behaviour pattern. Initially, a cluster of diverse symptoms and behavioural signs were involved in the characterization of this type-A pattern, but, eventually, hostility was considered to be one of the core features. A more recent and promising line of research is the work on type-D, a personality type predicting long-term mortality in CHD patients, independently of established biomedical risk factors (RF). Type-D refers to individuals who simultaneously tend to experience negative emotions and who tend to inhibit self-expression in social interaction [10]. Patients with type-D personality are at risk for numerous psychological risk factors, including depression, anxiety and irritability, low levels of self-esteem, and positive affect [11]. Type-D personality has a 4.1 to 8.9 times higher risk for heart disease and mortality from these diseases than non-Type-D personalities [12]. A meta-analysis of studies conducted on different populations of patients with CVD suggests that type-D personality is associated with twice the odds of worsening physical health status and 2.5 times the odds of worsening mental health status [13]. Meta-analyses suggest that patients with type-D personality have significantly impaired quality of life compared with patients with CVD without type-D personality characteristics [14]. Type-D personality is a characteristic of 21% to 52% of patients with CVD. In the general population, the prevalence of type-D personality ranges from 13% to 40% [15]. Type D is assessed by the ESC as a psychosocial risk factor for the development and prognosis of cardiovascular diseases [3].
2. The Aim of the Study
This cross-sectional study was conducted to verify the prevalence of tobacco use in hospitalized patients with coronary syndrome and to test the strength of tobacco and cigarette dependence in current smokers. Another aim was to verify the prevalence of type-D personality in hospitalized patients with coronary syndrome and to determine the prevalence of tobacco use in the groups obtained from the evaluation of the DS14 scale.
3. Materials and Methods
In the period from 2 of January 2017 to 15 of September 2017 we conducted a pilot study in which we addressed 100 patients. The patient cohort consisted of patients hospitalized with coronary syndrome at the National Institute for Cardiovascular Diseases, Acute Cardiology Department—Coronary Care in Bratislava. Patients’ participation in the study was voluntary, and the information obtained was treated confidentially. In current smokers, we used the Fageström test (FTCD) [16,17] to verify cigarette dependence; the test contains 6 items where 1 to 10 points can be obtained. In this study, the heavy smoking index (HSI) was used [18]; the test contains 2 items where 0 to 6 points can be obtained. The DS14 [11], a short psychometric instrument, was used to test the type-D personality, which consists of 14 items; it has two subscales: for negative affectivity and social inhibition; both contain 7 items. A total score of 0 to 28 points can be obtained on both subscales. The return rate of the questionnaires was 100%.
Statistical Method
All statistics were generated using SPSS 22. Descriptive statistics were calculated for the whole sample. Variables obtained were tested for normality of distribution by the Kolmogorov–Smirnov test. The non-parametric Mann–Whitney U-test was used to compare the means of the numerical variables. All tests were performed at a significance level of α = 0.05.
4. Results
4.1. Demographic Characteristics
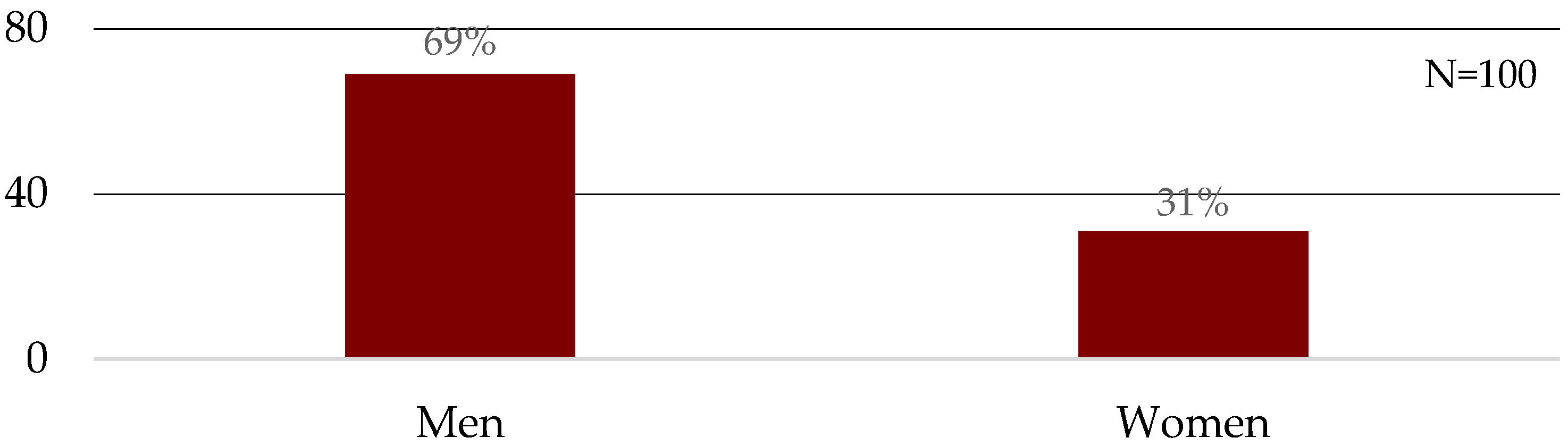
The cohort consisted of 69% male and 31% female participants (Figure 1). The mean age of the patients was 59.13 ± 10.98 SD years, 61.77 ± 12.16 SD years for females, and 57.94 ± 10.28 SD years for males.
Educational level: 35% of the patients had high-school education, 30% had apprenticeship education, 32% had university education, and 3% had primary education.
Work ability: 43% patients reported work ability as working/employed, 34% were retired, 11% were self-employed, 7% were working pensioners, and 3% were disabled pensioners.
Marital status: 57% of patients were married, 22% divorced, 7% widowed, 7% single, and 7% had a spouse. The mean number of days of hospitalization was 4.25 ± 3.82 SD.
4.2. Tobacco Use
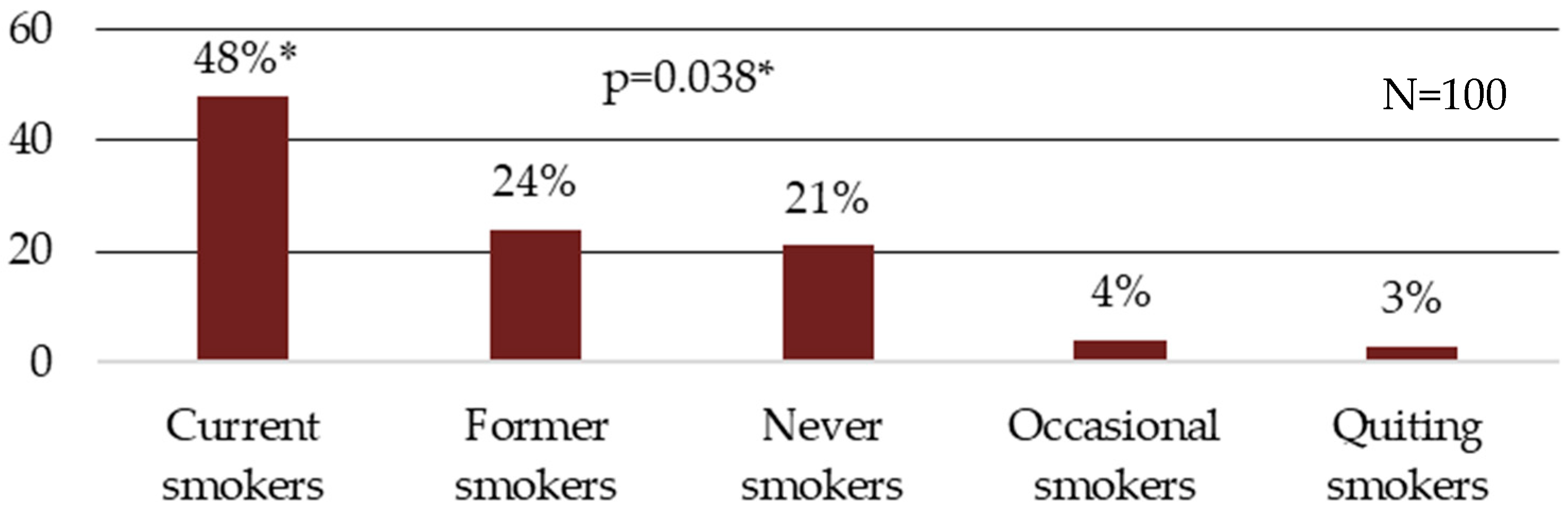
In this cohort, 48% were current smokers, 21% were never smokers, 24% were former smokers, 4% were occasional smokers, and 3% were quitters (Figure 2).
Gender and tobacco use: 52% of male were smokers, and 39% of female were smokers.
Education and tobacco use: 57% of smokers had an apprenticeship education, 49% had a high school diploma, and 34% had a university degree.
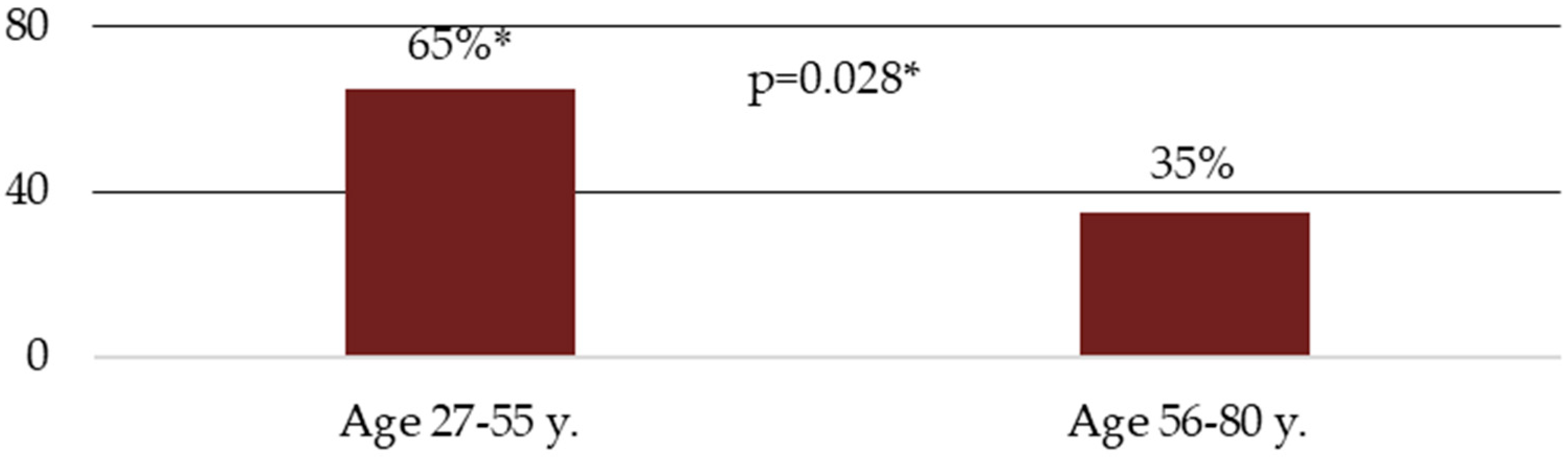
The age groups corelated with tobacco use: in the 27–55-year-old group, 65% were smokers, and in the 56–80-year-old group, 35% were smokers (Figure 3).
The mean number of cigarettes smoked in the current smokers was 19.37 ± 6.96 SD cigarettes per day, 16.67 ± 7.78 SD in females, and 20.28 ± 6.54 in males.
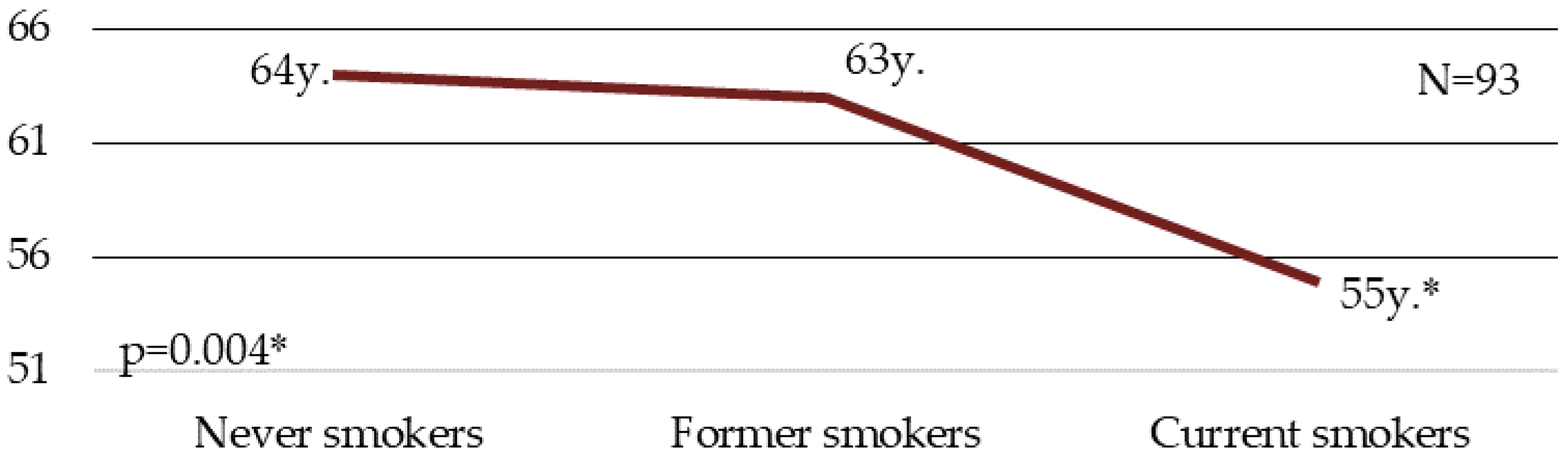
Median age and tobacco use: the median age in never smokers was 64 years; in former smokers 63 years and current smokers 55 years (Figure 4).
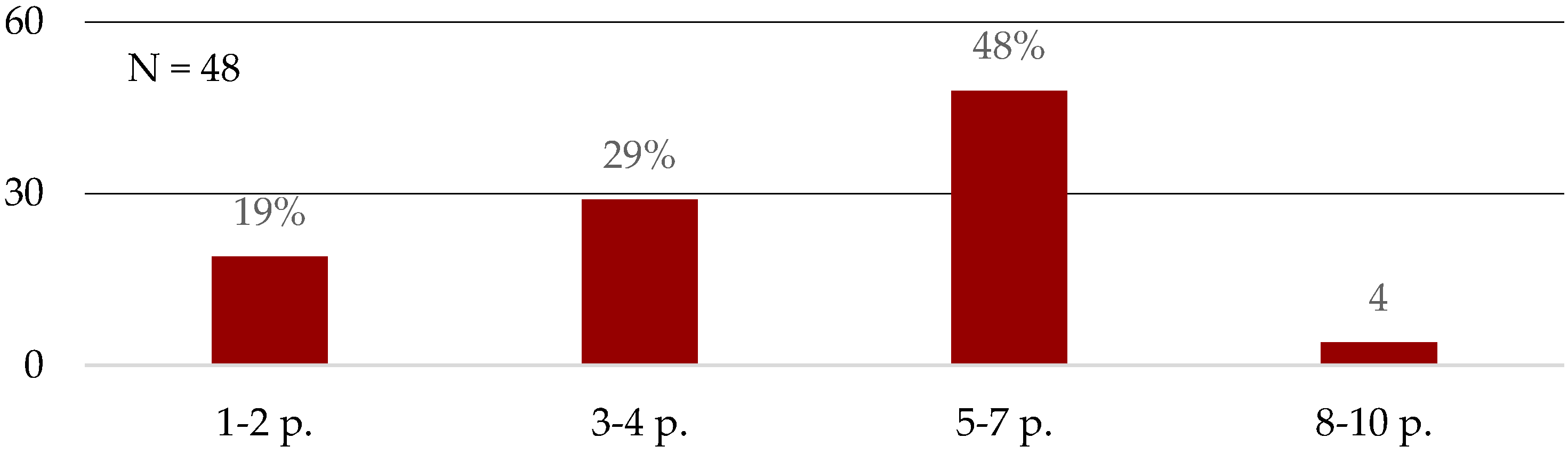
Evaluation of FTCD: 19% of current smokers scored 1–2 points; 29% scored 3–4 points; 48% of current smokers scored 5–7 points and 4% scored 8–10 points (Table 1) (Figure 5).
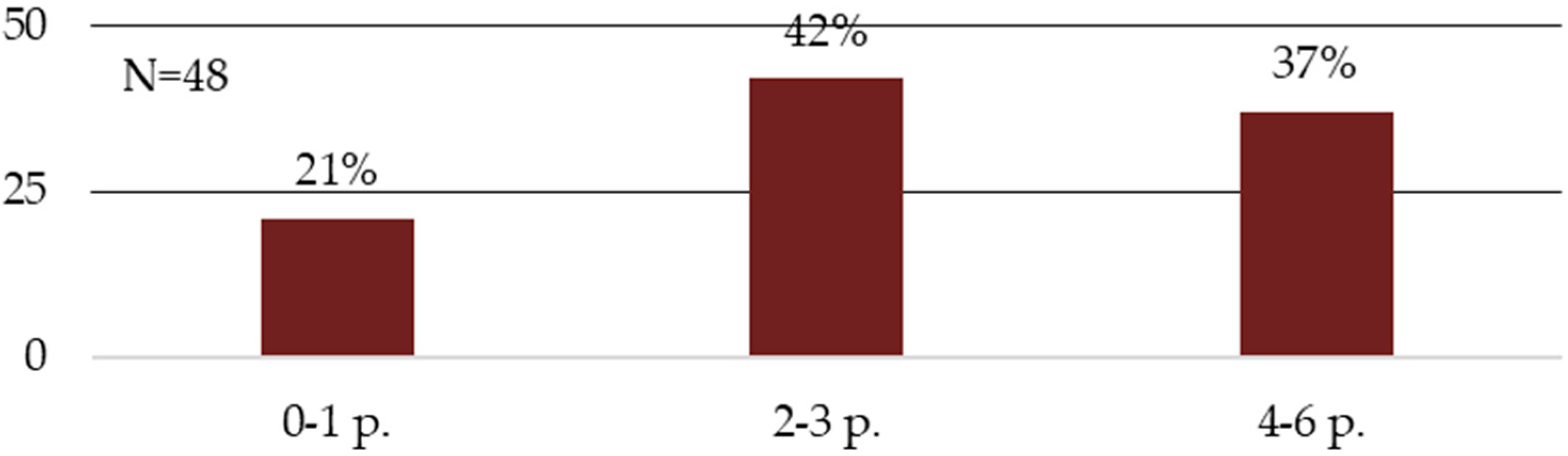
Evaluation of HIS: 21% of current smokers scored 0–1 points, 42% scored 2–3 points and 37% of current smokers scored 4–6 points (Table 2) (Figure 6).
Evaluation of DS 14: 21% of patients were a type-D personality, while 38% were non-type-D, and there were two sub-types: NA group 23% and SI group 18% (Table 3).
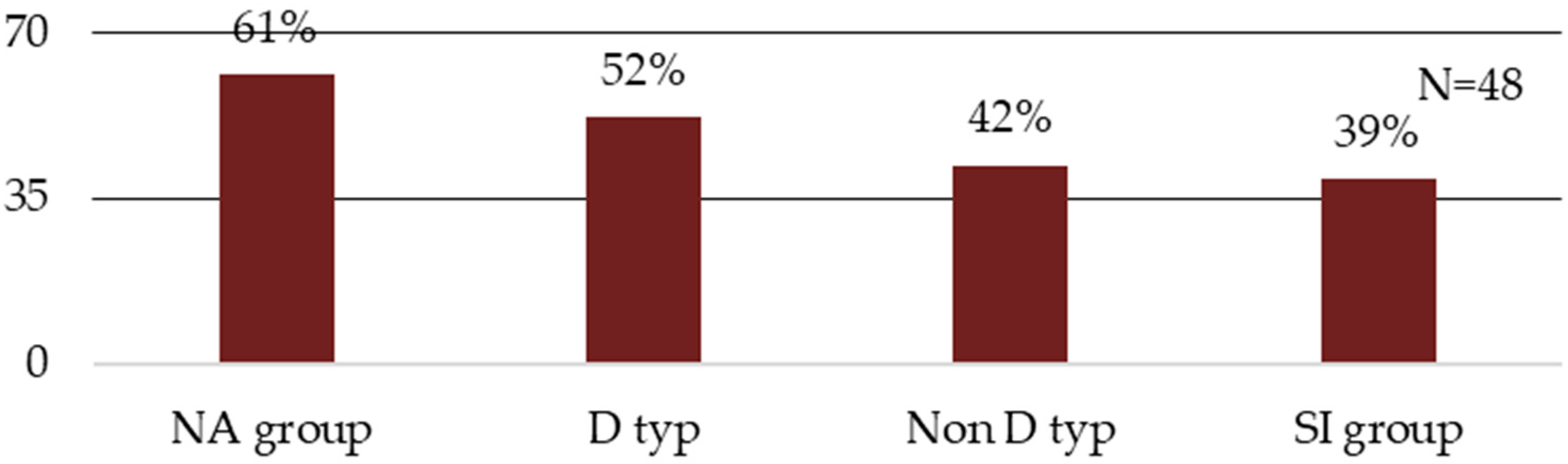
DS 14 and current smokers: 61% of NA group, 52% of type D, 42% of non-type-D, and 39% of the SI group were current smokers (Figure 7).
Eighty-one percent of the current smokers indicated that they wanted to quit smoking, 15% of the patients were undecided, and 4% indicated that they did not want to quit smoking. All current smokers used tobacco in the form of cigarettes.
5. Discussion
Almost half of the patients with coronary syndrome were current smokers. This represents a significant difference when compared to patients who never smoked, obviously when comparing the mean age of the two groups. After comparing the results of the two tests to verify cigarette and tobacco dependence, only one-fifth of the current smokers scored for very weak dependence. Even smokers who smoke a lower number of cigarettes are still at risk. Lower daily cigarette consumption is notably associated with an increased risk of coronary events and premature mortality [7]. Most current smokers scored values for moderate, strong, or very strong dependence.
A smoker who smokes at least 10–15 cigarettes a day and needs to light their first cigarette within an hour after waking up is strongly addicted to tobacco. In this cohort, the prevalence of current smokers is significantly higher in the younger age group than in the older age group. This risky behaviour can lead to a significantly higher cardiovascular risk and incidence of complications in terms of prognosis. Young smokers who smoke more than 20 cigarettes per day have 5.6 times higher risk of acute myocardial infarction (MI) than similarly aged non-smokers. For the population as a whole, i.e., independent of age, the risk of fatal MI is three times higher in smokers than in non-smokers. Smoking acts synergistically and in complex with other RF [19], referring to biomedical RF, which contributes markedly to the development of CVD, specifically in young people, and to possible complications in patients already with CVD. Dyslipidemia, positive family history, overweight and obesity are among the strong RF in young patients, right after smoking. Hypertension and diabetes are less represented but strongly apply in the group of young patients with coronary artery disease [20].
The cardiovascular risk drops by almost a third after 24 h of smoking cessation and by almost half after a year of abstinence. Patients who do not discontinue this risky behaviour after discharge remain at high cardiovascular risk. Health professionals have a key role in the secondary prevention, support, assistance, and treatment of smoking cessation. A brief intervention lasting up to 10 min should be given to any patient at clinical contact who wishes to quit smoking, either following the 5As model or the ABC brief intervention. A brief intervention of up to 10 min increases quit rates by 5 to 10%. In our study cohort, the vast majority of smokers said they wanted to quit. Part of proper and effective support includes maintaining anamnestic data in the medical record of tobacco use, based on which we can provide adequate support and assistance to the patient to quit smoking [19].
The prevalence of smokers in the NA and type-D group was higher than in the non-type-D and SI group. The prevalence of smokers is higher among subjects with anxiety or depression, and the correlation between these variables increases cardiovascular risk and acute cardiac events. Early depressive and anxiety symptoms occur more frequently in patients with acute coronary syndrome associated with type-D personality with adverse effects on cardiac outcomes. Smoking cessation for type-D patients or those with higher rates of survival anxiety is often more challenging compared to non-type-D personalities and post-cessation lapses and relapses are frequent, which significantly increases cardiovascular risk for these patients [21]. Psychosocial factors such as stress and distress, depression, and anxiety are associated with poorer outcomes in patients with CVD, making it difficult for patients to implement positive lifestyle changes and adhere to their treatment regimen [22]. In smokers with higher rates of survival anxiety and type-D personality, the incidence of cardiovascular risk is several times higher because it is notably associated with an unhealthy lifestyle: more cigarettes, higher alcohol consumption, consumption of unhealthy foods, less physical activity, and poorer adherence to treatment [21]. In routine clinical practice, type-D personality is not validated in patients with coronary syndrome. Therefore, during hospitalization health professionals ought to adequately inform and effectively educate the patient about proper lifestyle, risk factors, and the need for mental hygiene and relieving excessive stress, while letting the patient talk about difficulties because this is how we can help the patient, regardless of personality type. These are situations where the nurse can communicate more openly and actively with the patient, which could be effective to overcome high social inhibition in type-D patients who may have inhibitions to ask about their own health or treatment. Another way to help type-D patients may be psychosocial interventions that promote positivity and that reduce the experience of negative emotions. The appropriate nurse-led psychosocial interventions during hospitalization reveal beneficial effects on anxiety, depression, and overall well-being in patients with CVD [3]. In patients discharged, the percentage classified as type D was relatively stable; type D in patients after MI was stable over the next 18 months regardless of mood changes and severity of illness [23]. This fact implies a significant risk of cardiac complications considering other risk factors acting synergistically that an individual may have and experience in personal life.
Smokers are in a state of cessation during hospitalization when they may experience tobacco withdrawal syndrome, which often manifests itself in both behaviour and psychological well-being. The withdrawal state usually begins twenty-four hours after the last dose of nicotine, with some of the symptoms persisting for weeks or months. It includes craving for smoking, which is worse in the evening and which is accompanied by irritability, impatience, impaired concentration, depressive symptomatology, anxiety, restlessness, and sleep disturbance [2]. Smokers who have had an acute cardiac event may benefit from the application of nicotine replacement therapy both in managing withdrawal symptoms during hospitalization and in continuing smoking cessation after discharge [23]. Pharmacotherapy to support smoking cessation is effective, safe, and associated with significant reductions in rehospitalizations and mortality [24]. Health professionals should play an active and significant role in tobacco control and tobacco dependence treatment support [25]. During hospitalization and after assessing for relevance, the nurse should provide the patient with information regarding smoking cessation, support the patient’s efforts to quit, and empathically motivate the patient in brief interventions, while emphasizing the positives of quitting and pointing out the negatives of not quitting, the potential complications, and the poorer prognosis. During hospitalization for patients, who wish to quit smoking, should be advised to seek tobacco dependence treatment in one of the tobacco dependence treatment centres or the smoking cessation counselling service. Smoking cessation improves prognosis in patients with CVD, including a 36% reduction in mortality risk in those who have already quit smoking [22]. At the tobacco dependence treatment centre, the patient is dispensed for one year, where receiving psychological and behavioural interventions, pharmacotherapy if necessary, and regular check-ups [19]. It is known that smoking cessation is a complex and challenging process because tobacco is highly addictive both pharmacologically and psychologically. Therefore, family involvement and support are important in smoking cessation and can significantly help the process [24].
6. Conclusions
- 48% of patients with coronary syndrome were current smokers
- 52% of male and 39% of female patients were current smokers
- 55 years was the median of age in the group of current smokers
- 65% of the 27–55 age group and 35% of the 56–80 age group were smokers
- 21% of patients were a type-D personality, while 38% were non-type-D personality
- 61% of NA group, 52% of type—D personality were current smokers
- 80% of the current smokers scored for moderate, strong, or very strong dependence
- 19.37 ± 6.96 SD was the mean number of cigarettes smoked per day
- 81% of the current smokers indicated that they wanted to quit smoking.
We must pay increased attention to patients with cardiovascular disease not only in the area of smoking but also in experiencing negative emotions and mental well-being. Patients should be encouraged and motivated to quit smoking and to change their lifestyle by promoting mental well-being and supporting adherence to treatment, we can make a significant contribution to secondary prevention.
Author Contributions
G.B. pilot study researcher, Z.S. supervisor, E.M. supervisor specialist. Conceptualization, G.B. and Z.S.; methodology, G.B.; software, G.B.; validation, G.B., Z.S. and E.M.; formal analysis, G.B.; investigation, G.B.; resources, G.B.; data curation, G.B.; writing—original draft preparation, G.B.; writing—review and editing, Z.S.; visualization, E.M.; supervision, Z.S.; project administration, G.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and Principles for Medical Research Involving Human Subjects following the Regulation 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data (GDPR) as a data subject (research participant). Ethical review and approval were waived for this study, due to the legislation of the Slovak Republic, this type of research does not require the approval of an Ethics Committee. This pilot research was authorized and approved by the management of the Department of Acute Cardiology—Coronary Care, and by the management of National Institute for Cardiovascular Diseases on 30 of January 2017.
Informed Consent Statement
Patients’ participation in the study was voluntary. Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patients for publication of the study results.
Data Availability Statement
The data used in this pilot study are included within the article.
Acknowledgments
We acknowledge all the patients with coronary syndrome who participated in this pilot study.
Conflicts of Interest
The authors declare no conflict of interest.
Limitations
The limitation of this study was the low number of patients, and the results of this pilot study should not be generalized. Further research in this area is needed and recommended.
References
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. Available online: https://academic.oup.com/eurheartj/article/42/34/3227/6358713 (accessed on 10 November 2021). [CrossRef] [PubMed]
- Kalina, K. Klinická Adiktologie; GRADA: Prague, Czech Republic, 2015; p. 696. [Google Scholar]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2016, 37, 2315–2381. Available online: https://academic.oup.com/eurjpc/article/23/11/NP1/5927332?login=true (accessed on 15 April 2018). [CrossRef] [PubMed]
- Peto, R.; Boreham, J.; Lopez, A.D.; Thun, M.; Heath, C. Mortality from tobacco in developed countries: Indirect estimation from national vital statistics. Lancet 1992, 339, 1268–1278. Available online: https://gas.ctsu.ox.ac.uk/tobacco/SMK_P3_4.pdf (accessed on 20 February 2021). [CrossRef]
- European Union. Attitudes of Europeans towards Tobacco and Electronic Cigarettes. Spec. Eurobarom. 2015, 429. Available online: https://www.drugsandalcohol.ie/24004/2/Eurobarometer%20attitudes%20to%20tobacco%20summary.pdf (accessed on 8 October 2020).
- Noncommunicable Diseases. World Health Organization: Geneva, Switzerland, 2017; pp. 1–10. Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/350278/Fact-sheet-SDG-NCD-FINAL-25-10-17.pdf (accessed on 15 April 2021).
- Barnoya, J.; Glantz, S.A. Cardiovascular effects of secondhand smoke: Nearly as large as smoking. Circulation 2005, 111, 2684–2698. Available online: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.104.492215?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed (accessed on 8 October 2020). [CrossRef] [Green Version]
- Fernández-García, D.; Ordás, B.; Fernández-Peña, R.; Bárcena-Calvo, C.; Ordoñez, C.; Amo-Setién, F.J.; Gómez-Salgado, J.; Martínez-Isasi, S. Smoking in nursing students: A prevalence multicenter study. Medicine 2020, 99, e19414. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7220658/pdf/medi-99-e19414.pdf (accessed on 15 February 2021). [CrossRef] [Green Version]
- Hurt, R.D.; Ebbert, J.O.; Hays, J.T.; McFadden, D.D. Treating tobacco dependence in a medical setting. Cancer J. Clinitians 2009, 59, 314–326. Available online: https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.20031 (accessed on 5 April 2021). [CrossRef] [Green Version]
- De Fruyt, F.; Denollet, J. Type D Personality: A Five-Factor Model Perspective. Psychol. Health 2002, 17, 671–683. [Google Scholar] [CrossRef]
- Denollet, J. DS 14: Standard Assessment of Negative Affectivity, Social Inhibition, and Type D Personality. Psychosom. Med. 2005, 67, 89–97. Available online: https://tilburguniversity.edu/upload/72798a0a-2696-4145-b2f8-9d1c392e3516_DS14.Psychosom%20Med%202005.pdf (accessed on 10 January 2021). [CrossRef] [PubMed]
- Tuka, V. Preventivní Kardiologie Pro Praxi; NOL: Prague, Czech Republic, 2018; p. 319. [Google Scholar]
- Ďurka, R.; Holdoš, J. Sociálna inhibícia a negatívna afektivita a ich vzťah ku závislosti od internetu. Sociálna A Duch. Rev. 2013, 4, 36–44. [Google Scholar]
- Podlipný, J. Psychosociální rizikové faktory kardiovaskulárních onemocnění a možnosti jejich ovlivnění. Kardiol. Rev. Interní Med. 2013, 4, 230–233. [Google Scholar]
- Lukoševičiūtė, J.; Šmigelskas, K. Type D personality in cardiovascular patients and general population: Prevalence and retrospective perception of stability. Int. J. Psychol. A Biopsychosoc. Approach 2017, 19, 41–60. [Google Scholar] [CrossRef] [Green Version]
- Fagerström, K.O. Determinants of tobacco use and renaming the FTND to the Fagerstrom Test for Cigarette Dependence. Nicotine Tob. Res. 2012, 14, 75–78. Available online: https://academic.oup.com/ntr/article-abstract/14/1/75/1047894 (accessed on 15 February 2021). [CrossRef] [PubMed] [Green Version]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Chabrol, H.; Niezborala, M.; Chastan, E.; de Leon, J. Comparison of the Heavy Smoking Index and of the Fagerstrom Test for Nicotine Dependence in a sample of 749 cigarette smokers. Addict. Behav. 2005, 30, 1474–1477. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0306460305000316?via%3Dihub (accessed on 10 October 2020). [CrossRef] [PubMed]
- Králíková, E. Závislost na Tabáku, Epidemiologie, Prevence a Léčba; Adamira: Prague, Czech Republic, 2013; p. 469. [Google Scholar]
- Riečanský, I.; Pacák, J.; Péč, J.; Melicherčík, J. Infarkt Myokardu v Mladom Veku-Naše Výsledky a Skúsenosti. Vnitřní Lékařství 2012, 7–8, 536–543. [Google Scholar]
- Imbalzano, E.; Vatrano, M.; Quartuccio, S.; Ceravolo, R.; Ciconte, V.A.; Rotella, P.; Pardeo, R.; Trapani, G.; De Fazio, P.; Segura-Garcia, C.; et al. Effect of type D personality on smoking status and their combined impact on outcome after acute myocardial infarction. Clin. Cardiol. 2018, 41, 321–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Buckley, J.; Furze, G.; Sheppard, G. Cardiovascular Prevention and Rehabilitation in Practice, 2nd ed.; Wiley-Blackwell: London, UK, 2020; p. 336. [Google Scholar]
- Kotseva, K.; Wood, D.; De Backer, G.; De Bacquer, D.; Pyörälä, K.; Keil, U.; EUROASPIRE Study Group. Cardiovascular prevention guidelines in daily practice: A comparison of EUROASPIRE I, II, and III surveys in eight European countries. Lancet 2009, 373, 929–940. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)60330-5/fulltext (accessed on 20 February 2021). [CrossRef]
- The Role of Health Professionals in Tobacco Control; World Health Organization: Geneva, Switzerland, 2005; p. 39. Available online: https://apps.who.int/iris/handle/10665/43219 (accessed on 20 January 2021).
Figure 1.
Gender of patients.

Figure 2.
Tobacco profile of patients with coronary syndrome. * In this cohort, 48% were current smokers, 21% were never smokers, 24% were former smokers, 4% were occasional smokers, and 3% were quitters.
Figure 2.
Tobacco profile of patients with coronary syndrome. * In this cohort, 48% were current smokers, 21% were never smokers, 24% were former smokers, 4% were occasional smokers, and 3% were quitters.

Figure 3.
Prevalence of tobacco use in age groups. * The age groups corelated with tobacco use: in the 27–55-year-old group, 65% were smokers, and in the 56–80-year-old group, 35% were smokers.
Figure 3.
Prevalence of tobacco use in age groups. * The age groups corelated with tobacco use: in the 27–55-year-old group, 65% were smokers, and in the 56–80-year-old group, 35% were smokers.

Figure 4.
Median age and tobacco use. * Median age and tobacco use: the median age in never smokers was 64 years; in former smokers 63 years and current smokers 55 years.
Figure 4.
Median age and tobacco use. * Median age and tobacco use: the median age in never smokers was 64 years; in former smokers 63 years and current smokers 55 years.

Figure 5.
Obtained groups based on FTCD evaluation.

Figure 6.
Obtained groups based on HSI evaluation.

Figure 7.
DS 14 and current smokers.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Evaluation of FTCD and number of cigarettes per day.
| N = 48 | 1–2 p. | 3–4 p. | 5–7 p. | 8–10 p. |
|---|---|---|---|---|
| Smokers | 19% | 29% | 48% | 4% |
| Cigarettes/day | 11.11 ± 3.33 SD | 17.86 ± 4.76 SD | 22.61 ± 4.49 SD | 35.00 ± 7.07 SD |
Table 2.
Evaluation of HSI and number of cigarettes per day.
| N = 48 | 0–1 p. | 2–3 p. | 4–6 p. |
|---|---|---|---|
| Smokers | 21% | 42% | 37% |
| Cigarettes/day | 11.00 ± 3.16 SD | 19.00 ± 5.52 SD | 24.44 ± 5.11 SD |
Table 3.
Evaluation of DS 14.
| N = 100 | Type D | Non-Type-D | NA Group | SI Group |
|---|---|---|---|---|
| NA subscale | 14.52 ± 4.36 SD | 4.24 ± 2.93 SD | 11.96 ± 2.20 SD | 5.61 ± 2.85 SD |
| SI subscale | 14.48 ± 3.53 SD | 4.71 ± 2.66 SD | 6.26 ± 2.54 SD | 14.22 ± 3.70 SD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bálint, G.; Slezáková, Z.; Miklovičová, E. Tobacco Profile and Evaluation of the DS14 Scale in Patients with Coronary Syndrome. Psych 2021, 3, 694-702. https://doi.org/10.3390/psych3040044
AMA Style
Bálint G, Slezáková Z, Miklovičová E. Tobacco Profile and Evaluation of the DS14 Scale in Patients with Coronary Syndrome. Psych. 2021; 3(4):694-702. https://doi.org/10.3390/psych3040044
Chicago/Turabian StyleBálint, Gabriel, Zuzana Slezáková, and Emília Miklovičová. 2021. "Tobacco Profile and Evaluation of the DS14 Scale in Patients with Coronary Syndrome" Psych 3, no. 4: 694-702. https://doi.org/10.3390/psych3040044